
Abstract
Introduction
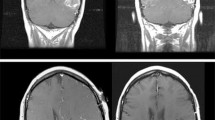
Pseudoprogression (PsP) is a diagnostic dilemma in glioblastoma (GBM) after chemoradiotherapy (CRT). Magnetic resonance imaging (MRI) features may fail to distinguish PsP from early true progression (eTP), however clinical findings may aid in their distinction.
Methods
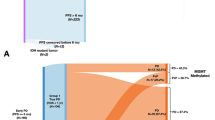
Sixty-seven patients received CRT for GBM between 2003 and 2016, and had pre- and post-treatment imaging suitable for retrospective evaluation using RANO criteria. Patients with signs of progression within the first 12-weeks post-radiation (P-12) were selected. Lesions that improved or stabilized were defined as PsP, and lesions that progressed were defined as eTP.
Results
The median follow up for all patients was 17.6 months. Signs of progression developed in 35/67 (52.2%) patients within P-12. Of these, 20/35 (57.1%) were subsequently defined as eTP and 15/35 (42.9%) as PsP. MRI demonstrated increased contrast enhancement in 84.2% of eTP and 100% of PsP, and elevated CBV in 73.7% for eTP and 93.3% for PsP. A decrease in FLAIR was not seen in eTP patients, but was seen in 26.7% PsP patients. Patients with eTP were significantly more likely to require increased steroid doses or suffer clinical decline than PsP patients (OR 4.89, 95% CI 1.003–19.27; p = 0.046). KPS declined in 25% with eTP and none of the PsP patients.
Conclusions
MRI imaging did not differentiate eTP from PsP, however, KPS decline or need for increased steroids was significantly more common in eTP versus PsP. Investigation and standardization of clinical assessments in response criteria may help address the diagnostic dilemma of pseudoprogression after frontline treatment for GBM.

Similar content being viewed by others

References
Chamberlain MC et al (2007) Early necrosis following concurrent Temodar and radiotherapy in patients with glioblastoma. J Neurooncol 82(1):81–83
Fink J, Born D, Chamberlain MC (2011) Pseudoprogression: relevance with respect to treatment of high-grade gliomas. Curr Treat Options Oncol 12(3):240–252
Brandes AA et al (2008) MGMT promoter methylation status can predict the incidence and outcome of pseudoprogression after concomitant radiochemotherapy in newly diagnosed glioblastoma patients. J Clin Oncol 26(13):2192–2197
Linhares P et al (2013) Early pseudoprogression following chemoradiotherapy in glioblastoma patients: the value of RANO evaluation. J Oncol 2013:690585
Young RJ et al (2013) MRI perfusion in determining pseudoprogression in patients with glioblastoma. Clin Imaging 37(1):41–49
Li H et al (2016) IDH mutation and MGMT promoter methylation are associated with the pseudoprogression and improved prognosis of glioblastoma multiforme patients who have undergone concurrent and adjuvant temozolomide-based chemoradiotherapy. Clin Neurol Neurosurg 151:31–36
Pouleau HB et al (2012) High levels of cellular proliferation predict pseudoprogression in glioblastoma patients. Int J Oncol 40(4):923–928
Wen PY et al (2010) Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol 28(11):1963–1972
Gerstner ER et al (2009) Effect of adding temozolomide to radiation therapy on the incidence of pseudo-progression. J Neurooncol 94(1):97–101
Kong DS et al (2011) Diagnostic dilemma of pseudoprogression in the treatment of newly diagnosed glioblastomas: the role of assessing relative cerebral blood flow volume and oxygen-6-methylguanine-DNA methyltransferase promoter methylation status. AJNR Am J Neuroradiol 32(2):382–387
Balana C et al (2017) Pseudoprogression as an adverse event of glioblastoma therapy. Cancer Med 6(12):2858–2866
Radbruch A et al (2015) Pseudoprogression in patients with glioblastoma: clinical relevance despite low incidence. Neuro Oncol 17(1):151–159
Gunjur A et al (2011) Early post-treatment pseudo-progression amongst glioblastoma multiforme patients treated with radiotherapy and temozolomide: a retrospective analysis. J Med Imaging Radiat Oncol 55(6):603–610
Ellingson BM, Wen PY, Cloughesy TF (2017) Modified Criteria for radiographic response assessment in glioblastoma clinical trials. Neurotherapeutics 14(2):307–320
Nowosielski M, Wen PY (2018) Imaging criteria in neuro-oncology. Semin Neurol 38(1):24–31
Di Stefano AL et al (2014) Facing contrast-enhancing gliomas: perfusion MRI in grade III and grade IV gliomas according to tumor area. Biomed Res Int 2014: 154350
Law M et al (2008) Gliomas: predicting time to progression or survival with cerebral blood volume measurements at dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging. Radiology 247(2):490–498
Thomas AA et al (2015) Dynamic contrast enhanced T1 MRI perfusion differentiates pseudoprogression from recurrent glioblastoma. J Neurooncol 125(1):183–190
Gahramanov S et al (2013) Pseudoprogression of glioblastoma after chemo- and radiation therapy: diagnosis by using dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging with ferumoxytol versus gadoteridol and correlation with survival. Radiology 266(3):842–852
Gahramanov S et al (2014) Diagnosis of pseudoprogression using MRI perfusion in patients with glioblastoma multiforme may predict improved survival. CNS Oncol 3(6):389–400
Nasseri M et al (2014) Evaluation of pseudoprogression in patients with glioblastoma multiforme using dynamic magnetic resonance imaging with ferumoxytol calls RANO criteria into question. Neuro Oncol 16(8):1146–1154
Nayak L et al (2014) The Neurologic Assessment in Neuro-Oncology (NANO) Scale: a tool to assess neurologic function for integration in the Radiologic Assessment in Neuro-Oncology (RANO) Criteria. Neurology 82(10 Supplement):S22.005
Lamborn KR, Chang SM, Prados MD (2004) Prognostic factors for survival of patients with glioblastoma: recursive partitioning analysis. Neuro Oncol 6(3):227–235
Ho J et al (2013) Chemoirradiation for glioblastoma multiforme: The National Cancer Institute experience. PLoS ONE 8(8):e70745
Yoon RG et al (2017) Different diagnostic values of imaging parameters to predict pseudoprogression in glioblastoma subgroups stratified by MGMT promoter methylation. Eur Radiol 27(1):255–266
Motegi H et al (2013) IDH1 mutation as a potential novel biomarker for distinguishing pseudoprogression from true progression in patients with glioblastoma treated with temozolomide and radiotherapy. Brain Tumor Pathol 30(2):67–72
Gzell C et al (2016) Proliferation index predicts survival after second craniotomy within 6 months of adjuvant radiotherapy for high-grade glioma. Clin Oncol (R Coll Radiol) 28(3):215–222
Kang HC et al (2011) Pseudoprogression in patients with malignant gliomas treated with concurrent temozolomide and radiotherapy: potential role of p53. J Neurooncol 102(1):157–162
Romano A et al (2013) Apparent diffusion coefficient obtained by magnetic resonance imaging as a prognostic marker in glioblastomas: correlation with MGMT promoter methylation status. Eur Radiol 23(2):513–520
Sanghera P et al (2010) Pseudoprogression following chemoradiotherapy for glioblastoma multiforme. Can J Neurol Sci 37(1):36–42
Roldan GB et al (2009) Population-based study of pseudoprogression after chemoradiotherapy in GBM. Can J Neurol Sci 36(5):617–622
Young RJ et al (2011) Potential utility of conventional MRI signs in diagnosing pseudoprogression in glioblastoma. Neurology 76(22):1918–1924
Funding
This research was funded by the intramural research program at the National Cancer Institute (Grant Number ZID BC 010990).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Rowe, L.S., Butman, J.A., Mackey, M. et al. Differentiating pseudoprogression from true progression: analysis of radiographic, biologic, and clinical clues in GBM. J Neurooncol 139, 145–152 (2018). https://doi.org/10.1007/s11060-018-2855-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-018-2855-z