
Abstract
Background
Waiting five to six minutes before measuring a train-of-four (TOF) after a 50-Hz tetanic stimulation or post-tetanic count (PTC) in order to allow the facilitation of transmission to subside is commonly recommended but is based on limited evidence. The purpose of this study was to measure the TOF responses after PTC in one hand and to compare the responses with those in the contralateral (control) hand.
Methods
Twenty-two adult patients undergoing elective surgery under opioid-desflurane anesthesia were fitted with sensors to measure displacement of their thumbs in response to ulnar nerve stimulation. Rocuronium 0.6 mg·kg−1 was administered and TOF stimulation was applied to both sides. One side was randomized to PTC (50-Hz tetanus followed by a three-second pause and 15 1-Hz stimuli) when the opposite (control) side recovered to 10% first twitch (T1) height. Train-of-four stimulation was continued bilaterally every 20 sec until 30 min after PTC. Comparisons of the T1 and TOF ratio (T4/T1) were made at two, five, ten, 20, and 30 min.
Results
The mean (standard deviation [SD]) T1 value in the PTC arm was 11.8 (7.1)% just before PTC. The T1 values were significantly greater in the PTC arm at two, five, and ten minutes, with mean (SD) differences of 6.3 (6.7)%, 9.4 (6.8)%, and 7.4 (3.9)%, respectively (P = 0.008). There were no significant differences in T1 values between groups at 20 and 30 min, and no statistically significant differences in T4/T1 values at any time.
Conclusion
A small but clinically insignificant increase in T1 is seen for at least ten minutes after PTC without any detectable change in T4/T1 values. The TOF responses are reliable as early as one minute after PTC.
Résumé
Contexte
Le fait d’attendre cinq à six minutes avant de mesurer un train-de-quatre (TdQ) après une stimulation tétanique de 50 Hz ou un compte post-tétanique (PTC) afin de permettre à la facilitation de transmission de diminuer est une pratique souvent recommandée, mais qui ne se fonde que sur des données probantes limitées. L’objectif de cette étude était de mesurer les réponses au TdQ après un PTC dans une main et de comparer ces réponses à celles observées dans la main contralatérale (témoin).
Méthode
Nous avons placé des senseurs sur vingt-deux patients adultes subissant une chirurgie non urgente sous anesthésie combinant opioïdes et desflurane afin de mesurer le déplacement de leurs pouces en réponse à une stimulation du nerf cubital. Nous leur avons administré 0,6 mg·kg−1 de rocuronium et la stimulation en TdQ a été appliquée des deux côtés. Un côté a été randomisé à un PTC (tétanos à 50 Hz suivi d’une pause de 3 sec puis 15 stimuli à 1 Hz), alors que l’autre côté (témoin) récupérait jusqu’à 10% de l’intensité de la première contraction (T1). La stimulation en train-de-quatre a été poursuivie bilatéralement toutes les 20 sec jusqu’à 30 min après le PTC. Des comparaisons du ratio entre la T1 et le TdQ (T4/T1) ont été effectuées à deux, cinq, dix, 20 et 30 min.
Résultats
La valeur moyenne (écart type [ÉT]) de T1 dans le bras PTC était de 11,8 (7,1) % juste avant le PTC. Les valeurs de T1 étaient significativement plus élevées dans le bras PTC à deux, cinq et dix minutes, avec des différences moyennes (ÉT) de 6,3 (6,7) %, 9,4 (6,8) % et 7,4 (3,9) %, respectivement (P = 0,008). Aucune différence n’a été observée dans les valeurs de T1 entre les groupes à 20 et 30 min, et aucune différence significative d’un point de vue statistique n’a été observée entre les valeurs T4/T1 non plus, à quelque moment que ce soit.
Conclusion
Une augmentation légère mais non significative d’un point de vue clinique de la valeur T1 est observée pour au moins dix minutes après le PTC, sans changement détectable des valeurs de T4/T1. Les réponses au TdQ sont fiables dès une minute après le PTC.
Similar content being viewed by others


Use of the post-tetanic count (PTC) is recommended to assess profound neuromuscular blockade when there is no response to train-of-four (TOF) stimulation.1-6 The principle behind this monitoring modality is based on the view that prolonging high frequency stimulation for a few seconds can produce enhanced neuromuscular transmission which continues after the stimulation is withdrawn.1 This phenomenon is called post-tetanic facilitation. With the PTC mode of stimulation, a 50-Hz tetanus is applied for five seconds, stimulation is interrupted for three seconds, and then a series of 15-20 impulses is given at a frequency of 1 Hz. When no twitch or TOF response is present before applying PTC, one or several twitch responses may be seen in response to 1-Hz stimulation after the 50-Hz tetanus, due to post-tetanic facilitation. The number of visible PTC responses is inversely related to the depth of the blockade, and it can be used as a guide either to predict the time remaining until recovery of visible TOF response1-6 or to determine the dose of sugammadex or other reversal agents required for adequate reversal.7
The PTC technique relies on inducing a transient improvement of neuromuscular transmission in the monitored muscle, usually the adductor pollicis. It follows that an artificial recovery is produced only in that muscle and that subsequent responses to single or TOF stimulation might be spuriously elevated. Thus, it is important to determine the duration of the phenomenon to avoid falsely optimistic assessments of recovery in the minutes following application of PTC. Most studies have been performed with a six-minute delay between successive PTC stimulation without any firm evidence for the value.1-6 Using the contralateral arm as control, Motamed et al. found that repeating PTC every three minutes did not affect the time course of recovery during atracurium blockade.8 Their findings contrast with those of Feldman et al. who reported that, when an extremity is subjected to repeated tetanic stimulation, neuromuscular function remains enhanced when compared with the contralateral (control) arm.9 Silverman and Brull evaluated the neuromuscular response in a constant vecuronium-induced neuromuscular blockade, and they suggested that neuromuscular transmission returns to normal two minutes after a 50-Hz stimulus.10 This result substantiates that the recommended six-minute time interval might be unnecessarily long; however, the actual intervening time required before TOF monitoring can be resumed after tetanic stimulation is uncertain.
This study was designed to determine the extent of facilitation of neuromuscular transmission in one arm using repeated TOF measurements for up to 30 min following PTC and to compare the responses with those in the patient’s contralateral (control) arm. We aimed to determine the duration of post-tetanic facilitation after a single PTC in order to estimate the time interval required before TOF responses could be considered reliable.
Methods
The protocol was approved by the Comité d’éthique de la recherche de l’Hôpital Maisonneuve-Rosemont on February 10, 2010. Eligibility criteria included adult patients of both sexes (aged 18-75 yr and American Society of Anesthesiologists physical status I-III) who were scheduled for elective surgery under general anesthesia requiring neuromuscular blocking agents. In addition, the patients needed to be placed in the supine position for the surgical procedure with both arms accessible and abducted to 90°. Exclusion criteria included neuromuscular disorders, anatomical or functional anomaly to one or both upper extremities, preoperative medications known or suspected to interfere with neuromuscular transmission, suspected full stomach, symptomatic gastroesophageal reflux, contraindication to any of the study medications, need for repeated doses of neuromuscular blocking agents, and anticipated duration of surgery less than 90 min.
In the operating room, intravenous access was secured in one of the patient’s upper extremities. Monitoring included electrocardiogram, pulse oximetry, inspired and expired gases, and central temperature. A probe was applied on the skin of each hand to measure peripheral temperature, and a noninvasive blood pressure cuff was applied to one of the patient’s lower extremities. A GE Healthcare NMT MechanoSensor (GE Healthcare, Waukesha, WI, USA) was applied to each upper extremity. This setup involved two stimulating electrodes placed over the course of the ulnar nerve at the wrist, with the negative electrode placed distally and a strip applied to the index finger and thumb to measure displacement. The assembly was inserted into protective plastic boxes firmly attached to the arm boards to protect it from inadvertent displacement and knocking by the surgeon and other operating room workers.
Anesthesia was induced with fentanyl or sufentanil, followed by propofol at doses deemed adequate by the attending anesthesiologist. The patient’s lungs were then ventilated manually while both neuromuscular devices were calibrated. After supramaximal current was determined, TOF stimulation was applied every 20 sec, and rocuronium 0.6 mg·kg−1 was injected intravenously. When twitch response disappeared, the patient’s trachea was intubated and the lungs were ventilated with an air-oxygen mixture using a minute volume adjusted to keep end-tidal pCO2 at 35-40 mmHg. Anesthesia was maintained with desflurane 4-8% and incremental doses of fentanyl or sufentanil as needed.
Randomization according to control or PTC extremity was achieved using a computer-generated list, and the assignment was inserted in a sealed envelope to be opened after the rocuronium injection. When first twitch height (T1) in the TOF reached 10% of pre-rocuronium value in the control arm, a PTC stimulus, i.e., a 50-Hz tetanus followed by a three-second pause and 15 1-Hz stimuli, was applied to the PTC arm. The TOF stimulations resumed in the PTC arm one minute after the start of the tetanic stimulation and repeated every 20 sec. In the control arm, TOF stimulations were applied throughout. During maintenance of anesthesia, both arms were monitored for at least 30 min after PTC was applied, and no additional rocuronium was given. The patients were then managed at the discretion of the attending anesthesiologist.
First twitch height was measured with respect to control (pre-rocuronium) value in the same arm. First twitch height (T1) and TOF ratio (T4/T1) were measured before PTC (baseline) and from one to 30 min after PTC. The primary outcome measurement was T1 vs time after PTC. The secondary outcome measurement was T4/T1 against time. Continuous data are presented as mean (standard deviation [SD]). Each patient served as his/her control. The data were plotted against time after PTC, and the area under the curve (AUC) for the PTC arm was compared with the control arm. For this comparison, a paired Student’s t test was used and all reported P values are two sided. The values were then compared at five specific pre-determined times: two, five, ten, 20, and 30 min after PTC. For these comparisons, a Student’s t test was used, and the P value was set at < 0.01 (two-sided) to adjust for the five multiple comparisons.
To avoid possible bias resulting from an imbalance in the baseline (pre-PTC) T1 and/or T4/T1 values, the data were also reanalyzed, with readjustment of the values for each side with respect to its own baseline. Furthermore, recovery for T1 up to 10% is slower than the rest of recovery due to non-linearity in this portion of the curve. We considered the use of logit transformation to linearize data for analysis11; however, it was not possible to do so because of zero values for T4/T1 ratios among our results.
To estimate the number of patients for inclusion in the study, we considered a 10% difference in T1 clinically significant. Also, according to the work of Claudius et al.,12 the difference in twitch response between arms has a typical SD of 13%. For a paired Student’s t test, using a power of 0.8 and an alpha value of 0.01 (to allow for five multiple comparisons), 20 patients were required. Thus, we recruited 22 patients to allow for possible incomplete data.
Results
Twenty-eight patients were approached to participate in this study in March and April, 2010. Three patients declined enrolment, and three were excluded because the procedure did not require a neuromuscular blocking agent (n = 1), a rapid sequence induction was indicated (n = 1), and the neuromuscular devices did not function properly (n = 1). The demographic data of the 22 patients who completed this study are shown in Table 1.
After injection of rocuronium, all patients had a minimum T1 < 10% in both arms, although four did not reach 0%. The mean (SD) interval from rocuronium injection until 10% T1 recovery in the control arm was 32.5 (13.6) min. Skin temperature was similar for the control and PTC arms [33.3 (2.2)°C and 33.3 (1.9)°C, respectively]. Other intraoperative variables appear in Table 2. When PTC was applied, the T1 value in the control arm did not deviate from 10% by more than 1%; however, the mean T1 value in the PTC arm was 11.8% with a range of 2-27% (Table 3).
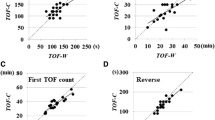
The mean T1 was greater in the PTC arm than in the control arm at all times from one to 30 min (Fig. 1). The mean (SD) difference in T1 between arms across the period was 5.8 (9.7)% (P = 0.011; paired Student’s t test). The mean (SD) AUC of the T1 vs time relationship was significantly greater in the PTC than in the control arm 1,620 (547)% ⋅min vs 1,447 (480)%⋅min, respectively (P = 0.011; paired Student’s t test). There were significant differences at two, five, and ten minutes (P = 0.008; to account for the five multiple comparisons), but not at 20 and 30 min (Table 3). Mean T4/T1 values were similar in both arms at all times (Fig. 2). The overall mean (SD) difference between arms was 2.4 (1.8)%, and the mean (SD) AUC was not statistically different between arms 717 (555)%⋅min for the PTC arm and 644 (501)%⋅min for the control arm (P = 0.054). The difference did not exceed 4% at any time, and the P value did not exceed 0.01 (to account for multiple comparisons) at any time (Table 3). The results remained essentially unchanged if adjusted for baseline values.

First twitch height (T1), expressed as % of respective control, in the control arm and in the arm where post-tetanic count (PTC) stimulation was applied. Bars denote standard deviation

Train-of-four ratio (T4/T1), expressed as %, in the control arm and in the arm where post-tetanic count (PTC) stimulation was applied. Bars denote standard deviation
Discussion
This study showed that the PTC mode of stimulation has limited impact on the TOF responses during one to 30 min after PTC was applied. There is a small increase in T1 at two to ten minutes after PTC, but the magnitude of this effect is marginal (< 10%). The effect of PTC is even less on T4/T1 (< 4% at all times), and for T4/T1, the difference between arms did not attain statistical significance. Paradoxically, the effect on T1 was greatest at five minutes, which is close to the recommended interval (six minutes) used in previous studies.1-6
The PTC comprises a tetanic stimulation at 50 Hz for five seconds (250 impulses), followed by a three-second pause and then a series of 15 test stimuli at 1 Hz . Thus, the duration of this stimulation pattern is 23 sec with a total of 265 impulses. Since both the PTC and the five-second 50-Hz tetanus involve approximately the same number of impulses, the two modes of stimulation likely have a similar impact on further stimulation. Therefore, in the following discussion, both modes of stimulation are considered equivalent in this regard.
This study was designed to avoid some of the shortcomings in previous investigations, such as attempts to define an interval of further stimulation after a PTC or a 50-Hz tetanus. In the studies validating the technique for pancuronium,1 vecuronium,2,4 atracurium,3 rocuronium,5 and cisatracurium,6 this interval was assumed to be six minutes. Nevertheless, there is a lack of further validation excepting the limited experience of Feldman and Tyrell.9 These investigators monitored the responses in both arms of one patient in conjunction with d-tubocurarine, a neuromuscular blocking agent which is no longer available.
The problem associated with the two-arm technique is that both extremities are not always exactly the same in their response to neuromuscular drugs.12 In the present study, the actual difference was small before PTC was applied, and randomization facilitated a mean difference between the control and PTC arms of less than 2%. Other techniques have been used to estimate the duration of post-tetanic facilitation, such as administering a constant infusion of neuromuscular blocking agent or randomizing different patients to tetanic stimulation or not. Using a constant infusion of vecuronium, Silverman and Brull10 delivered two successive tetanic stimuli separated by either two or five minutes and found identical tetanic responses. The T4/T1s before both tetanic stimuli, whether separated by two or five minutes, were similar, a finding consistent with the results of the present study. The T1 response was slightly (5%) greater before the second tetanic stimulus, for both the two- and five-minute intervals, which again is similar to the difference seen in the present study for the two- to five-minute period. In another study, the same investigators randomized different patients to have 50-Hz tetanic stimulation applied or not at 25% or 50% T1 recovery.13 Recovery to 50% or 75% T1, respectively, in the same arm, was accelerated by approximately two minutes. This slight increase in T1 was also found in the present study. Again using a single-arm design, Saitoh et al. estimated the duration of post-tetanic facilitation at less than one minute, both for the T1 and T4/T1 responses.14 The problem with using one arm is that testing can be performed only at one specific time in each patient, whereas in the present study, the phenomenon could be observed during 30 min by comparing both extremities. A two-arm design was employed by Motamed et al. 8 who administered atracurium and applied PTC every three minutes when blockade was complete. They found that visible twitch responses appeared one to two minutes earlier in the PTC arm. The limitation of that study is that slight degrees of facilitation might have been missed during the period of complete blockade. Nevertheless, all these previous studies are consistent with the present study, indicating that the facilitating effect of PTC or tetanic stimulation does not extend much beyond one to two minutes, apart perhaps from a slight increase in T1 lasting at least five minutes. In the present study, T1 was increased even beyond ten minutes.
The PTC mode of stimulation was created to evaluate the intensity of neuromuscular blockade when no twitch response is present in response to TOF stimulation. In the present study, the PTC was applied later, at 10% T1 recovery, to afford the possibility of measuring the time course and magnitude of subsequent facilitation with TOF stimulation. The decision to apply PTC early as opposed to later in the recovery period allowed measurements to be taken for at least 30 min. With this particular design and the use of a control arm for each patient, it was possible to determine the duration of facilitation of responses rather than whether the phenomenon was present at specific times, as in previous studies. The results indicate that T1 is greater in the PTC arm for at least ten minutes, but the magnitude of this effect is small (< 10%), which is negligible clinically. The effect is even less marked on T4/T1, which is the preferred mode of stimulation in clinical practice. As a result, TOF responses can be elicited in clinical practice as early as one minute after application of PTC or a five-second 50-Hz tetanus.
The present study has several limitations. First, only one neuromuscular agent was administered. Nevertheless, rocuronium is perhaps the most commonly used agent, and previous studies in which other agents (vecuronium,2-4 atracurium,3 cisatracurium6 have been utilized show similar results. This suggests that the conclusions in this study might apply with the use of other neuromuscular blocking drugs. Second, a difference between arms, not related to hand dominance, is normally present and has been previously documented.12 The difference seen at 10% T1 in the present study was less than anticipated, with an SD of 6.7% instead of 13%,12 which allowed differences as small as 5% or so to be detected. In addition, adjusting the results for different baselines on the PTC arm did not change the results. Third, the PTC was applied at a point (T1 = 10% of control) when recovery is not linear. Recovery is less rapid around 10% than in the 25-75% range. As mentioned above, early application of PTC during the recovery period made it possible for a long recovery period. Fourth, a PTC was applied when spontaneous recovery had started, which is in contrast to the clinical situation where PTC is indicated when there is no response to TOF stimulation. A late PTC application was chosen to obtain a measurable T1 value. Fifth, desflurane is known to potentiate neuromuscular blocking agents. The results could be different in the absence of halogenated agents. Nevertheless, because both arms were exposed to the same anesthetic, the degree of potentiation was likely the same in both extremities.
In conclusion, PTC or a 50-Hz tetanic stimulation may be applied without undue concern about spuriously exaggerated subsequent responses if TOF stimuli are generated after an interval of at least one minute. There is a small statistically significant but clinically insignificant increase in T1 that persists for at least ten minutes, suggesting that the recommended value of five to six minutes is, if anything, no better than shorter intervals. The present study did not identify a statistical or clinical difference for T4/T1, a more common monitoring modality.
References
Viby-Mogensen J, Howardy-Hansen P, Chraemmer-Jorgensen B, Ording H, Engbaek J, Nielsen A. Posttetanic count (PTC): a new method of evaluating an intense nondepolarizing neuromuscular blockade. Anesthesiology 1981; 55: 458-61.
Muchhal KK, Viby-Mogensen J, Fernando PU, Tamilarasan A, Bonsu AK, Lambourne A. Evaluation of intense neuromuscular blockade caused by vecuronium using posttetanic count (PTC). Anesthesiology 1987; 66: 846-9.
Bonsu AK, Viby-Mogensen J, Fernando PU, Muchhal K, Tamilarasan A, Lambourne A. Relationship of post-tetanic count and train-of-four response during intense neuromuscular blockade caused by atracurium. Br J Anaesth 1987; 59: 1089-92.
Saitoh Y, Toyooka H, Amaha K. Relationship between post-tetanic twitch and single twitch response after administration of vecuronium. Br J Anaesth 1993; 71: 443-4.
Schultz P, Ibsen M, Ostergaard D, Skovgaard LT. Onset and duration of action of rocuronium – from tracheal intubation, trough intense block to complete recovery. Acta Anaesthesiol Scand 2001; 45: 612-7.
El-Orbany MI, Joseph NJ, Salem MR. The relationship of posttetanic count and train-of-four responses during recovery from intense ciaatracurium-induced neuromuscular blockade. Anesth Analg 2003; 97: 80-4.
Suzuki T, Kitajima O, Ueda K, Kondo Y, Kato J, Ogawa S. Reversibility of rocuronium-induced profound neuromuscular block with sugammadex in younger and older patients. Br J Anaesth 2011; 106: 823-6.
Motamed C, Kirov K, Combes X, Duvaldestin P. Does repetition of post-tetanic count every 3 min during profound relaxation affect accelerographic recovery of atracurium blockade? Acta Anaesthesiol Scand 2005; 49: 811-4.
Feldman SA, Tyrrell MF. A new theory of the termination of action of muscle relaxants. Proc R Soc Med 1970; 63: 692-5.
Silverman DG, Brull SJ. The effect of a tetanic stimulus on the response to subsequent tetanic stimulation. Anesth Analg 1993; 76: 1284-7.
Fuchs-Buder T, Claudius C, Skovgaard LT, et al. Good clinical research practice in pharmacodynamic studies of neuromuscular blocking agents II: the Stockholm revision. Acta Anaesthesiol Scand 2007; 51: 789-808.
Claudius C, Skovgaard LT, Viby-Mogensen J. Arm-to-arm variation when evaluating neuromuscular block: an analysis of the precision and the bias and agreement between arms when using mechanomyography or acceleromyography. Br J Anaesth 2010; 105: 310-7.
Brull SJ, Silverman DG. Tetanus-induced changes in apparent recovery after bolus doses of atracurium or vecuronium. Anesthesiology 1992; 77: 642-5.
Saitoh Y, Masuda A, Toyooka H, Amaha K. Effect of tetanic stimulation on subsequent train-of-four responses at various levels of vecuronium-induced neuromuscular block. Br J Anaesth 1994; 73: 416-7.
Acknowledgment
This study was supported by internal departmental funds.
Conflicts of interest
None declared.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author contributions
François Donati, Louis-Philippe Fortier, David Hakim, and Pierre Drolet contributed substantially to the conception and design of the manuscript and to the analysis and interpretation of data. François Donati, Louis-Philippe Fortier, and David Hakim contributed substantially to the acquisition of data. François Donati and Louis-Philippe Fortier contributed substantially to drafting the article. David Hakim helped with drafting the article.
Rights and permissions
About this article

Cite this article
Hakim, D., Drolet, P., Donati, F. et al. Performing post-tetanic count during rocuronium blockade has limited impact on subsequent twitch height or train-of-four responses. Can J Anesth/J Can Anesth 63, 828–833 (2016). https://doi.org/10.1007/s12630-016-0619-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-016-0619-9