
Abstract
Background
The prevalence and characteristics of inappropriate use of proton pump inhibitors (PPIs) to prevent stress-related mucosal disease (SRMD) during the perioperative period and its associated factors are rarely reported. This study aimed to investigate the prevalence and characteristics of inappropriate prophylactic use of proton pump inhibitors (PPIs) during the perioperative period and identify its associated factors in a tertiary care and academic teaching hospital in China and to provide evidence for regulation authorities and pharmacists to take targeted measures to promote rational drug use.
Methods
Inpatients who underwent surgical operations and received prophylactic use of PPIs from June 2022 to November 2022 were included in this retrospective study. The appropriateness of perioperative prophylactic use of PPIs was evaluated by clinical pharmacists. Associated factors with inappropriate perioperative prophylactic use of PPIs were analyzed by univariable and multivariable logistic regression.
Results
Four-hundred seventy-two patients were finally included in this study, of which 131 (27.75%) patients had at least one problem with inappropriate perioperative prophylactic use of PPIs. The three most common problems were drug use without indication (52.0%), inappropriate usage and dosage (34.6%), and inappropriate duration of medication (6.7%). Multiple logistic regression analysis showed that oral dosage form of PPIs [OR = 18.301, 95% CI (7.497, 44.671), p < 0.001], discharge medication of PPIs [OR = 11.739, 95% CI (1.289, 106.886), p = 0.029], and junior doctors [OR = 9.167, 95% CI (3.459, 24.299), p < 0.001] were associated with more inappropriate prophylactic use of PPIs. Antithrombotics [OR = 0.313, 95% CI (0.136, 0.721), p = 0.006] and prolonged postoperative hospital stay (longer than 15 days) [OR = 0.262, 95% CI (0.072, 0.951), p = 0.042] were associated with less inappropriate prophylactic use of PPIs.
Conclusions
The inappropriate prophylactic use of PPIs during the perioperative period is common. Regulation authorities and pharmacists should take more targeted measures to promote the rational prophylactic use of PPIs during the perioperative period.
Similar content being viewed by others


Introduction
Stress-related mucosal disease (SRMD), also known as stress ulcer, refers to the acute gastrointestinal mucosal erosion, ulceration, and other lesions occurring in the body under various stress states such as severe trauma, complex surgery, and critical illness, which can lead to gastrointestinal bleeding or even perforation in severe cases (Bardou et al. 2015; Toews et al. 2018; Grube and May 2007). It can aggravate and worsen the degree of the original disease and increase the fatality rate (Bardou et al. 2015). Various difficult and complex surgeries are common stressors that induce SRMD (Li et al. 2022; Quenot et al. 2009). Prevention and treatment of perioperative SRMD can improve perioperative safety, shorten hospital stays, and reduce medical costs for high-risk surgical patients (Surgical Society of Chinese Medical Association 2015; Singh et al. 2016). Medications such as proton pump inhibitors (PPIs) and histamine-2 receptor antagonists (H2RAs) are commonly administered prophylactically to reduce the risk of SRMD (Clarke et al. 2022). PPIs, acting on H + /K + ATPase (the proton pump), inhibit the last channel of gastric acid secretion and have a good inhibitory effect on basal and food-stimulated acid secretions. Moreover, they have strong and longer-lasting inhibiting effects on gastric acid secretion and are safe and well tolerated (Helgadottir and Bjornsson 2019; Savarino et al. 2017; Ali et al. 2019). Currently, they are the preferred drugs for the clinical prevention and treatment of acid-related diseases (Bardou et al. 2015; Savarino et al. 2017; Alhazzani et al. 2018).
In recent years, PPIs have been widely used in the prevention of SRMD, especially in the perioperative period, and the problem of irrational drug use has become increasingly prominent (Chen et al. 2022; Savarino et al. 2018). The inappropriate prophylactic use of PPIs has not only increased the economic burden on patients, and caused the waste of medical resources, but has also raised the potential medical risks (Li et al. 2022). Therefore, the Chinese authorities have taken various measures to manage the inappropriate prophylactic use of PPIs and decrease medical costs. Studies have shown that 48.9–79% of surgical inpatients were inappropriately prescribed PPIs to prevent SRMD (Chen et al. 2022; Zhang et al. 2021; Bez et al. 2013). However, these studies were limited to specific single surgical departments such as general and hepatobiliary surgery and the analyses of pharmaceutical intervention. To date, research on the prevalence and characteristics of inappropriate prophylactic use of PPIs during the perioperative period and its associated factors is sparse.
Therefore, the primary objective of this study was to evaluate the appropriateness of perioperative prophylactic use of PPIs in inpatients. The second objective was to identify associated factors with the inappropriate prophylactic use of PPIs.
Methods
Setting and study design
This retrospective study was conducted in the Beijing Tongren Hospital affiliated with Capital Medical University, a 1759-bed tertiary care, teaching, and research institution. Patients who underwent surgical operations and received prophylactic use of PPIs during hospitalization from June 2022 to November 2022 were included in this study. Patients who were prescribed PPIs for the treatment of gastrointestinal diseases such as gastrointestinal hemorrhage, peptic ulcer, and gastroesophageal reflux disease were excluded. Patients with incomplete data were also excluded. The study was approved by the Beijing Tongren Hospital Ethics Committee (no. TREC2023-KY024). Patients were exempt from informed consent.
Data collection
The following information from the electronic medical records (EMRs) of Beijing Tongren Hospital was collected: demographics (age and gender), PPIs (drug name, dosage form, administration route, usage and dosage, time of medical orders, types of medical orders, professional titles of doctors), concomitant medications (nonsteroidal anti-inflammatory drugs [NSAIDs], systemic corticosteroids, antithrombotics), grade of surgery, intraoperative blood loss, types of medical insurance, length of postoperative hospital stay, and number of drugs used.
Evaluation criterion
The evaluation criterion was instituted to evaluate the appropriateness of perioperative prophylactic use of PPIs based on guidelines, expert consensuses, and drug instructions (American Society of Health-System Pharmacists 1999; Hospital Pharmacy Committee of Chinese Pharmaceutical Association 2020; Writing Group of Expert Consensus on the Preventive Application of Proton Pump Inhibitors 2018; Bai et al. 2018; National Health Commission of the People’s Republic of China 2020). The evaluation criterion included six aspects: indication, usage and dosage, drug selection, administration route, solvent, and duration, as shown in Table 1. The appropriateness of perioperative prophylactic use of PPIs was evaluated independently by two clinical pharmacists and then reviewed by each other. If there were any disputes, the two clinical pharmacists further discussed and reached a consensus. If there were still disputes, the clinical pharmacists’ supervisor decided the outcome.
Statistical analysis
Patients were divided into two groups based on the appropriateness of perioperative prophylactic use of PPIs. A descriptive analysis was performed on the patient’s demographics, PPIs (dosage form, time of medical orders, types of medical orders, professional titles of doctors), concomitant medications (NSAIDs, systemic corticosteroids, antithrombotics), grade of surgery, intraoperative blood loss, types of medical insurance, length of postoperative hospital stay, and number of drugs used.
For continuous variables, the Student’s t-test or the Mann–Whitney U-test was used to compare the two groups. Categorical variables were described by frequencies and percentages, and between-group differences were analyzed using the chi-square test and Fisher’s exact test if necessary. Variance inflation factor (VIF) values were calculated to measure the degree of multicollinearity among the variables that were significant in the univariate analysis (p < 0.1). A VIF of > 10 was considered indicative of multicollinearity and excluded from the logistic regression analysis. Based on the univariate analysis and VIF values, significant variables (p < 0.1) were included in the multiple logistic regression analysis to identify factors associated with the inappropriate prophylactic use of PPIs. All statistical analyses were carried out using SPSS (Version 26.0). p-values < 0.05 were considered statistically significant.
Results
Patient characteristics
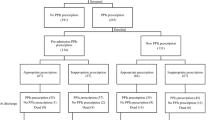
During the study period, a total of 472 patients were finally included in our study. The procedure of patient selection is presented in Fig. 1. Among the included patients, 112 (23.7%) were over 65 years old, 328 (69.5%) were male, and 144 (30.5%) were female. The top five departments in which patients were admitted were otorhinolaryngology-head and neck surgery (58.1%), neurosurgery (10.0%), orthopedics (8.3%), thoracic surgery (7.8%), and general surgery (5.7%).

Flowchart of the patient selection process
Appropriateness of perioperative prophylactic use of PPIs
According to the evaluation criterion, the inappropriateness of perioperative prophylactic use of PPIs was found in 131 of 472 patients, with an inappropriateness rate of 27.75%. A total of 179 cases of inappropriate drug use occurred in 131 patients, of which 93 cases (52.0%) were drug use without indication, 62 cases (34.6%) were inappropriate usage and dosage, and 12 cases (6.7%) were inappropriate duration of medication (Fig. 2).

Characterization and percentages of the 179 cases of inappropriate prophylactic use of PPIs during the perioperative period
Factors associated with the inappropriate prophylactic use of PPIs
In univariate analysis, 10 factors were significantly associated with inappropriate prophylactic use of PPIs (p < 0.05): gender, intraoperative blood loss, antithrombotics, systemic corticosteroids, dosage form, time of medical orders, types of medical orders, professional titles of doctors, number of drugs, and length of postoperative hospital stay (Table 2). The results of multicollinearity analysis showed that VIF values of 10 factors were less than 10. In multiple logistic regression analysis, the oral dosage form of PPIs, discharge medication of PPIs, and junior doctors were associated with more inappropriate prophylactic use of PPIs (p < 0.05) (Table 3). Antithrombotics and postoperative hospital stay longer than 15 days were associated with less inappropriate prophylactic use of PPIs (p < 0.05) (Table 3).
Discussion
To the best of our knowledge, this is the first study to explore the prevalence and characteristics of inappropriate prophylactic use of PPIs during the perioperative period and its associated factors. In our study, the inappropriateness rate of perioperative prophylactic use of PPIs was 27.75%, which was lower than in previous studies (Chen et al. 2022; Zhang et al. 2021; Bez et al. 2013). Different departments, study population size, different evaluation criteria, and study duration may lead to different inappropriateness rates (Liu et al. 2021). For example, previous studies had focused on patients admitted to specific surgical departments; however, our research was focused on patients in the perioperative period, which was also our biggest highlight. Meanwhile, the underprescription of PPIs was not considered in our study because our study population was limited to patients who had already used PPIs to prevent perioperative SRMD. In addition, we had taken some measures to improve the rationality of perioperative prophylactic use of PPIs prior to the study.
In our study, the most common problem was drug use without indication, which was also a major problem faced by other studies (Ali et al. 2019; Chen et al. 2022; Bez et al. 2013). Owing to concern about the risk of perioperative gastrointestinal bleeding, clinicians often prescribe PPIs to patients. In fact, the risk of perioperative gastrointestinal bleeding is only 4%, so there is no need to prescribe PPIs to prevent SRMD in low-risk perioperative patients (Li et al. 2022). Superior efficacy for acid suppression and the availability of generic formulations have led prescribers to favor the use of PPIs. This has also led to the overuse and abuse of PPIs (Savarino et al. 2018). A total of 25–70% of patients lack indications for PPIs use, resulting in unnecessary expenditure of close to £2 billion each year (Forgacs and Loganayagam 2008). In addition, overuse and abuse of PPIs are associated with a variety of adverse events in patients, such as acute kidney injury, Clostridioides difficile infection, pneumonia, and bone fractures (Savarino et al. 2017). Therefore, PPIs should only be used in patients with risk factors for SRMD during the perioperative period based on domestic and foreign guidelines and expert recommendations (American Society of Health-System Pharmacists 1999; Hospital Pharmacy Committee of Chinese Pharmaceutical Association 2020; Writing Group of Expert Consensus on the Preventive Application of Proton Pump Inhibitors 2018; Bai et al. 2018; National Health Commission of the People’s Republic of China 2020). Criteria for appropriate use include one serious risk factor or two potential risk factors, as shown in Table 1.
In this study, inappropriate usage and dosage were mainly reflected in the frequency of medication. The current literature showed that there was a contradiction in the frequency of administration, which focused on once or twice a day (American Society of Health-System Pharmacists 1999; Hospital Pharmacy Committee of Chinese Pharmaceutical Association 2020; Writing Group of Expert Consensus on the Preventive Application of Proton Pump Inhibitors 2018; Bai et al. 2018; National Health Commission of the People’s Republic of China 2020). PPIs maintain a longer-lasting acid inhibition, which is due to the fact that the proton pump cannot be recovered once it is deactivated, and its acid secretion can only be restored after the formation of a new proton pump. From the perspective of pharmacodynamics, the acid inhibition effect of PPIs can be maintained for 16–18 h (Savarino et al. 2018). Based on the above considerations, PPIs were administered once a day as an evaluation criterion in this study.
There is no clear standard for the duration of PPIs, but it is suggested that if patients can tolerate adequate enteral nutrition or have taken food, the clinical symptoms begin to improve as indications for drug withdrawal. Our study showed that 12 (9.2%) patients had an inappropriate duration of medication, which was mainly reflected in patients who continued to use PPIs even after discharge. Although the proportion of this problem is small, we should pay attention to it. Long-term use of PPIs may increase the risk of adverse reactions, especially in the absence of guidance from doctors or pharmacists after discharge. In our study, 78.4% of patients received intravenous PPIs, but only 3.1% of patients had a problem with the inappropriate route of administration, which was significantly lower than in previous studies (Li et al. 2022). This was attributed to the fact that patients admitted to otorhinolaryngology-head and neck surgery, neurosurgery, thoracic surgery, and other departments could not take medication orally or had gastrointestinal dysfunction after surgery.
Our study showed that oral dosage form of PPIs, discharge medication of PPIs, and junior doctors were associated with an increased risk of inappropriate prophylactic use of PPIs during the perioperative period, which was another highlight of this study. To our surprise, up to 87 of the 102 patients who received oral dosage form of PPIs had a problem with inappropriate prophylactic use of PPIs. In response to this study’s findings, a number of changes will be implemented in our hospital to address inappropriate use of PPIs for SRMD prophylaxis. Clinical pharmacists will strengthen training for doctors on the oral dosage form of PPIs. In particular, we recommend the prescriber to evaluate the need for ongoing PPI therapy at the time of the switch from injectable to oral and discontinue the PPI if it is no longer needed. Of the 87 patients who received inappropriate oral PPI orders, 48 were due to inappropriate discharge medication. It should be given more attention that discharge prescriptions make up 36.6% of the inappropriate orders. This result again confirms that inappropriate PPIs continuation upon discharge is a common issue despite several guidelines and ongoing global attention in recent years to highlight the risks versus benefit. The inappropriate PPIs continuation upon discharge exposes patients to excess risk of adverse events. Clinical pharmacists will rigorously review the surgical discharge medication of PPIs. In teaching hospital settings, it is often the primary responsibility of the junior doctor to enter medication orders after reviewing the case with the attending doctor. We will continue to explore the reasons behind the association between junior doctors and inappropriate prophylactic use of PPIs. In view of the current result, in addition to the training and education of doctors, especially junior doctors, adding a reminder function to the doctor’s order system may be a good approach (Clarke et al. 2021; Fan et al. 2023). When surgeons prescribe PPIs, the system will automatically pop up a reminder interface, including the indication of PPIs, usage and dosage, and the course of treatment, which will help surgeons use PPIs rationally.
The concomitant use of antithrombotics was associated with a decreased risk of inappropriate prophylactic use of PPIs during the perioperative period. Eid also found a similar conclusion that the combination of anticoagulants had a protective effect on the rational use of PPIs (Eid et al. 2010). However, another study showed that the concomitant use of aspirin or anticoagulants promoted inappropriate stress ulcer prophylaxis (Issa et al. 2012). Other studies had found that glucocorticoids were associated with the irrational use of PPIs, but our study did not find a similar conclusion (Li et al. 2022; Schepisi et al. 2016). The inappropriate prophylactic use of PPIs was reduced as the length of postoperative hospital stay (longer than 15 days) lengthened. This may be due to the increased risk factors for prophylactic use of PPIs in patients with prolonged hospital stay after surgery. Previous studies had explored the relationship between the length of hospital stay and the irrational use of PPIs, which was different from our study (Li et al. 2022; Mayet 2007).
Our study has the following limitations. First, this was a retrospective, single-center study. However, we believe our result is representative based on our hospital scale. Second, the study population size was small. The outbreak of the novel coronavirus reduced the number of inpatients during the study period. Third, there was a large percentage of otorhinolaryngology-head and neck surgery patients, which might not be representative of surgical patients in general. Finally, our study did not assess the underprescription of PPIs and track patient comorbidities and outcomes such as bleeding or other adverse events.
Conclusions
Our study demonstrates that the inappropriate prophylactic use of PPIs during the perioperative period is common in China. The most common problem is drug use without indication. Additionally, oral dosage form of PPIs, discharge medication of PPIs, and junior doctors are associated with more frequent inappropriate prophylactic use of PPIs. Consequently, regulation authorities and pharmacists should take more targeted measures to promote the rational prophylactic use of PPIs during the perioperative period.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- EMRs:
-
Electronic medical records
- H2RAs:
-
Histamine-2 receptor antagonists
- NSAIDs:
-
Nonsteroidal anti-inflammatory drugs
- PPIs:
-
Proton pump inhibitors
- SRMD:
-
Stress-related mucosal disease
- VIF:
-
Variance inflation factor
References
Alhazzani W, Alshamsi F, Belley-Cote E, Heels-Ansdell D, Brignardello-Petersen R, Alquraini M, et al. Efficacy and safety of stress ulcer prophylaxis in critically ill patients: a network meta-analysis of randomized trials. Intensive Care Med. 2018;44(1):1–11.
Ali O, Poole R, Okon M, Maunick S, Troy E. Irrational use of proton pump inhibitors in general practice. Ir J Med Sci. 2019;188(2):541–4.
American Society of Health-System Pharmacists. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health Syst Pharm. 1999;56:347–79.
Bai Y, Li Y, Ren X, Li Z. Expert advice on the prevention and treatment of stress ulcer (2018). Natl Med J China. 2018;98(42):3392–4.
Bardou M, Quenot JP, Barkun A. Stress-related mucosal disease in the critically ill patient. Nat Rev Gastroenterol Hepatol. 2015;12(2):98–107.
Bez C, Perrottet N, Zingg T, Leung Ki EL, Demartines N, Pannatier A. Stress ulcer prophylaxis in non-critically ill patients: a prospective evaluation of current practice in a general surgery department. J Eval Clin Pract. 2013;19(2):374–8.
Chen Q, Wang Q, Zhang Y. Clinical intervention increases rational use of proton pump inhibitors in the general surgery department. Front Pharmacol. 2022;13: 864081.
Clarke K, Adler N, Agrawal D, Bhakta D, Sata SS, Singh S, et al. Reducing overuse of proton pump inhibitors for stress ulcer prophylaxis and nonvariceal gastrointestinal bleeding in the hospital: a narrative review and implementation guide. J Hosp Med. 2021;16(7):417–23.
Clarke K, Adler N, Agrawal D, Bhakta D, Sata SS, Singh S, et al. Indications for the use of proton pump inhibitors for stress ulcer prophylaxis and peptic ulcer bleeding in hospitalized patients. Am J Med. 2022;135(3):313–7.
Eid SM, Boueiz A, Paranji S, Mativo C, Landis R, Abougergi MS. Patterns and predictors of proton pump inhibitor overuse among academic and non-academic hospitalists. Intern Med. 2010;49(23):2561–8.
Fan X, Chen D, Bao S, Dong X, Fang F, Bai R, et al. Prospective prescription review system correlated with more rational PPI medication use, better clinical outcomes and reduced PPI costs: experience from a retrospective cohort study. BMC Health Serv Res. 2023;23(1):1014.
Forgacs I, Loganayagam A. Overprescribing proton pump inhibitors. BMJ. 2008;336(7634):2–3.
Grube RR, May DB. Stress ulcer prophylaxis in hospitalized patients not in intensive care units. Am J Health Syst Pharm. 2007;64(13):1396–400.
Helgadottir H, Bjornsson ES. Problems associated with deprescribing of proton pump inhibitors. Int J Mol Sci. 2019;20(21):5469.
Hospital Pharmacy Committee of Chinese Pharmaceutical Association. Expert consensus on optimal application of proton pump inhibitors. Chin J Hosp Pharm. 2020;40(21):2195–213.
Issa IA, Soubra O, Nakkash H, Soubra L. Variables associated with stress ulcer prophylaxis misuse: a retrospective analysis. Dig Dis Sci. 2012;57(10):2633–41.
Li H, Li N, Jia X, Zhai Y, Xue X, Qiao Y. Appropriateness and associated factors of stress ulcer prophylaxis for surgical inpatients of orthopedics department in a tertiary hospital: a cross-sectional study. Front Pharmacol. 2022;13: 881063.
Liu P, Li G, Han M, Zhang C. Identification and solution of drug-related problems in the neurology unit of a tertiary hospital in China. BMC Pharmacol Toxicol. 2021;22(1):65.
Mayet AY. Improper use of antisecretory drugs in a tertiary care teaching hospital: an observational study. Saudi J Gastroenterol. 2007;13(3):124–8.
National Health Commission of the People’s Republic of China (NHCPRC) (2020). National Health Commission Office Notification on Guidelines for Clinical Application of Proton Pump Inhibitors. (2020 Edition). Beijing: National Health Commission. http://www.nhc.gov.cn/cms-search/xxgk/getManuscriptXxgk.htm?id=9aac2b191c844082aac2df73b820948f. Accessed 7 Jan 2022.
Quenot JP, Thiery N, Barbar S. When should stress ulcer prophylaxis be used in the ICU? Curr Opin Crit Care. 2009;15(2):139–43.
Savarino V, Dulbecco P, de Bortoli N, Ottonello A, Savarino E. The appropriate use of proton pump inhibitors (PPIs): need for a reappraisal. Eur J Intern Med. 2017;37:19–24.
Savarino V, Marabotto E, Zentilin P, Furnari M, Bodini G, De Maria C, et al. Proton pump inhibitors: use and misuse in the clinical setting. Expert Rev Clin Pharmacol. 2018;11(11):1123–34.
Schepisi R, Fusco S, Sganga F, Falcone B, Vetrano DL, Abbatecola A, et al. Inappropriate use of proton pump inhibitors in elderly patients discharged from acute care hospitals. J Nutr Health Aging. 2016;20(6):665–70.
Singh R, Trickett R, Meyer C, Lewthwaite S, Ford D.Prophylactic proton pump inhibitors in femoral neck fracture patients - a life - and cost-saving intervention. Ann R Coll Surg Engl. 2016;98(6):371-5.
Surgical Society of Chinese Medical Association. Prevention and treatment of stress related mucosal disease-expert consensus of Chinese general surgery (2015). Chin J Pract Surg. 2015;35(7):728–30.
Toews I, George AT, Peter JV, Kirubakaran R, Fontes LES, Ezekiel JPB, et al.Interventions for preventing upper gastrointestinal bleeding in people admitted to intensive care units. Cochrane Database Syst Rev. 2018;6(6):CD008687.
Writing Group of Expert Consensus on the Preventive Application of Proton Pump Inhibitors. Expert consensus on the preventive application of proton pump inhibitors (2018). Journal of Chinese physician. 2018;20(12):1775–80.
Zhang Y, Yang H, Kong J, Liu L, Ran L, Zhang X, et al. Impact of interventions targeting the inappropriate use of proton-pump inhibitors by clinical pharmacists in a hepatobiliary surgery department. J Clin Pharm Ther. 2021;46(1):149–57.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
PPL, GYL and CZ designed the study. PPL and GYL collected and the study data. PPL and MH performed the statistical analysis. PPL wrote the manuscript. PPL and QW revised the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Beijing Tongren Hospital Ethics Committee (No. TREC2023-KY024). Patients were exempt from informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
The evaluation criterion.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, P., Li, G., Wu, Q. et al. Analysis of inappropriate prophylactic use of proton pump inhibitors during the perioperative period: an observational study. Perioper Med 13, 19 (2024). https://doi.org/10.1186/s13741-024-00376-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13741-024-00376-w