
Abstract
Background
Pneumocystis jirovecii pneumonia (PCP) is a life-threatening opportunistic infection. In non-HIV immunocompromised patients with PCP, a standard second-line treatment has not been established up to now.
Methods
Non-HIV immunocompromised patients with confirmed PCP between April 2013 and December 2020 were included. Their PCP treatment history was tracked. Factors related to first-line trimethoprim/sulfamethoxazole (TMP/SMX) and second-line treatment failure were identified. Different second-line treatment strategies were compared.
Results
Among the 220 patients, 127 (57.73%) did not respond to first-line TMP/SMX treatment. Risk factors related to treatment failure included symptom triad with breathlessness at rest, persistent fever and cough (85% in the treatment failure group versus 74% in the treatment success group, P = 0.034), treatment with invasive mechanical ventilation (67 vs. 19%, P < 0.001), coinfection with CMV (69 vs. 47%, P = 0.035), and bacteremia (59 vs. 10%, P < 0.001). A total of 49 patients received second-line treatment on the basis of TMP/SMX, and 28 (57.1%) of them responded to the treatment. No clinical parameter, including selection of different therapies, was found to be significantly associated with second-line treatment failure. Further, the prognosis of different second-line therapies showed no drug or drug combination strategy superior to others. The primaquine group had lower 90-day mortality rate (45.9%) but showed no statistically significant difference compared with the non-primaquine group (64.6%). The patients in the clindamycin plus primaquine group had the lowest in-hospital mortality rate (22.2%, P = 0.042) among different second-line therapies, although the in-hospital mortality of the primaquine group was not significantly different from that of the non-primaquine group. The differences in 28 day mortality and overall mortality rates were not statistically significant, too.
Conclusion
CMV infection and bacteremia were risk factors significantly associated with treatment failure of TMP/SMX. The response and survival rates of second-line treatment, including clindamycin, primaquine, and caspofungin, were poor, maybe clindamycin plus primaquine as second line treatment was better than other treatment strategies. These results suggest that clinicians should carefully evaluate whether the treatment of TMP/SMX has failed due to a coinfection rather than hastily changing to a second-line drug when the patient worsens.
Similar content being viewed by others

Introduction
Pneumocystis jirovecii pneumonia (PCP) is a life-threatening opportunistic infection that often occurs in immunocompromised patients [1]. On one hand, although PCP most commonly occurs in HIV-positive patients, with the increased use of new HIV antiretroviral medications and routine prophylaxis of PCP, its incidence has decreased gradually [2]. On the other hand, the expanding use of immunosuppressive medications for patients with solid and hematological malignancies, the development of organ or hematopoietic stem cell transplants, and the increased prevalence of autoimmune and inflammatory diseases has made PCP a prevalent opportunistic infection among patients without HIV infection [3]. Furthermore, non-HIV immunocompromised patients are characterized by a more rapid disease progression, with a mortality rate of 35–55% compared with 10–20% in HIV-infected patients [3, 4].
Based on data from clinical trials, trimethoprim/sulfamethoxazole (TMP/SMX) is the first-line medications for PCP-infected patients because of its low cost and good clinical efficacy, but when clinicians are faced with its clinical failure, they have to switch drug therapy to second-line agents. The alternative treatment regimens included clindamycin with primaquine, dapsone with trimethoprim, atovaquone, or pentamidine [4, 5]. Recently, caspofungin was also found capable of slowing down or even stopping PCP progression via substantial depletion of the fungal burden [6]. However, there is no widely accepted consensus on an optimal second-line regimen. Meanwhile, the majority of information on PCP treatment is extrapolated from HIV-related studies, with limited literature that has determined the efficacy in the non-HIV population [6, 7].
The goal of this study was to explore the risk factors for treatment failure during TMP/SMX therapy for PCP and to compare the efficacy of the available second-line agents, including clindamycin, primaquine and caspofungin.
Methods
Patients
We conducted a retrospective study at Peking Union Medical College Hospital (PUMCH). The study cohort comprised all non-HIV immunocompromised patients who had confirmed PCP and were treated at PUMCH between April 1st, 2013, and December 31st, 2020.
Data collection
From the patients’ medical records, we collected their information, including age, sex, underlying diseases (autoimmune disease, hematological malignancies, solid tumor, organ transplantation and others), treatment history (glucocorticoid, immunosuppressant and preventive dose of sulfanilamide, PCP prophylaxis), clinical manifestations (fever, cough, wheeze), level of white blood cells (WBC), lymphocyte (LY#), lactate dehydrogenase (LDH) and (1–3)-beta-D-glucan (BDG), need for ICU and mechanical ventilation, dates of treatment initiation and cessation, treatment switches, complications [bacteremia, cytomegalovirus (CMV) infection] and outcome.
PCP treatment
During this 8-year period, primary PCP episodes in non-HIV immunocompromised patients were treated with TMP/SMX initiated at a standard dosage of 15–20 mg/kg/day of TMP equivalent in 3–4 doses per day. The duration of TMP/SMX treatment was 21 days for patients who responded. If the patient was previously allergic to sulfonamides, desensitization therapy would be adopted. If acute kidney injury appeared, the dose of TMP/SMX was adjusted according to the renal function.
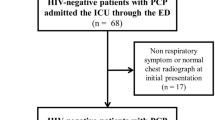
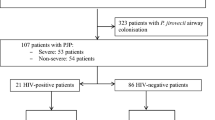
In cases of treatment failure, a second-line regimen could be used according to the clinician’s consideration. Because of the unavailability of most regimens and the lack of clinical experience, the second-line treatments used are shown in Fig. 1, including clindamycin (1200 mg, intravenous infusion, 2 times daily) (C), clindamycin (600 mg, oral, 3 times daily) plus primaquine (30 mg, oral, once daily) (C-P), clindamycin (1200 mg, intravenous infusion, 2 times daily) plus caspofungin (50 mg, intravenous infusion, once daily) (C-Ca), and clindamycin (1200mg, intravenous infusion, 2 times daily) plus primaquine (30 mg, oral, once daily) plus caspofungin (50 mg, intravenous infusion, once daily) (C-P-Ca).

Patients’ treatment flow and outcome. Clindamycin (C), clindamycin plus primaquine (C-P), clindamycin plus caspofungin (C-Ca), clindamycin plus primaquine plus caspofungin (C-P-Ca)
For patients with severe infection, adjunctive corticosteroids (40–80 mg daily) were given until PCP improvement. Except for steroids, other disease-related immunosuppressive drugs were stopped.
Definition
The eligible patients had clinical manifestations of PCP, such as dyspnea, cough, fever, or abnormal chest radiographs. The mycological and morphological diagnoses were confirmed by real-time fluorescence quantitative polymerase chain reaction (qPCR) and Grocott's methenamine silver (GMS) staining of respiratory samples, respectively [8]. Based on the criteria used in previous studies [5, 9, 10], the diagnosis of PCP was considered definitive if a positive PCR test for Pneumocystis jirovecii (P. jirovecii) DNA in bronchoalveolar lavage fluid (BALF) or GMS staining positive on BALF or sputum or a positive PCR test for P. jirovecii DNA in sputum was confirmed, combined with an increased level of BDG from patients with clinical manifestations (fever, dry cough, or dyspnea), hypoxemia, and radiologic findings compatible with PCP. The diagnosis of PCP was considered presumptive if patients met all clinical criteria and had either a positive PCR test for P. jirovecii DNA in sputum or an increased level of BDG, after excluding other fungal infections [9]. In our study, both definitive and presumptive cases were included.
Treatment success was defined as a clinical cure or showing definitive clinical improvement with resolution of dyspnea and chest infiltrates. Treatment failure was defined as clinical deterioration occurring 4–8 days after TMP/SMX treatment: (1) progressive clinical deterioration characterized by an inability to maintain a stable PaO2 despite an increased proportion of FiO2 and/or persistent fever; and (2) progressive deterioration of vital signs and/or radiographic worsening [11]. The classification of the PCP severity is based on clinical symptoms, arterial blood gases and oxygen saturation, and radiological findings [12]. CMV infection was defined as having CMV blood viral load of over 500 copies/ml, and all such patients received ganciclovir treatment.
The primary outcome was 90-day mortality, and the secondary outcomes included in-hospital mortality, 28-day mortality and overall survival, defined as the time from diagnosis to death or last follow-up.
Statistics
Risk factors associated with TMP/SMX treatment failure were analyzed by Mann–Whitney U or Fisher’s exact tests as appropriate. To identify independent risk factors, parameters with P < 0.05 in the univariate analysis were analyzed using a multivariate logistic regression model. Categorical variables were compared using the chi-square test. Kaplan–Meier analysis was used for survival analysis, and survival curves of different groups were compared using the log-rank test. P < 0.05 was considered statistically significant. Considering the limited sample size of our study, the standardized mean difference (SMD) was used to describe the effect after controlling the baseline confounding factors and to reflect the differences between groups if the p-value was > 0.05. SPSS version 22.0 (IBM Corporation, Armonk, New York, USA) was used for the statistical analysis.
Results
Identifying risk factors associated with first-line TMP/SMX treatment failure
Between April 1st, 2013, and December 31st, 2020, 220 non-HIV immunocompromised patients infected with PCP were hospitalized in our hospital. Among these 220 patients, 182 had definite PCP infection, and 38 had presumptive PCP infection. All of the patients were first treated with TMP/SMX. Acute kidney injury occurred in 35 of the 220 patients, and 8 of these patients were previously allergic to sulfonamides. Despite the adverse reactions, they still managed to use TMP/SMX after dose adjustment and desensitization therapy. Among these 220 patients, 127 (57.73%) did not respond to the first-line TMP/SMX treatment.
Complete clinical data were available in 209 patients. We compared the clinical characteristics between the treatment success group (n = 93) and the treatment failure group (n = 116) as shown in Table 1. The risk factors related to TMP/SMX treatment failure in PCP-infected non-HIV immunocompromised patients included symptom triad with breathlessness at rest, persistent fever and cough (P = 0.034), treatment with invasive mechanical ventilation (P < 0.001), coinfection with CMV (P = 0.035), and bacteremia (P < 0.001).
Risk factors associated with second-line treatment failure
Among the patients who did not respond to TMP-SMX, 78 died after not being given an alternative regimen, and 71 died during the administration of TMP/SMX. In the remaining 49 patients, 42 had definite PCP infection, and 7 had presumptive PCP infection. They received second-line treatment: C-P for 9 patients, C-P-Ca for 9 patients, C for 13 patients and C-Ca for 18 patients. In all, 57.1% (28/49) patients responded to the treatment, 42.9% (21/49) patients did not respond to the second-line therapies. According to different therapies, the response rates were 66.67% (6/9) in the C-P group, 33.3% (3/9) in the C-P-Ca group, 53.85% (7/13) in the C group, and 66.67% (12/18) in the C-Ca group. As shown in Table 2, the comparison of clinical features between second-line treatment success and treatment failure groups revealed no risk factor, including the factors associated with first-line TMP/SMX treatment failure.
Prognosis of different second-line therapies
As the sample sizes of these 4 groups were not large enough to conduct statistical analyses and all of the patients received clindamycin, the 49 patients were divided according to whether primaquine or caspofungin was used: the caspofungin group (n = 27) including patients treated with C-Ca and C-P-Ca, and the noncaspofungin group (n = 22) including patients treated with C and C-P; the primaquine group (n = 18) including patients treated with C-P and C-P-Ca, and the nonprimaquine group (n = 31) including patients treated with C and C-Ca.
The characteristics of these groups are summarized in Tables 3 and 4. During the median follow-up time of 44 days, the median overall survival of patients treated with C, C-P, C-Ca, and C-P-Ca was 33 days, 53 days, 40 days, and 23 days, respectively (P = 0.614) (Fig. 2). The 90-day mortality rate of the primaquine group (45.9%) was numerically lower than that of the nonpraquine group (64.6%), but the difference was not statistically significant [P = 0.171, SMD = 0.381, odds ratio (OR) = 0.467]. The overall in-hospital mortality rate was 53.1% (26/49), which was the lowest in the C-P group (22.2% in the C-P group, 46.2% in the C group, 66.7% in the C-Ca group, 66.7% in the C-P-Ca group; P = 0.042), although the in-hospital mortality of the primaquine group was not significantly different from that of the nonprimaquine group. Similarly, other secondary outcomes including 28-day mortality and overall survival also numerically improved in the primaquine group but the differences were not statistically significant (Table 5). The 90-day mortality was not improved in the caspofungin group, and it was even higher compared with the non-caspofungin group (64.6 vs.21.8%, P = 0.003, SMD = 0.958, OR = 6.549). In-hospital mortality, 28-day mortality and overall survival also significantly worsened in the caspofungin group (Table 5).

Kaplan–Meier analysis of patients’ overall survival. Clindamycin (C), clindamycin plus primaquine (C-P), clindamycin plus caspofungin (C-Ca), clindamycin plus primaquine plus caspofungin (C-P-Ca)
Discussion
Pneumocystis jirovecii pneumonia is a life-threatening complication following immunosuppressive therapy. When TMP/SMX treatment failure occurs, clinicians tend to blame it on the limited efficacy of TMP/SMX, and hastily change to a second-line drug without contemplating the real cause. Also, data on the efficacy of different second-line drugs remain limited. Therefore, the need to evaluate the risk factors for TMP/SMX treatment failure and consider alternative regimens has increased. We demonstrated that factors indicating co-infection were related to a poor response to first-line TMP/SMX treatment.
The factors related to first-line TMP/SMX treatment failure include symptom triad (breathlessness at rest, persistent fever and cough), treatment with invasive mechanical ventilation, coinfection with CMV and bacteremia. According to the guidelines for classifying the severity of PCP in HIV and non-HIV patients, the clinical features of severe PCP include breathlessness at rest, persistent fever and cough, PaO2 < 8 kPa in arterial blood gases, oxygen saturation < 91% at rest on air, and extensive interstitial shadowing [12]. We did not summarize the radiological findings, but the symptom triad and treatment with invasive mechanical ventilation indicated that the patients were in a severe condition [12]. Similarly, in Qing Yu’s study, CMV infection was proven to be associated with severe dyspnea and lower PaO2/FiO2, which also indicated severe PCP [13]. There are no published articles reporting the relationship between the severity of PCP and the treatment efficacy of TMP/SMX, but from our study, we may conjecture that severe PCP indicates a subgroup of patients who will have a poor response to first-line TMP/SMX therapy. In addition, both concurrent CMV infection and bacteremia were positively associated with mortality in non-HIV PCP patients, consistent with the results of published articles [13, 14]. Therefore, TMP/SMX treatment failure might be due to secondary infection rather than actual treatment failure.
To date, there are no high-quality guidelines or randomized controlled trials with a high grade of evidence supporting any second-line PCP treatment. The 6th European Conference on Infections in Leukemia published guidelines for the PCP treatment of non-HIV-infected hematology patients in 2016, there was no second-line intervention with a grade A strength of recommendation. Primaquine plus clindamycin and pentamidine were the two alternatives having a grade B strength of recommendation [15]. According to Helweg-Larsen and colleagues, primaquine plus clindamycin had similar second-line therapy survival rates compared with TMP/SMX, while pentamidine was associated with a greater risk of death [16]. Similarly, Kim and colleagues demonstrated that the response rate of patients to C-P was higher than that of patients to pentamidine (64% vs. 11%, p = 0.03) [17]. Koga M et al. concluded that primaquine plus clindamycin appears to be a better candidate as a salvage treatment than pentamidine or atovaquone [18]. In our research found there was no parameter significantly associated with better second-line treatment outcome. Among clindamycin, primaquine and caspofungin, no drug or drug combination strategy was shown superior to others in terms of response and survive.
In recent years, caspofungin, a novel antifungal agent that inhibits the synthesis of β-1,3-glucan in the cell wall, has been proven effective in the treatment of PCP infection [19, 20]. Combined with TMP/SMX in the first-line setting, the positive response rate was significantly better and the all-cause in-hospital mortality rate was significantly lower compared with TMP/SMX monotherapy. The number of adverse events was not increased [21]. However, caspofungin acts on cyst forms of P. jirovecii only [19]. Furthermore, caspofungin was significantly less effective in second-line treatment than in first-line treatment in terms of both the mortality rate and response rate [22, 23]. Additionally, caspofungin combined with clindamycin was used for PCP treatment in recent studies [24, 25]. In our study, we found that the 90-day mortality and other secondary outcomes were higher in the caspofungin group. The cause of worse prognosis could be attributed to the greater severity and higher percentage of bacteremia in patients receiving caspofungin. Meanwhile, in recent years, it was demonstrated that caspofungin had better efficacy in PCP patients having higher BDG levels [11]. However, in our study, the BDG level was lower in the caspofungin group than in the noncaspofungin group, indicating a non-optimized patient population. Considering the poor accessibility, relatively high cost and intravenous route of administration of caspofungin, we suggest C-P conbination as a preferred choice for second-line non-HIV PCP treatment in mainland China if co-infection has been carefully ruled out. Although its efficacy is not significantly better in our study, its efficacy should be further tested in future investigation with larger sample size.
Our study has several limitations. First, it is a single-center retrospective study with a limited sample size and without a randomized controlled design; thus, the results should be extended to the whole patient population with caution. Prospective studies with larger sample sizes are warranted in the future. Second, because there are no widely accepted guidelines for second-line PCP treatment, the selection of drugs was complicated in our study. Third, the first-line TMP/SMX treatment success rate was lower than previous work [17], probably due to selection bias in our hospital, since PUMCH is the last choice for many critically ill patients in mainland China.
Conclusion
CMV infection and bacteremia were risk factors significantly associated with treatment failure of TMP/SMX, the response and survival rates of second-line treatment, including clindamycin, primaquine, and caspofungin, were poor, maybe clindamycin plus primaquine as second line treatment was better than other treatment strategies. These results suggest that clinicians should carefully evaluate whether the treatment of TMP/SMX has failed due to a coinfection rather than hastily changing to a second-line drug when the patient worsens.
Availability of data and materials
The datasets used in the study are available from the corresponding author on reasonable request.
Abbreviations
- BDG:
-
(1–3)-Beta-D-glucan
- C:
-
Clindamycin
- C-P:
-
Clindamycin plus primaquine
- C-Ca:
-
Clindamycin plus caspofungin
- C-P-Ca:
-
Clindamycin plus primaquine plus caspofungin
- CI:
-
Confidence interval
- CMV:
-
Cytomegalovirus
- HIV:
-
Human immunodificiency virus
- IMV:
-
Invasive mechanical ventilation
- IS:
-
Immunosuppressant
- LY:
-
Lymphocyte
- LDH:
-
Lactate dehydrogenase
- OR:
-
Odds ratio
- PCP:
-
Pneumocystis jirovecii pneumonia
- p T/S:
-
Preventive T/S to 2nd days
- RID:
-
Rheumatic immune disease
- SD:
-
Standard deviation
- SMD:
-
Standardized mean difference
- SS:
-
Sufficient steroid
- TMP/SMX:
-
Trimethoprim/sulfamethoxazole
- TS:
-
Typical symptoms of simultaneous breathlessness at rest, persistent fever and cough
- T/S to 2nd days:
-
TMP/SMX to second-line therapy days
- WBC:
-
White blood cell
References
de Armas RY, Wissmann G, Müller AL, Pederiva MA, Brum MC, Brackmann RL, et al. Pneumocystis jirovecii pneumonia in developing countries. Parasite. 2011;18(3):219–28.
Kim SJ, Lee J, Cho YJ, Park YS, Lee CH, Yoon HI, et al. Prognostic factors of Pneumocystis jirovecii pneumonia in patients without HIV infection. J Infect. 2014;69(1):88–95.
Avino LJ, Naylor SM, Roecker AM. Pneumocystis jirovecii pneumonia in the non-HIV-infected population. Ann Pharmacother. 2016;50(8):673–9.
Salzer HJF, Schäfer G, Hoenigl M, Günther G, Hoffmann C, Kalsdorf B, et al. Clinical, diagnostic, and treatment disparities between HIV-infected and Non-HIV-infected immunocompromised patients with Pneumocystis jirovecii pneumonia. Respiration. 2018;96(1):52–65.
White PL, Backx M, Barnes RA. Diagnosis and management of Pneumocystis jirovecii infection. Expert Rev Anti Infect Ther. 2017;15(5):435–47.
Desoubeaux G, Lemaignen A, Ehrmann S. Scientific rationale for inhaled caspofungin to treat Pneumocystis pneumonia: a therapeutic innovation likely relevant to investigate in a near future. Int J Infect Dis. 2020;95:464–7.
Cooley L, Dendle C, Wolf J, Teh BW, Chen SC, Boutlis C, et al. Consensus guidelines for diagnosis, prophylaxis and management of Pneumocystis jirovecii pneumonia in patients with haematological and solid malignancies, 2014. Intern Med J. 2014;44(12b):1350–63.
Sun R, Lv D, Xiao M, Zhang L, Xu J, Yu X, et al. Diagnostic accuracy of the 1,3-beta-D-glucan test and lactate dehydrogenase for pneumocystis pneumonia in non-HIV patients. Sci Rep. 2021;11(1):9226.
Guegan H, Robert-Gangneux F. Molecular diagnosis of Pneumocystis pneumonia in immunocompromised patients. Curr Opin Infect Dis. 2019;32(4):314–21.
Perret T, Kritikos A, Hauser PM, Guiver M, Coste AT, Jaton K, et al. Ability of quantitative PCR to discriminate Pneumocystis jirovecii pneumonia from colonisation. J Med Microbiol. 2020;69:705–11.
Jin F, Liu XH, Chen WC, Fan ZL, Wang HL. High initial (1, 3) Beta-d-Glucan concentration may be a predictor of satisfactory response of c aspofungin combined with TMP/SMZ for HIV-negative patients with moderate to severe Pneumocystis jirovecii pneumonia. Int J Infect Dis. 2019;88:141–8.
Oladele RO, Otu AA, Richardson MD, Denning DW. diagnosis and management of pneumocystis pneumonia in resource-poor settings. J Health Care Poor Underserved. 2018;29(1):107–58.
Yu Q, Jia P, Su L, Zhao H, Que C. Outcomes and prognostic factors of non-HIV patients with pneumocystis jirovecii pneumonia and pulmonary CMV co-infection: a Retrospective Cohort Study. BMC Infect Dis. 2017;17(1):392.
Smego RA Jr, Nagar S, Maloba B, Popara M. A meta-analysis of salvage therapy for Pneumocystis carinii pneumonia. Arch Intern Med. 2001;161(12):1529–33.
Maschmeyer G, Helweg-Larsen J, Pagano L, Robin C, Cordonnier C, Schellongowski P. 6th European Conference on Infections in Leukemia (ECIL-6), a joint venture of The European Group for Blood and Marrow Transplantation (EBMT), The European Organization for Research and Treatment of Cancer (EORTC), the International Immunocompromised Host Society (ICHS) and The European LeukemiaNet (ELN). ECIL guidelines for treatment of Pneumocystis jirovecii pneumonia in non-HIV-infected haematology patients. J Antimicrob Chemother. 2016;71(9):2405–13.
Helweg-Larsen J, Benfield T, Atzori C, Miller RF. Clinical efficacy of first- and second-line treatments for HIV-associated Pneumocystis jirovecii pneumonia: a tri-centre cohort study. J Antimicrob Chemother. 2009;64(6):1282–90.
Kim T, Kim SH, Park KH, Cho OH, Sung H, Kim MN, et al. Clindamycin-primaquine versus pentamidine for the second-line treatment of pneumocystis pneumonia. J Infect Chemother. 2009;15(5):343–6.
Koga M, Suganuma A, Kikuchi T, Yoshimura Y, et al. Primaquine plus clindamycin as a promising salvage therapy for Pneumocystis jirovecii pneumonia: a retrospective analysis in Japanese patients. J Infect Chemother. 2021;27(6):924–8.
Nevez G, Le Gal S. Caspofungin and Pneumocystis pneumonia: it is time to go ahead. Antimicrob Agents Chemother. 2019;63(10):e01296-e1319.
Armstrong-James D, Stebbing J, John L, Murungi A, Bower M, Gazzard B, et al. A trial of caspofungin salvage treatment in PCP pneumonia. Thorax. 2011;66(6):537–8.
Tian Q, Si J, Jiang F, Xu R, Wei B, Huang B, et al. Caspofungin combined with TMP/SMZ as a first-line therapy for moderate-to-severe PCP in patients with human immunodeficiency virus infection. HIV Med. 2021;22(4):307–13.
Zhang G, Chen M, Zhang S, Zhou H, Ji X, Cai J, et al. Efficacy of caspofungin combined with trimethoprim/sulfamethoxazole as first-line therapy to treat non-HIV patients with severe pneumocystis pneumonia. Exp Ther Med. 2018;15(2):1594–601.
Kim T, Hong HL, Lee YM, Sung H, Kim SH, Choi SH, et al. Is caspofungin really an effective treatment for Pneumocystis jirovecii pneumonia in immunocompromised patients without human immunodeficiency virus infection? Experiences at a single center and a literature review. Scand J Infect Dis. 2013;45(6):484–8.
Li H, Huang H, He H. Successful treatment of severe Pneumocystis pneumonia in an immunosuppressed patient using caspofungin combined with clindamycin: a case report and literature review. BMC Pulm Med. 2016;16(1):144.
Yao Z, Hua Z, Jun X, Chan W, Xiao-jun M. Lack of response in severe pneumocystis pneumonia to combined caspofungin and clindamycin treatment: a case report. Chin Med Sci J. 2011;26(4):246–8.
Acknowledgements
Not applicable.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Author information
Authors and Affiliations
Contributions
AL and RS performed the data analyses and finished this manuscript. JY contributed to the study’s design, data analysis and interpretation, modified of the manuscript, and taken responsibility for the integrity of the data and the accuracy of the data analysis. HZ contributed to the conception of the study and helped perform the analysis with constructive discussions. XL and GC performed the data collection. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were performed in accordance with the relevant guidelines and regulations. The research was approved by the Ethics Committee of the Institutional Review Board at Peking Union Medical College Hospital (PUMCH, zs3400). The requirement for informed consent was waived by the Ethics Committee of the Institutional Review Board at Peking Union Medical College Hospital (PUMCH) because of the retrospective nature of the research.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, A., Sun, R., Cao, G. et al. Prognostic factors and clinical efficacy of second-line treatments of Pneumocystis jirovecii pneumonia for non-HIV patients after first-line treatment failure. BMC Infect Dis 22, 546 (2022). https://doi.org/10.1186/s12879-022-07523-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-022-07523-y