
Abstract
Acute appendicitis is a common surgical emergency in the paediatric population. Computed tomography (CT) has been shown to have high accuracy and low operator dependence in the diagnosis of appendicitis. However, with increased concerns regarding CT usage in children, ultrasound (US) is the imaging modality of choice in patients where appendicitis is suspected. This review describes and illustrates the step-wise graded-compression technique for the visualisation of the appendix, the normal and pathological appearances of the appendix, as well as the imaging characteristics of the common differentials.
Teaching points
• A step-wise technique improves the chances of visualisation of the appendix.
• There are often several causes for the non-visualisation of the appendix in children.
• A pathological appendix has characteristic US signs, with several secondary features also identified.
• There are multiple common differentials to consider in the paediatric patient.
Similar content being viewed by others



Introduction
In the paediatric population, acute appendicitis is a common condition that requires emergency abdominal surgery [1, 2]. It usually occurs in older children (ages 10–20) and is rare in children less than 2 years, but can occur at any age [3]. As the incidence of acute abdominal pain is common in children, differentiating acute appendicitis from non-surgical self-limiting illnesses is important.
Ultrasound (US) is often the diagnostic modality of choice in the diagnosis of appendicitis [4–6]. It lacks ionising radiation, allows dynamic visualisation of the abdominal organs and is of lower cost compared with computed tomography (CT). Many studies indicate a high sensitivity and specificity for US in the diagnosis of appendicitis. An 85–100 % sensitivity and 89–98 % specificity for US accuracy in appendicitis diagnosis have been documented [5, 7–12]. These studies tend to be reported by radiologists skilled in performing/interpreting paediatric sonography. However, some studies show lower rates due to the user-dependent nature of US [13, 14].
CT, on the other hand, has been shown to have a consistently high sensitivity and specificity in the diagnosis of appendicitis with reduced operator dependence [15, 16]. However, there is an increasing trend away from CT in the paediatric population because of the risk of radiation-induced cancer. Several risk models and studies have predicted higher risks for cancer in children exposed to CT compared with adults [17–19].
It is therefore important to know how to perform an adequate study using graded compression US, a well-established technique that maximises the chance of identifying the appendix [20].
Clinical features
Clinical features of appendicitis include right lower quadrant pain, pain migration, nausea or vomiting, anorexia, rebound tenderness, pyrexia and elevated white cell count [4]. However, not all children with appendicitis present with such classical symptoms and this can prolong the diagnosis [21]. Any delay in the surgical management can lead to complications as appendicitis usually does not resolve spontaneously [22]. Potential complications include perforation, peritonitis, abscess formation and death. Because of atypical presentations and the risk of potential complications, imaging is often requested. In children, this imaging technique is usually US.
Imaging technique
US allows the radiologist to clinically assess the patient, asking the child where they are sore, as well as other symptoms that have occurred. It is the imaging method of choice in the evaluation of suspected acute appendicitis due to the lack of non-ionising radiation and dynamic ability. A graded-compression US technique is performed using a high-resolution linear transducer. Graded-compression is the application of pressure through the transducer in order to displace and compress underlying bowel loops, thus allowing the visualisation of the appendix. A competent study should include the visualisation of the psoas muscle and iliac vessels.
Setting the scene: contact with the patient and parents
When meeting the paediatric patient for the first time, the patient should be asked where the point of maximum tenderness is located. The examination is explained to the patient. The patient is usually accompanied by a parent or guardian. In optimal conditions, the patient is fasted and has a full bladder to help in the exclusion of any ovarian or other pelvic pathology.
General abdominal US
US examinations of the liver, biliary tree, pancreas, both kidneys and spleen are performed with a 3.5–6 MHz curvilinear probe prior to graded US of the right iliac fossa and pelvis. This allows exclusion of any other possible cause for the acute abdominal pain. Free fluid is also looked for throughout the abdomen, as well as any echogenic omentum, large mass or collection, or pleural effusions at the lung bases. In girls, the assessment of the gynaecological structures, particularly the right ovary, should be performed at this stage.
Graded compression US
The scan is continued with a planar higher frequency probe, which allows higher resolution of more superficial structures. The frequency used depends on the size and age of the child (between 5 and 12 MHz).
-
Step 1:
Displacing small bowel loops out of the way
Normal bowel loops are displaced by gentle compression of the anterior abdominal wall using the US probe. These loops should be easily compressed and displaced away. The displacement of the bowel structures should allow the visualisation of the iliac vessels in the right iliac fossa as well as the psoas muscle. Two-plane scanning is performed (longitudinal and transverse).
-
Step 2:
Visualisation of the ascending colon and caecum
The ascending colon is visualised as a non-peristalsing structure containing gas and fluid in the right side of the abdomen. The probe is then moved inferiorly toward the caecum, using repeated compression and release to express gas and fluid from the bowel (Fig. 1a, b). The right psoas muscle should also be visualised (Fig. 2). The adjacent terminal ileum should be identified as a compressible structure that is undergoing peristalsis.
Fig. 1 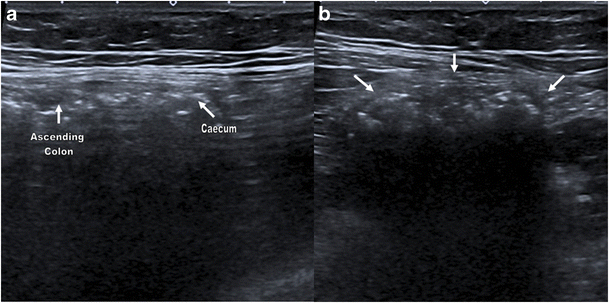
Longitudinal (a) and transverse (b) views using high frequency linear-array probe showing the caecum (small white arrows in b) and ascending colon in a 15-year-old girl
Fig. 2 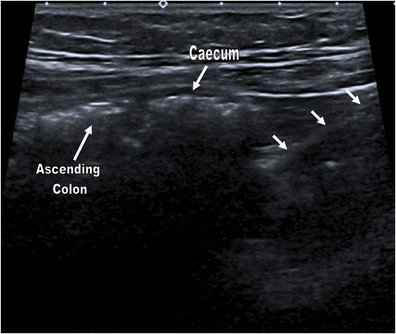
Longitudinal image showing the caecum and ascending colon, as well as the adjacent psoas muscle posteriorly (small white arrows) in a 15-year-old girl
-
Step 3:
Identification of the appendix
Once the caecum has been seen, the appendix should be visualised arising from it, separate to the terminal ileum (Fig. 3). The appendix should be followed along its whole length. A normal appendix should measure 6 mm or less in diameter from outside wall to outside wall. It should have a thin wall (less than 3 mm), be empty or gas/faecal-filled and compressible, and there should be no evidence of hypervascularisation [23–26].
Fig. 3 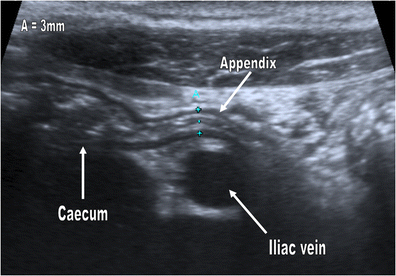
A normal appendix is seen draped over the iliac vessels in a 10-year-old girl. This is thin-walled, measuring less than 6 mm in diameter (A width of 3 mm). The caecum can be seen in continuity with the appendix superior to it
-
Step 4:
Assessment for features of acute appendicitis
An abnormal appendix can have any of the following characteristics which should be actively considered:
-
Compressibility: in acute appendicitis, the appendix is non-compressible [24]. One caveat here is perforation when the appendix can become compressible.
-
Maximum diameter: a maximum diameter of greater than 6 mm is considered abnormal (Figs. 4 and 5) [5, 24, 25].
-
Wall thickness: a single wall thickness of 3 mm or more is considered abnormal (Fig. 6) [24, 27].
-
Target sign appearance: this is caused by a fluid-filled centre (hypoechoic centre), surrounded by a hyperechoic ring (mucosa/submucosa) which is surrounded by a hypoechic muscularis layer giving a target sign on axial imaging (Fig. 7a, b) [15, 28].
-
The presence of an appendicolith (this will appear as an echogenic focus with posterior acoustic shadowing) (Fig. 8a, b) [15, 28].
-
Vascularity: peripheral appendiceal wall hyperaemia is seen in the early stages of acute appendicitis (Fig. 9a, b); this may not be seen with progression to necrosis [15, 29].
Fig. 4 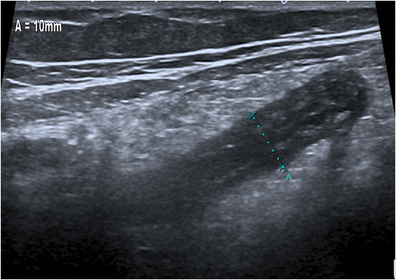
Longitudinal view of a thickened, oedematous appendix measuring 10 mm in diameter with surrounding increased echogenic omentum in an 8-year-old boy with confirmed appendicitis. Absent intraluminal gas is noted
Fig. 5 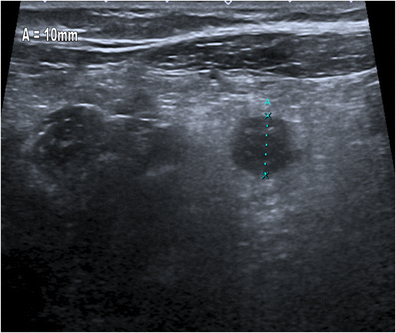
Transverse view of a thickened, oedematous appendix measuring 10 mm in diameter in an 8-year-old boy with confirmed appendicitis. Again, surrounding omentum of increased echogenicity is noted
Fig. 6 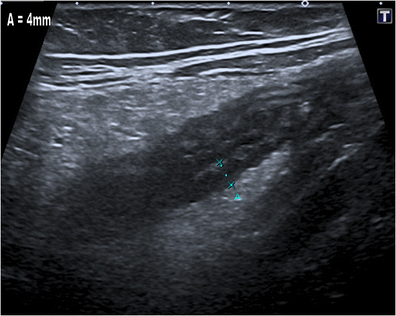
The wall of this oedematous appendix measures 4 mm in an 8-year-old boy with confirmed appendicitis. Increased echogenic omentum is seen adjacent to the appendix
Fig. 7 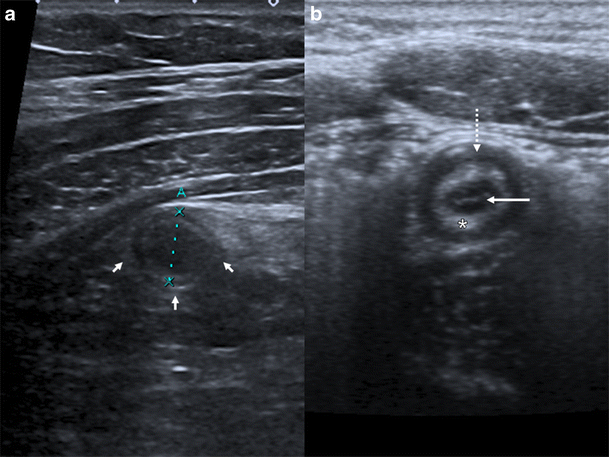
a A transverse view of an inflamed appendix in a 15-year-girl, showing the target sign appearance. b Similar appearances in an 11-year-old boy. This target sign comprises a hypoechoic fluid-filled centre (white arrow), inner hyperechoic mucosal/submucosal ring (white asterisk), and outer hypoechoic ring (dashed white arrow)
Fig. 8 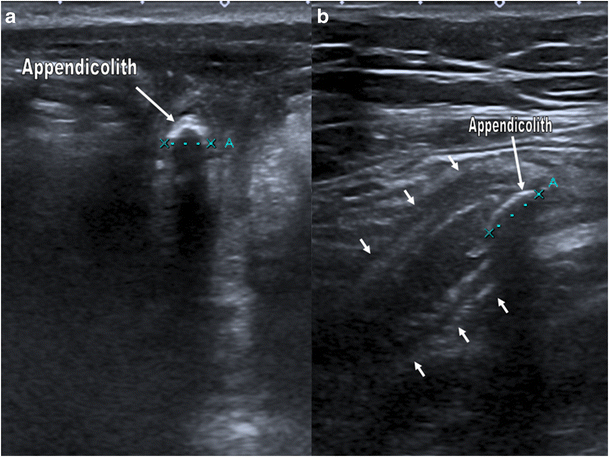
Appendicoliths (labelled) causing posterior acoustic shadowing in two patients, a 15-year-old girl (a) and a 10-year-old boy (b). The thickened, fluid-filled appendix is labelled in b (small white arrows)
Fig. 9 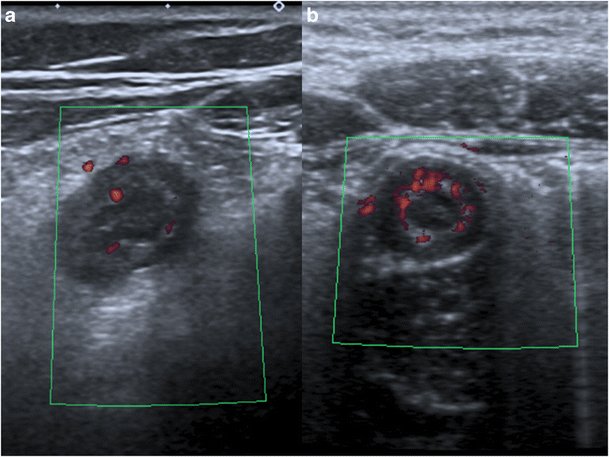
a Increased Doppler signal in a thickened, oedematous appendix in an 8 year-old-boy. b Similar appearances noted in a 10-year-old girl. The increased Doppler signal indicates hyperaemia
Secondary features can be observed around the inflamed appendix; these should be actively sought:
-
Free fluid or abscess in the periappendiceal region (Fig. 10) [6, 15, 28].
-
Increased echogenicity of the adjacent periappendiceal fat (Fig. 11) [6, 15, 28].
-
Thickening and hyperechogenicity of the overlying peritoneum (Fig. 13).
-
Dilated hyperactive small bowel from secondary small bowel obstruction (Fig. 14).
-
Focal apical caecal pole thickening or thickening of the adjacent small bowel can be seen as a secondary response [6, 30].
Fig. 10 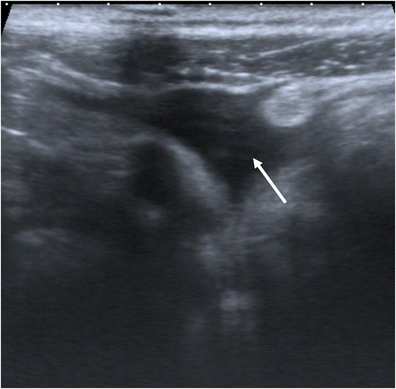
Small pocket of free fluid in the region of the appendix (white arrow) in a 10-year-old girl with confirmed appendicitis
Fig. 11 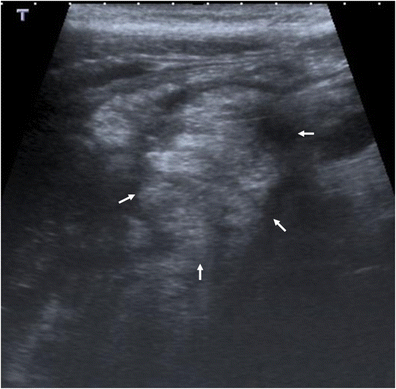
Omental fat with increased echogenicity with a mass-like appearance (small white arrows) in a 12-year-old boy with confirmed appendicitis
Fig. 12 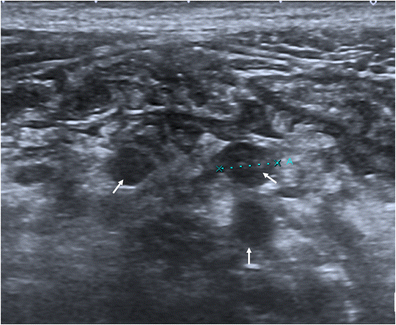
Multiple lymph nodes (arrows) in the mesentery of the periappendiceal region in an 8-year-old girl with confirmed appendicitis
Fig. 13 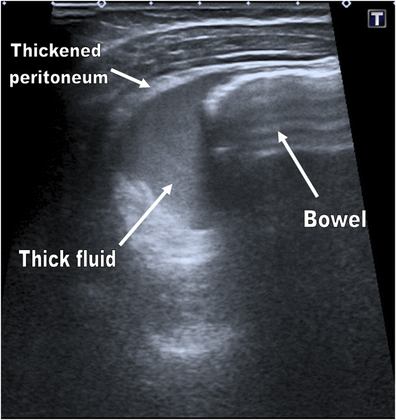
Increased echogenic free fluid in the right iliac fossa (indicating pus) with adjacent thickening of the peritoneum in a 2-year-old girl with confirmed appendicitis
Fig. 14 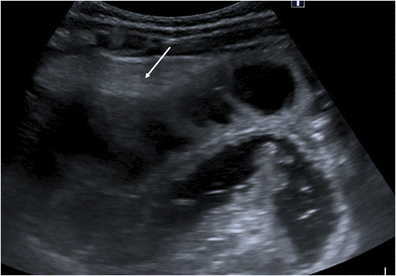
Loops of dilated, fluid-filled small bowel in a 2-year-old girl with confirmed appendicitis. Echogenic free fluid is seen adjacent to the bowel indicating pus (white arrow)
-














It is not uncommon that the appendix cannot be identified. There are varying rates quoted in the literature for the appendix being seen, between 24.4 % and 69.3 % [6, 13, 23]. In this situation, it is important to actively assess for the secondary features often seen which may help direct further management. Repeating the examination after a few hours has been shown to significantly increase the sensitivity of US [31].
Perforation is a well-documented complication of appendicitis [32]. US features suggesting this include loss of the echogenic submucosal layer or a periappendiceal fluid collection [28]. The periappendiceal fluid collections may be small or quite large (Fig. 15). There may also be thickening of the adjacent peritoneum, which is easier to see if there is free fluid. Cases of perforation may show mixed echogenic fluid in the right iliac fossa, indicating the presence of pus or faecal material (Figs. 13 and 14). Untreated, a walled-off appendiceal perforation can progress to form an inflammatory mass in the right iliac fossa, ranging from phlegmon to abscess (Fig. 16) [33]. This is seen as a mass-like lesion with areas of both increased echogenicity (representing inflamed omentum) and decreased echogenicity. The inflammatory mass will cause a pressure effect on the adjacent structures. It can be difficult to identify the appendix in the presence of such a mass.

Large collection (small white arrows) in a 4-year-old boy with a perforation secondary to appendicitis

Right iliac fossa inflammatory mass in a 14-year-old boy with proven appendicitis
Causes of inadequate visualisation of the appendix and possible solutions
There are a few common causes for the non-visualisation of the appendix.
Patient symptoms: pain and abdominal guarding
Pain can often limit the extent of compression of the abdominal wall, thus limiting the ability to displace the overlying bowel loops. Pain relief prior to the examination can help. Examining the rest of the abdomen first with a curvilinear probe prior to the graded compression of the right iliac fossa can help relax the patient. Gentle compression should be used initially to gauge the patient’s symptoms.
Appendix position
The position of the appendix can also lead to difficulty in its visualisation. A retrocaecal appendix can occur in 20.1–65 % of patients [34, 35] and will be difficult to visualise on US [6, 24, 30]. The appendix may be also anatomically abnormally positioned, such as abnormalities of situs, when the caecum is mobile or subhepatic, or in cases of congenital malrotation [36–38]. Rarely, it may also be located away from the right iliac fossa due to very long length. The average appendix measures between 8 and 10 cm in length, but can measure more than 20 cm [39, 40]. The use of the lower frequency 3.5 MHz curvilinear probe may reveal free fluid or omental reaction away from the right iliac fossa, giving a clue about an anatomically abnormal appendix location.
Various operator-dependent techniques have been shown to improve the visualisation of the appendix [41, 42]. A posterior manual compression technique uses the sonographer’s left hand to compress the posterior aspect of the colon, increasing the chance of identifying the appendix [41]. The four fingers of the left hand are used to compress the dorsal surface of the patient, on the opposite side of the right lower quadrant. Scanning the patient with the right or left side down can help move bowel loops out of the way, and may help find the appendix (Fig. 17). A left oblique lateral decubitus position displaces the caecum and terminal ileum medially, aiding the visualisation of a retrocaecal appendix [42]. Getting the patient to empty their bladder has been shown to help find the normal appendix [24].

Fluid-filled dilated appendix in a retrocaecal position (small white arrows) in a 15-year-old girl. Note is made of an appendicolith within the appendix
State of the pathological process
Appendiceal obstruction leading to appendicitis can occur anywhere along the appendix [15, 24]. Therefore, if only a small part of the appendix is involved, the inflammation may be limited to the tip [43]. Incomplete visualisation of the whole length of the appendix due to position can lead to a false-negative result if only the tip of the appendix is involved.
In an advanced stage of appendicitis, the appendix can be engulfed within an inflammatory mass and identification of the appendix itself may be impossible. This situation is also identified at surgery [44].
Differential diagnosis
Terminal ileitis
This is the inflammation of the terminal ileum and is most commonly caused by Crohn’s disease [45]. While symptoms of abdominal pain and diarrhoea can overlap with acute appendicitis, the symptoms have often been there for a longer period. Signs on US include a thickened terminal ileal wall (between 1.5 and 3 mm), luminal narrowing and hyperaemia [46] (Figs. 18 and 19). The appendix can often be involved in patients with Crohn’s disease [47]. The most reliable way of distinguishing between appendiceal involvement in Crohn’s disease and acute appendicitis is to use a terminal ileal thickness of more than 5 mm and visible flow on colour Doppler in the ileum [47]. Terminal ileitis can also be caused by infections (Yersinia spp., Salmonella spp., tuberculosis, typhilitis, Histoplasma capsulatum) [45, 48]. Similar features to Crohn’s disease are identified, and long segments can be involved. Stool cultures help yield a diagnosis. Other causes of terminal ileitis in children include backwash ileitis in ulcerative colitis, lymphoid hyperplasia and Henoch-Schonlein purpura.

Longitudinal view of the terminal ileum in a 10-year-old boy. The terminal ileum is thickened with luminal narrowing. The patient was subsequently confirmed to have Crohn’s disease

Transverse view of a thickened terminal ileum in a 10-year-old boy. Again, luminal narrowing is seen with surrounding increased echogenic omentum. The patient was subsequently confirmed to have Crohn’s disease
Omental infarction
This is a rare cause of acute abdominal pain in children. It is a benign self-limiting process that should be managed conservatively. It is more common in boys and in those who are obese [49, 50]. Symptoms are often acute or subacute in nature and often right-sided. The patient is often apyrexic and does not have symptoms of diarrhoea, vomiting or anorexia [51]. On US, there is evidence of an ovoid soft-tissue hyperechoic mass located between the anterior abdominal wall and the colon, which is non-compressible and painful [50]. If the normal appendix is not visualised, this soft-tissue mass can be mistaken for acute appendicitis.
Ovarian pathology
The most common differential diagnosis in older girls is ovarian pathology and the normal ovaries need to be imaged. This is aided by a full bladder. Possible acute pathologies include ovarian torsion and haemorrhagic ovarian cyst. Features of an ovarian torsion include unilateral ovarian enlargement (>4 cm), a heterogenous appearance (secondary to haemorrhage), multiple peripherally located cysts (string of pearl sign), an absence or lack of arterial flow and twisted vascular pedicle [52]. A haemorrhagic cyst is usually 3–3.5 cm in size, thin walled and has a lace-like pattern of internal echoes (Fig. 20a, b). Some circumferential Doppler flow can be seen in the wall, but no internal flow is identified. The blood products may separate into fluid-fluid or fluid-debris levels [53, 54].

a Haemorrhagic cyst in a 12-year-old girl presenting with right iliac fossa pain. A large, thin-walled right adnexal cyst (white arrows) is seen with a lace-like pattern of internal echoes. b Haemorrhagic cyst in a 13-year-old girl presenting with lower abdominal pain. Similar appearances to a are identified (white arrows), with a small amount of adjacent free fluid in the right adnexal (black arrow)
Mesenteric adenitis
Mesenteric adenitis is a self-limiting condition that presents in a similar way to acute appendicitis with pyrexia and right lower quadrant abdominal pain. US reveals multiple (usually five or more) lymph nodes that are clustered together (Fig. 21). These measure at least 5 mm in short-axis diameter and are often hyperaemic on Doppler examination [55]. Nodal size and number is often greater in mesenteric adenitis compared with appendicitis. Other findings include increased echogenicity and Doppler signal of the surrounding mesenteric fat, increased peristalsis of the adjacent bowel and free fluid. Mesenteric adenitis should be diagnosed if nodes reaching the criteria are seen in the presence of a normal appearing appendix

Mesenteric adenitis. Multiple enlarged lymph nodes in the right iliac fossa of a 7-year-old girl. Adjacent mesenteric increased echogenicity and a small pocket of free fluid (white arrow) are noted. A normal appendix was identified
Meckel’s diverticulum
Caused by failure of the omphalomesenteric-vitelline duct to regress, a Meckel’s diverticulum is found in 1–4 % of the population [56]. The US appearances of an inflamed Meckel’s diverticulum may mimic acute appendicitis [57]. On US examination, it may appear as a non-compressible, blind-ending, hypoechoic structure in the right-iliac fossa [57]. It may also appear as a cyst-like mass with a thick, irregular internal wall with an external hypoechoic rim (corresponding to the muscle layer) and an internal hyperechoic line corresponding to the submucosal and mucosal layers [58]. Doppler US can reveal hypervascularisation [57].
Indeterminate challenging cases
If the diagnosis remains unclear there are many further options. As described already, repeating the US has been shown to increase the diagnostic accuracy in patients with suspected appendicitis [31]. While CT seems to be the next choice in the difficult patient in many centres worldwide, it is increasingly difficult to justify due to the concerns over the effects of ionising radiation [17–19]. Magnetic resonance imaging (MRI) is beginning to be used in the evaluation of the paediatric patient with suspected appendicitis. Several recent studies have shown a sensitivity and specificity comparable to CT, with sensitivities between 97.6 % and 100 %, and specificities between 96 % and 99 % [59–61]. The use of MRI thus avoids the concerning effects of ionising radiation. While scoring systems such as the Alvarado score are available to stratify the risk of the presenting patient, they have been shown to be inadequate in the prediction of appendicitis on their own [62, 63]. However, when combined with US, such scores have been shown to be useful in indeterminate cases [64].
Conclusions
US examination of a paediatric patient where appendicitis is suspected includes examination of the abdominal organs with a curvilinear probe, followed by graded compression of the right colon and appendix using a linear-array probe. This should be performed in a systematic way to maximise the chance of identifying the appendix and the features that would suggest appendicitis.
References
Scholer SJ, Pituch K, Orr DP, Dittus RS (1996) Clinical outcomes of children with acute abdominal pain. Pediatrics 98:680–685
Addiss DG, Shaffer N, Fowler BS, Tauxe RV (1990) The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol 132:910–925
Humes DJ, Simpson J (2006) Acute appendicitis. BMJ 333:530–534
Acheson J, Banerjee J (2010) Management of suspected appendicitis in children. Arch Dis Child Educ Pract Ed 95:9–13
Vignault F, Filiatrault D, Brandt ML, Garel L, Grignon A, Ouimet A (1990) Acute appendicitis in children: evaluation with US. Radiology 176:501–504
Ang A, Chong NK, Daneman A (2001) Pediatric appendicitis in “real-time”: the value of sonography in diagnosis and treatment. Pediatr Emerg Care 17:334–340
Sivit CJ, Newman KD, Boenning DA, Nussbaum-Blask AR, Bulas DI, Bond SJ, Attorri R, Rebolo LC, Brown-Jones C, Garin DB (1992) Appendicitis: usefulness of US in diagnosis in pediatric population. Radiology 185:549–552
Hahn HB, Hoepner FU, Kalle T, MacDonald EB, Prantl F, Spitzer IM, Faerber DR (1999) Sonography of acute appendicitis in children: 7 years experience. Pediatr Radiol 28:147–151
Crady SK, Jones JS, Wyn T, Luttenton CR (1993) Clinical validity of ultrasound in children with suspected appendicitis. Ann Emerg Med 22:1125–1129
Rubin SZ, Martin DJ (1990) Ultrasonography in the management of possible appendicitis in childhood. J Pediatr Surg 25:737–740
Lessin MS, Chan M, Catallozzi M, Gilchrist MF, Richards C, Manera L, Wallach MT, Luks FI (1999) Selective use of ultrasonography for acute appendicitis in children. Am J Surg 177:193–196
Orr RK, Porter D, Hartman D (1995) Ultrasonography to evaluate adults for appendicitis: decision making based on meta-analysis and probabilistic reasoning. Acad Emerg Med 2:644–650
Trout AT, Sanchez R, Ladino-Torres MF, Pai DR, Strouse PJ (2012) A critical evaluation of US for the diagnosis of pediatric acute appendicitis in a real-life setting: how can we improve the diagnostic value of sonography? Pediatr Radiol 42:813–823
Pohl D, Golub R, Schwartz GE, Stein HD (1998) Appendiceal ultrasonography performed by nonradiologists: does it help in the diagnostic process? J Ultrasound Med 17:217–221
Sivit CJ, Siegel MJ, Applegate KE, Newman KD (2001) When appendicitis is suspected in children. Radiographics 21:247–262
Rao PM, Rhea JT, Novelline RA, McCabe CJ, Lawrason JN, Berger DL, Sacknoff R (1997) Helical CT technique for the diagnosis of appendicitis: prospective evaluation of a focused appendix CT examination. Radiology 202:139–144
Brenner D, Elliston C, Hall E, Berdon W (2001) Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR Am J Roentgenol 176:289–296
Krille L, Zeeb H, Jahnen A, Mildenberger P, Seidenbusch M, Schneider K, Weisser G, Hammer G, Scholz P, Blettner M (2012) Computed tomographies and cancer risk in children: a literature overview of CT practices, risk estimations and an epidemiologic cohort study proposal. Radiat Environ Biophys 51:103–111
Mathews JD, Forsythe AV, Brady Z, Butler MW, Goergen SK, Byrnes GB, Giles GG, Wallace AB, Anderson PR, Guiver TA, McGale P, Cain TM, Dowty JG, Bickerstaffe AC, Darby SC (2013) Cancer risk in 680 000 people exposed to computed tomography scans in childhood or adolescence: data linkage study of 11 million Australians. BMJ 346:f2360
Puylaert JB (1986) Acute appendicitis: US evaluation using graded compression. Radiology 158:355–360
Reynolds SL (1993) Missed appendicitis in a pediatric emergency department. Pediatr Emerg Care 9:1–3
Brender JD, Marcuse EK, Koepsell TD, Hatch EI (1985) Childhood appendicitis: factors associated with perforation. Pediatrics 76:301–306
Ozel A, Orhan UP, Akdana B, Disli C, Erturk SM, Basak M, Karpat Z (2011) Sonographic appearance of the normal appendix in children. J Clin Ultrasound 39:183–186
Rioux M (1992) Sonographic detection of the normal and abnormal appendix. AJR Am J Roentgenol 158:773–778
Goldin AB, Khanna P, Thapa M, McBroom JA, Garrison MM, Parisi MT (2011) Revised ultrasound criteria for appendicitis in children improve diagnositic accuracy. Pediatr Radiol 41:993–999
Rettenbacher T, Hollerweger A, Macheiner P, Rettenbacher L, Frass R, Schneider B, Gritzmann N (2000) Presence or absence of gas in the appendix: additional criteria to rule out or confirm acute appendicitis—evaluation with US. Radiology 214:183–187
Simonovsky V (2002) Normal appendix: is there any significant difference in the maximal mural thickness at US between pediatric and adult populations? Radiology 224:333–337
Quillin SP, Siegel MJ, Coffin CM (1992) Acute appendicitis in children: value of sonography in detecting perforation. AJR Am J Roentgenol 159:1265–1268
Quillin SP, Siegel MJ (1994) Appendicitis: efficacy of color Doppler sonography. Radiology 191:557–560
Birnbaum BA, Wilson SR (2000) Appendicitis at the millennium. Radiology 215:337–348
Schuh S, Man C, Cheng A, Murphy A, Mohanta A, Moineddin R, Tomlinson G, Langer JC, Doria AS (2011) Predictors of non-diagnostic ultrasound scanning in children with suspected appendicitis. J Pediatr 158:112–118
Livingston EH, Woodward WA, Sarosi GA, Haley RW (2007) Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management. Ann Surg 245:886–892
Nitecki S, Assalia A, Schein M (1993) Contemporary management of the appendiceal mass. Br J Surg 80:18–20
Ahmed I, Asgeirsson KS, Beckingham IJ, Lobo DN (2007) The position of the vermiform appendix at laparoscopy. Surg Radiol Anat 29:165–168
Oruc M, Muminagic S, Denjalic A, Tandir S, Hodzic H (2012) Retrocaecal appendix position-findings during the classic appendectomy. Med Arh 66:190–193
Oh JS, Kim KW, Cho HJ (2012) Left-sided appendicitis in a patient with situs inversus totalis. J Korean Surg Soc 83:175–178
Galván-Montaño A, Flores-Nava G, Suárez-Roa Mde L, Salazar-Herrera MC, Lavalle-Villalobos A (2010) Subhepatic appendicitis with subdiaphragmatic abscess in a pediatric patient without intestinal malrotation: case report. Cir Cir 78:79–81
Tawk CM, Zgheib RR, Mehanna S (2012) Unusual case of acute appendicitis with left upper quadrant abdominal pain. Int J Surg Case Rep 3:399–401
Collins DC (1932) The length and position of the vermiform appendix: a study of 4,680 specimens. Ann Surg 96(6):1044–1048
Park NH, Oh HE, Park HJ, Park JY (2011) Ultrasonography of normal and abnormal appendix in children. World J Radiol 3(4):85–91
Lee JH, Jeong YK, Hwang JC, Ham SY, Yang SO (2002) Graded compression sonography with adjuvant use of a posterior manual compression technique in the sonographic diagnosis of acute appendicitis. AJR Am J Roentgenol 178:863–868
Lee JH, Jeong YK, Park KB, Park JK, Jeong AK, Hwang JC (2005) Operator-dependent techniques for graded compression sonography to detect the appendix and diagnose acute appendicitis. AJR Am J Roentgenol 184:91–97
Mazeh H, Epelboym I, Reinherz J, Greenstein AJ, Divino CM (2009) Tip appendicitis: clinical implications and management. Am J Surg 197:11–215
Price MR, Haase GM, Sartorelli KH, Meagher DP Jr (1996) Recurrent appendicitis after initial conservative management of appendiceal abscess. J Pediatr Surg 31:291–294
DiLauro S, Crum-Cianflone NF (2010) Ileitis: when it is not Crohn’s disease. Curr Gastroenterol Rep 12:249–258
Alison M, Kheniche A, Azoulay R, Roche S, Sebag G, Belarbi N (2007) Ultrasonography of Crohn disease in children. Pediatr Radiol 37:1071–1082
Ripolles T, Martinez MJ, Morote V, Errando J (2006) Appendiceal involvement in Crohn’s disease: gray-scale sonography and color Doppler flow features. AJR Am J Roentgenol 186:1071–1078
Ebel KD, Blickman H, Willich E, Richter E (1998) Differential diagnosis in pediatric radiology. Thieme, New York, pp 250–251
Sakellaris G, Stathopoulos E, Kafousi M, Arbiros J, Bitsori M, Charissis G (2004) Primary idiopathic segmental infarction of the greater omentum: two cases of acute abdomen in childhood. J Pediatr Surg 39:1264–1266
Grattan-Smith JD, Blews DE, Brand T (2002) Omental infarction in pediatric patients: sonographic and CT findings. AJR Am J Roentgenol 178:1537–1539
Coulier B (2006) Segmental omental infarction in childhood: a typical case diagnosed by CT allowing successful conservative treatment. Pediatr Radiol 36:141–143
Chang HC, Bhatt S, Dogra VS (2008) Pearls and pitfalls in diagnosis of ovarian torsion. Radiographics 28:1355–1368
Levine D, Brown DL, Andreotti RF, Benacerraf B, Benson CB, Brewster WR, Coleman B, DePriest P, Doubilet PM, Goldstein SR, Hamper UM, Hecht JL, Horrow M, Hur HC, Marnach M, Patel MD, Platt LD, Puscheck E, Smith-Bindman R (2010) Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound consensus conference statement. Radiology 256:943–954
Jain KA (2002) Sonographic spectrum of hemorrhagic ovarian cysts. J Ultrasound Med 21:879–886
Simanovsky N, Hiller N (2007) Importance of sonographic detection of enlarged abdominal lymph nodes in children. J Ultrasound Med 26:581–584
Thurley PD, Halliday KE, Somers JM, Al-Daraji WI, Ilyas M, Broderick NJ (2009) Radiological features of Meckel’s diverticulum and its complications. Clin Radiol 64:109–118
Baldisserotto M, Maffazzoni DR, Dora MD (2003) Sonographic findings of Meckel’s diverticulitis in children. AJR Am J Roentgenol 180:425–428
Daneman A, Lobo E, Alton DJ, Shuckett B (1998) The value of sonography, CT and air enema for detection of complicated Meckel diverticulum in children with nonspecific clinical presentation. Pediatr Radiol 28:928–932
Moore MM, Gustas CN, Choudhary AK, Methratta ST, Hulse MA, Geeting G, Eggli KD, Boal DK (2012) MRI for clinically suspected pediatric appendicitis: an implemented program. Pediatr Radiol 42:1056–1063
Johnson AK, Filippi CG, Andrews T, Higgins T, Tam J, Keating D, Ashikaga T, Braff SP, Gallant J (2012) Ultrafast 3-T MRI in the evaluation of children with acute lower abdominal pain for the detection of appendicitis. AJR Am J Roentgenol 198:1424–1430
Herliczek TW, Swenson DW, Mayo-Smith WW (2013) Utility of MRI after inconclusive ultrasound in pediatric patients with suspected appendicitis: retrospective review of 60 consecutive patients. AJR Am J Roentgenol 200:969–973
Mandeville K, Pottker T, Bulloch B, Liu J (2011) Using appendicitis scores in the pediatric ED. Am J Emerg Med 29:972–977
Kulik DM, Uleryk EM, Maguire JL (2013) Does this child have appendicitis? A systematic review of clinical prediction rules for children with acute abdominal pain. J Clin Epidemiol 66:95–104
Escribá A, Gamell AM, Fernández Y, Quintillá JM, Cubells CL (2011) Prospective validation of two systems of classification for the diagnosis of acute appendicitis. Pediatr Emerg Care 27:165–169
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Quigley, A.J., Stafrace, S. Ultrasound assessment of acute appendicitis in paediatric patients: methodology and pictorial overview of findings seen. Insights Imaging 4, 741–751 (2013). https://doi.org/10.1007/s13244-013-0275-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13244-013-0275-3