
Abstract
Background
Femoroacetabular impingement (FAI) morphology can lead to range-of-motion deficits in football players. It is therefore important for physicians treating these players to be aware of the location and implications of FAI morphology.
Purpose/Questions
We sought to characterize the radiographic deformity and dynamic impingement observed in a consecutive series of American football linemen with symptomatic, mechanical hip pain who underwent surgical treatment for FAI and to use software analysis to identify the location of impingement and terminal range of motion and the effects of simulated correction.
Methods
A retrospective analysis was conducted of 17 hips in 13 football linemen who underwent arthroscopic correction for symptomatic FAI. Computed tomography (CT) scans were used to generate preoperative three-dimensional models of the hips. Femoral and acetabular measurements, maximum hip flexion, abduction, internal rotation at 90° flexion (IR90), and flexion/adduction/internal rotation (FADIR) were determined, and areas of bony collision were defined. Simulated femoral correction was performed and motion analysis was repeated.
Results
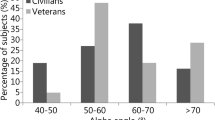
Mean femoral version was 13.1° (range, 0 to 26°), while mean femoral neck-shaft angle was 132.1° (range, 123 to 145°). Mean maximum alpha angle on the radial reformatted CT was 69.2° (range, 48 to 95°) and was located at the 12:45 clock-face position (range, 11:30 to 2:15). Mean acetabular version values at 1:30 and 3:00 were 1.1° (range, − 11 to 11°) and 12.7° (range, 2 to 20°), respectively. Fifty-three percent of hips showed a “crossover” sign. Mean lateral center-edge angle was 31.7° (range, 25 to 44°). CT-derived motion analysis demonstrated a mean preoperative flexion of 108.2° (range, 73 to 127°), IR90 of 20.5° (range, 0 to 52°), and FADIR of 12.3° (range, 0 to 39°). Simulated correction resulted in significant improvements in flexion (6.6°), IR90 (11.3°), and FADIR (10.6°).
Conclusions
While cephalad retroversion was observed in approximately half of the hips, a significant cam deformity was seen maximally at 12:45, a more posterior cam location than that of the general population. Managing this pathology required obtaining preoperative and intraoperative images to characterize lesions and allow for their complete correction. With complete correction of the deformity, simulated range of motion demonstrated significant improvement in flexion, IR90, and FADIR maneuvers.


Similar content being viewed by others


References
Agricola R, Waarsing JH, Thomas GE, Carr AJ, Reijman M, Bierma-Zeinstra SMA, et al. Cam impingement: defining the presence of a cam deformity by the alpha angle: data from the CHECK cohort and Chingford cohort. Osteoarthritis Cartilage. 2014;22(2):218–225.
Alradwan H, Philippon MJ, Farrokhyar F, Chu R, Whelan D, Bhandari M, et al. Return to preinjury activity levels after surgical management of femoroacetabular impingement in athletes. Arthroscopy. 2012;28:1567–1576.
Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med. 2001;29:521–533.
Ayeni OR, Adamich J, Farrokhyar F, Simunovic N, Crouch S, Philippon MJ, et al. Surgical management of labral tears during femoroacetabular impingement surgery: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2014;22:756–762.
Ayeni OR, Belzile EL, Musahl V, Naudie D, Crouch S, Sprague S, et al. Results of the PeRception of femOroaCetabular impingEment by Surgeons Survey (PROCESS). Knee Surg Sports Traumatol Arthrosc. 2014;22:906–910.
Beaule PE, Zaragoza E, Motamedi K, Copelan N, Dorey FJ. Three-dimensional computed tomography of the hip in the assessment of femoroacetabular impingement. J Orthop Res. 2005;23:1286–1292.
Bedi A, Dolan M, Hetsroni I, Magennis E, Lipman J, Buly R, Kelly BT. Surgical treatment of femoroacetabular impingement improves hip kinematics: a computer-assisted model. Am J Sports Med. 2011;39 Suppl:43S–49S.
Bedi A, Dolan M, Magennis E, Lipman J, Buly R, Kelly BT. Computer-assisted modeling of osseous impingement and resection in femoroacetabular impingement. Arthroscopy. 2012;28:204–210.
Bogunovic L, Gottlieb M, Pashos G, Baca G, Clohisy JC. Why do hip arthroscopy procedures fail? Clin Orthop Relat Res. 2013;471:2523–2529.
Botser IB, Smith TW, Nasser R, Domb BG. Open surgical dislocation versus arthroscopy for femoroacetabular impingement: a comparison of clinical outcomes. Arthroscopy. 2011;27:270–278.
Casartelli NC, Leunig M, Maffiuletti NA, Bizzini M. Return to sport after hip surgery for femoroacetabular impingement: a systematic review. Br J Sports Med. 2015;49:819–824.
Chaudhry H, Ayeni OR. The etiology of femoroacetabular impingement: what we know and what we don’t. Sports Health. 2014;6:157–161.
Clohisy JC, Dobson MA, Robison JF, Warth LC, Zheng J, Liu SS, Yehyawi TM, Callaghan JJ. Radiographic structural abnormalities associated with premature, natural hip-joint failure. J Bone Joint Surg Am. 2011;93 Suppl 2:3–9.
Domayer SE, Ziebarth K, Chan J, Bixby S, Mamisch TC, Kim YJ. Femoroacetabular cam-type impingement: diagnostic sensitivity and specificity of radiographic views compared to radial MRI. Eur J Radiol. 2011;80:805–810.
Dudda M, Albers C, Mamisch TC, Werlen S, Beck M. Do normal radiographs exclude asphericity of the femoral head-neck junction? Clin Orthop Relat Res. 2009;467:651–659.
Feeley BT, Powell JW, Muller MS, Barnes RP, Warren RF, Kelly BT. Hip injuries and labral tears in the national football league. Am J Sports Med. 2008;36:2187–2195.
Frank RM, Lee S, Bush-Joseph CA, Kelly BT, Salata MJ, Nho SJ. Improved outcomes after hip arthroscopic surgery in patients undergoing T-capsulotomy with complete repair versus partial repair for femoroacetabular impingement: a comparative matched-pair analysis. Am J Sports Med. 2014;42: 2634–2642.
Gerhardt MB, Romero AA, Silvers HJ, Harris DJ, Watanabe D, Mandelbaum BR. The prevalence of radiographic hip abnormalities in elite soccer players. Am J Sports Med. 2012;40:584–588.
Hetsroni I, Larson CM, Dela Torre K, Zbeda RM, Magennis E, Kelly BT. Anterior inferior iliac spine deformity as an extra-articular source for hip impingement: a series of 10 patients treated with arthroscopic decompression. Arthroscopy. 2012;28:1644–1653.
Hetsroni I, Poultsides L, Bedi A, Larson CM, Kelly BT. Anterior inferior iliac spine morphology correlates with hip range of motion: a classification system and dynamic model. Clin Orthop Relat Res. 2013;471:2497–2503.
Heyworth BE, Shindle MK, Voos JE, Rudzki JR, Kelly BT. Radiologic and intraoperative findings in revision hip arthroscopy. Arthroscopy. 2007;23:1295–1302.
Kapron AL, Anderson AE, Aoki SK, Phillips LG, Petron DJ, Toth R, Peters CL. Radiographic prevalence of femoroacetabular impingement in collegiate football players: AAOS Exhibit Selection. J Bone Jt Surgery Am. 2011;93:e111(1–10).
Kapron AL, Anderson AE, Peters CL, Phillips LG, Stoddard GJ, Petron DJ, et al. Hip internal rotation is correlated to radiographic findings of cam femoroacetabular impingement in collegiate football players. Arthroscopy. 2012;28:1661–1670.
Khan M, Ayeni O, Madden K, Bedi A, Ranawat AS, Kelly BT, et al. Femoroacetabular impingement: have we hit a global tipping point in diagnosis and treatment? Results from the InterNational Femoroacetabular Impingement Optimal Care Update Survey (IN FOCUS). Arthroscopy. 2016;32(5):779–787.
Khan M, Bedi A, Fu F, Karlsson J, Ayeni OR, Bhandari M. New perspectives on femoroacetabular impingement syndrome. Nat Rev Rheumatol. 2016;12:303–310.
Khan M, Habib A, de Sa D, Larson CM, Kelly BT, Bhandari M, et al. Arthroscopy up to date: hip femoroacetabular impingement. Arthroscopy. 2016;32:177–189.
Khan M, Ranawat A, Williams D, Gandhi R, Choudur H, Parasu N, et al. Relationship between the alpha and beta angles in diagnosing cam-type femoroacetabular impingement on frog-leg lateral radiographs. Knee Surg Sports Traumatol Arthrosc. 2015;23(9):2595–2600.
Larson CM, Sikka RS, Sardelli MC, Byrd JWT, Kelly BT, Jain RK, et al. Increasing alpha angle is predictive of athletic-related “hip” and “groin” pain in collegiate National Football League prospects. Arthroscopy. 2013;29:405–410.
Milone MT, Bedi A, Poultsides L, Magennis E, Byrd JWT, Larson CM, et al. Novel CT-based three-dimensional software improves the characterization of cam morphology. Clin Orthop Relat Res. 2013;471:2484–2491.
Nepple JJ, Brophy RH, Matava MJ, Wright RW, Clohisy JC. Radiographic findings of femoroacetabular impingement in National Football League Combine athletes undergoing radiographs for previous hip or groin pain. Arthroscopy. 2012;28:1396–1403.
Nepple JJ, Martel JM, Kim YJ, Zaltz I, Clohisy JC, Group AS. Do plain radiographs correlate with CT for imaging of cam-type femoroacetabular impingement? Clin Orthop Relat Res. 2012;470:3313–3320.
Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Jt Surgery Br. 2002;84:556–560.
Nwachukwu BU, Rebolledo BJ, McCormick F, Rosas S, Harris JD, Kelly BT. Arthroscopic versus open treatment of femoroacetabular impingement: a systematic review of medium- to long-term outcomes. Am J Sports Med. 2016;44(4):1062–1068.
Packer JD, Safran MR. The etiology of primary femoroacetabular impingement: genetics or acquired deformity? J Hip Preserv Surg. 2015;2:249–257.
Pfirrmann CWA, Mengiardi B, Dora C, Kalberer F, Zanetti M, Hodler J. Cam and pincer femoroacetabular impingement: characteristic MR arthrographic findings in 50 patients. Radiology. 2006;240:778–785.
Philippon MJ, Schenker ML, Briggs KK, Kuppersmith DA, Maxwell RB, Stubbs AJ. Revision hip arthroscopy. Am J Sports Med. 2007;35:1918–1921.
Ross JR, Bedi A, Stone RM, Sibilsky Enselman E, Kelly BT, Larson CM. Characterization of symptomatic hip impingement in butterfly ice hockey goalies. Arthroscopy. 2015;31:635–642.
Ross JR, Bedi A, Stone RM, Sibilsky Enselman E, Leunig M, Kelly BT, et al. Intraoperative fluoroscopic imaging to treat cam deformities: correlation with 3-dimensional computed tomography. Am J Sports Med. 2014;42:1370–1376.
Ross JR, Larson CM, Adeoye O, Adeoyo O, Kelly BT, Bedi A. Residual deformity is the most common reason for revision hip arthroscopy: a three-dimensional CT study. Clin Orthop Relat Res. 2015;473:1388–1395.
Sampson JD, Safran MR. Biomechanical implications of corrective surgery for FAI: an evidence-based review. Sports Med Arthrosc Rev. 2015;23:169–173.
Sawyer GA, Briggs KK, Dornan GJ, Ommen ND, Philippon MJ. Clinical outcomes after arthroscopic hip labral repair using looped versus pierced suture techniques. Am J Sports Med. 2015;43:1683–1688.
Shindle MK, Voos JE, Heyworth BE, Mintz DN, Moya LE, Buly RL, et al. Hip arthroscopy in the athletic patient: current techniques and spectrum of disease. J Bone Joint Surg Am. 2007;89 Suppl 3:29–43.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Moin Khan, MD, and Benjamin C. Noonan, MD, declare that they have no conflicts of interest. James R. Ross, MD, reports being a paid consultant and educator for Smith & Nephew, outside the submitted work. Bryan T. Kelly, MD, reports receiving personal fees from Arthrex, outside the submitted work. Christopher M. Larson, MD, reports receiving personal fees as a consultant from Smith & Nephew and A3 Surgical and stock options from A3 Surgical, outside the submitted work. Asheesh Bedi reports receiving personal fees from Arthrex, outside the submitted work.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was obtained from all patients for being included in this study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.
Additional information
Level of Evidence: Level IV, Case Series
Rights and permissions
About this article

Cite this article
Ross, J.R., Khan, M., Noonan, B.C. et al. Characterization and Correction of Symptomatic Hip Impingement in American Football Linemen. HSS Jrnl 14, 128–133 (2018). https://doi.org/10.1007/s11420-018-9605-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11420-018-9605-9