
Abstract
Purpose
To compare the short- and long-term clinical outcomes, operation times, restoration rate, dosage of polymethylmeth-acrylate (PMMA) injected, complications and X-rays exposure frequency between unilateral and bilateral kyphoplasty approaches for the treatment of OVCF.
Study design
Systematic review and meta-analysis.
Methods
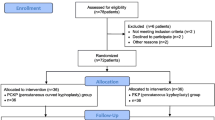
Randomized or non-randomized controlled trials published up to April 2015 that compared the unilateral and bilateral PKP for the treatment of OVCF were acquired by a comprehensive search in the Cochrane Controlled Trial Register, PubMed, MEDLINE, EMBASE, Web of Science, OVID. Exclusion criteria were patients with neoplastic etiology (metastasis or myeloma), infection, neural compression syndrome, invasive and degenerative disease, traumatic fracture, re-operation, neurological deficits, significant scoliosis and spinal stenosis. The main end points included: operation times, the short- and long-term postoperative Visual Analogue Scale (VAS) scores, the short-term postoperative Oswestry Disability Index (ODI), restoration rate, dosage of PMMA injected, cement leakage, X-ray exposure frequency and postoperative adjacent-level fractures.
Results
A total of 8 studies involving 428 patients were included in the meta-analysis. The mean operative time was shorter in the unilateral groups compared with the bilateral groups [P < 0.05, weighted mean difference (WMD) −19.74 (−30.56, −8.92)]. There was no significant difference in the short-term postoperative VAS scores [P > 0.05, WMD 0.03 (−0.34, 0.40)], the long-term postoperative VAS scores between them [P > 0.05, WMD 0.01 (−0.42, 0.45)] and the short-term postoperative ODI [P > 0.05, WMD −0.33 (−2.36, 1.69)] between the two groups. The unilateral approaches required significantly less dosage of PMMA than the bipedicular approaches did [P < 0.05, WMD −1.56 (−1.59, −1.16)]. The restoration rate in the bilateral groups was higher than the unilateral groups [P < 0.05, WMD −7.82 (−12.23, −3.41)]. There was no significant difference in the risk ratio of cement leakage [P > 0.05, RR 0.86 (0.36, 2.06)] and postoperative adjacent-level fractures [P > 0.05, RR 0.91 (0.25, 3.26)] between the two methods. The mean X-ray exposure frequency in the unilateral groups was greater than the bilateral groups [P < 0.05, WMD −5.69 (−10.67, −0.70)].
Conclusions
A definitive verdict could not be reached regarding which approach is better for the treatment of OVCF. Although unilateral PKP was associated with shorter operative time, less X- ray exposure frequency and dosage of PMMA than bilateral PKP. There was no apparent difference in the short- and long-term clinical outcomes and complications between them. However, bilateral PKP approaches were higher than unilateral PKP in term of the restoration rate. But on account of lack of some high-quality evidence, we hold that amounts of high-quality randomized controlled trials should be required and more complications should be analysed to resolve which surgical approach is better for the treatment of OVCF in the future.










Similar content being viewed by others


References
Garfin SR, Yuan HA, Reiley MA (2001) New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine (Phila Pa 1976) 26:1511–1525
Chen H, Tang P, Zhao Y, Gao Y, Wang Y (2014) Unilateral versus bilateral balloon kyphoplasty in the treatment of osteoporotic vertebral compression fractures. Orthopedics 37:e828–e835
Klazen CA, Lohle PN, de Vries J, Jansen FH, Tielbeek AV, Blonk MC, Venmans A, van Rooij WJ, Schoemaker MC, Juttmann JR, Lo TH, Verhaar HJ, van der Graaf Y, van Everdingen KJ, Muller AF, Elgersma OE, Halkema DR, Fransen H, Janssens X, Buskens E, Mali WP (2010) Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): an open-label randomised trial. Lancet 376:1085–1092
Wardlaw D, Cummings SR, Van Meirhaeghe J, Bastian L, Tillman JB, Ranstam J, Eastell R, Shabe P, Talmadge K, Boonen S (2009) Efficacy and safety of balloon kyphoplasty compared with non-surgical care for vertebral compression fracture (FREE): a randomised controlled trial. Lancet 373:1016–1024
Boonen S, Van Meirhaeghe J, Bastian L, Cummings SR, Ranstam J, Tillman JB, Eastell R, Talmadge K, Wardlaw D (2011) Balloon kyphoplasty for the treatment of acute vertebral compression fractures: 2-year results from a randomized trial. J Bone Miner Res 26:1627–1637
Ma XL, Xing D, Ma JX, Xu WG, Wang J, Chen Y (2012) Balloon kyphoplasty versus percutaneous vertebroplasty in treating osteoporotic vertebral compression fracture: grading the evidence through a systematic review and meta-analysis. Eur Spine J 21:1844–1859
Korovessis P, Hadjipavlou A, Repantis T (2008) Minimal invasive short posterior instrumentation plus balloon kyphoplasty with calcium phosphate for burst and severe compression lumbar fractures. Spine (Phila Pa 1976) 33:658–667
Rhyne A, Banit D, Laxer E, Odum S, Nussman D (2004) Kyphoplasty: report of eighty-two thoracolumbar osteoporotic vertebral fractures. J Orthop Trauma 18:294–299
Huang Z, Wan S, Ning L, Han S (2014) Is unilateral kyphoplasty as effective and safe as bilateral kyphoplasties for osteoporotic vertebral compression fractures? A meta-analysis. Clin Orthop Relat Res 472:2833–2842. doi:10.1007/s11999-014-3745-0
Steinmann J, Tingey CT, Cruz G, Dai Q (2005) Biomechanical comparison of unipedicular versus bipedicular kyphoplasty. Spine 30:201–205. doi:10.1097/01.brs.0000150831.46856.87
Chen C, Chen L, Gu Y, Xu Y, Liu Y, Bai X, Zhu X, Yang H (2010) Kyphoplasty for chronic painful osteoporotic vertebral compression fractures via unipedicular versus bipedicular approachment: a comparative study in early stage. Injury 41:356–359. doi:10.1016/j.injury.2009.09.021
Song BK, Eun JP, Oh YM (2009) Clinical and radiological comparison of unipedicular versus bipedicular balloon kyphoplasty for the treatment of vertebral compression fractures. Osteoporos Int 20:1717–1723. doi:10.1007/s00198-009-0872-7
Chen CM, Wei HF, Zhang WJ, Gu Y, Tang GL, Dong RB, Xu Y, Chen L (2011) Comparative study of kyphoplasty for chronic painful osteoporotic vertebral compression fractures via unipedicular versus bipedicular approach. J Spinal Disord Tech 24:E62–E65
Chung HJ, Chung KJ, Yoon HS, Kwon IH (2008) Comparative study of balloon kyphoplasty with unilateral versus bilateral approach in osteoporotic vertebral compression fractures. Int Orthop 32:817–820. doi:10.1007/s00264-007-0439-1
Wang Z, Wang G, Yang H (2012) Comparison of unilateral versus bilateral balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. J Clin Neurosci 19:723–726. doi:10.1016/j.jocn.2011.08.023
Wang H, Sun Z, Wang Z, Jiang W (2015) Single-balloon versus double-balloon bipedicular kyphoplasty for osteoporotic vertebral compression fractures. J Clin Neurosci 22:680–684. doi:10.1016/j.jocn.2014.10.014
Chen L, Yang H, Tang T (2011) Unilateral versus bilateral balloon kyphoplasty for multilevel osteoporotic vertebral compression fractures: a prospective study. Spine (Phila Pa 1976) 36:534–540. doi:10.1097/BRS.0b013e3181f99d70
Rebolledo BJ, Gladnick BP, Unnanuntana A, Nguyen JT, Kepler CK, Lane JM (2013) Comparison of unipedicular and bipedicular balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures: a prospective randomised study. Bone Joint J 95-B:401–406
Yang LY, Wang XL, Zhou L, Fu Q (2013) A systematic review and meta-analysis of randomized controlled trials of unilateral versus bilateral kyphoplasty for osteoporotic vertebral compression fractures. Pain Phys 16:277–290
Graham J, Ahn C, Hai N, Buch BD (2007) Effect of bone density on vertebral strength and stiffness after percutaneous vertebroplasty. Spine (Phila Pa 1976) 32:E505–E511
Fehlings MG (2009) The safety of percutaneous vertebroplasty and kyphoplasty. J Neurosurg Spine 11:605–606
Chen B, Li Y, Xie D, Yang X, Zheng Z (2011) Comparison of unipedicular and bipedicular kyphoplasty on the stiffness and biomechanical balance of compression fractured vertebrae. Eur Spine J 20:1272–1280
Lin J, Zhang L, Yang HL (2013) Unilateral versus bilateral balloon kyphoplasty for osteoporotic vertebral compression fractures. Pain physsician 16:447–453
Feng JZQ, Xiao SX, Xia P (2012) Clinical comparison of unilateral and bilateral percutaneous kyphoplasty for treating osteoporotic vertebral compression fracture. Chinese J Trad Med Traum Orthop 20:26–29
Doo TH, Shin DA, Kim HI, Shin DG, Kim HJ, Chung JH, Lee JO (2008) Clinical relevance of pain patterns in osteoporotic vertebral compression fractures. J Korean Med Sci 23:1005–1010
Ren HL, Jiang JM, Chen JT, Wang JX (2015) Risk factors of new symptomatic vertebral compression fractures in osteoporotic patients undergone percutaneous vertebroplasty. Eur Spine J 24:750–758
Chong T, Lieu J, Alamin T, Mitra R (2011) Pulmonary cement embolism after kyphoplasty. Pain Pract 11:570–573
Krueger A, Bliemel C, Zettl R, Ruchholtz S (2009) Management of pulmonary cement embolism after percutaneous vertebroplasty and kyphoplasty: a systematic review of the literature. Eur Spine J 18:1257–1265
Wang E, Yi H, Wang M, Huang C (2013) Treatment of osteoporotic vertebral compression fractures with percutaneous kyphoplasty: a report of 196 cases. Eur J Orthop Surg Tr 23:S71–S75
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest concerning this article.
Rights and permissions
About this article

Cite this article
Cheng, X., Long, HQ., Xu, JH. et al. Comparison of unilateral versus bilateral percutaneous kyphoplasty for the treatment of patients with osteoporosis vertebral compression fracture (OVCF): a systematic review and meta-analysis. Eur Spine J 25, 3439–3449 (2016). https://doi.org/10.1007/s00586-016-4395-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-016-4395-6