
Abstract
Introduction
Patients with ankylosing spondylitis (AS) are burdened with symptoms impacting work productivity measured by presenteeism, absenteeism, overall work impairment, and activity impairment. Ixekizumab, a high-affinity monoclonal antibody selectively targeting interleukin-17A, has been demonstrated to improve disease signs and symptoms in two phase 3 trials of AS. This study investigated for 52 weeks the effect of ixekizumab treatment on work productivity in patients with active AS.
Methods
COAST-V (NCT02696785) and COAST-W (NCT02696798) were phase 3, multicenter, randomized, controlled trials investigating the efficacy of ixekizumab 80 mg every 4 weeks (Q4W) and every 2 weeks (Q2W) in patients with AS naïve to biologic disease-modifying antirheumatic drugs (bDMARDs; COAST-V) or who were inadequate responders or intolerant to tumor necrosis factor inhibitors (TNFi; COAST-W). Work productivity was measured with the Work Productivity and Activity Impairment Questionnaire for Spondyloarthritis at weeks 16 and 52. Absenteeism, presenteeism, and overall work impairment were assessed for patients reporting paid work. Activity impairment was assessed regardless of work status.
Results
At baseline, 66.2% (434/656) of patients reported paid work. At week 16, bDMARD-naïve patients treated with both ixekizumab dose regimens and TNFi-experienced patients treated with ixekizumab Q2W reported significant improvements in activity impairment (p < 0.01 and p < 0.05, respectively). TNFi-experienced patients treated with ixekizumab showed significant improvements versus placebo in presenteeism and overall work impairment (p < 0.05); bDMARD-naïve patients had numeric improvements. After week 16, patients initially on placebo switched to ixekizumab and patients already treated with ixekizumab continued treatment. Improvements in work productivity and daily activity were sustained through week 52 for both bDMARD-experienced and -naïve patients.
Conclusion
Both bDMARD-naïve and TNFi-experienced patients with AS had greater improvements in work productivity and activity impairment when receiving ixekizumab compared to placebo at week 16. Improvements in work productivity and activity impairment achieved at week 16 were sustained through week 52 with ixekizumab treatment.
Similar content being viewed by others


Why carry out this study? |
Impaired work productivity burdens patients with ankylosing spondylitis (AS). |
This study investigated the effect of ixekizumab treatment for 52 weeks on work productivity in patients with active AS who were naïve to biologic disease-modifying antirheumatic drugs (bDMARDs) or who were inadequate responders or intolerant to tumor necrosis factor inhibitors (TNFi). |
What was learned from the study? |
Treatment with ixekizumab improved work productivity in both bDMARD-naïve and TNFi-experienced patients with AS at week 16, and improvements were maintained through 52 weeks. |
The results of this study suggest that health-related quality of life in patients with AS may be improved with ixekizumab treatment. |
Introduction
Ankylosing spondylitis (AS), also known as radiographic axial spondyloarthritis (r-axSpA), is a chronic inflammatory disease characterized by spinal inflammation and radiographically defined structural damage to the sacroiliac joint [1, 2]. One of the hallmarks of the disease is new bone formation (syndesmophytes, joint ankyloses), which can lead to additional functional limitations. Other features include peripheral musculoskeletal manifestations (inflammatory arthritis, enthesitis, dactylitis). Patients can also have extra-musculoskeletal manifestations (anterior uveitis, psoriasis, inflammatory bowel disease) [3, 4]. Patients with AS often have a reduced quality of life and experience impaired work productivity [2, 5]. Compared to the general population, patients with AS are burdened with lower rates of employment and greater rates of work disability as well as more absences from work [2]. Half of patients with AS experience work instability, and patients with AS withdraw from work threefold more often than the general population [6]. Employment loss is associated with greater physical impairment and negative psychosocial outcomes, both of which contribute to significant personal and societal impacts [6]. Because patients begin experiencing AS symptoms relatively early in life (often during early adulthood), there is a need to manage symptoms over many years to decrease both individual and societal burdens [2,7]. The overall mean age of patients in this analysis was 43.8 years, which is generally considered to be a productive time in one’s life.
Since some patients with AS receiving tumor necrosis factor inhibitors (TNFi) continue to suffer from symptoms that impact their health-related quality of life (HRQoL) despite treatment, the development and use of therapies with different mechanisms are needed [5]. Ixekizumab, a high-affinity monoclonal antibody selectively targeting interleukin 17A (IL-17A), has been shown to improve disease signs and symptoms in two phase 3 trials of patients with active AS, COAST-V and COAST-W [3,8]. In the study reported here, we used data from these 2 clinical trials to evaluate the effect of ixekizumab treatment for 52 weeks on work productivity in patients with active AS who were naïve to biologic disease-modifying antirheumatic drugs (bDMARDs, COAST-V) and patients who were inadequate responders or intolerant to TNFi (COAST-W).
Methods
Study Design
Descriptions of the designs of the COAST-V and COAST-W trials have been published previously [3, 8]. COAST-V and COAST-W were phase 3, multicenter, randomized, double-blind, placebo-controlled trials conducted at 84 and 106 sites in 12 and 15 countries, respectively, across the regions of North America, South America, Europe, and Asia. COAST-V and COAST-W were registered at ClinicalTrials.gov (NCT0269785 and NCT2696798, respectively).
Ethical review boards approved COAST-V and COAST-W at each site before the trials began. Procedures involving human participants were performed within the ethical standards of the institutional and national research committees at all sites. Both trials were conducted in accordance with the standards of the Declaration of Helsinki of 1964 and its later amendments. All patients gave written informed consent before undergoing procedures related to the trials. The master ethics committee was Schulman Associates IRB, Cincinnati, OH, USA, Complete listings of sites and investigators are available in the supplements of previously published results from COAST-V and COAST-W [3,8, 9].
Patients
Patients enrolled in COAST-V and COAST-W were adults fulfilling the Assessment of SpondyloArthritis International Society (ASAS) criteria for r-axSpA (having evidence of radiographic sacroilitis according to the modified New York criteria and having ≥ 1 spondyloarthritis feature). Patients in COAST-V had no prior history of receiving bDMARDs; patients in COAST-W had prior treatment with one or two TNFi and had discontinued at least one TNFi due to inadequate response or intolerance. Full inclusion and exclusion criteria have been published previously [3, 8].
Randomization and Blinding
In COAST-V, 341 patients were randomized 1:1:1:1 to receive ixekizumab 80 mg every 2 weeks (Q2W; N = 83); ixekizumab 80 mg every 4 weeks (Q4W) (N = 81), adalimumab 40 mg Q2W (N = 90), or placebo Q2W (N = 87). In COAST-W, 316 patients were randomized 1:1:1 to receive ixekizumab 80 mg Q2W (N = 98), ixekizumab 80 mg Q4W (N = 114), or placebo Q2W (N = 104). At week 0 in both trials, patients receiving ixekizumab were randomized 1:1 to receive a starting dose of either 80 mg or 160 mg. In both trials, weeks 0–16 comprised the randomized blinded treatment period, and weeks 16–52 comprised the dose double-blind extended treatment period in which patients initially assigned to placebo (COAST-V and COAST-W) or adalimumab (COAST-V) were randomly assigned to 80 mg ixekizumab Q2W or Q4W with a starting dose of 160 mg for patients initially assigned to placebo and a starting dose of 80 mg for patients initially assigned to adalimumab. In the dose double-blind extended treatment period, patients initially assigned to ixekizumab Q2W or Q4W remained on their assigned regimen through week 52.
Outcome Measures
Work productivity was measured with the Work Productivity and Activity Impairment Questionnaire for Spondyloarthritis (WPAI-SpA), which has been validated in patients with r-axSpA [10]. The WPAI-SpA has six questions assessing the previous week to determine employment status, hours missed from work because of spondyloarthritis (SpA), hours missed from work for other reasons, hours actually worked, the degree to which SpA affected work productivity while at work, and the degree to which SpA affected activities outside of work. Scores are calculated for four domains: percentage of absenteeism, percentage of presenteeism (reduced productivity at work), an overall work impairment score combining absenteeism and presenteeism, and percentage of impairment in activities outside of work. Higher scores indicate greater impairment. WPAI scores were recorded at baseline and weeks 16 and 52. Absenteeism, presenteeism, and overall work impairment were measured in patients reporting part- or full-time paid work; activity impairment was measured in patients regardless of employment status.
Statistical Analyses
Statistical analyses were performed on data from the intent-to-treat populations of COAST-V and COAST-W comparing ixekizumab regimens and adalimumab (COAST-V) to placebo. Analysis of covariance (ANCOVA) models were used to analyze changes from baseline for work productivity measures for the blinded dosing treatment period (weeks 0–16). As independent variables, the ANCOVA models included treatment, geographic region, baseline C-reactive protein level, number of prior TNFi received (COAST-W), and WPAI baseline values. Least squared means (LSM) were reported for treatment groups during the blinded dosing treatment period (weeks 0–16). For the dose double-blind extended treatment period (weeks 16–52), means and standard deviations (SD) were reported for work productivity outcome measures. Missing data was imputed using the modified baseline observation carried forward (mBOCF) approach. All statistical testing was made at the 0.05 level without adjustment for multiple testing.
Results
Baseline Characteristics
Baseline characteristics for patients across treatment arms were generally similar among treatment groups in both trials. Patients who were TNFi-experienced (COAST-W) were older and had longer disease duration than bDMARD-naïve (COAST-V) patients [mean age 46.1 (SD 12.4) years vs. 41.7 (SD 11.7); mean disease duration 18.4 (SD 11.1) vs. 16.0 (SD 10.3) years] (Table 1). A majority of patients participated in part- or full-time paid work, with 74.1% (252/340) of bDMARD-naïve patients (COAST-V) and 57.6% (182/316) of TNFi-experienced patients (COAST-W) reporting paid employment (Table 1). WPAI scores were similar for both bDMARD-naïve and TNFi-experienced groups (Table 1). Domain scores were comparable across treatment arms (Tables 2, 3).
Changes from Baseline in Absenteeism, Presenteeism, and Overall Work Impairment
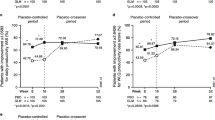
Absenteeism, presenteeism, and overall work impairment were assessed for patients reporting part- or full-time paid work. Patients treated with ixekizumab showed improvements from baseline in terms of percentage of absenteeism, percentage of presenteeism, and overall work impairment at weeks 16 and 52 [Fig. 1 and Electronic Supplementary Material (ESM) Fig. S1; Tables 4, 5]. At week 16, TNFi-experienced patients (COAST-W) treated with ixekizumab showed significant improvements in presenteeism compared to those on placebo [LSM change from baseline: − 19.5 for ixekizumab Q4W (Nx = 44) and − 22.2 for ixekizumab Q2W (Nx = 43) vs. − 8.9 for placebo (Nx = 54); p = 0.042 and p = 0.011, respectively; Nx = number of patients in the analysis subgroup] (ESM Fig. S1; Table 5). In comparison, bDMARD-naïve patients showed numeric but not significant improvements [LSM change: − 22.7 for ixekizumab Q4W (Nx = 55) and − 23.3 for ixekizumab Q2W (Nx = 47) vs. 17.7 for placebo (Nx = 50); nonsignificant difference (NS)] (ESM Fig. S1; Table 4). TNFi-experienced patients receiving ixekizumab also had significant improvements in overall work impairment compared to placebo at week 16 [LSM change: − 21.0 for ixekizumab Q4W (Nx = 44) and − 23.5 for ixekizumab Q2W (Nx = 43) vs. − 9.8 for placebo (Nx = 54); p = 0.038 and p = 0.012, respectively] (Fig. 1; Table 5), with bDMARD-naïve patients also having numeric improvements [LSM change: − 21.4 for ixekizumab Q4W (Nx = 55) and − 24.1 for ixekizumab Q2W (Nx = 47) vs. − 21.7 for placebo (Nx = 50); NS] (Fig. 1; Table 4).

Changes from baseline in Work Productivity and Activity Index for Spondyloarthritis (WPAI-SpA) scores at weeks 16 and 52. a, b Overall work impairment in bDMARD-naïve (a) and TNFi-experienced (b) patients; c, d activity impairment in bDMARD-naïve (c) and TNFi-experienced (d) patients. For week 16, values are the least squares mean (standard error) from analysis of covariance (ANCOVA) with missing data imputed via modified baseline observation carried forward (mBOCF). For week 52, values are means (standard deviation) with missing data imputed via mBOCF. At week 16, patients receiving placebo (COAST-V, bDMARD-naïve; COAST-W, TNFi-experienced) or adalimumab (COAST-V, bDMARD-naïve) were switched to ixekizumab Q4W or Q2W. Data for IXE Q4W and IXE Q2W were combined for the PBO/IXE and ADA/IXE groups. Overall work impairment was measured in patients reporting part- or full-time paid work. The sample sizes for randomized patients (intent-to-treat population) were: a, c COAST-V (bDMARD-naïve) treatment groups: PBO (N = 87) → PBO/IXE (N = 86); ADA (N = 90) → ADA/IXE (N = 86); IXE Q4W (N = 81) → IXE Q4W/IXE Q4W (N = 78); and IXE Q2W (N = 83) → IXE Q2W/IXE Q2W (N = 79). Number of patients eligible for analysis of overall work impairment: PBO (Nx = 50) → PBO/IXE (Nx = 49); ADA (Nx = 60) → ADA/IXE (Nx = 59); IXE Q4W (Nx = 55) → IXE Q4W/IXE Q4W (Nx = 57); and IXE Q2W (Nx = 47) → IXE Q2W/IXE Q2W (Nx = 49). Number of patients eligible for analysis of activity impairment: PBO (Nx = 86) → PBO/IXE (Nx = 85); ADA (Nx = 88) → ADA/IXE (Nx = 85); IXE Q4W (Nx = 80) → IXE Q4W/IXE Q4W (Nx = 78); and IXE Q2W (Nx = 83) → IXE Q2W/IXE Q2W (Nx = 79). b, d COAST-W (TNFi-experienced) treatment groups: PBO (N = 104) → PBO/IXE (N = 93); IXE Q4W (N = 114) → IXE Q4W/IXE Q4W (N = 98); and IXE Q2W (N = 98) → IXE Q2W/IXE Q2W (N = 90). Number of patients eligible for analysis of overall work impairment: PBO (Nx = 54) → PBO/IXE (Nx = 47); IXE Q4W (Nx = 44) → IXE Q4W/IXE Q4W (Nx = 42); and IXE Q2W (Nx = 43) → IXE Q2W/IXE Q2W (Nx = 43). Number of patients eligible for analysis of activity impairment: PBO (Nx = 99) → PBO/IXE (Nx = 89); IXE Q4W (Nx = 112) → IXE Q4W/IXE Q4W (Nx = 98); and IXE Q2W (Nx = 96) → IXE Q2W/IXE Q2W (Nx = 90). p values were from ANCOVA (treatment vs. placebo) for weeks 0–16. *p < 0.05, ‡p < 0.01, †p < 0.001. ADA 40 mg adalimumab every 2 weeks, bDMARD biologic disease-modifying anti-rheumatic drug, IXE Q2W 80 mg ixekizumab every 2 weeks, IXE Q4W 80 mg ixekizumab every 4 weeks, N number of patients in the treatment group, Nx number of patients eligible for analysis, PBO placebo,TNFi tumor necrosis factor inhibitor
Improvements in work productivity from baseline were sustained up to week 52 (Fig. 1, ESM Fig. S1). After switching from placebo to ixekizumab, bDMARD-naïve patients showed greater improvement as the mean change from baseline increased in magnitude: for absenteeism, − 1.0 at week 16 (Nx = 50) to − 3.9 at week 52 (Nx = 49); for presenteeism, − 21.4 at week 16 (Nx = 50) to − 31.6 at week 52 (Nx = 49); for overall work impairment, − 21.7 at week 16 (Nx = 50) to − 31.9 at week 52 (Nx = 49); and for activity impairment, − 16.4 at week 16 (Nx = 86) to − 25.6 at week 52 (Nx = 85) (Table 4). After switching from placebo to ixekizumab, TNFi-experienced patients showed greater improvement as the mean change from baseline increased in magnitude: for absenteeism, − 2.6 at week 16 (Nx = 57) to − 6.7 at week 52 (Nx = 49); for presenteeism, − 8.8 at week 16 (Nx = 54) to − 24.0 at week 52 (Nx = 47); and for overall work impairment, − 9.8 at week 16 (Nx = 54) to − 24.5 at week 52 (Nx = 47). Both bDMARD-naïve and TNFi-experienced patients randomized to ixekizumab Q4W or Q2W reported sustained improvements in absenteeism, presenteeism, and overall work impairment, with slightly greater changes from baseline at week 52 compared to week 16 (Tables 4, 5).
Changes from Baseline in Activity Impairment
Activity impairment was assessed for patients regardless of work status. Patients treated with ixekizumab had greater improvements from baseline in activity impairment at weeks 16 and 52 compared to placebo (Fig. 1; Tables 4, 5). For bDMARD-naïve patients (COAST-V) treated with ixekizumab, improvements in activity impairment were significant at week 16 [LSM change: − 23.0 for ixekizumab Q4W (Nx = 80) and − 23.4 for ixekizumab Q2W (Nx = 83) vs. − 14.1 for placebo (Nx = 86); p = 0.006 and p = 0.004, respectively] (Fig. 1; Table 4). Compared to placebo, significant improvements in activity impairment at week 16 were seen for TNFi-experienced patients treated with ixekizumab Q2W and nonsignificant improvements were seen in those treated with ixekizumab Q4W [LSM change: − 16.5 for ixekizumab Q4W (Nx = 112) and − 18.4 for ixekizumab Q2W (Nx = 96) vs. − 10.1 for placebo (Nx = 99); p = 0.071 and p = 0.024, respectively] (Fig. 1; Table 5).
In bDMARD-naïve patients who switched from placebo to ixekizumab, the mean change from baseline increased in magnitude for activity impairment from − 16.4 at week 16 (Nx = 86) to − 25.6 at week 52 (Nx = 85) (Table 4). In TNFi-experienced patients who switched from placebo to ixekizumab, the mean change from baseline increased in magnitude for activity impairment from − 8.3 at week 16 (Nx = 99) to − 21.7 at week 52 (Nx = 89) (Table 5). Both bDMARD-naïve and TNFi-experienced patients randomized to ixekizumab Q4W or Q2W reported sustained improvements in activity impairment with changes in baseline slightly greater in magnitude at week 52 than week 16 (Tables 4, 5).
Discussion
Previously published results have shown the superiority of ixekizumab compared to placebo in the treatment of patients with AS. These results have also demonstrated the safety and efficacy of ixekizumab in both bDMARD-naïve and TNFi-experienced patients with AS [3,8]. In this analysis, we have shown that treatment with ixekizumab also improved patient-reported outcomes centered on work productivity and activity impairment in bDMARD-naïve and TNFi-experienced patients with AS. In summary, improvements in presenteeism, overall work impairment, and activity impairment were seen at weeks 16 and 52, with greater numeric changes from baseline at week 52. Across all WPAI domains, the observed improvements at week 16 were sustained to week 52. Consistent with previous efficacy analyses, no apparent differences were seen between the ixekizumab Q4W and Q2W dosing regimens [11].
As an aspect of HRQoL, work productivity is associated with overall health outcomes in AS. Decreased physical functioning in patients with AS has been found to be associated with work outcome, and disease activity was found to have an independent association with presenteeism [7]. Fatigue has been shown to predict negative effects on presenteeism and overall activity impairment in etanercept-treated patients with AS [12].
The use of biologics has improved HRQoL outcomes in patients with AS [5]. In a prospective, real-world cohort of patients with AS, treatment with golimumab or infliximab for 6 months resulted in improved work productivity and activity impairment as well as fewer missed days of work [13]. Patients with AS who received secukinumab, another anti-IL-17 inhibitor, also reported improved HRQoL, including improvements in WPAI measures, through 52 weeks [14].
A previous analysis of results from three clinical trials demonstrated the effectiveness of ixekizumab in improving work productivity for patients with moderate-to-severe plaque psoriasis [15]. Ixekizumab has also been shown to improve patient-reported outcomes, including work productivity, in bDMARD-naïve and TNFi-experienced patients with psoriatic arthritis [16,17]. Here, in the context of AS, ixekizumab has demonstrated effectiveness in improving work productivity, with changes from baseline sustained up to 52 weeks. The improvements in work productivity and activity impairment seen in this analysis of two clinical trials suggest that treatment with ixekizumab can result in improved HRQoL for patients with AS.
The strengths of this study include the inclusion of both bDMARD-naïve and TNFi-experienced patients as well as a 52-week follow-up for patient-reported outcomes. Due to ethical concerns, the COAST-V and COAST-W studies did not have placebo arms through week 52, which limited this analysis. This study was also limited in the evaluation of absenteeism, presenteeism, and work productivity loss due to the requirement of being employed and, consequently, reduced sample size which did not provide adequate statistical power to detect treatment differences in comparison to placebo. While improvements in work productivity at week 16 were significant in TNFi-experienced patients (COAST-W), these were not significant in bDMARD-naïve patients (COAST-V). Both TNFi-experienced and bDMARD-naïve patients treated with ixekizumab had a similar magnitude of change from baseline in work productivity, but the bDMARD-naïve placebo group had a larger change from baseline at week 16.
Conclusions
Both bDMARD-naïve and TNFi-experienced patients with AS treated with ixekizumab had improvements in presenteeism, overall work productivity, and activity impairment compared to those treated with placebo. The improvements for these outcomes were seen at week 16, the first assessment after baseline measurements, and these improvements were sustained through week 52 of both studied trials, supporting the notion that treatment with ixekizumab can improve important aspects of HRQoL in patients with active AS.
References
Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. 2017;390(10089):73–84.
Boonen A, van der Linden SM. The burden of ankylosing spondylitis. J Rheumatol Suppl. 2006;78:4–11.
Ritchlin CT, Okada M, Cuchacovich RS, et al. Efficacy and safety of ixekizumab in patients with active psoriatic arthritis: 52-week results from a phase III study (SPIRIT-P1). Ann Rheum Dis. 2018;45(3):367–77.
Sieper J, Braun J, Dougados M, Baeten D. Axial spondyloarthritis. Nat Rev Dis Primers. 2015;1:15013.
Strand V, Singh JA. Patient burden of axial spondyloarthritis. J Clin Rheumatol. 2017;23(7):383–91.
Martindale J, Shukla R, Goodacre J. The impact of ankylosing spondylitis/axial spondyloarthritis on work productivity. Best Pract Res Clin Rheumatol. 2015;29(3):512–23.
Boonen A, Brinkhuizen T, Landewe R, van der Heijde D, Severens JL. Impact of ankylosing spondylitis on sick leave, presenteeism and unpaid productivity, and estimation of the societal cost. Ann Rheum Dis. 2010;69(6):1123–8.
Deodhar A, Poddubnyy D. Efficacy and safety of ixekizumab in the treatment of radiographic axial spondyloarthritis: sixteen-week results from a phase III randomized, double-blind, placebo-controlled trial in patients with prior inadequate response to or intolerance of tumor necrosis factor inhibitors. Arthritis Rheumatol. 2019;71(4):599–611.
Mease P, Walsh JA, Baraliakos X, et al. Translating improvements with ixekizumab in clinical trial outcomes into clinical practice: ASAS40, pain, fatigue, and sleep in ankylosing spondylitis. Rheumatol Ther. 2019;6(3):435–50.
Reilly MC, Gooch KL, Wong RL, Kupper H, van der Heijde D. Validity, reliability and responsiveness of the Work Productivity and Activity Impairment Questionnaire in ankylosing spondylitis. Rheumatology (Oxford). 2010;49(4):812–9.
Dougados M, Wei JC, Landewé R, et al. Efficacy and safety of ixekizumab through 52 weeks in two phase 3, randomised, controlled clinical trials in patients with active radiographic axial spondyloarthritis (COAST-V and COAST-W). Ann Rheum Dis. 2020;79(2):176–85.
Druce KL, Aikman L, Dilleen M, Burden A, Szczypa P, Basu N. Fatigue independently predicts different work disability dimensions in etanercept-treated rheumatoid arthritis and ankylosing spondylitis patients. Arthritis Res Ther. 2018;20(1):96.
Claudepierre P, Van den Bosch F, Sarzi-Puttini P, Vastesaeger N, Govoni M, Kachroo S. Treatment with golimumab or infliximab reduces health resource utilization and increases work productivity in patients with ankylosing spondylitis in the QUO-VADIS study, a large, prospective real-life cohort. Int J Rheum Dis. 2019;22(6):995–1001.
Deodhar AA, Dougados M, Baeten DL, et al. Effect of secukinumab on patient-reported outcomes in patients with active ankylosing spondylitis: a phase III randomized trial (MEASURE 1). Arthritis Rheumatol (Hoboken, NJ). 2016;68(12):2901–10.
Armstrong AW, Lynde CW, McBride SR, et al. Effect of ixekizumab treatment on work productivity for patients with moderate-to-severe plaque psoriasis: analysis of results from 3 randomized phase 3 clinical trials. JAMA Dermatol. 2016;152(6):661–9.
Gottlieb AB, Strand V, Kishimoto M, et al. Ixekizumab improves patient-reported outcomes up to 52 weeks in bDMARD-naive patients with active psoriatic arthritis (SPIRIT-P1). Rheumatology (Oxford). 2018;57(10):1777–888.
Kavanaugh A, Marzo-Ortega H, Vender R, et al. Ixekizumab improves patient-reported outcomes in patients with active psoriatic arthritis and inadequate response to tumour necrosis factor inhibitors: SPIRIT-P2 results to 52 weeks. Clin Exp Rheumatol. 2019;37(4):566–74.
Acknowledgements
The views expressed are those of the author and not necessarily those of the (UK) National Health Service (NHS), the NIHR, or the (UK) Department of Health.
Funding
Eli Lilly and Company provided funding for the sponsorship for this study and the journal’s Rapid Service Fee. All authors had complete access to the data used in this study and take full responsibility for the integrity of the data and accuracy of the data analysis.
Medical Writing and Editorial Assistance
Nicole Lipitz of Syneos Health provided writing and editorial assistance with funding provided by Eli Lilly and Company.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICJME) criteria for authorship of this manuscript, take responsibility for the integrity of the whole work, and have given approval for the publication of this version of the manuscript.
Disclosures
Helena Marzo-Ortega has received grant/research support from Celgene, Janssen, and Novartis; is a consultant for AbbVie, Celgene, Eli Lilly and Company, Janssen, Novartis, Pfizer, and UCB; and is a member of the speakers’ bureau for AbbVie, Celgene, Eli Lilly and Company, Janssen, Novartis, Pfizer, Takeda, and UCB. Helena Marzo-Ortega is supported by the National Institute for Health Research (NIHR) Leeds Biomedical Research Centre (LBRC). Philip J. Mease has received research grants from AbbVie, Amgen, BMS, Celgene, Janssen, Eli Lilly and Company, Novartis, Pfizer, Sun, and UCB; received consultant fees from AbbVie, Amgen, BMS, Boehringer Ingelheim, Celgene, Galapagos, Gilead, GlaxoSmithKline, Janssen, Eli Lilly and Company, Novartis, Pfizer, Sun, and UCB; and is a speaker for AbbVie, Amgen, BMS, Celgene, Genentech, Janssen, Eli Lilly and Company, Novartis, Pfizer, and UCB. Proton Rahman has not received a research grant from Eli Lilly and Company but has received consulting fees from Abbott, AbbVie, Amgen, BMS, Celgene, Eli Lilly and Company, Janssen, Novartis, and Pfizer. Victoria Navarro-Compán has received grant/research support from AbbVie, Eli Lilly and Company, MSD, Novartis, Pfizer, and UCB; is a paid consultant for AbbVie, Eli Lilly and Company, MSD, Novrtis, Pfizer, and UCB; and is a paid speaker for AbbVie, Eli Lilly and Company, MSD, Novartis, Pfizer, and UCB. Vibeke Strand is a paid consultant for Abbvie, Amgen, Biogen, Celltrion, Consortium of Rheumatology Researchers of North America, Crescendo Bioscience, Eli Lily and Company, Genentech/Roche, GlaxoSmithKline, Hospira, Janssen, Merck, Novartis, Pfizer, Regeneron Pharmaceuticals, Sanofi, and UCB. Maxime Dougados reports receiving grant/research support from AbbVie, Eli Lilly and Company, Merck, Novartis, Pfizer, and UCB Pharma; is a consultant and member of the speakers bureau for AbbVie, Eli Lilly and Company, Merck, Novartis, Pfizer, and UCB Pharma. Bernard Combe has received grant/research support from Pfizer, Novartis, and Roche-Chugai; is a paid consultant for AbbVie, Gilead, Eli Lilly and Company, Janssen, Pfizer, Roche-Chugai, Sanofi, and UCB; and is on the speakers’ bureau for BMS, Gilead, Eli Lily and Company, Merck, Pfizer, and Roche-Chugai. James Cheng-Chung Wei reports receiving consulting fees from TSH biopharm, AbbVie, BMS, Celgene, Chugai, Eisai, Janssen, Novartis, Pfizer, Sanofi-Aventis, and UCB pharma; and grant support from Abbvie, BMS, Celgene, Eli Lilly and Company, Janssen, Novartis, Pfizer, and UCB. Xenofon Baraliakos has received grant/research support from AbbVie, BMS, Chugai, Celgene, Pfizer, Galapagos, UCD, and MSD; has worked as a paid consultant for AbbVie, BMS, Chugai, Celgene, Pfizer, Galapagos, UCB, add MSD; and is a paid speaker for AbbVie, BMS, Chugai, Celgene, Pfizer, Galapagos, UCB, and MSD. Theresa Hunter, David Sandoval, Xiaoqi Li, and Baojin Zhu are employees and stockholders of Eli Lilly and Company. Louis Bessette has received grant/research support from Amgen, GMS, Janssen, UCB, AbbVie, Pfizer, Celgene, Sanofi, Lily, and Novartis; has worked as a paid consultant for Amgen, BMS, Janssen, UCB, AbbVie, Pfizer, Merck, Celgene, Sanofi, and Novartis; and was a paid speaker for Amgen, BMS, Janssen, UCB, AbbVie, Pfizer, Merck, Celgene, Sanofi, Eli Lilly and Company, and Novartis. Atul Deodhar has received grant/research support from AbbVie, Boehringer Ingelheim, Eli Lilly and Company, GlaxoSmith&Kline, Novartis, Pfizer, and UCB; and is a consultant for AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Eli Lilly and Company, Giliad, GlaxoSmith&Kline, Janssen, Novartis, Pfizer, and UCB.
Compliance with Ethics Guidelines
Ethical review boards approved COAST-V and COAST-W at each site before the trials began. Procedures involving human participants were performed within the ethical standards of the institutional and national research committees at all sites. Both trials were conducted in accordance with the standards of the Declaration of Helsinki and its later amendments. All patients gave written informed consent before undergoing procedures related to the trials. The master ethics committee was Schulman Associates IRB, Cincinnati, OH, USA; complete listings of sites and investigators are available in the supplements of previously published results from COAST-V and COAST-W [3, 8, 9].
Data Availability
The datasets analyzed in this study are available from the corresponding author upon reasonable request.
Open Access
This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
Author information
Authors and Affiliations
Corresponding author
Additional information
Digital Features
To view digital features for this article go to https://doi.org/10.6084/m9.figshare.12681980.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Marzo-Ortega, H., Mease, P.J., Rahman, P. et al. Impact of Ixekizumab on Work Productivity in Patients with Ankylosing Spondylitis: Results from the COAST-V and COAST-W Trials at 52 Weeks. Rheumatol Ther 7, 759–774 (2020). https://doi.org/10.1007/s40744-020-00225-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-020-00225-4