
Abstract
Introduction
Chronic pruritus (CP) is a common symptom defined as a sensation that provokes the desire to scratch and which lasts for at least 6 weeks. CP remains a problem for up to 21.3% of renal transplant recipients (RTRs). Our research aimed to establish the possible association between serum levels of neurotrophin-4 (NT-4) and brain-derived neurotrophic factor (BDNF) and the presence and intensity of CP in RTR.
Methods
The study was performed on a group of 129 RTRs, who were divided according to the presence or absence of pruritus in the previous 3 days. The assessment of pruritus was performed with the use of a numeric rating scale (NRS), 4-Item Itch Questionnaire (4IIQ), and Itchy Quality of Life (Itchy QoL). A total of 129 blood samples with a volume of 9 ml were drawn from RTRs during the monthly routine control. Serum levels (pg/mL) of NT-4 and BDNF were measured by the ELISA.
Results
Pruritic RTRs have statistically significantly higher serum concentrations of NT-4 serum level compared to non-pruritic RTRs (229.17 ± 143.86 pg/mL and 153.08 ± 78.19 pg/mL [p = 0.024], respectively). Moreover, a statistically significant difference between pruritic and non-pruritic RTRs with healthy controls was shown (p < 0.001 and p < 0.001, respectively). Although there was a numerically higher serum concentration of BDNF in pruritic RTRs (32.18 ± 7.31 pg/mL vs. 31.58 ± 10.84 pg/mL), the difference did not reach statistical significance. No statistically significant difference was also seen in BDNF serum levels between RTRs and healthy controls. Furthermore, there was a statistically significant, positive correlation between serum concentration of NT-4 and NRS score (p = 0.008, r = 0.357).
Conclusions
The results indicate higher NT-4 serum concentration in RTRs with pruritus compared to RTRs without pruritus. Furthermore, the study revealed a statistically significant, positive correlation between the serum concentration of NT-4 and NRS score.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Chronic pruritus remains a problem for up to 21.3% of renal transplant recipients (RTRs). |
The pathogenesis of chronic pruritus in RTRs remains unknown. |
Data on the association of neurotrophin-4 (NT-4) and brain-derived neurotrophic factor (BDNF) with pruritus is limited. |
Serum levels of NT-4 are statistically higher in pruritic RTRs in comparison to non-pruritic RTRs and healthy controls. |
Serum levels of NT-4 correlate positively with pruritus severity assessed with numeric rating scale (NRS). |
There are no differences between BDNF serum levels between pruritic and non-pruritic RTRs, as well as healthy controls. |
Further research is warranted on the inhibition of NT-activated neuronal sensory pathways as a promising treatment modality. |
Introduction
Chronic pruritus (CP) is a common symptom defined as a sensation that provokes the desire to scratch and which lasts for at least 6 weeks. It affects approximately 13.5% of the general adult population, and its prevalence increases with age [1]. However, the epidemiological data on CP are still limited and vary depending on sources [1, 2]. CP may be a consequence of both dermatological and systemic disorders such as metabolic, endocrine, infective, hematological, neurological, psychiatric, or psychosomatic disease [1]. Notwithstanding, up to 20% of CP is of undetermined origin [1]. One of the specific types of CP is chronic kidney disease-associated pruritus (CKD-aP), also known as uremic pruritus. CKD-aP can affect up to 13% of patients with CKD at every stage (worsens as kidney function decreases) and up to 60% of patients during hemodialysis (HD) [3, 4]. The pathophysiology of CKD-aP remains unclear. Among factors potentially involved in the development of CKD-aP, authors distinguish the following disturbances: microinflammation; increased level of parathyroid hormone; increased concentration of histamine and tryptase; increased concentration of calcium and magnesium; neuropathy; altered opioid transmission; xerosis; infectious agents; immune dysfunction; dialysis-associated aspects [5,6,7,8,9,10,11]. Moreover, increased concentrations of uremic toxins such as p-cresyl sulfate and indoxyl sulfate conceivably may play a role in the underlying mechanism of CKD-aP [1]. Researchers from our center focused on recent studies on serum levels of interleukin (IL)-31 and neurotrophin-4 in patients with CKD-aP requiring HD, proving that their concentrations are significantly higher in this particular group [12, 13]. Moreover, a recent study demonstrated that disturbance in the balance between the concentrations of the individual components of the opioid system might lead to the development of pruritus or modulate it in patients requiring HD [14].
According to current medical knowledge, renal transplantation (RTx) comprises the best renal replacement therapy, improving quality-of-life and decreasing mortality rates [15]. Notwithstanding, the associated pruritus remains a problem for up to 21.3% of renal transplant recipients (RTRs) [15]. It should be emphasized that, according to our study, pruritus in the majority of pruritic RTR develops after RTx [4]. Both the prevalence and intensity of CKD-aP in RTR are not dependent on comorbidities, graft function, electrolyte disturbance, or chronic inflammation [4]. The pathomechanism of CKD-aP in RTR seems to be even more complex and unclear. Uremic toxins, which are often said to be responsible for the development of CKD-aP, are at much lower levels after successful RTx [11, 16]. Furthermore, our group has proven the association between IL-31 levels and CP in patients after renal transplantation [17].
As a result of the lack of fully explored and understood pathomechanism of CP in RTR, treatment of pruritus in those groups is based on very limited data and seems unsatisactory for both patients and clinicians. Our research aimed to establish the possible association between serum levels of neurotrophin-4 (NT-4) and brain-derived neurotrophic factor (BDNF) and presence and intensity of CP in RTR.
Methods
Study Design and Participants
The study was conducted in accordance with the Declaration of Helsinki and received ethical approval from Wroclaw Medical University Institutional Review Board (KB-750/2021). All included patients provided their informed consent. The study had a protocol-based interventional character and was performed between March and November 2021 in the Department of Nephrology and Transplantation Medicine of Wroclaw Medical University, Wroclaw, Poland.
A total of 129 RTRs were enrolled on the basis of inclusion and exclusion criteria. Each participant of the study had to be an adult with a functioning renal transplant. All included patients were examined by a doctor trained in the assessment of pruritus. During the examination, patients with chronic dermatological disorders, as well as any other disorder which may have resulted in the development of pruritus, were excluded. Subsequently, a thorough medical history was taken with an emphasis on any itching disorder that may have biased the results. Later, various demographic and clinical data such as sex, age, BMI, disease duration, time on dialysis, time after RTx, atopic predilection, and family history were collected for analysis. All kidney recipients were divided into two groups depending on the absence or presence of chronic CP in the preceding 3 days. After the collection of a sufficient number of RTRs without pruritus, consecutive RTRs with pruritus were collected in order to create two similar groups. Subsequently, 47 healthy volunteers formed a control group from the Wroclaw Blood Donation Center.
Pruritus and Psychosocial Assessment
To assess the intensity of pruritus, the numeric rating scale (NRS), and the 4-Item Itch Questionnaire (4IIQ) were implemented [18, 19]. The 11-point NRS enables pruritus severity assessment according to the following scheme: 0 points, no pruritus; 1–2 points, mild pruritus; 3–6 points, moderate pruritus; 7–8 points, severe pruritus; and ≥ 9 points, very severe pruritus [18]. The 4IIQ is a validated tool not only to assess the intensity of pruritus but also allow to determine its frequency and sleep impairment. For each of the 6-point scales, 0 points correspond to the absence of a given parameter, and 5 points indicate the most severe pruritus, the highest frequency, and the greatest sleep disturbance due to pruritus, respectively [19]. Finally, the Itchy Quality of Live (Itchy Qol) was employed. Itchy Qol is a questionnaire used to evaluate the quality of life in patients with chronic pruritus. It consists of 22 items, divided into three categories: symptoms, functioning, and emotions. The frequent items are scored on a scale from 1 (never), through 2 (rarely), 3 (sometimes), and 4 (often) to 5 (all the time). The bother items are scored on a scale from 1 (no bothered), through 2 (little bothered), 3 (somewhat bothered), and 4 (very bothered) to 5 (severely bothered). The results are presented as scores from individual categories and overall scores [20].
Laboratory Tests
A total of 129 blood samples with a volume of 9 ml were drawn from RTRs during the monthly routine control. The samples were centrifuged at 3000×g for 15 min. Then, the obtained serum was stored at − 80 °C. Subsequently, the serum level (pg/mL) of NT-4 and BDNF were measured by ELISA (enzyme-linked immunosorbent assay) using the commercially available Nori Human NT-4 ELISA Kit (catalog number GR111502, Genorise Scientific, Inc., Pennsylvania, PA, USA) and Nori Human BDNF ELISA Kit (catalog number GR111085, Genorise Scientific, Inc., Pennsylvania, PA, USA). Every procedure was performed according to the manufacturer’s instructions. The absorbance was measured by EPOCH multiplate reader (BioTEK® Instruments, Inc., Winooski, VT, USA) at a wavelength of 450 nm.
Statistical Analysis
The statistical analysis was perfumed using the IBM SPSS Statistics v. 26 software (SPSS Inc., Chicago, IL, USA). Primarily, all data were examined to determine whether or not they followed a normal distribution. Quantitative data analysis required the use of the Mann–Whitney U test and either Pearson or Spearman correlations. The Kruskal–Wallis test with Bonferroni correction was applied to distinguish differences in concentration of NT-4 and BDNF in each of the three groups. Multiple regression analyses of NT-4 and BDNF on itch were adjusted for gender, age, duration of the disease, dialysis, and time after renal transplantation in order to examine the partial correlations. Qualitative results were assessed using the chi-square test. Data were presented as minimum, maximum, mean ± SD, median, and first and third quantiles, with statistical significance at p < 0.05.
Results
Baseline Characteristics
The study group consisted of 129 RTRs, 74 men (57.4%) and 55 women (42.6%), with an average age of 52.01 ± 13.54 years. The group was considered somewhat overweight with an average BMI of 25.92 ± 5.3 kg/m2. The mean duration of CKD was 19.90 ± 12.23 years. On average, patients spent 2.38 ± 1.97 years on dialysis, and were 7.77 ± 7.10 years after RTx. Atopy was reported by 21 (16.3%), and positive family history of atopy by 22 responders (17.1%). Pruritus was experienced by 46 patients (35.7%) during dialysis, and 70 (54%) patients after RTx. Thirty responders (42.86%) claimed that the pruritus had post-transplant character. Post-dialysis persistent CP was observed in 40 patients (57.14%); 33 patients (82.5%) assessed the severity of pruritus after RTx as lower, while 7 patients (17.5%) reported it to be the same as during the hemodialysis period.
The patients were divided into two groups (pruritic and non-pruritic RTRs) depending on the presence of pruritus in the preceding 3 days. The differences in demographics between the two groups are presented in Table 1.
Pruritus Assessment
The pruritus assessment in pruritic RTRs indicates the presence of moderate pruritus with an average score of 4.98 ± 2.41 points, with no statistically significant difference between male and female patients. According to NRS, most frequently patients reported mild pruritus (21 patients, 38.9%), followed by moderate pruritus (20 patients, 37%), severe pruritus (7 patients, 13%), and very severe pruritus (6 patients, 11.1%). According to 4IIQ, pruritus was on average rated at 6.61 ± 2.51 points, with no statistically significant difference between sexes. The mean score of Itchy QoL Overall was 41.76 ± 16.05, likewise with no statistically significant difference between male and female patients (Table 2).
Serum Level of NT-4 and BDNF
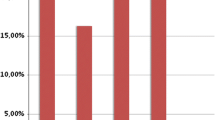
The results of the study showed that pruritic RTRs have statistically significantly higher serum concentrations of NT-4 serum level compared to non-pruritic RTRs (229.17 ± 143.86 pg/mL and 153.08 ± 78.19 pg/mL [p = 0.024], respectively) (Fig. 1). Moreover, a statistically significant difference between pruritic and non-pruritic RTRs with healthy controls was shown (p < 0.001 and p < 0.001, respectively). Although there was a numerically higher serum concentration of BDNF in pruritic RTRs (32.18 ± 7.31 pg/mL vs. 31.58 ± 10.84 pg/mL) (Fig. 1), the difference did not reach statistical significance. No statistically significant difference was also seen in BDNF serum levels between RTRs and healthy controls (Table 3).

Differences in serum concentrations of a neurotrophin-4 and b brain-derived neurotrophic factor in renal transplant recipients
Furthermore, there was a statistically significant, positive correlation between serum concentration of NT-4 and NRS score (p = 0.008, r = 0.357) (Fig. 2). No statistically significant correlation was found between NT-4 serum level and 4IIQ score. We were unable to find significant relationships between pruritus intensity (all methods evaluating pruritis intensity) and Itchy QoL (p > 0.05). BDNF serum concentration did not correlate with any scores used for the assessment of pruritus intensity (p > 0.05).

Correlation between serum levels of neurotrophin-4 and pruritus assessed with the numeric rating scale (NRS)
On multiple linear regression NT-4 showed a significant association with itch intensity assessed by NRS (p = 0.01) with a standardized coefficient beta of 0.357. There was no such association visible for BDNF.
Discussion
Neurotrophins (NTs) are defined as a family of signaling molecules, similar in sequence and structure, that play relevant roles in nervous system development, survival, and function [21]. Thus far, four NTs have been identified in mammals: nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), neurotrophin-3 (NT-3), and neurotrophin-4 (NT-4) [21]. The multifunctional character of NTs has been the subject of research for decades. Through the Trk receptors and p75NTR, NTs activate a wide range of signaling pathways [21]. NTs have the ability to control a number of surviving neurons, regulate axon growth, dendrite pruning, innervation pattering, and expression proteins such as neurotransmitters and ion channels.
Moreover, NTs in the mature nervous system are responsible for the plasticity of nerves, resulting in shape and physiology changes, but also indicate the ability to modulate synaptic processes, such as neurotransmitter secretion [22, 23]. The contribution of NTs to dermatological conditions remains unclear. However, researchers constantly investigate their role in numerous skin disorders, including pruritus.
NT-4 is the most recently discovered NTs in mammals which makes it also considered the least studied. The ubiquitous expression of NT-4 distinguishes NT-4 from other NTs. Timmusk et al. [24] found NT-4 mRNA expression in every 12 examined peripheral rat organs, including the skin [24]. Moreover, NT-4 expression seems to be less influenced by environmental signals than other NTs. There are few very specific reports of NT-4 expression regulation, such as the effects of mitogens and mediators of inflammation on immunocompetent cells and the effect of vitamin D3 on cultured astrocytes [25]. Furthermore, skeletal muscle expression depends on muscle activity. The activity of innervating motor neurons increases NT-4 production, which provides trophic support [26].
Available studies about the contribution of NT-4 to skin disease associated with pruritus are very limited [27]. According to Grewe et al.’s [28] study conducted in 2000, keratinocytes activated by interferon-γ have the ability to express NT-4 [28]. Moreover, intense epidermal staining was observed in the prurigo lesions of atopic dermatitis (AD) skin. In 2007, Chang et al. [29] recruited 152 patients with chronic plaque-type psoriasis to evaluate the expression of various neuropeptides. Their results did not reveal any differences in NT-4 serum level between pruritic and non-pruritic groups [29]. The study by Sorour et al. [30], published in 2019, reported that patients diagnosed with CKD-aP had significantly higher NT-4 levels compared to controls and established a correlation between NT-4 and the severity of CKD-aP. A 2022 study performed by Wala-Zielinska et al. [12] on 126 subjects requiring HD showed elevated serum levels of NT-4 in patients with chronic pruritus. Nevertheless, no significant correlation was found between pruritus intensity and NT-4 concentration [12]. Our study aimed to establish whether a similar dependency in RTR can be observed. Our results showed that RTRs with CP are characterized by significantly higher NT-4 serum concentration than RTRs without pruritus and healthy controls. Furthermore, positive correlations between serum level of NT-4 and pruritus severity, measured by NRS, was proven. On the basis of our research and the articles mentioned above, one may conclude that NT-4 contributes to CKD-aP development in patients with CKD before dialysis, undergoing dialysis, and CP after RTx [12, 30]. However, further research is needed to determine the exact pathogenetic mechanism of CP in those individual groups.
Slightly more studies are available on the role of BDNF in dermatological disorders connected with pruritus. Notwithstanding, they show numerous discrepancies. In 2005, Raap et al. [31] aimed to assess BDNF levels and TrkB expression in patients with AD. The study revealed the functional role of BDNF in eosinophils, presumably mediated by increased expression of BDNF receptors. Patients with AD showed higher concentrations of BDNF in serum, plasma, eosinophils, and supernatants of stimulated eosinophils compared to the control group [31]. Hon et al. [32] recruited 28 patients with AD under 18 years of age to not only measure the concentration of BDNF but also to assess the SCORing Atopic Dermatitis (SCORAD) index and quality of life with the Children’s Dermatology Life Quality Index (CDLQI). Furthermore, using a DigiTrack monitor, researchers recorded dominant limb motion while patients slept. The study demonstrated a correlation between BDNF serum level, SCORAD index, and quality of life scores. Furthermore, a strong correlation with nocturnal wrist movements was observed, which authors interpreted as a possible result/outcome of BDNF-induced pruritus [32]. According to a study conducted in 2009 by Ma et al. [33], serum BDNF level correlated with the severity of AD in adults, evaluated by SCORAD index [33]. In 2016, Folster-Holst et al. [34] also confirmed increased serum levels of BDNF in children with AD [34]. Rossing et al.’s 2011 study performed on 50 adult patients with chronic spontaneous urticaria (CSU) revealed a higher serum concentration of BDNF in this group compared to healthy subjects [35]. Nevertheless, there was no difference in the expression of TrkB between CSU and controls [35]. Regarding psoriasis, Nakamura et al. [36] in 2003 described a lack of difference in BDNF expression in 38 patients with psoriasis vulgaris divided into two groups according to the presence or absence of pruritus [36]. On the other hand, Brunoni et al. [37] and Sjahriri et al. [38] showed decreased BDNF serum concentration in psoriasis compared to the healthy controls [37, 38]. Regarding BDNF levels in patients with CKD, the literature showed significant differences in the results of studies. According to some authors, BDNF expression was higher in patients with CKD both before and during HD [30, 39,40,41]. As NTs not only play a relevant role in glomerular development, morphology, and function but also efficiently repair podocyte damage, their serum concentration may be higher in the case of renal impairment [40, 41]. Notwithstanding, Sorour et al. [30] did not establish any difference in BDNF serum levels between patients with CKD-aP, without CKD-aP, and the healthy control group [30]. What is more, Zoladz et al. [42] claimed that according to their research, BDNF level in patients requiring HD was even lower than in healthy subjects [42]. The authors suggest that this condition may be a consequence of enhanced oxidative stress induced by HD [42]. In the case of diabetic nephropathy, BDNF plasma level happened to be significantly elevated compared to CKD with different origins [40]. The results of our study do not demonstrate any significant difference in BDNF concentration in patients divided according to the presence and absence of CP in the preceding 3 days. Available data on the aforementioned issue are insufficient to state BDNF’s involvement in the mechanism of CKD-aP.
As a result of limited knowledge about the underlying mechanism of CKD-aP, its treatment usually remains ineffective and unsatisfactory for both patients and clinicians. Recently approved by US Food and Drug Administration (FDA), difelikefalin is a synthetic agonist of the kappa opioid receptor used in moderate-to-severe pruritus. Studies proved that, by reducing pruritus intensity, difelikefalin improves the quality of life for patients with CKD-aP. However, the lack of data about its long-term effectiveness is a limitation that further research needs to overcome [43]. The search for alternative CKD-aP treatment is still ongoing. NTs receptors are a promising direction to explore a potential therapy. Thus far, none of the TrkB receptor antagonists has been considered a possible cure for CKD-aP in clinical trials. However, pegkantratinib (CT327, SNA-120), an antagonist of TrkA (the high-affinity NGF receptor), has been tested to treat pruritus in patients with AD or psoriasis [44]. The use of pegkantratinib ointment has already shown effectiveness in reducing pruritus in patients with psoriasis [44].
We understand the limitations of our study. Firstly, this is a single-center study with a limited number of RTRs. Moreover, our assessment only included NT-4 and BDNF; further research, with the inclusion of the rest of NTs, as well as IL-4, IL-13, and B-type natriuretic peptide (BNP), is needed to fully elucidate their involvement in CP in this group of patients.
Conclusions
To the best of our knowledge, this is the first study evaluating NT-4 and BDNF serum levels in RTRs. The results indicate higher NT-4 serum concentration in RTRs with pruritus compared to RTRs without pruritus. Furthermore, the study revealed a statistically significant, positive correlation between the serum concentration of NT-4 and NRS score. No relationship between BDNF serum level and the occurrence of CP in RTRs was shown. In light of the aforementioned results and the possible involvement of NTs in the pathomechanism of CP in patients with CKD and RTRs, further research is warranted on the inhibition of NT-activated neuronal sensory pathways as a promising treatment modality.
Data Availability
The data that support the findings of this study are available from the corresponding author on reasonable request and with permission of all the authors. The data are not publicly available due to reasons of sensitivity and other reasons.
References
Weisshaar E, Szepietowski JC, Dalgard FJ, et al. European S2k guideline on chronic pruritus. Acta Derm Venereol. 2019;99(5):469–506.
Stander S, Schafer I, Phan NQ, et al. Prevalence of chronic pruritus in Germany: results of a cross-sectional study in a sample working population of 11,730. Dermatology. 2010;221(3):229–35.
Hayani K, Weiss M, Weisshaar E. Clinical findings and provision of care in haemodialysis patients with chronic itch: new results from the German epidemiological haemodialysis itch study. Acta Derm Venereol. 2016;96(3):361–6.
Krajewski PK, Olczyk P, Krajewska M, Krajewski W, Szepietowski JC. Clinical characteristics of itch in renal transplant recipients. Front Med (Lausanne). 2020;7: 615334.
Stahle-Backdahl M, Hagermark O, Lins LE, Torring O, Hilliges M, Johansson O. Experimental and immunohistochemical studies on the possible role of parathyroid hormone in uraemic pruritus. J Intern Med. 1989;225(6):411–5.
Gill DS, Fonseca VA, Barradas MA, Balliod R, Moorhead JF, Dandona P. Plasma histamine in patients with chronic renal failure and nephrotic syndrome. J Clin Pathol. 1991;44(3):243–5.
Dugas-Breit S, Schopf P, Dugas M, Schiffl H, Rueff F, Przybilla B. Baseline serum levels of mast cell tryptase are raised in hemodialysis patients and associated with severity of pruritus. J Dtsch Dermatol Ges. 2005;3(5):343–7.
Duque MI, Thevarajah S, Chan YH, Tuttle AB, Freedman BI, Yosipovitch G. Uremic pruritus is associated with higher kt/V and serum calcium concentration. Clin Nephrol. 2006;66(3):184–91.
Kimmel M, Alscher DM, Dunst R, et al. The role of micro-inflammation in the pathogenesis of uraemic pruritus in haemodialysis patients. Nephrol Dial Transplant. 2006;21(3):749–55.
Blachley JD, Blankenship DM, Menter A, Parker TF 3rd, Knochel JP. Uremic pruritus: skin divalent ion content and response to ultraviolet phototherapy. Am J Kidney Dis. 1985;5(5):237–41.
Reszke R, Kilis-Pstrusinska K, Szepietowski JC. Chronic kidney disease-associated itch (CKD-aI) in children—a narrative review. Toxins (Basel). 2021;13(7):450.
Wala-Zielinska K, Swierczynska-Mroz K, Krajewski PK, Nowicka-Suszko D, Krajewska M, Szepietowski JC. Elevated level of serum neurotrophin-4, but not of brain-derived neurotrophic factor, in patients with chronic kidney disease-associated pruritus. J Clin Med. 2022;11(21):6292.
Swierczynska K, Krajewski PK, Nowicka-Suszko D, Bialynicki-Birula R, Krajewska M, Szepietowski JC. The serum level of IL-31 in patients with chronic kidney disease-associated pruritus: what can we expect? Toxins (Basel). 2022;14(3):197.
Wala-Zielinska K, Swierczynska-Mroz K, Krajewski PK, Nowicka-Suszko D, Krajewska M, Szepietowski JC. Endogenous opioid imbalance as a potential factor involved in the pathogenesis of chronic kidney disease-associated pruritus in dialysis patients. J Clin Med. 2023;12(7):2474.
Krajewski PK, Tyczynska K, Bardowska K, Olczyk P, Krajewska M, Szepietowski JC. Psychosocial burden of itch among renal transplant recipients. Toxins (Basel). 2022;14(5):320.
Te-Linde E, van Roij CJM, Meijers BKI, De Loor H, Kessels RPC, Wetzels JFM. Cognitive function and uremic toxins after kidney transplantation: an exploratory study. Kidney 360. 2020;1(12):1398–406.
Krajewski PK, Tyczynska K, Bardowska K, et al. High serum IL-31 concentration is associated with itch among renal transplant recipients. J Clin Med. 2022;11(15):4309.
Reich A, Chatzigeorkidis E, Zeidler C, et al. Tailoring the cut-off values of the visual analogue scale and numeric rating scale in itch assessment. Acta Derm Venereol. 2017;97(6):759–60.
Reich A, Mędrek K, Szepietowski J. Czteropunktowy kwestionariusz oceny świądu – walidacja kwestionariusza. Dermatol Rev/Przegląd Dermatologiczny. 2012;99(5):600–4.
Desai NS, Poindexter GB, Monthrope YM, Bendeck SE, Swerlick RA, Chen SC. A pilot quality-of-life instrument for pruritus. J Am Acad Dermatol. 2008;59(2):234–44.
Dechant G, Neumann H. Neurotrophins. Adv Exp Med Biol. 2002;513:303–34.
Berninger B, Poo M. Exciting neurotrophins. Nature. 1999;401(6756):862–3.
Huang EJ, Reichardt LF. Neurotrophins: roles in neuronal development and function. Annu Rev Neurosci. 2001;24:677–736.
Timmusk T, Belluardo N, Metsis M, Persson H. Widespread and developmentally regulated expression of neurotrophin-4 mRNA in rat brain and peripheral tissues. Eur J Neurosci. 1993;5(6):605–13.
Ibanez CF. Neurotrophin-4: the odd one out in the neurotrophin family. Neurochem Res. 1996;21(7):787–93.
Brady ST, Siegel GJ, Albers RW, Price DL, Benjamins J. Basic neurochemistry: principles of molecular, cellular and medical neurobiology. 8th ed. Amsterdam: Elsevier/Academic; 2012.
Damiani G, Kridin K, Pacifico A, et al. Antihistamines-refractory chronic pruritus in psoriatic patients undergoing biologics: aprepitant vs antihistamine double dosage, a real-world data. J Dermatol Treat. 2022;33(3):1554–7.
Grewe M, Vogelsang K, Ruzicka T, Stege H, Krutmann J. Neurotrophin-4 production by human epidermal keratinocytes: increased expression in atopic dermatitis. J Invest Dermatol. 2000;114(6):1108–12.
Chang SE, Han SS, Jung HJ, Choi JH. Neuropeptides and their receptors in psoriatic skin in relation to pruritus. Br J Dermatol. 2007;156(6):1272–7.
Sorour NE, Elesawy FM, Tabl HA, Ibrahim ME, Akl EM. Evaluation of serum levels of neurotrophin 4 and brain-derived nerve growth factor in uremic pruritus patients. Clin Cosmet Investig Dermatol. 2019;12:109–14.
Raap U, Goltz C, Deneka N, et al. Brain-derived neurotrophic factor is increased in atopic dermatitis and modulates eosinophil functions compared with that seen in nonatopic subjects. J Allergy Clin Immunol. 2005;115(6):1268–75.
Hon KL, Lam MC, Wong KY, Leung TF, Ng PC. Pathophysiology of nocturnal scratching in childhood atopic dermatitis: the role of brain-derived neurotrophic factor and substance P. Br J Dermatol. 2007;157(5):922–5.
Ma L, Gao XH, Zhao LP, et al. Brain-derived neurotrophic factor gene polymorphisms and serum levels in Chinese atopic dermatitis patients. J Eur Acad Dermatol Venereol. 2009;23(11):1277–81.
Folster-Holst R, Papakonstantinou E, Rudrich U, et al. Childhood atopic dermatitis-brain-derived neurotrophic factor correlates with serum eosinophil cationic protein and disease severity. Allergy. 2016;71(7):1062–5.
Rossing K, Novak N, Mommert S, et al. Brain-derived neurotrophic factor is increased in serum and skin levels of patients with chronic spontaneous urticaria. Clin Exp Allergy. 2011;41(10):1392–9.
Nakamura M, Toyoda M, Morohashi M. Pruritogenic mediators in psoriasis vulgaris: comparative evaluation of itch-associated cutaneous factors. Br J Dermatol. 2003;149(4):718–30.
Brunoni AR, Lotufo PA, Sabbag C, Goulart AC, Santos IS, Bensenor IM. Decreased brain-derived neurotrophic factor plasma levels in psoriasis patients. Braz J Med Biol Res. 2015;48(8):711–4.
Sjahrir M, Roesyanto-Mahadi ID, Effendy E. Correlation between serum brain-derived neurotrophic factor level and depression severity in psoriasis vulgaris patients. Open Access Maced J Med Sci. 2019;7(4):583–6.
Li M, Armelloni S, Zennaro C, et al. BDNF repairs podocyte damage by microRNA-mediated increase of actin polymerization. J Pathol. 2015;235(5):731–44.
Endlich N, Lange T, Kuhn J, et al. BDNF: mRNA expression in urine cells of patients with chronic kidney disease and its role in kidney function. J Cell Mol Med. 2018;22(11):5265–77.
Shin SJ, Yoon HE, Chung S, Kim YG, Kim DJ. Plasma brain-derived neurotrophic factor in hemodialysis patients. Int J Med Sci. 2012;9(9):772–7.
Zoladz JA, Smigielski M, Majerczak J, et al. Hemodialysis decreases serum brain-derived neurotrophic factor concentration in humans. Neurochem Res. 2012;37(12):2715–24.
Fugal J, Serpa SM. Difelikefalin: a new kappa-opioid receptor agonist for the treatment of hemodialysis-dependent chronic kidney disease-associated pruritus. Ann Pharmacother. 2023;57(4):480–8.
Roblin D, Yosipovitch G, Boyce B, et al. Topical TrkA kinase inhibitor CT327 is an effective, novel therapy for the treatment of pruritus due to psoriasis: results from experimental studies, and efficacy and safety of CT327 in a phase 2b clinical trial in patients with psoriasis. Acta Derm Venereol. 2015;95(5):542–8.
Acknowledgements
We thank the participants of this study.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Funding
The study was funded by a research grant from Wroclaw Medical University (SUBZ.C260.23.041). No funding or sponsorship was received for the publication of this article.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Kinga Tyczyńska, Dariusz Janczak, Hanna Augustyniak-Bartosik and Magdalena Krajewska. Laboratory tests were performed by Danuta Nowicka-Suszko. The first draft of the manuscript was written by Kinga Tyczyńska, Piotr K Krajewski and Jacek C Szepietowski and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors do not have any conflict of interest regarding this work.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki of 1964 and received ethical approval from Wroclaw Medical University Institutional Review Board (KB-750/2021). All included patients provided their informed consent.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Tyczyńska, K., Krajewski, P.K., Nowicka-Suszko, D. et al. Neurotrophin-4 and Brain-Derived Neurotrophic Factor Serum Levels in Renal Transplant Recipients with Chronic Pruritus. Dermatol Ther (Heidelb) 13, 2785–2796 (2023). https://doi.org/10.1007/s13555-023-01029-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-023-01029-4