
Abstract
Purpose of Review
Clinician burnout has significant socioeconomic, health, and quality of life implications. However, there has been little attention directed at medical students and house officers (i.e., medical learners). This review provides pertinent evidence regarding burnout as it relates to medical learners including risk factors and potential interventions. We conclude with recommendations on future research directions and potential approaches to address this epidemic of medical learner burnout.
Recent Findings
Burnout is a significant issue among medical learners that is impacted both by interpersonal and environmental factors. There are points of heightened vulnerability for medical learners throughout their training. However, studies are unable to reach consensus regarding effective interventions to mitigate the impact of burnout. Furthermore, some elements of burnout are not readily reversible even after removing risk factors.
Summary
Burnout is a significant concern for medical learners with wide-ranging physical, emotional, and psychosocial consequences. However, the current body of literature is sparse and does not provide consistent guidance on how to address burnout in medical learners. It is clear additional attention is needed in understanding burnout among learners and establishing proactive approaches to minimize its negative impact.
Similar content being viewed by others

Introduction
Defined as emotional and physical exhaustion due to excessive stress, burnout is associated with feeling overwhelmed, or emotionally drained, and an inability to meet demands. Due to burnout’s significant physical (e.g., fatigue), social (e.g., decreased interest in family, friends, and community), and emotional (e.g., depression, anxiety, and suicidality) impact on health and well-being, quality of life (including marital and family discord), and socioeconomic (including decreased work productivity) implications, it is receiving increasing attention across all public and private sectors [1]. In fact, the World Health Organization (WHO) recently recognized the importance of occupational burnout. They first introduced it in the ICD-10 and provided a more detailed definition in the ICD-11 [2]. The WHO defines “burnout” as a syndrome resulting from chronic workplace stress that has not been successfully managed. It is characterized by three dimensions: (1) feelings of energy depletion or exhaustion; (2) increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job; and (3) reduced professional efficacy. It does not apply to other parts of an individual’s life and is not a medical condition [3]. Thus, to combat burnout, there is a need to focus on the aspects of work environment itself and how individuals are thriving or not in the environment.
There has also been increasing interest in the predictors, causal factors, and impact of clinician burnout [4]. The WHO’s interest in burnout suggests there are universal themes in occupational burnout that do not differ by culture or nationality [5]. Physician well-being is receiving increasing attention, yet there has been little attention directed at those becoming clinicians and health professionals. Specifically, medical learners (i.e., students and trainees) are operating in the same, potentially unhealthy environment as their attending physicians, clinician educators, and patients while also being participant observers [6]. Medical learner burnout in the clinical learning environment and its impact on patients and families have not been well elucidated. The novel and deadly coronavirus (COVID-19) caused a global pandemic in early 2020 and set the stage for sweeping changes in the healthcare landscape including clinical practice, health professional education, and clinical learning environments. Concerns focused on how to keep clinicians safe (including ensuring personal protective equipment or PPE) and stopping and preventing the spread to the community via good public health practices [7]. The media and personal reports as well as the literature show clinicians are experiencing extreme stress and fatigue due to the global pandemic’s immediate and emergent acuity which extends beyond caring for critically ill, dying, and distressed patients. A myriad of other stressors ranging from protecting themselves (and loved ones) from the deadly virus to home schooling children have also contributed [8, 9]. Nonetheless, fleeting attention has been given to learners and burnout as trainees were redeployed, 4th year medical students were often allowed to graduate early, and other medical students were sent home to learn remotely (often isolated from family, friends, and colleagues). In addition, learners not on the frontlines were dealt a significant and unexpected change in their daily routines and were often isolated as well.
Often considered occupational hazards, depression and burnout were major issues among physicians prior to the pandemic, and both are associated with devastating consequences. A recent 2019 Medscape poll found nearly 50% of physicians reported burnout [10]. Although still a taboo subject, approximately 300 physicians die in the United States via suicide annually, a rate that is > 2 times that of the general population [11••, 12••, 13••, 14••, 15]. More alarming is that 28% of residents report major depression at some time during their training. Physicians often fear the repercussions of seeking mental treatment and are less likely to be receiving mental health treatment at the time of their death due to suicide [15]. Since suicide is the second-leading cause of death (behind accidents) among 24- to 34-year-olds, the high rate of physician suicide and burnout has tremendous public health implications in general but especially in the context of a global pandemic. The recent suicides of physicians, medical students, and other health professionals reveal the increasing mental health challenges of frontline workers during a pandemic while providing a glimpse at the impact on all physicians [16]. However, rarely discussed in the national conversation are the prevalence, predictors, and consequences nor the prevention and treatment of burnout among those learning to become physicians.
For medical learners, COVID-19 has created an uncertain world that will last even after the virus has left our communities. Specifically, COVID-19 has clearly changed not only job demands, (including being deployed and furloughed) employee and employer relationships (including the shuttering and subsequent fiscal decline of many hospitals requiring federal bail outs), and expectations (including salary and retirement cuts) regardless of the setting in academic, teaching, or community hospitals. Furthermore, COVID-19 created a multitude of new unforeseen stressors for physicians beyond physical health that impact mental health such as job insecurity, income reduction, unemployment, and continued debt accumulation for a profession that was thought to be immune. Moreover, similar to the early years of the AIDS crisis, COVID-19 presented an additional stress for physicians, residents, and medical students—an emerging infectious disease and public health threat we were largely powerless to fix. As participant observers, we wondered whether the events of 2020 would contribute to hastening the pace and impact of physician burnout among those who are learners during the COVID-19 pandemic.
Of import, in late 2019 (and prior to the COVID-19 pandemic), the National Academy of Medicine (NAM) released a consensus study report entitled, “Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being.” The NAM reported a range of 35 to 54% of nurses and physicians in the USA having substantial burnout symptoms with a range of 45 to 60% for medical students and residents [4]. They noted burnout is a problem across all clinical disciplines and care settings. The report included six goals to eliminate burnout and enhance professional well-being. Specifically, the NAM’s second recommendation focuses on medical learners and aims to “transform health professions education and training to optimize learning environments that prevent and reduce burnout and foster professional well-being.” Furthermore, since burnout prevents the clinician workforce from working at its highest level, its high prevalence is a harbinger for a failing healthcare system and an inability to achieve its triple aims [4]. Healthcare organizations, health professional educational institutions, government, and industry must prioritize improvements in clinical work and learning environments in all settings and across disciplines to prevent and mitigate burnout [2]. The 2019 Medscape poll revealed generational differences as well as differences between disciplines [10]. Hence, fostering well-being within a multi-generational workplace (Millennials, Generation X, and Baby Boomers) is necessary. Consistent with media reports and personal experience, COVID-19 may hasten and increase the prevalence of burnout as funds within medical schools, hospitals, and health systems decrease and stress increases for patients, clinicians, and learners alike in an increasingly uncertain environment. In this context, we explore what is known and the long-term impact on the most vulnerable healthcare workforce: medical students and house officers.
Methods
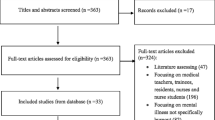
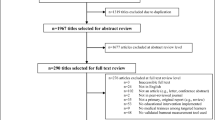
Overall, there is an emerging urgency to understand clinician burnout across a wide variety of populations, generations, job classes, training statuses, and social determinants of health. Its increasing occurrence and devastating ramifications deserve attention. This article seeks to examine the available pertinent literature regarding burnout for learners: medical students and trainees (i.e., house officers, residents, and fellows) including causal factors and treatment. A selective literature review was performed. Although much can be learned from other countries, the literature cited only includes studies associated with North American medical schools since they undergo a similar accreditation process and their curricula mirror each other. The reviewers (all learners: a medical student and two resident house officers) developed abstracts with relevant citations on burnout in learners. Scientific evidence was given precedence over anecdotal evidence. The abstracts were compiled for this manuscript and reviewed prior to submission for publication. This article also outlines research priorities to improve the quality of science, move the research and treatment community closer together, and address and eliminate burnout. Lastly, this article serves as a platform for discussion among interested parties (e.g., healthcare policy analysts, higher education leaders, the general public, and those who fund research at the community, state, and federal level).
Results
Several studies suggest the overall prevalence of burnout may approach 50%, and the medical education process is directly responsible, with burnout increasing in the latter years of medical school [17, 18••]. Brazeau et al. showed matriculating medical students begin medical school with similar or better mental health than their non-medical school college educated peers [17]. In this cross-sectional study, matriculating medical students and age-similar college graduates were surveyed to measure burnout, mental health, and quality of life. At the beginning of medical school, matriculating students had statistically significant lower rates of burnout and depression and had higher scores across quality of life domains. However, their mental health worsened relative to their peers during medical school.
Hansell et al. used the Medical Student Well-being Index to survey 120 medical students from the class of 2016 over 4 years of medical education at a single Liaison Committee on Medical Education (LCME) accredited medical school [18••]. They identified associated stressors and found distress increased from 2% at matriculation to 38% after the match while depersonalization (altered response towards others) increased from 13% to 35%. Similarly, emotional exhaustion increased from 5% to 22%, but peaked after the first year of medical school at 45%. Importantly, Hansell found that once depersonalization occurs, it is extremely difficult to remedy as evidenced by lack of improvement in this domain, even following vacations when other well-being domains tend to improve. Of note, the Hansell study did not include any interventions or strategies.
Not surprisingly, Wolf’s 1994 narrative literature review on medical student well-being revealed academic demands, financial responsibilities (e.g., loans), foregoing personal interests, and emotional isolation were common sources of stress for medical students [19]. In 2008, Dunn et al. described the propensity of medical students towards burnout as a dynamic phenomenon [20]. Specifically, they proposed a conceptual model in which medical students have a “coping reservoir,” and different medical student experiences either replenish or drain this reservoir. They proposed several replenishing factors: psychosocial support, social activities, mentorship, and intellectual stimulation. Family, friends, therapists, faith groups, and school staff could be sources of psychosocial support. Spontaneous socializing inside and outside the healthcare system can also replenish coping reservoirs. They also noted mentoring is needed for a variety of professional, clinical, and research roles. Nonetheless, the impact of the proposed strategies was not measured.
Medical learners must focus on professional development, even though they often feel they are unbalanced. Through semi-structured interviews of residents from a variety of fields, Ratanawongsa et al. found residents reported losing a sense of themselves during residency due to physical exhaustion from sleep deprivation, heavy workloads, emotional intensity of work, dysfunctional work systems, and lack of time for personal lives [21]. Similar to other life-changing events (e.g., birth of a child, loss of a parent/spouse), these findings recognize medical training as a time of imbalance and thus the process of becoming a physician may need to be reconceptualized. Since these imbalances are predictable and occur in multiple realms across the life course, putting together a team of advisors may be necessary. Furthermore, mechanisms need to be in place, going beyond restrictions in duty hours, to accommodate activities that promote total health and well-being.
Individual Level Predictors of Burnout
The knowledge related to predictors of burnout is limited. In Lin et al.’s cohort study evaluating the association between emotional intelligence and various well-being and burnout measures in surgery residents, they found emotional intelligence correlated strongly with psychological well-being and inversely with emotional exhaustion, depersonalization, and depression [22]. In a cohort study, Salles et al. assessed residents’ perseverance, burnout, psychological well-being, depression, and risk of attrition [23]. Regression analyses determined grit to be a significant positive predictor of psychological well-being and a negative predictor of depression and of frequency of thoughts of leaving residency training [23].
Bughi et al. evaluated whether the Myers-Briggs personality type can be used as a predictor of distress and burnout in medical students. Using the General Well-Being (GWB) scale and the Maslach Burnout Index (MBI), they found the GWB subscales are unique predictors of all 3 MBI dimensions [24]. They also found extroverts had lower depression scores and higher scores in positive well-being and self-control. Furthermore, those with a feeling personality type (vs thinking) had higher vitality scores on the GWB. A significant limitation of the study is the binary categorization of extroversion and introversion; in reality they exist on a continuum and can fluctuate depending on the circumstances. Furthermore, this study may be biased towards extroversion as is our society. Lastly, the validity of using non-DSM personality types as predictors for mental health outcomes has not been established.
Wachholtz and Rogoff showed medical students who have higher levels of spiritual well-being and daily spiritual experiences are less likely to experience burnout and are more likely to be satisfied with their lives [25]. Even after controlling for demographics, mental health variables, and adaptive coping, burnout remained significantly associated with lower scores on spirituality measures. This study supports the long-held belief that as long as tests are given, there will be prayer in schools. What needs to be explored is whether spiritual well-being comes from reading sacred texts, spiritual exercises, deriving insight and wisdom from a higher power, or being in community with others. Those who regularly attended spiritual services and were previously at decreased risk for burnout may now be at risk due to the abrupt cessation of services during the pandemic. On the contrary, they and others may also be turning more to their spiritual foundation for support. Just as spirituality is an important social determinant of health for patients, it is also important for clinicians, especially those who are vulnerable and early in their career [25]. In the spirit of learning from our patients, and consistent with providing high-quality care, it follows more work is needed in assessing spirituality’s role in preventing burnout [26].
In a 2018 to 2019 correlational, prospective cross-sectional study in medical residents, Fowler et al. found optimism remained constant from 2018 to 2019 and was negatively correlated with burnout [27•]. In addition, trait forgiveness, the disposition to forgive interpersonal transgressions over time and across situations, has been linked strongly with healthy workplace relationships, positive occupational outcomes, and general well-being. In a study exploring the link between trait forgiveness and well-being among physicians, hierarchical multiple regression modeling was used to examine burnout. Residents showed lower levels of burnout when their trait forgiveness was high [28•]. Although more study is needed, trait forgiveness and optimism, both of which may be pre-established character traits, might also be promising as potential character traits or skills that can be cultivated in order to protect residents from burnout.
Existing Wellness Programs and Interventions
Several studies have focused on developing wellness programs. Others have recommended adding physical exercise to medical school curricula to reap its mental health benefits. Although Bitonte and DeSanto support 90 min of weekly exercise or 30 min three times a week, they do not provide any pre or post data or outcomes [29]. Spiotta et al studied the impact of a pilot wellness initiative on anxiety, depression, quality of life, and sleepiness in 8 neurosurgery residents at the University of South Carolina. The program included biweekly wellness lectures, team-based exercise sessions, and independent activity (e.g., running, cycling). Although participants saw improvement in generalized anxiety, quality of life, and sleepiness using the same measures, no significant improvement in depression was found 1 year later [30]. Significant study limitations include the small sample size and lack of control group yielding difficulties in generalizability to other learners. Another small but national survey study of urology trainees examined the prevalence and influence of personal, programmatic, and institutional factors on burnout rates. [31] Although the response rate (20.9%) was small, the prevalence of burnout in urology trainees was high [31]. A multi-institutional cross-sectional survey of over 5000 obstetrics and gynecology residents found that self-directed activities were not always associated with increased well-being [32••]. Respondents identified alcohol use, social activity, cooking, napping, pursuing hobbies, reading, spiritual practices, playing an instrument, tobacco use, marijuana use, and exercise as activities they used to promote their well-being. However, the study found that only exercise was associated with reduced problems with wellness [32••]. The results of the study imply learners need guidance to pursue their well-being, and residency programs must be intentional in promoting wellness as a pillar of medical training. Thus, institutional factors such as formal mentorship and evidence-based programs and access to mental health services are important to learner well-being.
A common component of most wellness programs for learners is access to counseling services within the training environment. Golob et al. discussed the many causes of emotional distress among medical and surgical residents and fellows that led them to seek out counseling [33]. In an observational study, 14.1% of residents seeking counseling reported mental health, personal relationship, or career concerns, with the majority reporting severe distress per the counselors’ assessment [33]. The original intent of the academic or personal counseling was not well understood. However, Lazarus and Folkman discussed the importance of assessing both problem-focused and emotion-focused coping strategies for specific stressful encounters [34].
Unfortunately, most studies focusing on burnout prevention strategies are anecdotal, small, and underpowered and remain untested while assessments of interventions to prevent burnout often yield discouraging results. A small longitudinal study by Dyrbye et al. examined the impact of a mindfulness-based stress management course for two cohorts of first year Mayo Clinic medical students [35]. The course was a required part of the first-year core curriculum and was based on the Stress Management and Resilience Training (SMART) program. An interdisciplinary faculty (social workers, psychologists, and physicians) with specific expertise in communication, resilience, and small-group facilitation led small-group discussions throughout the year. Topics included the value and practice of gratitude, compassion, acceptance, meaning, and forgiveness. Students in the first cohort were also offered two 30-min individual meetings with a trained SMART facilitator; the second cohort was preemptively scheduled for these meetings. In total, the first cohort received 12 h of instruction while the second cohort received 10 h; all students received a copy of “The Mayo Clinic Guide to Stress-Free Living.” Despite the intervention, the study determined the participants had higher burnout scores and lower quality of life and empathy scores at the end of the first year compared to baseline measurements taken upon matriculation. How this translates to actual feelings of burnout remains unknown.
Most medical schools and training programs have programs designed to enhance wellness and mentoring as well as crisis management. However, no data on the efficacy, effectiveness, utilization, nor outcomes associated with these programs has been provided. Drolet and Rodgers provided information on Vanderbilt School of Medicine’s framework for a three-pronged wellness program consisting of mentoring and advising, student leadership, and personal growth [36]. The program consists of support from medical school staff and faculty as well as senior students. The University of Pittsburgh Medical Center Neurosurgery Wellness Initiative surveyed neurosurgery residents before and after instituting a series of initiatives including gym access and group gym visits, a mentoring program, and a lecture series targeting multiple facets of health and well-being. After a year of the wellness initiative, two-thirds of their residents still showed moderate to severe signs of burnout. Residents reported their work schedule and time availability were barriers to participating in the initiative, and less than half reported contentment with their work-life balance [37].
Slavin, Schindler, and Chibnall detailed the implementation of comprehensive integrated longitudinal efforts of Saint Louis University Medical School to improve medical student wellness through a series of curricular changes, after finding 57% of first year students reported moderate to high anxiety and 27% reported moderate to severe depression [38••]. Although the program was not designed to examine burnout, it was designed to guard medical student mental health using the requisite therapy-oriented services and by introducing a paradigm shift designed to address the causes of medical student distress by changing the curriculum (e.g., required resilience and mindfulness program, changing the placement and grading of human anatomy). As the curriculum evolved over the years, each class of medical students seemed to experience less psychological distress (i.e., depression and anxiety symptoms). Despite its promise, the authors noted significant limitations such as the lack of a comparison group at SLU or other comparable medical schools for comparison. Overall, despite decades of interest in learner burnout, little has changed in our understanding of how to prevent or mitigate it.
Environmental and Institutional Factors Contributing to Burnout
To enhance patient safety and quality care, reductions in duty hours were thought to be a mechanism to decrease burnout. Antiel et al.’s study on the effect of reducing duty hours in general surgery interns confirmed that emotional exhaustion and depersonalization were common experiences for residents. Even with reduced work hours, they showed nearly one-third of surgical interns reported weekly emotional exhaustion or depersonalization. Furthermore, suboptimal quality of life, burnout, and thoughts of giving up surgery were common among residents [39]. Similarly in a study of burnout in internal medicine residents and specialists, Panagopoulou et al. found the number of hours worked per week and emotional labor contributed to depersonalization and emotional exhaustion [40]. However, in West et al.’s repeated cross-sectional study of internal medicine residents, there were no significant associations between well-being measures and medical knowledge [41].
Surprisingly and despite their advocacy role, program directors may not always prioritize trainee well-being. In 2019, radiology program directors were surveyed to assess their knowledge of the common program requirements, department well-being curricula, and residency well-being innovations [42]. Most responding program directors (n = 121) agreed their knowledge was incomplete (67%), had not implemented a comprehensive well-being curriculum (74%), and did not offer the mandated burnout self-screening tool (53%). A minority (15%) did not offer residents protected time for medical, mental health, and dental appointments while 42% did not offer their trainees access to an institutional mental health clinic [42]. Carson et al.’s mixed-methods study of pediatric program directors evaluated their skillset in supporting resident well-being; the importance of doing so was a significant theme of the study responses. However, program directors noted it was an undervalued or unrecognized part of their job and they lacked the training to facilitate resident well-being [43•]. This study again shows there is little guidance about how to best support learners and prevent burnout even when there is a desire to do so. All in all, these studies highlight how little has been done to address or measure resident wellness and burnout and academic medicine’s failure to invest in resident physicians.
These data suggest that for a significant change in burnout rates to occur, several key factors must be addressed. It will require targeted initiatives focused on specific local needs, honest buy-in from departmental leaders, and physicians recognizing a problem exists. Since traditional methods of didactic instruction and mentoring alone are insufficient in preventing burnout, multifaceted approaches are needed. Active cultivation of traits and skills known to build resilience against burnout must be woven into wellness promotion curricula.
Both the medical school and residency training curricula and learners have significantly changed since the latter part of the twentieth century (1970s and 1980s) where most of the literature on learner burnout exists. These studies reveal medical students find difficulty balancing their professional and personal lives and make their academic pursuits their priority at the expense of their mental and physical health and well-being [44]. Furthermore, these articles suggest that the combined academic demands, emotional isolation, and status deprivation take a toll. These imbalanced lifestyles are problematic and yield limited time for recreational and social activities and contribute to physical and emotional exhaustion, depression, and even addiction and suicide. Despite a purported interest in learner health and well-being, the significant literature gap presents several challenges as twenty-first century learners are faced with increasing demands to acquire more knowledge faster and to produce more sooner. Hence, the literature needs to be reconceptualized or replicated for a new generation of learners who will face continued personal and professional issues amidst increased academic and clinical demands. What also remains unknown is whether ongoing changes to medical school curricula specialty specific training or unforeseen public health threats, e.g., COVID-19, will negatively or positively impact learner burnout.
Discussion
Burnout among physicians is a topic of great interest in the professional, academic, scientific, and lay community. It is well established that burnout and work-life balance can contribute to poor physician work satisfaction and suboptimal or worse patient outcomes. The approach to mitigating burnout is not a one size fits all and must include multidisciplinary science and an interprofessional team.
Dr. Sinsky, Vice President of Professional Satisfaction at the American Medical Association, stated that the optimal response to burnout “is to focus on fixing the workplace rather than focusing on fixing the worker…The ICD-11 definition of burnout is consistent with our research and our approach, which is that burnout is related to stressors within the environment rather than related to weakness on the part of susceptible individuals.” [45] A similar transformation, shifting the focus to changing the environment, needs to be carried out for learners. Learners joining the medical field are not only gaining clinical knowledge, they are also becoming acculturated to possible toxicity within the environment. Unfortunately, learners may be internalizing unhealthy norms regarding what is acceptable for personal well-being that may not be appropriate in the twenty-first century. Hence, the WHO’s approach to creating a healthy workspace can be adopted to spaces where learners participate. Building a healthy work environment includes implementing and enforcing health policies that identify distress, inform employees about available support, involve employees in decision-making, create employee career development programs, and recognize employee contributions.
In 1984, Muller stated, “It appears as though graduating medical students are worse off psychosocially than when they entered as first-years. The stress of medical education is probably one important determinant of this change. It is essential to revise the present system of general professional education for medical students.” [46] This remains true today.
Conclusions
We conclude with a few recommendations to move the field forward.
Future Research Directions
The research that is currently available is based on a population that does not reflect the gender, ethnic, racial, socioeconomic and demographic diversity of twenty-first century learners. Thus, new research is needed to guide us. Specifically, research on how social determinants of health such as race, ethnicity, gender, economic factors, language, acculturation, and family, community, spiritual, and health support systems influence learner well-being is essential. Multidisciplinary approaches are necessary to integrate qualitative and quantitative research methodologies such that research findings can be triangulated and translated into interventions. Well-designed, randomized control trials using validated and reliable measures should then be undertaken with an intervention and implementation lens. Furthermore, to the extent possible, measures should be developed that are learner-specific, and these measures should be used consistently to create a body of evidence across institutions and disciplines.
Efforts Must Be Directed at Prevention
Since depersonalization is difficult to remediate, efforts must be directed at prevention and new models incorporating what can be learned from other disciplines such as the military and airline industry. There is a need for more wellness programs focusing on the domains most important to learners and their patients. Consistent with modeling the organization’s vision statement, those responsible for advocating for learners, e.g., program directors and student affairs deans, should be accountable for ensuring learner health and well-being.
Considering most aptitude tests are essentially achievement tests and do not correlate with physician quality, consideration must be given to a holistic licensure, accreditation, and examination process. Due to the COVID-19 pandemic, many standardized examinations transitioned to a pass/fail grading system or were waived entirely. So as to not create additional, meaningless, and unneeded stress, a competency-based pass/fail system should be used in the examination process to ensure professionalism and competency while preventing burnout.
The expectations for wellness programs and assumptions about the relative “value” of self-care activities (e.g., exercise vs going to the movies) must be reset. No single intervention will solve the burnout problem and new multifaceted learner-centered wellness programs are needed. These programs should begin with the learner’s matriculation and continue throughout the medical training. They should focus on prevention and maintaining health and well-being as opposed to using a crisis-oriented response while incorporating learner perspectives and continuous evaluation and quality assurance principles. To support the learner’s self-care goals, well-designed programs should be detached from administration and include an assigned interdisciplinary mentoring and advocacy team—spiritual advisor, senior peer student/trainee advisor, athletic trainer, and counselor.
The National Academy of Medicine paid particular attention to learner burnout with their goal to create positive learning environments to reduce burnout and foster professional well-being. The American Psychiatric Association (APA) should assume leadership to move beyond the NAM report. The APA is uniquely positioned to establish protocols and mechanisms to assess the burden of burnout and craft unique solutions based on a multidisciplinary framework.
Lastly, a healthy physician workforce is vital to achieving the triple aims in healthcare and a safe, high-value health system. Thus, licensing (LCME and ACGME), accrediting (JCAHO), advocacy (AAMC), professional (APA), and scientific (NIH) organizations should institute programs to assess and monitor burnout within medical schools, training programs, and hospitals while also holding them accountable for ensuring clinician health and well-being.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Inc, G. Employee burnout, Part 1. The 5 main causes: Gallup.Com; 2018. https://www.gallup.com/workplace/237059/employee-burnout-part-main-causes.aspx. Accessed 2 Sept.
WHO. Burn-out an “occupational phenomenon”: International Classification of Diseases. WHO; World Health Organization. n.d.. Retrieved September 1, 2020, from http://www.who.int/mental_health/evidence/burn-out/en/. Accessed 1 Sept.
ICD-11—mortality and morbidity statistics. n.d.. Retrieved September 1, 2020, from https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/129180281. Accessed 1 Sept.
National Academies of Sciences, E. Taking action against clinician burnout: a systems approach to professional well-being 10.17226/25521. 2019.
Grant A. Burnout isn’t just in your head. It’s in your circumstances. The New York Times; 2020. https://www.nytimes.com/2020/03/19/smarter-living/coronavirus-emotional-support.html. Accessed 2 Sept.
Green CR, McCullough WR, Hawley JD. Visiting Black patients: racial disparities in security standby requests. J Natl Med Assoc. 2018;110(1):37–43. https://doi.org/10.1016/j.jnma.2017.10.009.
Bernstein L, Safarpour A. Mask shortage for most health-care workers extended into May, Post-Ipsos poll shows. Washington Post; n.d.. Retrieved September 1, 2020, from https://www.washingtonpost.com/health/mask-shortage-for-most-health-care-workers-extended-into-may-post-ipsos-poll-shows/2020/05/20/1ddbe588-9a21-11ea-ac72-3841fcc9b35f_story.html.
Blaschka, A. This is the best way to avoid COVID burnout. Forbes. n.d.. Retrieved September 2, 2020, from https://www.forbes.com/sites/amyblaschka/2020/07/30/this-is-the-best-way-to-avoid-covid-burnout/.
Grose J. School’s out. Parental burnout isn’t going away. The New York Times; 2020. https://www.nytimes.com/2020/06/23/parenting/parental-burnout-coronavirus.html. Accessed 2 Sept.
Medscape national physician burnout, depression & suicide report 2019. n.d. Medscape. Retrieved September 1, 2020, from http://www.medscape.com/slideshow/2019-lifestyle-burnout-depression-6011056. Accessed 1 Sept.
•• Center C, Davis M, Detre T, Ford DE, Hansbrough W, Hendin H, et al. Confronting depression and suicide in physicians. JAMA. 2003;289(23):3161. https://doi.org/10.1001/jama.289.23.3161. This article discusses the high rate of suicide among physicians.
•• Gold KJ, Sen A, Schwenk TL. Details on suicide among US physicians: data from the National Violent Death Reporting System. Gen Hosp Psychiatry. 2013;35(1):45–9. https://doi.org/10.1016/j.genhosppsych.2012.08.005. This article shows most of the physicians who die via suicide were not receiving mental health treatment.
•• Schernhammer ES, Colditz GA. Suicide rates among physicians: a quantitative and gender assessment (meta-analysis). Am J Psychiatry AJP. 2004;161(12):2295–302. https://doi.org/10.1176/appi.ajp.161.12.2295. This article shows physicians are more likely than the general population to die via suicide and female physicians are more likely than male physicians to die via suicide.
•• Mata DA, Ramos MA, Bansal N, Khan R, Guille C, Angelantonio ED, et al. Prevalence of depression and depressive symptoms among resident physicians. JAMA. 2015;314(22):2373. https://doi.org/10.1001/jama.2015.15845. This article shows the high prevalence of psychological distress among resident physicians.
When doctors struggle with suicide, their profession often fails them. n.d. NPR.Org. Retrieved September 1, 2020, from https://www.npr.org/sections/health-shots/2018/07/31/634217947/to-prevent-doctor-suicides-medical-industry-rethinks-how-doctors-work. Accessed 2 Sept.
Hoffman J. ‘I can’t turn my brain off’: PTSD and burnout threaten medical workers. The New York Times; 2020. https://www.nytimes.com/2020/05/16/health/coronavirus-ptsd-medical-workers.html. Accessed 1 Sept.
Brazeau CMLR, Shanafelt T, Durning SJ, Massie FS, Eacker A, Moutier C, et al. Distress among matriculating medical students relative to the general population. Acad Med. 2014;89(11):1520–5. https://doi.org/10.1097/ACM.0000000000000482.
•• Hansell M, Ungerleider R, Brooks C, Knudson M, Kirk J, Ungerleider J. Temporal trends in medical student burnout. Family Medicine; STFM. 2019. https://doi.org/10.22454/FamMed.2019.270753. This study highlights specific points in medical school at which students are particularly susceptible to burnout and notes dimensions of burnout that are difficult to reverse.
Wolf TM. Stress, coping and health: enhancing well-being during medical school. Med Educ. 1994;28(1):8–17; discussion 55-57. https://doi.org/10.1111/j.1365-2923.1994.tb02679.x.
Dunn LB, Iglewicz A, Moutier C. A conceptual model of medical student well-being: promoting resilience and preventing burnout. Acad Psychiatry. 2008;32(1):44–53. https://doi.org/10.1176/appi.ap.32.1.44.
Ratanawongsa N, Wright SM, Carrese JA. Well-being in residency: a time for temporary imbalance? Med Educ. 2007;41(3):273–80. https://doi.org/10.1111/j.1365-2929.2007.02687.x.
Lin DT, Liebert CA, Tran J, Lau JN, Salles A. Emotional intelligence as a predictor of resident well-being. J Am Coll Surg. 2016;223(2):352–8. https://doi.org/10.1016/j.jamcollsurg.2016.04.044.
Salles A, Lin D, Liebert C, Esquivel M, Lau JN, Greco RS, et al. Grit as a predictor of risk of attrition in surgical residency. Am J Surg. 2017;213(2):288–91. https://doi.org/10.1016/j.amjsurg.2016.10.012.
Bughi SA, Lie DA, Zia SK, Rosenthal J. Using a personality inventory to identify risk of distress and burnout among early stage medical students. Educ Health (Abingdon, England). 2017;30(1):26–30. https://doi.org/10.4103/1357-6283.210499.
Wachholtz A, Rogoff M. The relationship between spirituality and burnout among medical students. J Contemp Med Educ. 2013;1(2):83–91. https://doi.org/10.5455/jcme.20130104060612.
Ernecoff NC, Curlin FA, Buddadhumaruk P, White DB. Health care professionals’ responses to religious or spiritual statements by surrogate decision makers during goals-of-care discussions. JAMA Intern Med. 2015;175(10):1662–9. https://doi.org/10.1001/jamainternmed.2015.4124.
• Fowler JB, Fiani B, Kiessling JW, Khan YR, Li C, Quadri SA, et al. The correlation of burnout and optimism among medical residents. Cureus. 2020;12(2):e6860. https://doi.org/10.7759/cureus.6860. This prospective cross-sectional study identified optimism as a relative stable quality that is protective against burnout in residents in various disciplines.
• Firulescu L, May RW, Fincham FD, Arocha EA, Sanchez-Gonzalez MA. 147 Training forgiveness. A novel approach to reducing physician burnout. CNS Spectr. 2020;25(2):293–4. https://doi.org/10.1017/S1092852920000632. This study identified trait-forgiveness as a characteristic that is associated with lower levels of burnout in residents.
Bitonte RA, DeSanto DJ. Mandatory physical exercise for the prevention of mental illness in medical students. Ment Illn. 2014;6(2):5549. https://doi.org/10.4081/mi.2014.5549.
Spiotta AM, Fargen KM, Patel S, Larrew T, Turner RD. Impact of a residency-integrated wellness program on resident mental health, sleepiness, and quality of life. Neurosurgery. 2019;84(2):341–6. https://doi.org/10.1093/neuros/nyy112.
Marchalik D, Brems J, Rodriguez A, Lynch JH, Padmore J, Stamatakis L, et al. The impact of institutional factors on physician burnout: a national study of urology trainees. Urology. 2019;131:27–35. https://doi.org/10.1016/j.urology.2019.04.042.
•• Winkel AF, Woodland MB, Nguyen AT, Morgan HK. Associations between residents’ personal behaviors and wellness: a national survey of obstetrics and gynecology residents. J Surg Educ. 2020;77(1):40–4. https://doi.org/10.1016/j.jsurg.2019.08.014. This single-group, multi-institutional cross-sectional survey represents the largest cohort study of residents to evaluate traits and activities protective against burnout.
Golob A, Beste LA, Stern M, Johnson K. Emotional distress among physician residents and fellows: an observational study of trainees seeking counseling visits. Acad Psychiatry. 2018;42(1):25–30. https://doi.org/10.1007/s40596-017-0740-2.
Lazarus RS, Folkman S. Stress, appraisal, and coping: Springer publishing company; 1984.
Dyrbye LN, Shanafelt TD, Werner L, Sood A, Satele D, Wolanskyj AP. The impact of a required longitudinal stress management and resilience training course for first-year medical students. J Gen Intern Med. 2017;32(12):1309–14. https://doi.org/10.1007/s11606-017-4171-2.
Drolet BC, Rodgers S. A comprehensive medical student wellness program—design and implementation at Vanderbilt School of Medicine. Acad Med. 2010;85(1):103–10. https://doi.org/10.1097/ACM.0b013e3181c46963.
Ares WJ, Maroon JC, Jankowitz BT. In pursuit of balance: the UPMC Neurosurgery Wellness Initiative. World Neurosurg. 2019;132:e704–9. https://doi.org/10.1016/j.wneu.2019.08.034.
•• Slavin SJ, Schindler DL, Chibnall JT. Medical student mental health 3.0: improving student wellness through curricular changes. Acad Med. 2014;89(4):573–7. https://doi.org/10.1097/ACM.0000000000000166. This article provides an overview of a comprehensive integrated longitudinal curriculum at Saint Louis University Medical School that is designed to prevent psychological distress among medical students.
Antiel RM, Reed DA, Van Arendonk KJ, Wightman SC, Hall DE, Porterfield JR, et al. Effects of duty hour restrictions on core competencies, education, quality of life, and burnout among general surgery interns. JAMA Surg. 2013;148(5):448–55. https://doi.org/10.1001/jamasurg.2013.1368.
Panagopoulou E, Montgomery A, Benos A. Burnout in internal medicine physicians: differences between residents and specialists. Eur J Intern Med. 2006;17(3):195–200. https://doi.org/10.1016/j.ejim.2005.11.013.
West CP, Shanafelt TD, Cook DA. Lack of association between resident doctors’ well-being and medical knowledge. Med Educ. 2010;44(12):1224–31. https://doi.org/10.1111/j.1365-2923.2010.03803.x.
Jordan SG, Robbins JB, Sarkany D, England E, Kalia V, Patel MD, et al. The Association of Program Directors in Radiology Well-Being 2019 Survey: identifying residency gaps and offering solutions. J Am Coll Radiol. 2019;16(12):1702–6. https://doi.org/10.1016/j.jacr.2019.06.017.
• Carson SL, Perkins K, Reilly MR, Sim M-S, Li S-TT. Pediatric program leadership’s contribution toward resident wellness. Acad Pediatr. 2018;18(5):550–5. https://doi.org/10.1016/j.acap.2018.02.013. This study highlights the lack of guidance for program directors on how to best support learners and prevent burnout despite the acknowledgment of its central importance to their role.
Gaensbauer TJ, Mizner GL. Developmental stresses in medical education. Psychiatry. 1980;43(1):60–70. https://doi.org/10.1080/00332747.1980.11024050co.
WHO adds burnout to ICD-11. What it means for physicians. n.d.. American Medical Association. Retrieved September 1, 2020, from https://www.ama-assn.org/practice-management/physician-health/who-adds-burnout-icd-11-what-it-means-physicians.
Physicians for the twenty-first century. Report of the Project Panel on the General Professional Education of the Physician and College Preparation for Medicine. J Med Ed. 1984;59(11):1–208 Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=ovfta&NEWS=N&AN=00004999-198411000-00001. Accessed 2 Sept.
Acknowledgments
The editors would like to thank Dr. Victor Schwartz for taking the time to review this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical collection on Complex Medical-Psychiatric Issues
Rights and permissions
About this article

Cite this article
Gaston-Hawkins, L.A., Solorio, F.A., Chao, G.F. et al. The Silent Epidemic: Causes and Consequences of Medical Learner Burnout. Curr Psychiatry Rep 22, 86 (2020). https://doi.org/10.1007/s11920-020-01211-x
Accepted:
Published:
DOI: https://doi.org/10.1007/s11920-020-01211-x