
Abstract
Background
Knowledge of types and co-morbidities of disorders seen in any facility is useful for clinical practice and planning for services.
Aim
To study the pattern of co-morbidities of and correlations between psychiatric disorders in in-patients of Mathari Hospital, the premier psychiatric hospital in Kenya.
Study Design
Cross-sectional.
Methods
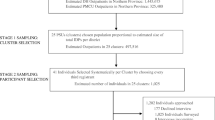
All the patients who were admitted at Mathari Hospital in June 2004 and were well enough to participate in the study were approached for informed consent. Trained psychiatric charge nurses interviewed them using the Structured Clinical Interview for DSM-IV Axis I disorders Clinical Version (SCID-I). Information on their socio-demographic profiles and hospital diagnoses was extracted from their clinical notes using a structured format.
Results
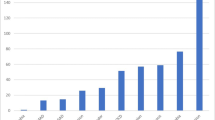
Six hundred and ninety-one patients participated in the study. Sixty-three percent were male. More than three quarters (78%) of the patients were aged between 21 and 45 years. More than half (59.5%) of the males and slightly less than half (49.4%) of the females were single. All the patients were predominantly of the Christian faith. Over 85% were dependants of another family member and the remainder were heads of households who supported their own families. Schizophrenia, bipolar I disorder, psychosis, substance use disorder and schizo-affective disorder were the most common hospital and differential diagnoses. Of the anxiety disorders, only three patients were under treatment for post-traumatic stress disorder (PTSD). Nearly a quarter (24.6%) of the patients were currently admitted for a similar previous diagnosis. Schizophrenia was the most frequent DSM-IV (Diagnostic and Statistical Manual of Mental Disorders—fourth edition) diagnosis (51%), followed by bipolar I disorder (42.3%), substance use disorder (34.4%) and major depressive illness (24.6%). Suicidal features were common in the depressive group, with 14.7% of this group reporting a suicidal attempt. All DSM-IV anxiety disorders, including obsessive–compulsive disorders, were highly prevalent although, with the exception of three cases of PTSD, none of these anxiety disorders were diagnosed clinically. Traumatic events were reported in 33.3% of the patients. These were multiple and mainly violent events. Despite the multiplicity of these events, only 7.4% of the patients had a PTSD diagnosis in a previous admission while 4% were currently diagnosed with PTSD. The number of DSM-IV diagnoses was more than the total number of patients, suggesting co-morbidity, which was confirmed by significant 2-tailed correlation tests.
Conclusion
DSM-IV substance use disorders, major psychiatric disorders and anxiety disorders were prevalent and co-morbid. However, anxiety disorders were hardly diagnosed and therefore not managed. Suicidal symptoms were common. These results call for more inclusive clinical diagnostic practice. Standardized clinical practice using a diagnostic tool on routine basis will go a long way in ensuring that no DSM-IV diagnosis is missed. This will improve clinical management of patients and documentation.
Similar content being viewed by others

References
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, 4th edn. APA, Washington DC
Baumeister H, Härter M (2007) Prevalence of mental disorders based on general population surveys. Soc Psychiatry Psychiatr Epidemiol 42(7):537–546
Bruffaerts R, Sabbe M, Demyttenaere K (2004) Attenders of a university hospital psychiatric emergency service in Belgium. Soc Psychiatry Psychiatr Epidemiol 39(2):146–153
Cwikel J, Zilber N, Feinson M, Lerner Y (2008) Prevalence and risk factors of threshold and sub-threshold psychiatric disorders in primary care. Soc Psychiatry Psychiatr Epidemiol 43(3):184–191
First MB, Spitzer RL, William JDW (1996) Structured clinical interview for DSM-IV axis I disorders clinical version (SCID-I CV). American Psychiatric Press Inc., Washington DC
Gorman LL, O’Hara MW, Figueiredo B, Hayes S, Jacquemain F, Kammerer M, Klier CM, Rosi S, Seneviratne G, Sutter-Dallay A-L, the TCS-PND Group (2004) Adaptation of the structured clinical interview for DSM-IV disorders for assessing depression in women during pregnancy and post-partum across countries and cultures. Br J Psychiat 184(suppl 46):s17–s23
Klein DN, Riso LP (1993) Psychiatric disorders: problems of boundaries and comorbidity. In: Costello CG (ed) Basic issues in psychopathology. Guilford, New York, pp 19–66
Muhwezi WW, Ågren H, Musisi S (2007) Detection of major depression in Ugandan primary health care settings using simple questions from a subjective well-being (SWB) subscale. Soc Psychiatry Psychiatr Epidemiol 42:61–69
Myers JK, Weissman MM, Tischler GL, Holzer CE 3rd, Leaf PJ, Orvaschel H, Anthony JC, Boyd JH, Burke JD Jr, Kramer M, et al (1984) Six months prevalence of psychiatric disorders in three communities 1980–1982. Arch Gen Psychiatr 41: 959–967
Ndetei DM, Ongecha FA, Mutiso V, Kuria M, Khasakhala LI, Kokonya DA (2007) The challenges of human resources in mental health in Kenya. S Afr Psychiatry Rev 10:33–36
Osman AA, Alkateeb SO, Ali AS (1993) The pattern of admission to Jeddah Psychiatric Hospital. Saudi Med J 14:334–339
Pincus HA, Tew JD Jr, First MB (2004) Psychiatric comorbidity: is more less? World Psychiatry 3(1):18–23
Stanley B, Gibson AT (1985) The prevalence of chronic psychiatric morbidity: a community sample. Br J Psychiat 146:372–376
Stromgren KH, Nielsen JA, Sartorius N (1989) Changes in frequency of mental disorder over time (Results of repeated surveys of mental disorders in general population). Acta Psychiatr Scand 79(suppl 348):167–168
Acknowledgements
The Africa Mental Health Foundation (AMHF) provided administrative support for this study. The authors would like to thank Grace Mutevu of AMHF for analysis of the data and for preparation of the paper, and Patricia Wekulo for editing the paper.
Declaration of interest None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ndetei, D.M., Khasakhala, L., Maru, H. et al. Clinical epidemiology in patients admitted at Mathari Psychiatric Hospital, Nairobi, Kenya. Soc Psychiat Epidemiol 43, 736–742 (2008). https://doi.org/10.1007/s00127-008-0360-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-008-0360-y