
Abstract
Several risk stratification tools are available to predict short-term mortality in patients with acute pulmonary embolism (PE). The presence of right ventricular (RV) dysfunction is an independent predictor of mortality and may be a more efficient way to stratify risk for patients assessed by a Pulmonary Embolism Response Team (PERT). We evaluated 571 patients presenting with acute PE, then stratified them by the pulmonary embolism severity index (PESI), by the BOVA score, or categorically as low risk (no RV dysfunction by imaging), intermediate risk/submassive (RV dysfunction by imaging), or high risk/massive PE (RV dysfunction with sustained hypotension). Using imaging data to firstly define the presence of RV strain, and plasma cardiac biomarkers as additional evidence for myocardial dysfunction, we evaluated whether PESI, BOVA, or RV strain by imaging were more appropriate for determining patient risk by a PERT where rapid decision making is important. Cardiac biomarkers poorly distinguished between PESI classes and BOVA stages in patients with acute PE. Cardiac TnT and NT-proBNP easily distinguished low risk from submassive PE with an area under the curve (AUC) of 0.84 (95% CI 0.73–0.95, p < 0.0001), and 0.88 (95% CI 0.79–0.97, p < 0.0001), respectively. Cardiac TnT and NT-proBNP easily distinguished low risk from massive PE with an area under the curve (AUC) of 0.89 (95% CI 0.78–1.00, p < 0.0001), and 0.89 (95% CI 0.82–0.95, p < 0.0001), respectively. In patients with RV dysfunction, the predicted short-term mortality by PESI score or BOVA stage was lower than the observed mortality by a two-fold order of magnitude. The presence of RV dysfunction alone in the context of acute PE is sufficient for the purposes of risk stratification. More complicated risk stratification tools which require the consideration of multiple clinical variables may under-estimate short-term mortality risk.




Similar content being viewed by others

References
Wood KE (2002) Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest 121(3):877–905
Friedman T et al (2018) Patient assessment: clinical presentation, imaging diagnosis, risk stratification, and the role of pulmonary embolism response team. Semin Intervent Radiol 35(2):116–121
Jimenez D et al (2007) Prognostic models for selecting patients with acute pulmonary embolism for initial outpatient therapy. Chest 132(1):24–30
Aujesky D et al (2005) Derivation and validation of a prognostic model for pulmonary embolism. Am J Respir Crit Care Med 172(8):1041–1046
Aujesky D et al (2006) Validation of a model to predict adverse outcomes in patients with pulmonary embolism. Eur Heart J 27(4):476–481
Aujesky D et al (2007) Validation of a clinical prognostic model to identify low-risk patients with pulmonary embolism. J Intern Med 261(6):597–604
Masotti L et al (2009) Prognostic stratification of acute pulmonary embolism: focus on clinical aspects, imaging, and biomarkers. Vasc Health Risk Manag 5(4):567–575
Bova C et al (2014) Identification of intermediate-risk patients with acute symptomatic pulmonary embolism. Eur Respir J 44(3):694–703
Bikdeli B et al (2018) Early use of echocardiography in patients with acute pulmonary embolism: findings from the RIETE registry. J Am Heart Assoc 7(17):e009042
Kucher N et al (2005) Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure of 90 mm Hg or higher. Arch Intern Med 165(15):1777–1781
Cho JH et al (2014) Right ventricular dysfunction as an echocardiographic prognostic factor in hemodynamically stable patients with acute pulmonary embolism: a meta-analysis. BMC Cardiovasc Disord 14:64
Darwish OS et al (2018) Cardiac troponins in low-risk pulmonary embolism patients: a systematic review and meta-analysis. J Hosp Med 13(10):706–712
Kearon C et al (2016) Antithrombotic therapy for VTE disease: chest guideline and expert panel report. Chest 149(2):315–352
Konstantinides SV et al (2014) ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J 35(43):3033–3069
Rosovsky R et al (2019) Changes in treatment and outcomes after creation of a pulmonary embolism response team (PERT), a 10-year analysis. J Thromb Thrombolysis 47(1):31–40
Xenos ES et al (2019) The implementation of a pulmonary embolism response team in the management of intermediate- or high-risk pulmonary embolism. J Vasc Surg Venous Lymphat Disord 7(4):493–500
Mahar JH et al (2018) A pulmonary embolism response team (PERT) approach: initial experience from the Cleveland Clinic. J Thromb Thrombolysis 46(2):186–192
Elbadawi A et al (2018) The impact of a multi-specialty team for high risk pulmonary embolism on resident and fellow education. Vasc Med 23(4):372–376
Secemsky E et al (2018) Contemporary management and outcomes of patients with massive and submassive pulmonary embolism. Am J Med 131(12):1506–1514
Jaff MR et al (2011) Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation 123(16):1788–1830
Sanchez O et al (2008) Prognostic value of right ventricular dysfunction in patients with haemodynamically stable pulmonary embolism: a systematic review. Eur Heart J 29(12):1569–1577
Chan CM, Woods CJ, Shorr AF (2012) Comparing the pulmonary embolism severity index and the prognosis in pulmonary embolism scores as risk stratification tools. J Hosp Med 7(1):22–27
Vanderheyden M et al (2010) B-type natriuretic peptide as a marker of heart failure: new insights from biochemistry and clinical implications. Biomark Med 4(2):315–320
Mair J (2008) Biochemistry of B-type natriuretic peptide–where are we now? Clin Chem Lab Med 46(11):1507–1514
Goetze JP (2004) Biochemistry of pro-B-type natriuretic peptide-derived peptides: the endocrine heart revisited. Clin Chem 50(9):1503–1510
Semenov AG, Seferian KR (2011) Biochemistry of the human B-type natriuretic peptide precursor and molecular aspects of its processing. Clin Chim Acta 412(11–12):850–860
Panteghini M, Clerico A (2004) Understanding the clinical biochemistry of N-terminal pro-B-type natriuretic peptide: the prerequisite for its optimal clinical use. Clin Lab 50(5–6):325–331
Arbustini E et al (1990) Expression of natriuretic peptide in ventricular myocardium of failing human hearts and its correlation with the severity of clinical and hemodynamic impairment. Am J Cardiol 66(12):973–980
Klok FA, Mos IC, Huisman MV (2008) Brain-type natriuretic peptide levels in the prediction of adverse outcome in patients with pulmonary embolism: a systematic review and meta-analysis. Am J Respir Crit Care Med 178(4):425–430
Jimenez D et al (2009) Troponin-based risk stratification of patients with acute nonmassive pulmonary embolism: systematic review and metaanalysis. Chest 136(4):974–982
Becattini C, Vedovati MC, Agnelli G (2007) Prognostic value of troponins in acute pulmonary embolism: a meta-analysis. Circulation 116(4):427–433
Ferrando-Castagnetto F et al (2017) Atrial arrhythmias and scintigraphic “D-shape” sign in pulmonary artery hypertension. World J Nucl Med 16(1):75–77
Movahed MR (2014) D-shaped left ventricle seen on gated single-photon emission computed tomography is suggestive of right ventricular overload: the so-called Movahed’s sign. Am J Med 127(12):e37
Lodato JA, Ward RP, Lang RM (2008) Echocardiographic predictors of pulmonary embolism in patients referred for helical CT. Echocardiography 25(6):584–590
Funding
The following financial funding agencies provided financial support: National Institutes of Health (NIH) grants NIH 3K08HL128856, and HL12020 to Dr. Cameron
Author information
Authors and Affiliations
Contributions
Study concept, design, and development (YC, CW, AE, JD, AP, DP, DT, IG, BB, and SC), data acquisition (YC, AE, CW, DP, and SC), statistical analysis and interpretation (YC and SC), drafting of the manuscript (YC and SC).
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
11239_2019_1922_MOESM4_ESM.tiff
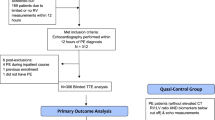
Supplementary Figure 4 Inclusion criteria for patients screened by ICD-9 Code and stratification according to category, PESI Class, or Bova Stage (TIFF 1522 kb)
Rights and permissions
About this article

Cite this article
Chen, Y.L., Wright, C., Pietropaoli, A.P. et al. Right ventricular dysfunction is superior and sufficient for risk stratification by a pulmonary embolism response team. J Thromb Thrombolysis 49, 34–41 (2020). https://doi.org/10.1007/s11239-019-01922-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11239-019-01922-w