
Abstract
Background
Follow-up is critical to the success of laparoscopic adjustable gastric banding (LAGB). Few data guide this and expected norms of satiety, adverse symptoms, and outcomes have not been defined.
Methods
Consecutive patients, who underwent LAGB, were evaluated using a newly developed instrument that assessed satiety, adverse upper gastrointestinal (dysphagia, reflux, and epigastric pain), and outcomes (overall satisfaction, weight loss, and quality of life (SF-36)).
Results
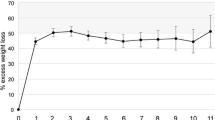
Three hundred twenty-three of 408 patients responded (80%; mean age 44.4 ± 11.8 years, 56 males). Excess weight loss was 52%. Satiety was greater at breakfast compared to lunch (5.3 ± 1.9 vs. 4.1 ± 1.7, p < 0.005) or dinner (3.8 ± 1.8, p < 0.005). The satisfaction score was 8.3 ± 2.1 out of 10, and 91% would have the surgery again. Quality of life was less than community norms, except in physical functioning (83.4 ± 20.5 vs. 84.7 ± 22.0, p = 0.25) and bodily pain (78.4 ± 15.2 vs. 75.9 ± 25.3, p = 0.004). Inability to consume certain foods was cited as the biggest problem by 66% of respondents. The dysphagia score was 19.9 ± 8.7; softer foods were tolerated, although difficulty was noted with firmer foods. The reflux score was 8.7 ± 9.8 and regurgitation occurred a mean of once per week. Weight loss and the mental component score were the only predictors of overall satisfaction (r 2 = 0.46, p = 0.01).
Conclusions
Patients are highly satisfied with the outcome of LAGB and achieve substantial weight after 3 years. Expected ranges of satiety, adverse symptoms, and outcomes have been defined. The most troublesome symptom is the inability to consume certain foods. Weight loss predicted overall satisfaction, regardless of adverse symptoms.





Similar content being viewed by others


References
O'Brien PE, Brown WA, Smith A, et al. Prospective study of a laparoscopically placed, adjustable gastric band in the treatment of morbid obesity. Br J Surg. 1999;86:113–8.
O'Brien PE, McPhail T, Chaston TB, et al. Systematic review of medium-term weight loss after bariatric operations. Obes Surg. 2006;16:1032–40.
Dixon JB, O'Brien PE, Playfair J, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA. 2008;299:316–23.
Dixon JB, Dixon ME, O'Brien PE. Quality of life after lap-band placement: influence of time, weight loss, and comorbidities. Obes Res. 2001;9:713–21.
Dixon AF, Dixon JB, O'Brien PE. Laparoscopic adjustable gastric banding induces prolonged satiety: a randomized blind crossover study. J Clin Endocrinol Metab. 2005;90:813–9.
Gamagaris Z, Patterson C, Schaye V, et al. Lap-band impact on the function of the esophagus. Obes Surg. 2008;18:1268–72.
Gutschow CA, Collet P, Prenzel K, et al. Long-term results and gastroesophageal reflux in a series of laparoscopic adjustable gastric banding. J Gastrointest Surg. 2005;9:941–8.
O'Brien PEPE, Brown WAWA, Dixon JBJB. Obesity, weight loss and bariatric surgery. Med J Aust. 2005;183:310–4.
Dixon JB, Anderson M, Cameron-Smith D, et al. Sustained weight loss in obese subjects has benefits that are independent of attained weight. Obes Res. 2004;12:1895–902.
Brown W, Burton P, Anderson M, et al. Symmetrical pouch dilatation after laparoscopic adjustable gastric banding: incidence and management. Obesity Surgery. 2008;18:1104–8.
Burton P, Richards M, Hebbard G, et al. Understanding the physiology of the lap-band using high resolution video manometry. Gastroenterology. 2008;134:A134.
Burton PR, Brown WA, Laurie C, et al. The effect of laparoscopic adjustable gastric bands on esophageal motility and the gastroesophageal junction; analysis using high resolution video manometry. Obes Surg. 2009;19(7):905–14.
Anvari M, Allen C, Borm A. Laparoscopic Nissen fundoplication is a satisfactory alternative to long-term omeprazole therapy. Br J Surg. 1995;82:938–42.
Dakkak M, Bennett JR. A new dysphagia score with objective validation. J Clin Gastroenterol. 1992;14:99–100.
Grande ED, Taylor A. Quality of life in South Australia as measured by the SF-36: population norms for 2002, trends from 1994 to 2002 and impact of chronic diseases and health risk factors on quality of life: population research and outcome studies unit. South Australia: Department of Human Services; 2004.
O'Brien PE, Dixon JB, Laurie C, et al. A prospective randomized trial of placement of the laparoscopic adjustable gastric band: comparison of the perigastric and pars flaccida pathways. Obes Surg. 2005;15:820–6.
Dixon JB, O'Brien PE. Gastroesophageal reflux in obesity: the effect of lap-band placement. Obes Surg. 1999;9:527–31.
Tolonen P, Victorzon M, Niemi R, et al. Does gastric banding for morbid obesity reduce or increase gastroesophageal reflux? Obes Surg. 2006;16:1469–74.
Vakil N. Review article: the role of surgery in gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2007;25:1365–72.
Financial disclosure
The Centre for Obesity Research and Education has received unrestricted research funding from Allergan, Inc., the manufacturer of the LAP-BAND.
Conflict of interest
None of the authors have a conflict of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Grant support: Paul Burton has received funding from the National Health and Medical Research Council (NHMRC) and the Royal Australasian College of Surgeons.
Rights and permissions
About this article
Cite this article
Burton, P.R., Brown, W., Laurie, C. et al. Outcomes, Satiety, and Adverse Upper Gastrointestinal Symptoms Following Laparoscopic Adjustable Gastric Banding. OBES SURG 21, 574–581 (2011). https://doi.org/10.1007/s11695-010-0073-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-010-0073-7