
Abstract
Introduction
A decline in sports activities among children and adolescents was noted during the stay-at-home restrictions imposed by COVID-19. With the easing of restrictions, physical activities are being resumed.
Evidence acquisition
A data search was conducted to identify the role of parents in resuming sporting activities, the risks and benefits of doing so, the physical examination to be conducted prior to physical activity, the existence of guidelines/protocols for return to sports and physical activity, the role of comorbidities in influencing the restart of the same.
Evidence synthesis
Parents should consult the child’s physician prior to allowing he/she to resume physical exercise. In preparation for this, a careful physical examination should be performed. Children with COVID-19, even if asymptomatic, should not resume any physical activity until at least 10 days after testing positive. Those with moderate or severe COVID-19 should be referred for cardiological evaluation. The level of activity should be resumed gradually, as per the GRTP protocol. Athletes with a positive COVID-19 test in the presence of concomitant medical conditions (diabetes, cardiovascular or respiratory or renal disease) should undergo medical evaluation prior to adhering to a GRTP. Those with complicated COVID19 infection or long Covid may need additional investigations.
Conclusions
While there is no doubt that it will bring multiple benefits in terms of general health, returning to play sport should be gradual and preceded by an accurate physical examination in those young subjects previously affected by the coronavirus disease, especially when their heart and/or lungs and/or kidneys were affected.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The global expansion of the COVID-19 pandemic, characterised by a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), represents a major ongoing threat to public health. In an attempt to combat the spread of infection, governments worldwide have issued recommendations aimed at restricting personal contacts and mobility [1]. Lockdowns have been implemented globally to control the COVID-19 pandemic, limiting daily activities, including schooling and physical education in young people, resulting in extended periods of scarce activity [2, 3].
A data search was conducted to assess the effect of lockdown on children and adolescents and to determine how best to resume sporting activities in a safe environment. Specifically, the search was aimed at identifying the role of parents in resuming sporting activities, the risks and benefits of doing so, the physical examination to be conducted prior to physical activity, the existence of guidelines/protocols for return to sports and physical activity, the role of comobidities in influencing the restart of sports activities.
Search strategy
A systematic electronic search into Pubmed/Medline, Scopus, and Web of Science databases was performed from their inception up to December 10th, 2021. All searches were conducted using Boolean operators to combine MeSH terms and free text words. The following terms were searched: children, adolescents, parents, COVID-19, SARS-CoV-2, sport, physical activity, exercise, guidelines, protocol, comorbidities.
Sources
Reference lists of the identified papers and relevant manuscripts were examined. Emails were sent to the Authors of the above articles for further information when needed. Five reviewers were calibrated for the identification of eligible studies (Calcaterra G, Fanos V, Cataldi L, Cugusi L, and Crisafulli A) by a sixth reviewer (Bassareo PP) through successive stages of quintuplicate independent screening among randomly selected titles and abstracts in groups of five, until a complete intra-examiner agreement was obtained (k scores from the first to the last calibration exercise: 0.79, 0.82, 0.89, 0.94 and 1). A parallel, quadruple-blind screening procedure of all titles and abstracts retrieved by the electronic search was performed by four reviewers (Calcaterra G, Fanos V, Cugusi L, and Crisafulli A). The titles and abstracts were screened for subject importance. Studies that were not definitively excluded on the basis of abstract information were also selected for full-text screening. The reviewers examined the full text of all relevant studies to evaluate the possibility of inclusion. In the case of disagreement over study inclusion, a discussion was held with the sixth reviewer (Bassareo PP) to reach an agreement. Studies were eligible for inclusion on meeting the following criterion: all studies relating to the need for resuming sports activities in youth during the COVID-19 pandemic with no limitation on the period of publication. The exclusion criteria were as follows: (a) studies not focused on the topic selected; (b) papers in a language other than English; (c) duplicates, and (d) studies not available from libraries for full-text assessment.
Data extraction
Five reviewers (Calcaterra G, Fanos V, Cataldi L, Cugusi L, and Crisafulli A) independently extracted data using a structured form specifically developed for this review. The following information was extracted from each included study: authors, year of publication, type of paper, need for resuming physical activities, age of the targeted people, familiar/environmental/health factors influencing such a restart in physical activities, and already published consensus documents/guidelines/protocols in the field. Thus, five possible outcomes were recognized: (a) the role of parents in resuming sporting activities; (b) the risks and benefits of doing so; (c) the physical examination to be conducted prior to physical activity; (d) the existence of guidelines/protocols for return to sports and physical activity; (e) the role of comorbidities in influencing the restart of sports activities.
Any discrepancy that occurred during data extraction was solved by consensus or discussion with the fifth reviewer (Bassareo PP).
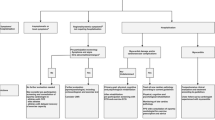
As this systematic review included a large number of heterogeneous study designs and sources, the findings of our data search have been summarized in the form of a narrative review (see Fig. 1 for the flow chart concerning research strategy).

Flow chart of the study selection process
General considerations
Data collected by the American Academy of Paediatrics on May 13th revealed how more than 3.94 million children had contracted COVID-19 infection, and approximately 16,000 hospitalized. A total of approximately 316 children have died in the United States, with COVID-19 listed as one of the 10 major causes of death in children since the start of the pandemic in late 2019 [4].
Severe illness in this age group however remains rare. The USA, UK, Italy, Germany, Spain, France, and South Korea have reported a death rate of 0.17 per 100,000 children up to February 2021, compared to 48 per 100,000 of estimated total mortality from all causes in a normal year [5].
Children who contract COVID-19 infection frequently display no symptoms, whilst others experience fever, cough, difficulty breathing, muscle aches, headache, or diarrhoea [6].
Unfortunately, older children and/or those of Black, Hispanic, Asian or American Indian extraction are at higher risk of severe disease and death from COVID-19. The results remained consistent even once key demographic factors and specific pre-existing comorbidities had been taken into account [7]. A cross-sectional study of 43,465 patients aged 18 or younger affected by COVID-19 revealed how more than 25% of subjects presented with at least one concurrent condition; asthma, obesity, neurodevelopmental disorders, together with specific mental health conditions were the most frequently observed. These conditions were associated with a higher risk of severe COVID-19 illness [8].
Following COVID-19 infection, children are at risk of developing multisystem inflammatory syndrome (MIS-C), Kawasaki-like syndrome or being affected by long COVID, associated with the onset of inflammation of the heart and lung tissues. Symptoms of MIS-C, an abnormal immune response following COVID-19 infection in children, develop 2 to 4 weeks following the initial COVID-19 infection [9, 10].
SARS-CoV-2 is capable of affecting all organs throughout the body, at times leading to inflammatory vasculopathy, with children requiring careful monitoring or admittance to the ICU for treatment. Due to the ongoing pandemic, additional data should be collected from children affected by long COVID to assess the damage caused by the virus and the effects produced on the children’s mental health and wellbeing [11].
Resuming play or physical activity following COVID-19 infection
Across the US and the EU, approximately 35 to 45 million young people are actively involved in some form of physical activity [12].
The COVID-19 pandemic has produced a significant impact on the lives of children and their families. A lack of sports and physical exercise has at times resulted in the onset of eating disorders, poor quality sleep and reduced sense of wellbeing [13].
Moreover, a lack of physical activity may result in breathing problems, reduced muscle tone and loss of sport-specific skills. On resuming activity, a rapid increase in energy demand may increase the risk of injury if adequate periods of acclimatization and recovery are not envisaged [13].
A rapid rise in frequency, duration and intensity of physical activity all constitute risk factors for injury, including stress fracture and tendinopathy [13].
Children affected by long-term complications of COVID-19 should obtain appropriate medical certification to ensure a safe return to physical activity. Indeed, many paediatricians are of the opinion that all young people who have contracted COVID-19 infection should be assessed and their symptoms reviewed prior to resuming physical activity [14].
Additional testing may be prescribed for children receiving irregular findings. Although the majority of children will be able to safely resume physical activity, a few may need to take a slower, gradual approach to safely resume their pre-COVID-19 activity levels [14].
Medical advice should be promptly sought if children experience any unexpected difficulties in resuming play. Children and adolescents who are athletically competitive should moreover be carefully assessed prior to resuming sports or physical activity [14].
The role of parents
Parents should be aware of the potential long-term consequences of COVID-19 and seek medical advice if their children display symptoms including persistent fever, difficulty breathing, chest pain, palpitations, dizziness, swelling of hands or feet, or fatigue following COVID-19 infection. If their child practises sport or takes part in physical activities, they should consult the child’s physician prior to allowing their son or daughter to resume physical exercise [14,15,16]. Current guidelines recommend that all children over the age of 12 should be vaccinated against COVID-19 [17].
In preparing to return to sports and physical activities, both parents and athletes attending medical appointments are bound to ask questions relating to the best way of achieving this as safely as possible. Physicians should raise awareness in families of the measures to be taken to mitigate risk and prevent the spread of COVID-19 [18].
The risks and benefits of resuming sports and physical activity
Physicians are univocal in recommending that children and adolescents resume sports and/or physical activities once measures aimed at mitigating the transmission of COVID-19 are in place [14, 17].
The present review relates to children and adolescents who engage in, or wish to resume, sports and other physical activities, providing an overview of the impact produced by a lack of physical activity programmes for young people. Moreover, the key contribution afforded by the correct application of risk mitigation strategies, advising all people to have their COVID-19 vaccination and to use face masks in sporting environments is highlighted [19].
The participation of children and young people in sports and physical activities produces a series of physical and psychological benefits, promoting cardiovascular health, strength and physical fitness. Increased socializing with fellow athletes and coaches, together with a return to a more structured routine are also highly beneficial aspects that may contribute toward developmental growth and boosting of the immune system [14, 17, 20, 21].
On resuming physical activity, children should increase the frequency, duration and intensity of physical activity in a gradual manner in order to prevent injury. Indeed, in growing children, a rapid increase in physical activity may contribute stress injuries. Moreover, following a period of inactivity, athletes may be at risk of exertion-related conditions such as muscle cramps, heat-related syncope, heat exhaustion and heat stroke, due to a difficulty in dissipating body heat [14, 17, 20, 22, 23].
Physical examination prior to physical activity
Physicians should counsel parents and children to underline the need to resume sports and physical activities gradually after a period of inactivity.
In preparation for this, a careful physical examination should be performed based on the child’s personal and family history, prior to resuming physical activities to screen for risk factors for injury and sudden death. History of COVID-19 infection and symptoms should also be assessed [14, 17].
Children who contract COVID-19 infection, even in the absence of symptoms, should not resume physical activity until at least 10 days after testing positive. All children should undergo a thorough physical examination to identify chest pain, shortness of breath, syncope and palpitations [14, 17]. Children affected by moderate or severe COVID-19 infection should be referred for cardiological evaluation [24].
Guidelines for return to sports and physical activity
Children and adolescents will likely be keen to resume their sports and physical activities as soon as possible. However, the importance of increasing the level of activity in a gradual manner should be underlined [14, 17].
A gradual increase in sports should be based on a pre-established activity schedule. Indeed, taking into account previous activity levels, sports should be resumed at a level of no more than 25–50% of their previous participatory output. Adequate recovery times should be scheduled between activities. Activity loads may be increased as the body adapts to increasing demands. Conversely, loads should be decreased if difficulties in maintaining the progression of activity are experienced [25, 26].
When resuming physical activity, the main focus should be on skill sets and movement, whilst competitive levels should be reached gradually. Progression to previous levels of activity should take into account the duration of inactivity and proceed gradually, especially in competitive sports. Lengthier periods of inactivity will dictate a need for the child to progress at a slower pace [25, 26].
Gradual return to play (GRTP) protocol
The GRTP protocol is aimed at reintroducing sports and physical activity in a gradual manner [27] (See Table 1).
Key considerations
-
Prior to implementing a GRTP, the athlete should be able to complete routine activities and walk 500 m without experiencing severe fatigue or breathlessness.
-
Athletes who tested positive should be symptom-free for at least 7 days and undergo a 10 day rest period prior to resuming physical activities.
-
More rapid progress may be made with sports such as golf, which are less aerobically intense, although athletes purportedly require more than 3 weeks to return to their previous condition [27].
Initial monitoring may be beneficial to assess the following:
-
Resting heart rate.
-
Self-perceived exertion.
-
Quality of sleep, stress, fatigue, and muscle soreness.
-
Injury-Psychological Readiness to Return to Sport.
Should symptoms, including severe fatigue, be manifested whilst adhering to a GRTP, the athlete should not progress further but return to the previous step and undergo a symptom-free period of at least 24 h rest [27].
Comorbidities in athletes
Athletes who receive a positive COVID-19 test in the presence of concomitant medical conditions including diabetes and cardiovascular or respiratory or renal disease should undergo medical evaluation prior to adhering to a GRTP [28,29,30].
Further assessments
Athletes characterized by complex COVID-19 infection or long COVID may need to undergo additional investigations, including.
-
Blood testing for markers of inflammation (high sensitivity-Troponin, Brain Natriuretic Peptide and C reactive protein).
-
Cardiac monitoring (12-lead ECG, echocardiogram, exercise tolerance test, and cardiac MRI).
-
Respiratory function assessment (spirometry).
-
Renal and haematological monitoring [27].
Discussion
So far not particularly extended scientific literature on resuming sports activities in young people has been summarized in this review. COVID-19 pandemic has negatively impacted the life of a number of children and adolescents worldwide, in terms of compelling them to stay at home and not to practice sport. This forced cocooning has led to unhealthy habits, such as an excess in food intake which in turn has caused an increased incidence of overweight, and low mood, owing to the sense of isolation and the lack of social interaction with their peers. With the cautious reopening, there is a need for resuming sports activities and physical exercise.
However, this cannot be done without precaution, for many reasons. First, the risk of muscular injuries due to muscular deconditioning. Parents should consult their child’s physician prior to allowing the same child to resume physical exercise. This is to make sure that the child is ready to play exercise. In preparation for this, a careful physical examination is mandatory. Children with COVID-19, even if they are asymptomatic, should not resume any physical activity until at least 10 days after testing positive. The stay-at-home period should be extended in case of prolonged positivity. Young people with moderate or severe COVID-19 should be referred for cardiological evaluation. This is because a cardiac involvement is not rare even in children, myocarditis, pericarditis, and MIS-C with or without coronary arteries dilatation/aneurysms being the most harmful manifestations of the disease. The level of activity should be resumed gradually, as per that reported in the GRTP protocol. At least seven days are needed before returning to full activities, including competitive sports. Young athletes with a positive COVID-19 test in the presence of concomitant medical conditions (diabetes, cardiovascular or respiratory or renal disease) should undergo an in-depth medical evaluation prior to adhering to a GRTP. Those with complicated COVID-19 infection or long COVID may need additional investigations.
Though COVID-19 represents and absolute and unpredictable novel situation, the current suggestions concerning resuming physical activity in children and adolescents are in accordance with that previously outlined in a number of documents on restarting playing sport following any injury or long-lasting inactivity [31, 32]. The two most important principles in the field are caution and graduality. Both are evidence-based and support the concept of post-injury vulnerability. In this respect, the GRTP protocol is an objective tool providing progressive tasks to the young athlete, although limited validation of the same is available. Additional research is needed to validate it, which is consistent with almost any previous documents on resuming exercise after different kinds of injuries [27, 33]. The approach to post-COVID athletes who are vulnerable because of comorbidities or who are suffering from long-COVID is similar to the way to manage those at risk of prolonged post-injury symptoms or other long-term complications. In fact, recovery from injury and medical care to full performance can be a lengthy and difficult process [34].
Overall, all the available scientific evidence suggests promoting physical activity resumption in young people after COVID-19. The proposed approach, however, should be cautious, gradual, and preceded by a physical examination done by a general paediatrician or general practitioner and sometimes by a specialist in Cardiology. This is with the goal of certifying that the young athlete is fit and ready to restart playing sport.
Conclusions
Public health authorities worldwide should recognize the potentially negative consequences that may be produced on the physical and mental health of young people by cutting-back sports and other physical activities during periods of lockdown. It is an acknowledged fact that lockdowns have invariably generated a negative impact on levels of physical fitness, socialization and life satisfaction amongst children and adolescents, at times resulting in a detrimental self-perception of well-being. Indeed, as the young frequently have a very active lifestyle, they have proved to be particularly susceptible to disruptions. As scientifically proved, a concerted effort should be made to develop effective strategies aimed at motivating children to lead an all-round healthy lifestyle (diet, avoidance of harmful substances, mental health, etc.), with particular emphasis on reducing the periods of time spent sitting down or watching TV and gradually resuming physical activity [35].
References
Bassareo PP, Melis MR, Marras S, Calcaterra G (2020) Learning from the past in the COVID-19 era: rediscovery of quarantine, previous pandemics, origin of hospitals and national healthcare systems, and ethics in medicine. Postgrad Med J 96:633–638
Medrano M, Cadenas-Sanchez C, Oses M, Arenaza L et al (2021) Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: a longitudinal analysis from the MUGI project. Pediatr Obes 16:e12731
Crisafulli A, Pagliaro P (2020) Physical activity/inactivity and COVID-19. Eur J Prev Cardiol 19:2047487320927597 (online ahead of print)
Children and COVID-19: (2021) State-level data report. https://www.aap.org/en/pages/2019-novel-coronaviruscovid-19-infections/children-and-covid-19-state-level-data-report/. Accessed 7 July 2021
Centers for disease control and prevention website. (2021). Demographic characteristics of people receiving COVID-19 Vaccinations in the United States. https://covid.cdc.gov/covid-data-tracker/#vaccinationdemographic. Accessed 23 May 2021
Pinna G, Sanfilippo L, Bassareo PP, Fanos V et al (2021) COVID-19 and comorbidities: is inflammation the underlying condition in children? Narrat Rev Curr Pediatr Rev 17:38–44
Bassareo pp. (2021) Pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the United Kingdom and Ireland: what is new? Lancet Reg Health Eur 3:100090
Kompaniyets L, Agathis NT, Nelson JM, Preston LE et al (2021) Underlying medical conditions associated with severe COVID-19 illness among children. JAMA Netw Open 4:e2111182
Calcaterra G, Mehta JL, Fanos V, Bassareo PP (2021) Insights on kawasaki disease and multisystem inflammatory syndrome: relationship with COVID-19 infection. Minerva Pediatr (Torino) 73:203–8
Feldstein LR, Tenforde MW, Friedman KG, Newhams M et al (2021) Overcoming COVID-19 investigators. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA 325:1074–87
Bourgeois FT, Gutiérrez-Sacristán A, Keller MS, Liu M et al (2021) Consortium for clinical characterization of COVID-19 by EHR (4CE). International analysis of electronic health records of children and youth hospitalized with COVID-19 infection in 6 countries. JAMA Netw Open 4:e2112596
Bean CN, Fortier M, Post C, Chima K (2014) Understanding how organized youth sport maybe harming individual players within the family unit: a literature review. Int J Environ Res Public Health 11:10226–10268
Rahman AM, Chandrasekaran B (2021) Estimating the impact of the pandemic on children’s physical health: a scoping review. J Sch Health 91:936–947
Thompson LA, Kelly MN (2021) Return to play after COVID-19 infection in children. JAMA Pediatr 175:875
Moore SA, Faulkner G, Rhodes RE, Vanderloo LM et al (2021) Few canadian children and youth were meeting the 24-hour movement behaviour guidelines 6-months into the COVID-19 pandemic: follow-up from a national study. Appl Physiol Nutr Metab 46:1225–1240
Calcaterra G, Mehta JL, de Gregorio C, Butera G et al (2021) COVID 19 vaccine for adolescents. Concern about myocarditis and pericarditis. Pediatr Rep 13:530–3
McBride DL (2021) New guidelines for children returning to sports after covid-19. J Pediatr Nurs 59:196–197
Tulchin-Francis K, Stevens W Jr, Gu X, Zhang T et al (2021) The impact of the coronavirus disease 2019 pandemic on physical activity in U.S. children. J Sport Health Sci 10:323–32
Haraf RH, Faghy MA, Carlin B, Josephson RA (2021) The physiological impact of masking is insignificant and should not preclude routine use during daily activities, exercise, and rehabilitation. J Cardiopulm Rehabil Prev 41:1–5
Kuitunen I, Uimonen MM, Ponkilainen VT (2021) Team-to-team transmission of COVID-19 in ice hockey games - a case series of players in finnish ice hockey leagues. Infect Dis (Lond) 53:201–205
Roberts WO, Satin DJ (2020) Resuming high school and youth sports: what would your institutional review board say? Curr Sports Med Rep 19:345–346
Dove J, Gage A, Kriz P, Tabaddor RR et al (2013) COVID-19 and review of current recommendations for return to athletic play. R I Med J 2020(103):15–20
Wang C, Vander Voort W, Haus BM, Carter CW (2021) COVID-19 and youth sports: what are the risks of getting back on the field too quickly? Pediatr Ann 50:e465–e469
Rajpal S, Tong MS, Borchers J, Zareba KM et al (2021) Cardiovascular magnetic resonance findings in competitive athletes recovering from COVID-19 infection. JAMA Cardiol 6:116–118
Bhatia RT, Marwaha S, Malhotra A, Iqbal Z et al (2020) Exercise in the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) era: a question and answer session with the experts endorsed by the section of sports cardiology and exercise of the european association of preventive cardiology (EAPC). Eur J Prev Cardiol 27:1242–1251
Baggish A, Drezner JA, Kim J, Martinez M et al (2020) Resurgence of sport in the wake of COVID-19: cardiac considerations in competitive athletes. Br J Sports Med 54:1130–1131
Elliott N, Martin R, Heron N, Elliott J et al (2020) Infographic. Graduated return to play guidance following COVID-19 infection. Br J Sports Med 54:1174–5
Harmon KG, Clugston JR, Dec K, Hainline B, Herring S, Kane SF, Kontos AP, Leddy JJ, McCrea M, Poddar SK, Putukian M, Wilson JC, Roberts WO (2019) American medical society for sports medicine position statement on concussion in sport. Br J Sports Med 53:213–215
Hamilton MT, Healy GN, Dunstan DW, Zderic TW, Owen N (2008) Too little exercise and too much sitting: inactivity physiology and the need for new recommendations on sedentary behavior. Curr Cardiovasc Risk Rep 2:292–298
Harmon KG, Drezner JA, Gammons M, Guskiewicz KM, Halstead M, Herring SA, Kutcher JS, Pana A, Putukian M, Roberts WO (2013) American Medical society for sports medicine position statement: concussion in sport. Br J Sports Med 47:15–26
Kraemer W, Denegar C, Flanagan S (2009) Recovery from injury in sport: considerations in the transition from medical care to performance care. Sports Health 1:392–395
Kim JH, Levine BD, Phelan D, Emery MS et al (2021) Coronavirus disease 2019 and the athletic heart: emerging perspectives on pathology, risks, and return to play. JAMA Cardiol 6:219–227
Hull JH, Loosemore M, Schwellnus M (2020) Respiratory health in athletes: facing the COVID-19 challenge. Lancet Respir Med 8:557–558
Perico L, Benigni A, Remuzzi G (2020) Should COVID-19 concern nephrologists? why and to what extent? the emerging impasse of angiotensin blockade. Nephron 144:213–221
Tandon PS, Zhou C, Johnson AM, Gonzalez ES et al (2021) Association of children’s physical activity and screen time with mental health during the COVID-19 pandemic. JAMA Netw Open 4:e2127892
Funding
None.
Author information
Authors and Affiliations
Contributions
GC and PPB: have given substantial contributions to the conception or the design of the manuscript, VF, LCa, LCu, and AC: to acquisition, analysis and interpretation of the data. All authors have participated to drafting the manuscript, author PPB revised it critically. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Calcaterra, G., Fanos, V., Cataldi, L. et al. Need for resuming sports and physical activity for children and adolescents following COVID-19 infection. Sport Sci Health 18, 1179–1185 (2022). https://doi.org/10.1007/s11332-022-00930-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-022-00930-3