
Abstract
Introduction
Wherever access to direct-acting antiviral agents is restricted, dual peginterferon/ribavirin (PegIFN/RBV) therapy remains an option for treatment of hepatitis C virus (HCV) genotype 4 (GT4) infection, which predominates in the Middle East and Sub-Saharan Africa. Our goal was to develop a baseline scoring system to identify GT4-infected patients with a low or high probability of achieving a sustained virologic response (SVR) with PegIFN alfa-2a/RBV using data from two large cohort studies.
Methods
Associations between baseline characteristics and SVR were explored by generalized additive models and multiple logistic regression analysis to develop a predictive model, which was then checked by bootstrapping. The score comprised four factors with points assigned thus: age ≤40, 3 points; >40 but ≤55, 2 points; alanine aminotransferase ≤1 or >3× the upper limit of normal, 1 point; no cirrhosis, 1 point; HCV RNA <50,000 IU/mL, 2 points; 50,000 to <400,000 IU/mL, 1 point. The values for a given patient are summed to produce a score from 0 to 7 where higher scores indicate higher chances of SVR.
Results
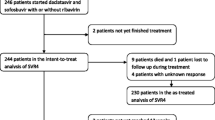
Among the 459 patients, 28 (6%), 50 (11%), 92 (20%), 121 (26%), 103 (22%), and 65 (14%) patients had scores of 0–1, 2, 3, 4, 5, and 6–7, respectively, with respective SVR rates of 11%, 28%, 50%, 57%, 63%, and 83%. Relapse rates decreased with increasing prediction score (80%, 39%, 15%, 19%, 5%, and 7%, respectively). SVR rates were consistently higher in Caucasian than Black patients and in patients with a rapid virologic response HCV RNA <50 IU/mL at week 4); however, the trend toward higher SVR rates with increasing score remained apparent in each subgroup.
Conclusion
In conclusion, a simple scoring system can be used to identify GT4-infected patients with a high probability of achieving an SVR with PegIFN alfa-2a/RBV.
Funding
F. Hoffmann-La Roche Ltd.




Similar content being viewed by others

References
Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013;57:1333–42.
Ward JW, Mermin JH. Simple, effective, but out of reach? Public health implications of HCV drugs. N Engl J Med. 2015;373:2678–80.
Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol. 2014;61:S45–57.
Asselah T, Bourlière M. Hepatitis C virus: current and evolving treatments for genotype 4. Gastroenterol Clin N Am. 2015;44:859–70.
Asselah T. Optimism for patients with genotype 4 HCV infection: clinical trials with direct-acting antivirals finally available. J Hepatol. 2015;62:996–9.
European Association for Study of Liver. EASL recommendations on treatment of hepatitis C 2015. J Hepatol. 2015;63:199–236.
Hezode C, Asselah T, Reddy KR, Hassanein T, Berenguer M, Fleischer-Stepniewska K, et al. Ombitasvir plus paritaprevir plus ritonavir with or without ribavirin in treatment-naive and treatment-experienced patients with genotype 4 chronic hepatitis C virus infection (PEARL-I): a randomised, open-label trial. Lancet. 2015;385:2502–9.
Abergel A, Metivier S, Samuel D, Jiang D, Kersey K, Pang PS, et al. Ledipasvir plus sofosbuvir for 12 weeks in patients with hepatitis C genotype 4 infection. Hepatology. 2016 (in press).
Lawitz E, Mangia A, Wyles D, Rodriguez-Torres M, Hassanein T, Gordon SC, et al. Sofosbuvir for previously untreated chronic hepatitis C infection. N Engl J Med. 2013;368:1878–87.
Moreno C, Hezode C, Marcellin P, Bourgeois S, Francque S, Samuel D, et al. Efficacy and safety of simeprevir with PegIFN/ribavirin in naive or experienced patients infected with chronic HCV genotype 4. J Hepatol. 2015;62:1047–55.
Hezode C, Hirschfield GM, Ghesquiere W, Sievert W, Rodriguez-Torres M, Shafran SD, et al. Daclatasvir plus peginterferon alfa and ribavirin for treatment-naive chronic hepatitis C genotype 1 or 4 infection: a randomised study. Gut. 2015;64:948–56.
American Association for the Study of Liver Diseases (AASLD), Infectious Diseases Society of America (IDSA). HCV guidance: recommendations for testing, managing, and treating hepatitis C. Updated 2016. http://www.hcvguidelines.org/. Accessed June 17, 2016.
Fried MW, Shiffman ML, Reddy KR, Smith C, Marinos G, Gonçales FL Jr, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med. 2002;347:975–82.
Manns MP, McHutchison JG, Gordon SC, Rustgi VK, Shiffman M, Reindollar R, et al. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised trial. Lancet. 2001;358:958–65.
Hadziyannis SJ, Sette H Jr, Morgan TR, Balan V, Diago M, Marcellin P, et al. Peginterferon-alpha2a and ribavirin combination therapy in chronic hepatitis C: a randomized study of treatment duration and ribavirin dose. Ann Intern Med. 2004;140:346–55.
Esmat G, El Kassas M, Hassany M, Gamil M, El Raziky M. Optimizing treatment for HCV genotype 4: PEG-IFN alfa 2a vs. PEG-IFN alfa 2b; the debate continues. Liver Int. 2014;34(Suppl 1):24–8.
Ferenci P, Laferl H, Scherzer TM, Gschwantler M, Maieron A, Brunner H, et al. Peginterferon alfa-2a and ribavirin for 24 weeks in hepatitis C type 1 and 4 patients with rapid virological response. Gastroenterology. 2008;135:451–8.
Kamal SM, El Kamary SS, Shardell MD, Hashem M, Ahmed IN, Muhammadi M, et al. Pegylated interferon alpha-2b plus ribavirin in patients with genotype 4 chronic hepatitis C: the role of rapid and early virologic response. Hepatology. 2007;46:1732–40.
Asselah T, De Muynck S, Broet P, Masliah-Planchon J, Blanluet M, Bieche I, et al. IL28B polymorphism is associated with treatment response in patients with genotype 4 chronic hepatitis C. J Hepatol. 2012;56:527–32.
January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–104.
Estrabaud E, Vidaud M, Marcellin P, Asselah T. Genomics and HCV infection: progression of fibrosis and treatment response. J Hepatol. 2012;57:1110–25.
Marcellin P, Cheinquer H, Curescu M, Dusheiko GM, Ferenci P, Horban A, et al. High sustained virologic response rates in rapid virologic response patients in the large real-world PROPHESYS cohort confirm results from randomized clinical trials. Hepatology. 2012;56:2039–50.
Foster GR, Coppola C, Derbala M, Ferenci P, Orlandini A, Reddy KR, et al. Impact of safety-related dose reductions or discontinuations on sustained virologic response in HCV-infected patients: results from the GUARD-C cohort. PLoS One. 2016;11:e0151703.
Clinical Steyerberg E, Models Prediction. A practical approach to development, validation, and updating. New York: Springer; 2009.
Sullivan LM, Massaro JM, D’Agostino RBS. Presentation of multivariate data for clinical use: the Framingham Study risk score functions. Stat Med. 2004;23:1631–60.
Jeffers LJ, Cassidy W, Howell CD, Hu S, Reddy KR. Peginterferon alfa-2a (40 kd) and ribavirin for black American patients with chronic HCV genotype 1. Hepatology. 2004;39:1702–8.
Muir AJ, Bornstein JD, Killenberg PG. Peginterferon alfa-2b and ribavirin for the treatment of chronic hepatitis C in blacks and non-hispanic whites. N Engl J Med. 2004;350:2265–71.
Conjeevaram HS, Fried MW, Jeffers LJ, Terrault NA, Wiley-Lucas TE, Afdhal N, et al. Peginterferon and ribavirin treatment in African American and Caucasian American patients with hepatitis C genotype 1. Gastroenterology. 2006;131:470–7.
Ge D, Fellay J, Thompson AJ, Simon JS, Shianna KV, Urban TJ, et al. Genetic variation in IL28B predicts hepatitis C treatment-induced viral clearance. Nature. 2009;461:399–401.
Poordad F, McCone J Jr, Bacon BR, Bruno S, Manns MP, Sulkowski MS, et al. Boceprevir for untreated chronic HCV genotype 1 infection. N Engl J Med. 2011;364:1195–206.
Fried MW, Hadziyannis SJ, Shiffman ML, Messinger D, Zeuzem S. Rapid virological response is the most important predictor of sustained virological response across genotypes in patients with chronic hepatitis C virus infection. J Hepatol. 2011;55:69–75.
Shiffman ML, Suter F, Bacon BR, Nelson D, Harley H, Sola R, et al. Peginterferon alfa-2a and ribavirin for 16 or 24 weeks in HCV genotype 2 or 3. N Engl J Med. 2007;357:124–34.
Lee SS, Roberts SK, Berak H, Dusheiko GM, Harley HA, Gane EJ, et al. Safety of peginterferon alfa-2a plus ribavirin in a large multinational cohort of chronic hepatitis C patients. Liver Int. 2012;32:1270–7.
Ferenci P, Aires R, Ancuta I, Arohnson A, Cheinquer H, Delic D, et al. A tool for selecting patients with a high probability of sustained virological response to peginterferon alfa-2a (40kD)/ribavirin. Liver Int. 2014;34:1550–9.
Asselah T, Thompson AJ, Flisiak R, Romero-Gomez M, Messinger D, Bakalos G, et al. A predictive model for selecting patients with HCV genotype 3 chronic Infection with a high probability of sustained virological response to peginterferon alfa-2a/ribavirin. PLoS One. 2016;11(3):e0150569.
Ditah I, Al Bawardy B, Gonzalez HC, Saberi B, Ditah C, Kamath PS, et al. Lack of health insurance limits the benefits of hepatitis C virus screening: insights from the National Health and Nutrition Examination Hepatitis C follow-up study. Am J Gastroenterol. 2015;110:1126–33.
Barua S, Greenwald R, Grebely J, Dore GJ, Swan T, Taylor LE. Restrictions for Medicaid reimbursement of sofosbuvir for the treatment of hepatitis C virus infection in the United States. Ann Intern Med. 2015;163:215–23.
Stattermayer AF, Stauber R, Hofer H, Rutter K, Beinhardt S, Scherzer TM, et al. Impact of IL28B genotype on the early and sustained virologic response in treatment-naive patients with chronic hepatitis C. Clin Gastroenterol Hepatol. 2011;9:344–50.
Acknowledgments
Sponsorship of these studies and article processing charges were funded by F. Hoffmann-La Roche Ltd, Basel, Switzerland. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. Editorial assistance in the preparation of this manuscript was provided by Dr. Manda Gent and Blair Jarvis of Health Interactions. Support for this assistance was funded by F. Hoffmann-La Roche Ltd, Basel, Switzerland. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published.
Disclosures
Tarik Asselah is a speaker/consultant for Roche, AbbVie, Achillion, Boehringer-Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck. Gamal Esmat is a speaker, investigator and/or advisory board member for AbbVie, Bristol-Myers Squibb, Janssen, Merck, F Hoffmann-La Roche. Faisal M. Sanai is a consultant for/advises, is on the speakers’ bureau of, and has received grant support from F. Hoffmann-La Roche, and Bristol-Myers Squibb. He has been a consultant for, and advised Merck, Gilead Sciences, Janssen Pharmaceuticals and AbbVie. He is on the speakers’ bureau of Merck, Gilead Sciences, and AbbVie. Ioannis Goulis is a speaker, investigator and/or advisory board member for AbbVie, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, F Hoffmann-La Roche. Diethelm Messinger is an employee of PROMETRIS GmbH. PROMETRIS GmbH has a contract with F. Hoffmann-La Roche Ltd to provide statistical support. Georgios Bakalos is an employee of F. Hoffmann-La Roche Ltd. Imam Waked is a speaker, investigator and/or advisory board member for AbbVie, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck, Pharco, F Hoffmann-La Roche.
Compliance with Ethics Guidelines
All procedures followed in the original studies were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964. Informed consent was obtained from all patients for being included in the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/6AE4F060111952BB.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Asselah, T., Esmat, G., Sanai, F.M. et al. Simple Predictive Model for Identifying Patients with Chronic Hepatitis C and Hepatitis C Virus Genotype 4 Infection with a High Probability of Sustained Virologic Response with Peginterferon Alfa-2a/Ribavirin: Pooled Analysis of Data from Two Large, International Cohort Studies. Adv Ther 33, 1797–1813 (2016). https://doi.org/10.1007/s12325-016-0396-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-016-0396-4