
Abstract
Background
Surgical site infections (SSIs) occur at a rate exceeding 40 % after head and neck reconstruction and are due in part to the clean-contaminated surgical field, in which cutaneous fields interact with oral or pharyngeal fields. The aim of this study was to clarify the most important risk factors for SSI and to identify effective strategies for preventing SSI.
Methods
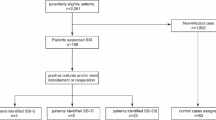
In 2011 and 2012, 197 patients who underwent head and neck reconstructive surgery were studied at National Cancer Center Hospital East, Japan. The SSI rate, risk factors for SSI, and biological aspects of SSI were evaluated prospectively.
Results
A total of 42 patients (21.3 %) had SSIs, and 62 bacterial species were identified at infection sites. Significant risk factors for SSI identified with multivariate analysis were hypoalbuminemia [P = 0.002, odds ratio (OR) = 3.37], reconstruction with vascularized bone transfer (P = 0.006, OR = 3.99), and a poor American Society of Anesthesiologists Physical Status score (P = 0.041, OR = 3.00). Most bacteria identified were species that persist around cutaneous and pharyngeal fields, but multidrug-resistant bacteria were rare.
Conclusions
The SSI rate at our hospital is lower than rates in previous studies. To minimize SSI, intervention to improve the patient’s perisurgical nutritional status and a more appropriate mandible reconstructive strategy should be considered.
Similar content being viewed by others


References
Cancer of the Oral Cavity.: NCCN clinical practice guidelines in oncology, version 2. 2011. http://www.nccn.org.
Hayashi R, Ebihara S. The treatment of locally advanced tongue cancer. Otologia Fukuoka. 2001;47:51–55.
Karakida K, Aoki T, Ota Y, Yamazaki H, Otsuru M, Takahashi M, et al. Analysis of risk factors for surgical-site infections in 276 oral cancer surgeries with microvascular free-flap reconstructions at a single university hospital. J Infect Chemother. 2010;16:334–9.
Liu SA, Wong YK, Poon CK, Wang CC, Wang CP, Tung KC. Risk factors for wound infection after surgery in primary oral cavity cancer patients. Laryngoscope. 2007;117:166–71.
Robbins KT, Storniolo AM, Kerber C, Seagren S, Berson A, Howell SB. Rapid superselective high-dose cisplatin infusion for advanced head and neck malignancies. Head Neck. 1992;14:364–71.
Kadota H, Fukushima J, Yoshida S, Kamizono K, Kumamoto Y, Masuda M, et al. Microsurgical free flap transfer in previously irradiated and operated necks: feasibility and safety. Auris Nasus Larynx. 2012;39:496–501.
Liu SA, Wong YK, Wang CP, Wang CC, Jiang RS, Ho HC, et al. Surgical site infection after preoperative neoadjuvant chemotherapy in patients with locally advanced oral squamous cell carcinoma. Head Neck. 2011;33:954–8.
Lee DH, Kim SY, Nam SY, Choi SH, Choi JW, Roh JL. Risk factors of surgical site infection in patients undergoing major oncological surgery for head and neck cancer. Oral Oncol. 2011;47:528–31.
Ogihara H, Takeuchi K, Majima Y. Risk factors of postoperative infection in head and neck surgery. Auris Nasus Larynx. 2009;36:457–60.
Hirakawa H, Hasegawa Y, Hanai N, Ozawa T, Hyodo I, Suzuki M. Surgical site infection in clean-contaminated head and neck cancer surgery: risk factors and prognosis. Eur Arch Otorhinolaryngol. 2013;270:1115–23.
Lotfi CJ, Cavalcanti Rde C, Costa e Silva AM, Latorre Mdo R, Ribeiro Kde C, Carvalho AL, et al. Risk factors for surgical-site infections in head and neck cancer surgery. Otolaryngol Head Neck Surg. 2008;138:74–80.
Cunha TF, Soares Melancia TA, Zagalo Fernandes Ribeiro CM, Almeida de Brito JA, Abreu Miguel SS, Andre Abreu Esteves Bogalhao do Casal D. Risk factors for surgical site infection in cervico-facial oncological surgery. J Craniomaxillofac Surg. 2012;40:443–8.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for Prevention of Surgical Site Infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27:97–132; quiz 133–4; discussion 196.
Sakuraba M, Miyamoto S, Kimata Y, Nakatsuka T, Harii K, Ebihara S, et al. Recent advances in reconstructive surgery: head and neck reconstruction. Int J Clin Oncol. 2013;18:561–5.
van Bokhorst-de van der Schueren MA, van Leeuwen PA, Sauerwein HP, Kuik DJ, Snow GB, Quak JJ. Assessment of malnutrition parameters in head and neck cancer and their relation to postoperative complications. Head Neck. 1997;19:419–25.
Hennessey DB, Burke JP, Ni-Dhonochu T, Shields C, Winter DC, Mealy K. Preoperative hypoalbuminemia is an independent risk factor for the development of surgical site infection following gastrointestinal surgery: a multi-institutional study. Ann Surg. 2010;252:325–9.
Braga M, Ljungqvist O, Soeters P, Fearon K, Weimann A, Bozzetti F. ESPEN Guidelines on Parenteral Nutrition: surgery. Clin Nutr. 2009;28:378–86.
Weimann A, Braga M, Harsanyi L, Laviano A, Ljungqvist O, Soeters P. ESPEN Guidelines on enteral nutrition: surgery including organ transplantation. Clin Nutr. 2006;25:224–44.
Snyderman CH, Kachman K, Molseed L, Wagner R, D’Amico F, Bumpous J, et al. Reduced postoperative infections with an immune-enhancing nutritional supplement. Laryngoscope. 1999;109:915–21.
Tsuchiya S, Nakatsuka T, Sakuraba M, Kimata Y, Sakurai H, Nakagawa M, et al. Clinical factors associated with postoperative complications and the functional outcome in mandibular reconstruction. Microsurgery. 2013;33:337–41.
Dormand EL, Banwell PE, Goodacre TE. Radiotherapy and wound healing. Int Wound J. 2005;2:112–27.
Miyamoto S, Sakuraba M, Nagamatsu S, Kamizono K, Fujiki M, Hayashi R. Combined use of free jejunum and pectoralis major muscle flap with skin graft for reconstruction after salvage total pharyngolaryngectomy. Microsurgery. 2013;33:119–24.
Sato J, Goto J, Harahashi A, Murata T, Hata H, Yamazaki Y, et al. Oral health care reduces the risk of postoperative surgical site infection in inpatients with oral squamous cell carcinoma. Support Care Cancer. 2011;19:409–16.
Bhathena HM, Kavarana NM. Prophylactic antibiotics administration head and neck cancer surgery with major flap reconstruction: 1-day cefoperazone versus 5-day cefotaxime. Acta Chir Plast. 1998;40:36–40.
Simo R, French G. The use of prophylactic antibiotics in head and neck oncological surgery. Curr Opin Otolaryngol Head Neck Surg. 2006;14:55–61.
Simons JP, Johnson JT, Yu VL, Vickers RM, Gooding WE, Myers EN, et al. The role of topical antibiotic prophylaxis in patients undergoing contaminated head and neck surgery with flap reconstruction. Laryngoscope. 2001;111:329–35.
Acknowledgment
This work was supported by National Cancer Center Research and Development Fund 23-A-26. This study was performed in conformity with the Declaration of Helsinki. Kenichi Kamizono and Minoru Sakuraba performed statistical analysis. Kenichi Kamizono, Shogo Nagamatsu, Minoru Sakuraba, Shimpei Miyamoto, and Ryuichi Hayashi performed operations.
Disclosure
The authors have no commercial associations or financial disclosures that might pose or create a conflict of interest with the information presented in this article
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kamizono, K., Sakuraba, M., Nagamatsu, S. et al. Statistical Analysis of Surgical Site Infection After Head and Neck Reconstructive Surgery. Ann Surg Oncol 21, 1700–1705 (2014). https://doi.org/10.1245/s10434-014-3498-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-3498-8