
Abstract
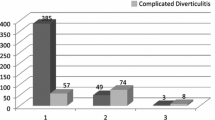
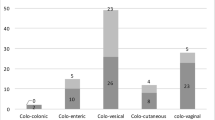
PURPOSE: The purpose of this study was to evaluate the safety and efficacy of laparoscopic-assisted sigmoid colectomy for the treatment of diverticulitis. METHODS: The Norfolk Surgical Group Laparoscopic Surgery Registry identified all patients undergoing laparoscopic colon and rectal surgery. Retrospective chart review was performed for all patients undergoing elective sigmoid resection for a final diagnosis of diverticulitis and minimum follow-up of 12 months. Demographic data, indications for surgery, operative data, conversion rate, reason for conversion, complications, postoperative course (days to flatus and regular diet), and length of stay were identified. A telephone survey determined the incidence of recurrent diverticulitis. Statistical analysis was performed to evaluate the frequency of conversion over time, to determine risk factors for conversion, and to compare the laparoscopic-assisted and conversion groups with regard to postoperative days to flatus, regular diet, and discharge. RESULTS: From June 1992 to September 1997, elective laparoscopic-assisted sigmoid colectomy was attempted in 69 patients. Uncomplicated recurrent diverticulitis was the most common indication for surgery, occurring in 51 of 69 patients (75 percent). No deaths occurred. Complications were identified in seven patients (10.1 percent) including one wound infection and one incarcerated port-site hernia with small bowel obstruction. There were no anastomotic leaks or major septic complications. Conversion to laparotomy occurred in 18 of 69 patients (26 percent). Uncomplicated, recurrent diverticulitis was associated with conversion in 7 of 51 patients (14 percent), whereas complicated diverticulitis required conversion in 11 of 18 patients (61 percent). Logistic regression identified fistula and abscess as predictors of conversion (P=0.0009). Comparison of the laparoscopic-assisted sigmoid colectomy group with the conversion group revealed that postoperative days to regular diet were 3.5 and 5.2 (P=0.0004), respectively, and lengths of stay were 4.2 and 6.4 days (P<0.0001), respectively. No difference was noted with regard to operative time or postoperative complications. Median follow-up was 48 (range, 13–76) months, and a single recurrence of diverticulitis has been identified. CONCLUSIONS: Laparoscopic-assisted sigmoid colectomy for diverticulitis can be safely performed. Conversion appears to be associated with complicated diverticulitis (fistula or abscess), which may be better approached by laparotomy. Short-term follow-up indicates that recurrence is rare and suggests that laparoscopic-assisted sigmoid colectomy achieves adequate resection. Laparoscopic-assisted sigmoid colectomy offers benefits of decreased ileus and length of stay and may represent the procedure of choice for elective resection for uncomplicated sigmoid diverticulitis.
Similar content being viewed by others

References
Mayo WJ. Acquired diverticulitis of the large intestine. Surg Gynecol Obstet 1907;5:8–15.
Standards Task Force, American Society of Colon and Rectal Surgeons. Practice parameters for sigmoid diverticulitis—supporting documentation. Dis Colon Rectum 1995;38:126–32.
Hackford AW, Schoetz DJ, Coller JA, Veidenheimer MC. Surgical management of complicated diverticulitis: the Lahey Clinic experience, 1967 to 1982. Dis Colon Rectum 1985;28:317–21.
Benn P, Wolff B, Ilstrup D. Level of anastomosis and recurrent diverticulitis. Am J Surg 1986;151:269–71.
Phillips EH, Franklin M, Carroll BT, Fallas M, Ramos R, Rosenthal D. Laparoscopic colectomy. Ann Surg 1992;216:703–7.
Wexner SD, Reissman P, Pfeifer J, Bernstein M, Geron N. Laparoscopic colorectal surgery: analysis of 140 cases. Surg Endosc 1996;10:133–6.
Bokey EL, Chapuis PH, Pheils MT. Elective resection for diverticular disease and carcinoma: comparison of post-operative morbidity and mortality. Dis Colon Rectum 1981;24:181–2.
Cooperman AM, Katz V, Zimmon D, Botero G. Laparoscopic colon resection: a case report. J Laparoendosc Surg 1991;1:221–4.
Lumley JW, Fielding GA, Rhodes M, Nathanson LK, Siu S, Stitz RW. Laparoscopic-assisted colorectal surgery: lessons learned from 240 consecutive cases. Dis Colon Rectum 1996;39:155–9.
Falk PM, Beart RW Jr, Wexner SD,et al. Laparoscopic colectomy: a critical appraisal. Dis Colon Rectum 1993;36:28–34.
Zucker KA, Pitcher DE, Martin DT, Ford RS. Laparoscopic assisted colon resection. Surg Endosc 1994;8:12–8.
Hoffman GC, Baker JW, Fitchett CW, Vansant JH. Laparoscopic-assisted colectomy: initial experience. Ann Surg 1994;219:732–43.
Stevenson A, Stitz R, Lumley J, Fielding G. Laparoscopically assisted anterior resection for diverticular disease. Ann Surg 1998;227:335–42.
Elashry OM, Nakada SY, Wolf JS Jr, Figenshau RS, McDougall EM, Clayman RV. Comparative clinical study of port-closure techniques following laparoscopic surgery. J Am Coll Surg 1996;183:335–44.
Wishner J, Baker J, Hoffman G,et al. Laparoscopic-assisted colectomy: the learning curve. Surg Endosc 1995;9:1179–83.
Sher M, Agachan F, Bortul M, Nogueras J, Weiss E, Wexner S. Laparoscopic surgery for diverticulitis. Surg Endosc 1997;11:264–7.
Liberman M, Phillips H, Carroll B, Fallas M, Rosenthal R. Laparoscopic colectomy vs. traditional colectomy for diverticulitis. Surg Endosc 1996;10:15–8.
Ou H. Laparoscopic-assisted mini laparotomy with colectomy. Dis Colon Rectum 1995;38:324–6.
Bruce CJ, Coller JA, Murray JJ, Schoetz DJ Jr, Roberts PL, Rusin LC. Laparoscopic resection for diverticular disease. Dis Colon Rectum 1996;39:S1–6.
Author information
Authors and Affiliations
Additional information
Read at The American Society of Colon and Rectal Surgeons' 100th Anniversary and Tripartite Meeting, Washington, D.C., May 1 to 6, 1999.
About this article
Cite this article
Vargas, H.D., Ramirez, R.T., Hoffman, G.C. et al. Defining the role of laparoscopic-assisted sigmoid colectomy for diverticulitis. Dis Colon Rectum 43, 1726–1731 (2000). https://doi.org/10.1007/BF02236858
Issue Date:
DOI: https://doi.org/10.1007/BF02236858