
Abstract
Background
As the indications for endoscopic submucosal dissection (ESD) for early gastric cancer have been revised, diagnostic ESD has increased. However, despite the technical difficulty of ESD for large lesions, the degree to which curative resection can be achieved has not been clarified. This study investigated the feasibility and safety of ESD for gastric lesions larger than 5 cm.
Methods
This retrospective multicenter study included 3474 gastric lesions treated by ESD from April 2012 to December 2021. We compared clinicopathological characteristics and treatment outcomes between lesions ≥ 5 cm and lesions < 5 cm.
Results
There were 128 lesions in the ≥ 5 cm group and 3282 lesions in the < 5 cm group. In the ≥ 5 cm group, upper location and fibrosis during ESD were more common, with a lower rate of 0–IIc type. Both en bloc resection rate and R0 resection rate were comparable, but there was a difference in curative resection rate (65.6% in the ≥ 5 cm group and 91.5% in the < 5 cm group). The frequency of adverse events (post-ESD bleeding, perforation, or stenosis) was almost similar, but delayed perforation was significantly more common (1.6% in the ≥ 5 cm group vs. 0.1% in the < 5 cm group).
Conclusions
About two-thirds of curative resections were obtained with ESD for early gastric lesions larger than 5 cm, but delayed complications should be noted (Number: UMIN000047725).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Endoscopic submucosal dissection (ESD) has become popular as local treatment for early gastric lesions without lymph node metastasis [1, 2]. Also, ESD is less invasive than surgery and preserves organ function. Initially, the absolute indications for ESD were lesions ≤ 2 cm, ulceration (UL)-negative, and differentiated carcinoma with cT1a [3]. Later, in 2018, based on the results of the Japan Clinical Oncology Group [JCOG] 0607 (Phase II trial for expanded indications for endoscopic mucosal resection in early gastric cancer), the guidelines for gastric cancer treatment were revised [4]. After this revision, T1a intestinal-type gastric adenocarcinoma with UL-negative tumor > 2 cm, UL-positive tumor ≤ 3 cm, or T1a undifferentiated-type adenocarcinoma with UL-negative tumor ≤ 2 cm was added as an absolute indication for ESD [5]. Therefore, there has been an increase in ESD cases for large gastric lesions in recent years. Yano et al. demonstrated in the post hoc analysis of JCOG0607 that a UL-negative tumor > 5 cm showed the largest odds ratio as a significant risk factor of difficult ESD taking ≥ 120 min or complicated with perforation [6]. In practice, however, it is often difficult to accurately diagnose the presence of pathological UL (p-UL) preoperatively [7]. In some cases, unexpected fibrosis may be encountered intraoperatively, especially in large lesions, and after a lengthy treatment process, the pathological evaluation may result in a noncurative resection, requiring additional surgery. Thus, it is clinically valuable to know the extent of curability of large-sized lesions by ESD. The degree to which ESD for large-size lesions is curative is of great clinical value but has not yet been reported. This study investigated the feasibility and safety of ESD for gastric lesions larger than 5 cm.
Method
Patients and study design
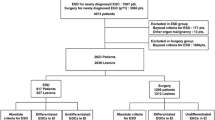
This retrospective study evaluated 3474 gastric lesions treated by ESD from April 2012 to December 2021. This study was conducted at the Omori Red Cross Hospital and one affiliated hospital. Inclusion criteria were patients aged 20 years or older with clinically diagnosed gastric cancer or gastric adenoma. We excluded 11 neuroendocrine tumors, 26 submucosal tumors, and 27 unidentified lesions and enrolled the remaining 3410 gastric lesions in 2722 patients. To evaluate the feasibility and safety of ESD for large lesions ≥ 5 cm, we compared patient and tumor characteristics and ESD outcomes between 128 lesions ≥ 5 cm and 3282 lesions < 5 cm. The criteria used to diagnose early-stage gastric cancer for ESD were consistent with the Japanese gastric cancer treatment guidelines [3, 5]. Absolute and extended indication lesions were the main focus; however, this study also included cases with diagnostic ESD as relative indication lesions, depending on age and comorbidities according to the ESD/EMR guideline [5]. Diagnostic endoscopy with image-enhanced endoscopy was used to identify ESD indications for all cases. Antithrombotic and anticoagulant agents were stopped before each procedure in accordance with current guidelines [8, 9]. The tumor size was measured with reference to the length of the fully opened biopsy forceps, including Radial Jaw™ 4 (the length was approximately 6 mm) (Boston Scientific, Tokyo, Japan) or EndoJaw (the length was approximately 6.5 mm) (Olympus, Tokyo, Japan), the diameter of the endoscope shaft (approximately 1 cm), or by measuring forceps. The final tumor size was determined after the histopathological evaluation of the resected specimen.
Histopathological assessment
The fresh specimen was stretched and fixed on a rubber plate with the mucosal surface facing upward, using mounting pins, to obtain the tumor size consistent with endoscopic observation. All specimens were diagnosed by pathologists familiar with gastrointestinal pathology at the respective institutions in accordance with the Japanese classification of gastric carcinoma [10]. Histopathologic examination, by hematoxylin and eosin staining of the specimens resected by endoscopic treatment, was performed in parallel 2 to 3 mm thick.
ESD procedure
ESD was performed using a single-channel or a double-channel endoscope (GIF-Q260J, GIF-H290T, GIF-2TQ260M; Olympus Medical Systems, Tokyo, Japan) with a transparent cap with carbon dioxide insufflation. All ESD procedures were performed by experienced endoscopists (with experience of ≥ 200 ESD procedures) or by other endoscopists under the supervision of an experienced endoscopist. ESD was performed with patients under conscious sedation with flunitrazepam and buprenorphine. As a standard strategy of ESD, the natural traction by gravity force was mainly used. The tunnel method or the traction-assisted method was determined according to the circumstances for all cases to optimize the endoscopic view or achieve good traction (Figs. 1, 2). For mucosal incision and submucosal dissection, the physician decided the device intended for use, including IT-Knife2 (KD-611L; Olympus, Tokyo, Japan) or Dual knife (KD-650L; Olympus, Tokyo, Japan) and other needle-type knives. After resecting the lesion, all visible vessels on the ulcer floor were coagulated using hemostatic forceps. Patients who did not develop complications started a soft diet on day 1 after ESD and were discharged 5 days after the procedure.

ESD procedure for 50 mm gastric lesion in the lesser curvature of the middle body. a A slightly elevated lesion is seen in the lesser curvature of the middle body. b The tumor diameter was measured with reference to the long axis of the endoscope. c Mild fibrosis was observed during ESD. d The resected specimen; The pathological findings revealed well-differentiated tubular adenocarcinoma, 54 mm, 0–IIa, pT1a, Ly0, V0, UL0, vertical margin negative, horizontal margin negative

ESD procedure for 55 mm gastric lesion in the greater curvature of the lower body. a A flat elevated lesion is seen in the greater curvature of the lower body. b The tumor diameter was measured with measuring forceps. c Treatment strategy with gravity force enabled en bloc resection. d The resected specimen; The pathological findings revealed well-differentiated tubular adenocarcinoma, 58 mm, 0–IIa, pT1a, Ly0, V0, UL0, vertical margin negative, horizontal margin negative
Data analysis and definitions of outcomes after ESD
The primary outcome measure was the rate of curative resection, defined as eCuraA or eCuraB with R0 resection. R0 resection was also defined as en bloc resection with negative margins. Endoscopic curability (eCura) A or B was classified when the tumor was negative for vertical margins, had no lymphovascular invasion, and met one of the following conditions: (1) dominantly differentiated-type tumor, pT1a, and UL0; (2) dominantly differentiated-type tumor, pT1a, UL1, and tumor size ≤ 3 cm; (3) dominantly differentiated-type tumor, pT1b1 (tumor invaded submucosa less than 500 µm from the muscularis mucosa), and tumor size ≤ 3 cm; (4) dominantly undifferentiated-type tumor, pT1a, and tumor size ≤ 2 cm. eCuraC-1 was classified when the tumor was dominantly differentiated-type and corresponded to eCura A or B, but either was not resected en bloc or was positive for horizontal margins. eCura C-2 was classified when the resection did not correspond to eCuraA, B, and C-1.
Post-ESD bleeding was defined as the condition requiring endoscopic hemostasis. Perforation was defined as confirmation of a perforated site on endoscopy or free air on the postoperative radiograph or computed tomography (CT) scan. Delayed perforation was defined in cases in which perforation had not been detected during and just after completion of ESD, but subsequent endoscopy showed perforation, and CT showed free air after ESD. Post-ESD stenosis was defined as narrowing of the stomach lumen to the extent that a standard 10-mm diameter endoscope could not smoothly pass through without endoscopic dilation. A subanalysis of pretreatment factors for non-curative resection in ESD for differentiated predominant cancer greater than 3 cm, which was usually the standard for size, was performed.
Statistical analysis
We used the chi-square test, Fisher’s exact test, and Student’s t test. Factors identified significant by univariate analysis (p < 0.10) were entered in the multivariate logistic regression analysis model. The odds ratio (OR) and 95% confidence interval (95% CI) was calculated for each variable. All analyses were performed using SPSS Statistics for Windows, version 23 (IBM Corp., Armonk, NY, USA). p values ≤ 0.05 were considered statistically significant.
Ethics
The study was conducted according to the principles of the Declaration of Helsinki. All patients provided informed consent before undergoing treatment. The institutional review board of our hospital approved this study (21–43), and the clinical trial was registered in the UMIN clinical trial registration database (UMIN000047725).
Results
Table 1 shows the baseline characteristics of the patients who underwent ESDs for gastric lesions ≥ 5 vs. < 5 cm. In the lesion ≥ 5 cm group, the upper location was more common. For the macroscopic type, the rate of 0–IIc was relatively lower (1722 lesions (52.5%) in the < 5 cm group vs. 42 lesions (32.8%) in the ≥ 5 cm group). Table 2 summarizes perioperative or postoperative results. The median procedure time was 30 min in the < 5 cm group and 110 min in the ≥ 5 cm group. Although the overall percentage of assisted ESD was 46 cases (1.3%), both the ring thread counter traction and the submucosal tunnel method were used more often in the > 5 cm group (0.8% and 0.2% in the < 5 cm group, respectively, vs. 6.3% and 7.0% in the ≥ 5 cm group, respectively). Three of the 46 cases had ESD using a combination of the two methods. There was significantly more frequent fibrosis during ESD observed in the > 5 cm group. Regarding major adverse events, the post-ESD bleeding rate and the perforation rate were comparable between the two groups. In the < 5 cm group, one remnant stomach lesion of ESD performed in 2014 required emergency surgery due to intraoperative perforation, but all others received conservative treatment. Meanwhile, a delayed perforation rate was significantly higher in the ≥ 5 cm group (4 lesions (0.1%) in the < 5 cm group vs. 2 lesions (1.6%) in the ≥ 5 cm group, p = 0.019). Three of the six cases with delayed perforation were sutured by various methods (one over-the-scope clip and two endoclips); one case required percutaneous drainage, and the remaining three underwent emergency surgery.
Table 3 summarizes the outcome of ESD comparisons between the two groups. R0 resection rate and curative rate in the ≥ 5 cm group were 98.5% and 65.6%, respectively. However, pT1b cancer, UL1, and vascular involvement positive was significantly more frequent in the ≥ 5 cm group (9.5%, 0.8%, and 2.0%, respectively, in the < 5 cm group vs. 25.8%, 4.7%, and 5.5%, respectively, in the ≥ 5 cm group, p < 0.05). Lateral margin negative rates were comparable, but vertical margin positive rates were higher in the ≥ 5 cm group (1.1% in the < 5 cm group vs. 7.8% in the ≥ 5 cm group, p < 0.01).
The most common reasons for noncurative resection in the < 5 cm group were differentiated pT1b2 cancer (47.1%), lymphovascular invasion without other noncurative factors (12.5%), and undifferentiated > 2 cm pT1a cancer with UL negative (12.1%), whereas differentiated pT1b2 cancer (36.4%), differentiated > 3 cm pT1b1 cancer (36.4%), and undifferentiated > 2 cm pT1a cancer with UL0 (11.4%) were the most common reasons for noncurative resection in the ≥ 5 cm group (Table 4). Additional surgery and additional endoscopic treatment for cases with noncurative resection were more frequently observed in the ≥ 5 cm group (6.3% and 0.09%, respectively, in the < 5 cm group vs. 27.3% and 0.8%, respectively, p < 0.01).
In the subanalysis, univariate and multivariate analysis of pretreatment factors that resulted in noncurative resection among 505 lesions of differentiated predominant cancer greater than 3 cm was performed (Table 5). The following factors of noncurative resection were found to be higher: endoscopic UL (e-UL) (odds ratio [OR], 2.259; 95% CI [confidence interval], 1.241–4.113; p = 0.008), depressed type (OR, 2.292; 95% CI 1.503–3.496; p < 0.001), upper location (OR, 2.137; 95% CI 1.24–3.68; p = 0.006), size ≥ 5 cm (OR, 1.831; 95% CI 1.154–2.906; p = 0.01), and middle location (OR, 1.811; 95% CI 1.003–3.270; p = 0.049) in that order.
Discussion
This is the first report to identify the outcomes of ESD for large gastric lesions ≥ 5 cm. The results of this study showed that 100% of tumors were resected en bloc, 91.4% of tumors were resected en bloc with negative margins, and 65.6% of tumors were resected curatively. Although the frequency of intraoperative complications (post-ESD bleeding or perforation) for ESD of large lesions was comparable to that of lesions smaller than 5 cm, delayed perforation was significantly more common. Therefore, more attention is required for postoperative management.
ESD for early-stage gastric cancer has been widely reported for high en bloc resection [11]. This study also showed that ESD has a high en bloc resection rate, even for large lesions ≥ 5 cm. The indicated size for gastric ESD has changed based on the results of large prospective trials [4, 12], and diagnostic ESD is now performed even for large lesions unless there is an obvious e-UL or submucosal invasion. Although large lesions, especially greater than 5 cm, have been reported to be a difficult factor of gastric ESD [6], there have been no reports on the extent of curative resection, even with en bloc resection of large lesions after long and arduous efforts. Our study achieved curative resection in 65% or about two-thirds of cases of ESD with 5 cm or larger lesions, which may help explain the results to patients before treatment for such large lesions.
The reasons for noncurative resection of lesions ≥ 5 cm are also significant concerns, and 5 cm or larger lesions do not meet the criteria for curative resection, even if one of the conditions is unmet: differentiated, UL0, or intramucosal carcinoma. Therefore, it is also important to know how well these three conditions can be predicted preoperatively. The tumor diameter was measured preoperatively, as indicated in the ESD/EMR guidelines [3]. Accurate evaluation of larger sizes preoperatively can be challenging. However, lesions larger than 5 cm were almost half IIa lesions (47.7%) and relatively few IIc lesions compared to lesions smaller than 5 cm, making it easy to measure the approximate size of the lesions with conventional endoscopic observation. First, it is possible to estimate to a certain extent whether the lesion is predominantly differentiated or undifferentiated based on its color and magnified endoscopic findings [13]. There was no difference in the proportion of undifferentiated predominant cancers between the two groups. Second, the difficulty of p-UL preoperative diagnosis is mentioned above. Yabuuchi et al. investigated the discrepancy between e-UL and p-UL and reported that 5.5% of e-UL0 lesions were identified as p-UL1, while 38.7% of e-UL1 lesions were p-UL0 [14]. Moreover, they concluded that especially for lesions in the lower third of the stomach were prone to overestimation. Third, it is challenging to predict whether the lesion depth is T1a or T1b1. In particular, in depressed carcinomas, T1b1 cancer should be suspected when nodular protuberance or a deeper depression is present on the surface of the lesion; however, the thickening of the submucosa in response to cancer invasion is also mild, and clear differentiation from T1a cancer is challenging [15]. As indicated in the subanalysis, depressed tumors may be difficult to predict preoperative depth diagnosis.
The reasons for noncurative resection are presented in Table 4, which shows that the percentage of pT1b1, D, ≥ 3 cm increased in the ≥ 5 cm group. Among lesions ≥ 5 cm, those with a lesion size of 25 cm2 or larger are considered superficial spreading types of early gastric cancer (SSEGC) [16] with the following characteristics: undifferentiated type, depressed type, middle location and lesser curvature, and association with ulcers. A mechanism of multicentric occurrence is also under consideration, and reports show that 23.5% of SSEGC patients develop multiple cancers [17]. The nature of multicentric gastric cancer may make preoperative diagnosis more difficult. Therefore, before ESD of large lesions, a detailed evaluation of lesion thickness by adjusting air volume and/or endoscopic ultrasonography (EUS) for depth prediction may be useful. In our institutions, EUS is performed more often for suspected submucosal (SM) cancer. Therefore, most cases of suspected SM cancer determined by EUS for lesions larger than 5 cm are not included in the present case because surgery is selected in such cases. Tsujii et al. investigated the ability of conventional endoscopy (CE) and EUS to diagnose the depth of early gastric cancer and reported that 93% of those diagnosed as cM-SM1 by CE were pM-SM1, while 62% of those diagnosed as deeper than SM2 by CE were pM-SM1 by EUS [18]. When the diagnosis by EUS was preferentially applied to these lesions, it salvaged 62% of the over-diagnosed cancers. Based on these results, they proposed an algorithm to perform EUS when CE findings were suspicious for deep invasion of SM, and we mainly use that algorithm to diagnose early gastric cancer. Yamamoto et al. showed that lesions in the upper and middle portions of the stomach (and of a large size) were significantly associated with poor image quality and incorrect diagnosis of EUS. For large lesions, it is difficult to examine the entire lesion with EUS, which may be the reason for many misdiagnoses. The usefulness of depth diagnosis, including EUS, for large lesions should be further investigated.
Regarding treatment strategies, en bloc resection could be performed safely in most cases (approximately 98%) only by considering natural traction and appropriate resection sequence, probably because ESD was performed by experts or well-trained trainees supervised by experts [19]. It was up to the physicians to decide whether or which assist method (countertraction method or tunneling method), to use in combination with standard ESD. However, assisted ESD was used relatively often for 5 cm or larger lesions, probably because the ≥ 5 cm group included more complex cases with fibrosis or more gastric lesions in the middle-upper body with intraoperative bleeding and difficult proximity to the lesion. Meanwhile, in terms of adverse events, the rate of post-ESD bleeding, intraoperative perforation, and stenosis was comparable, but delayed perforation was more common in the ≥ 5 cm group. The incidence of delayed perforation is rare (0.4%) [5]. The cause of delayed perforation is unclear, but previous reports suggest that delayed perforation is more common in gastric tube cases, and intraoperative excessive thermal damage may be a contributing factor [20, 21]. There were no cases of delayed perforation in the gastric tube cases in this study. In the > 5 cm group, there were two cases of delayed perforation, and both lesions were upper gastric lesions > 10 cm, one of which was a remnant stomach case. Both cases had lesions larger than 10 cm and increased coagulation procedures, which may have led to the risk of delayed perforation. Meanwhile, Tanaka et al. evaluated the technical difficulty of ESD in cases of the remnant stomach after distal gastrectomy (DG) [22]. Out of 201 patients, 4 (2.0%) reported delayed perforation. After DG, bile and pancreatic juice may easily backflow into the stomach, causing the gastric mucosa to become fragile and prone to easy bleeding. Apart from gastric tube cancer, large-size lesions after DG also need careful evaluation for ESD indications.
There are some limitations to this study. First, this retrospective study may have an institutional selection bias. All cases received treatment in the high-volume center with some experienced endoscopists, which may lead to overestimating the effectiveness and feasibility of the technique. Second, the patient with endoscopic findings of obvious deep submucosal invaded cancer was excluded from this study and underwent surgery as an alternative strategy. However, there were no cases treated by ESD due to technical difficulties. Third, this study only assessed short-term prognosis, and the long-term prognosis remains unclear. Given these limitations, a prospective, multicenter study is needed.
In conclusion, this study demonstrated that ESD for gastric lesions larger than 5 cm could achieve a high en bloc resection rate with the development of a strategy during the procedure, and curative resection was achieved in about two-thirds of cases, while delayed complications required attention.
References
Ono H, Kondo H, Gotoda T, Shirao K, Yamaguchi H, Saito D, et al. Endoscopic mucosal resection for treatment of early gastric cancer. Gut. 2001;48:225–9.
Gotoda T. Endoscopic resection of early gastric cancer. Gastric Cancer. 2007;10:1–11.
Ono H, Yao K, Fujishiro M, Oda I, Nimura S, Yahagi N, et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer. Dig Endosc. 2016;28:3–15.
Hasuike N, Ono H, Boku N, Mizusawa J, Takizawa K, Fukuda H, et al. A non-randomized confirmatory trial of an expanded indication for endoscopic submucosal dissection for intestinal-type gastric cancer (cT1a): the Japan Clinical Oncology Group study (JCOG0607). Gastric Cancer. 2018;21:114–23.
Ono H, Yao K, Fujishiro M, Oda I, Uedo N, Nimura S, et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer (second edition). Dig Endosc. 2021;33:4–20.
Yano T, Hasuike N, Ono H, Boku N, Ogawa G, Kadota T, et al. Factors associated with technical difficulty of endoscopic submucosal dissection for early gastric cancer that met the expanded indication criteria: post hoc analysis of a multi-institutional prospective confirmatory trial (JCOG0607). Gastric Cancer. 2020;23:168–74.
Higashimaya M, Oka S, Tanaka S, Sanomura Y, Yoshida S, Hiyama T, et al. Outcome of endoscopic submucosal dissection for gastric neoplasm in relationship to endoscopic classification of submucosal fibrosis. Gastric Cancer. 2013;16:404–10.
Fujimoto K, Fujishiro M, Kato M, Higuchi K, Iwakiri R, Sakamoto C, et al. Guidelines for gastroenterological endoscopy in patients undergoingantithrombotic treatment. Dig Endosc. 2014;26:1–14.
Kato M, Uedo N, Hokimoto S, Ieko M, Higuchi K, Murakami K, et al. Guidelines for gastroenterological endoscopy in patients undergoing antithrombotic treatment: 2017 appendix on anticoagulants including direct oral anticoagulants. Dig Endosc. 2018;30:433–40.
Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer. 2021;24:1–21.
Suzuki H, Takizawa K, Hirasawa T, Takeuchi Y, Ishido K, Hoteya S, et al. Short-term outcomes of multicenter prospective cohort study of gastric endoscopic resection: ‘Real-world evidence’ in Japan. Dig Endosc. 2019;31:30–9.
Takizawa K, Ono H, Hasuike N, Takashima A, Minashi K, Boku N, et al. A non-randomized single-arm confirmatory trial of endoscopic submucosal dissection to expand its indication for early gastric cancer of undifferentiated type: Japan Clinical Oncology Group Study (JCOG1009/1010). Gastrointest Endosc. 2019;89:AB347–8.
Okada K, Fujisaki J, Kasuga A, Omae M, Hirasawa T, Ishiyama A, et al. Diagnosis of undifferentiated type early gastric cancers by magnification endoscopy with narrow-band imaging. J Gastroenterol Hepatol. 2011;26:1262–9.
Yabuuchi Y, Takizawa K, Kakushima N, Kawata N, Yoshida M, Yamamoto Y, et al. Discrepancy between endoscopic and pathological ulcerative findings in clinical intramucosal early gastric cancer. Gastric Cancer. 2021;24:691–700.
Mitsunaga A, Shirato I, Nishino T, Imai R, Kishino M, Konishi H, et al. Diagnosis of SM1 differentiated type early gastric cancer (penetrates into the submucosa less than 500 m)—compared with SM2 early gastric cancer (penetrates into the submucosa over 500 m): endoscopic diagnosis of depressed type early gastric cancer with converging folds. Stomach Intest. 2007;42:61–8 (in Japanese with English abstract).
Yasui A, Hirase Y, Miyake M, Kidokoro T, Murakami T, et al. Pathology of superficial spreading type of gastric cancer. Stomach Intest. 1973;8:1305–10 (in Japanese with English abstract).
Mizutani M, Takahashi H, Hanamura S, Nagahama M. Superficial spreading type of early gastric cancer on the basis of clinicopathological features and the progress: a clinical study. J Showa Univ Soc. 2015;75:551–60 (in Japanese with English abstract).
Tsujii Y, Kato M, Inoue T, Yoshii S, Nagai K, Fujinaga T, et al. Integrated diagnostic strategy for the invasion depth of early gastric cancer by conventional endoscopy and EUS. Gastrointest Endosc. 2015;82:452–9.
Tsuji Y, Ohata K, Sekiguchi M, Ito T, Chiba H, Gunji T, et al. An effective training system for endoscopic submucosal dissection of gastric neoplasm. Endoscopy. 2011;43:1033–8.
Suzuki H, Oda I, Sekiguchi M, Abe S, Nonaka S, Yoshinaga S, et al. Management and associated factors of delayed perforation after gastric endoscopic submucosal dissection. World J Gastroenterol. 2015;21:12635–43.
Hanaoka N, Uedo N, Ishihara R, Higashino K, Takeuchi Y, Inoue T, et al. Clinical features and outcomes of delayed perforation after endoscopic submucosal dissection for early gastric cancer. Endoscopy. 2010;42:1112–5.
Tanaka S, Yoshizaki T, Yamamoto Y, Ose T, Ishida T, Kitamura Y, et al. The risk scoring system for assessing the technical difficulty of endoscopic submucosal dissection in cases of remnant gastric cancer after distal gastrectomy. Surg Endosc. 2022;36:1482–9.
Acknowledgements
The authors would like to thank the staff of the participating institutions for their support in recruiting eligible patients, and also the patients who participated in this study.
Funding
This study was not externally funded. There was no sponsor for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chiba, H., Ohata, K., Tachikawa, J. et al. The feasibility and safety of endoscopic submucosal dissection of gastric lesions larger than 5 cm. Gastric Cancer 25, 1031–1038 (2022). https://doi.org/10.1007/s10120-022-01323-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-022-01323-8