
Abstract
Introduction
Midflexion stability can potentially improve the outcome of total knee arthroplasty (TKA). The purpose of this study was to evaluate the correlation between varus–valgus stability at 0° of extension and 90° of flexion and that at the midflexion range in posterior-stabilized (PS)-TKA.
Materials and methods
Forty-three knees that underwent PS-TKA were evaluated. Manual mild passive varus–valgus stress was applied to the knees, and the postoperative maximum varus–valgus stability was measured every 10° throughout range of motion, using a navigation system. Correlations between the stability at 0°, 90° of flexion, and that at each midflexion angle were evaluated using Spearman’s correlation coefficients.
Results
The stability of 0° modestly correlated with that of 10°–20°, but it did not significantly correlate with that of 30°–80°. However, the stability of 90° strongly correlated with that of 60°–80°, modestly correlated with that of 40°–50°, weakly correlated with that of 20°–30°, and did not correlate with that of 10°.
Conclusions
The present study confirmed the importance of acquiring stability at 90° flexion to achieve midflexion stability in PS-TKA. However, initial flexion stability did not strongly correlate with the stability at either 0° or 90°. Our findings can provide useful information for understanding varus–valgus stability throughout the range of motion in PS-TKA. Attention to soft tissue balancing is necessary to stabilize a knee at the initial flexion range in PS-TKA.
Similar content being viewed by others


Introduction
Analyses of failure mechanisms following total knee arthroplasty (TKA) show that instability is a commonly identified cause for revision [1,2,3]. Advantages of adequate soft tissue balancing include enhanced clinical outcomes and postoperative patient satisfaction [3, 4]. In contrast, increased implant wear, pain, loosening, and instability are linked to inadequate soft tissue balance [3, 5,6,7,8]. Recently, there has been increased interest in the varus–valgus stability in the coronal plane [9,10,11]. In addition, activities of daily living cause mechanical load on the knee joint, both in full extension and in midflexion [12]. However, studies on midflexion stability have been limited due to the difficulty of correctly assessing the knee flexion angle, despite its importance. Insufficient assessment of the midflexion stability may have resulted in apparently contradictory conclusions about the association between stability and outcomes in previous studies. Practically speaking, unexpected wear and complications with the post-cam mechanism have been reported [13, 14]. Midflexion stability may improve outcomes and patient satisfaction.
The acquisition of appropriate soft tissue balance is largely dependent on the surgeon’s intraoperative judgment. To avoid instability caused by inappropriate soft tissue balance, a widely recognized goal is to adjust the soft tissue envelope to feel stable in 0° extension and 90° flexion by using a manual stress test, gap spacer, or tension meter. This technique can reliably achieve a more stabilized knee in 0° extension and 90° flexion. However, it is unclear whether it can achieve stability at the midflexion range.
It is hypothesized that intraoperative varus–valgus stability at 0° and 90° has an impact on postoperative varus–valgus stability at the midflexion range, and this impact differs between each degree of flexion. The purpose of this study was to evaluate the correlation between varus–valgus stability at 0° extension and 90° flexion and that at the midflexion range.
Materials and methods
Forty-three patients underwent TKA with the PS prosthesis (LPS-flex; Zimmer, Warsaw, IN, USA) using a navigation system (precisioN Knee Navigation Software, version 4.0; Stryker, Kalamazoo, MI, USA). To minimize the influences of clinical variables, patients with valgus knee or preoperative severe contracture (>20° or <90°) were excluded. The patient population included 28 women and 15 men with a mean age of 77 ± 4.8 years. The study population was normally distributed. The average preoperative hip knee ankle angle was 14.2° ± 5.5° in varus knees and the postoperative hip knee ankle angle was 0.0° ± 2.0°.
The institutional review board of our university approved this study, and informed consent was obtained from all patients.
Surgical procedure and varus–valgus stability measurements
The air tourniquet was inflated to 250 mmHg under general anesthesia in all cases intraoperatively, and specific anatomic reference points were located by anchoring infrared signal transducers into the femur and tibia with pins. Then, the skin incision was made, and the subcutaneous tissue was exposed. Registration was performed with osteophytes and soft tissues, including the intact preservation of the anterior cruciate ligament (ACL). The anteroposterior and rotational axes of the femur and tibia were identified based on anatomical landmarks. The femoral rotation axis was defined by referring to the average rotation axis of the axis perpendicular to the white side line and parallel to the transepicondylar axis. The tibial rotation axis was directed along the line from one-third of the tibial tubercle to the central point of the transverse diameter, excluding the osteophytes calculated during preoperative planning.
In the next step, the distal femur was cut using the navigation-assisted measured resection technique; the proximal tibial cut was made using extramedullary alignment rods. After removing the osteophytes, trial components were placed into the knee, and the knee was manually maneuvered throughout flexion to assess soft tissue balance. When the soft tissue balance was inappropriate, the medial collateral ligament, posterior knee capsule, or other tissue was carefully avulsed in an incremental manner for adjustment. After confirming that the TKA components and inserts were firmly placed in an appropriate position, the surgical incision was completely closed. The investigator gently applied physiologically allowable maximal manual varus–valgus stress to the knee without angular acceleration, and the varus–valgus angle of the femorotibial axis was measured automatically by the navigation system every 10° throughout flexion. The results obtained by a single investigator. The navigation system determined the varus–valgus orientation using Euler angles and spatial coordinates, which allowed for the assessment of varus–valgus angulation independent of knee flexion and rotation (positive values indicate varus orientation, and negative values indicate valgus orientation).
Power sample analysis and validation
To achieve a correlation of ρ = 0.5 with 80% power and an α = 0.05, it was calculated that a minimum sample size of 30 participants would be required. The accuracy of the navigation system was established at 0.5°. Preliminary investigations confirmed that the test–retest reliability of varus–valgus stress angles indicated that the interclass and intraclass correlation coefficients (ICCs) were sufficiently high, with values >0.8 at each measured knee flexion angle.
Statistical analysis
Non-parametric tests were used because of the small sample size, although an arithmetically sufficient normal distribution was found. Correlations were evaluated using Spearman’s coefficients of correlation. Analyses were performed with JMP, version 11.0 (SAS Institute, Tokyo, Japan). A ρ value >0.7 was considered a strong correlation; 0.4 < ρ < 0.7 was considered a modest correlation; and 0.2 < ρ < 0.4 was considered a weak correlation. A P value < 0.05 was considered statistically significant. Statistical analyses for ICCs were performed using IBM SPSS, version 23 (IBM Corp., Armonk, NY, USA). An ICC >0.8 was considered an almost perfect correlation.
Results
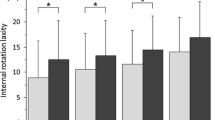
The measurements of postoperative varus–valgus stability throughout range of motion are presented in Fig. 1. Varus–valgus stability increased sharply for the flexion range of 0°–20°, and it changed gradually thereafter.

Bar chart showing the mean postoperative varus–valgus stability throughout the range of flexion in posterior-stabilized total knee arthroplasty. For both charts Y axis varus–valgus stability (°), X axis flexion angle (°). Upper whiskers indicate the standard deviation
Table 1 shows Spearman’s correlations (ρ) between 0°, 90°, and each measured midflexion varus–valgus stability. Results of the assessment of the correlation showed that the stability of 0° modestly correlated with that of 10°–20°, but it did not significantly correlate with that of 30°–80° (Table 1; Fig. 2). However, the stability of 90° strongly correlated with that of 60°–80°, modestly correlated with that of 40°–50°, weakly correlated with that of 20°–30°, and did not correlate with that of 10° (Table 1; Fig. 2).

Scatterplots of varus–valgus stability at 0° and 90° (horizontal axis) and varus–valgus stability at each midflexion angle (vertical axis). a 20°, b 40°, c 60°, d 80°
Values dividing the amount of varus–valgus stability at 90° by the amount of varus–valgus stability at 0° were significantly correlated with the amount of varus–valgus stability at 10° and 50°–80° (Table 2). However, no significant correlation was observed between the amount of varus–valgus stability at 20°–40° and the values dividing the amount of varus–valgus stability at 90° by the amount of varus–valgus stability at 0° (Table 2).
Discussion
The most important finding of this study was that stability at 0° modestly correlated with stability in the narrow range up to 20°. However, stability at 90° correlated with stabilities in the comparatively wide range from 20° to 80°. This suggests the importance of acquiring stability at 90° flexion to achieve midflexion stability in PS-TKA.
Accurate intraoperative soft tissue evaluation is made possible by recent technological advances, such as the tension meter and navigation system [10, 15,16,17,18]. However, clear indicators of soft tissue balance remain elusive. Traditionally, the aim of TKA is to achieve equal medial and lateral gaps as well as equal flexion and extension gaps. Yet, the feasibility of this concept for all cases remains controversial. One reason is that normal knees do not always have equal medial and lateral gaps or equal flexion and extension gaps [19, 20]. Nowakowski et al. demonstrated that extension and flexion gaps are asymmetric and unequal. They also showed that ACL and posterior cruciate ligament (PCL) resections produce varying gap changes using a prototypical force determining ligament balancer without the need for bony resection. The sequential cruciate ligament resections tended to reflect varying TKA designs [21]. The cruciate ligaments, functioning as secondary stabilizers against varus–valgus torque, bear approximately one-fourth of the varus–valgus load of the collateral ligaments [22, 23]. Therefore, in PS-TKA, instability in the midflexion range is suspected to occur. Medial release is a classic method for adjusting soft tissue balance. Complete release of the medial collateral ligament (MCL) increases medial stability to 6.9° in full extension and 13.4° at 90° flexion [24]. Releasing the MCL enlarges the medial flexion gap more than the extension gaps [25]. These results illustrate the difficulty in managing extension imbalance using only medial release.
To avoid instability caused by inappropriate soft tissue balance, a widely recognized goal in PS-TKA is to create symmetric, rectangular gaps (equal medial and lateral gaps as well as equal flexion and extension gaps); this has been named the gap technique. This concept can reliably achieve a more stable knee in 0° extension and 90° flexion. However, it is unclear if this technique can achieve stability at the midflexion range. Minoda et al. reported that the center size of the joint gap was loose, especially at 30° flexion in PS-TKA, even when using the gap technique. The authors postulate that this is probably because in PS-TKA, both the ACL and PCL are sacrificed and a cam-post mechanism regulates the anterior–posterior translation. There is no stabilizer of the anterior–posterior translation in the midflexion range in which the cam-post mechanism does not engage. Incavo et al. [11] examined the relationship between the difference of alignment axes and the implication of medial–lateral soft tissue balance in TKA. Their result indicated that measurements of medial and lateral joint spacing are statistically significantly different at all flexion angles between the two alignments. The anatomic alignment axes’ pattern demonstrates midflexion lateral opening and late-flexion medial joint space opening. On the other hand, mechanical axes have a consistent 2–3 mm larger lateral space than a medial joint space. In addition to these factors, the insert thickness, changes of posterior condylar offset, and design of the prosthesis has been also reported affect midflexion stability [26,27,28].
The present study showed that varus–valgus stability in the initial flexion range did not strongly correlate with stability at 0° or 90°. We expected a similar correlation at the wide range in midflexion and 0° in extension positions. However, modest correlation was found with 10° and 20°. Moreover, the present study showed that the values dividing the amount of varus–valgus stability at 90° by the amount of varus–valgus stability at 0° were significantly correlated only with the amount of varus–valgus stability at 10° and 50°–80°. No significant correlation was observed with the amount of varus–valgus stability at 20°–40°. These findings indicate that it is not possible to reliably acquire stability at the initial flexion range, even when achieving a stable knee at 0° extension and 90° flexion, and even when achieving equal flexion and extension stability. This suggests the possibility that another element is involved in stabilities at the initial flexion range. In some cases, removing the ACL/PCL in PS-TKA would lead to large stability at the initial flexion range, despite the recovery of proper soft tissue balance in 0° knee extension and 90° knee flexion. Careful attention would be necessary to prevent varus–valgus instability in the initial flexion range in PS-TKA. To adjust the stability of the initial flexion range in PS-TKA, it has been suggested that precise surgical measures, further improvement in the implant design, joint line control, matching implant sizes, and other factors are needed.
One limitation of this study is that it reported on the LPS-flex model only. The measured resection technique was used for bone cutting, and surgery was performed using tourniquet vascularization and non-load-bearing conditions under general anesthesia. Additionally, only patients with varus-type arthritis were treated, and the procedure involved manual passive stress by the operator. Furthermore, stress force was not standardized. These limitations restrict the generalization of our results. Ghosh et al. [10] confirmed that computer navigation can be used to analyze soft tissue balance during TKA beyond the coronal plane and throughout range of motion, and stress test results showed reproducible patterns of soft tissue balance. The strengths of the current study include the use of a navigation system that enabled precise evaluation of varus–valgus position throughout the range of motion. Additionally, evaluating the postoperative outcome at a final state of healing with a strong suture to the capsule and skin was clinically meaningful. Future research is required to determine the degree of varus–valgus stability adequate for TKA procedures. Moreover, further study is required to improve the surgical theory and implant design to reliably achieve full range stability, and to investigate the relationship between midflexion stability and patients’ clinical outcome.
Conclusions
Varus–valgus stability at 0° extension correlates with narrow, initial flexion range stability. Varus–valgus stability at 90° flexion correlates with stability at a wide midflexion range, confirming its importance in acquiring stability at 90° flexion to achieve midflexion stability. The present results will help orthopedists understand the midflexion stability after PS-TKA.
References
Mulhall KJ, Ghomrawi HM, Scully S, Callaghan JJ, Saleh KJ (2006) Current etiologies and modes of failure in total knee arthroplasty revision. Clin Orthop Relat Res 446:45–50. doi:10.1097/01.blo.0000214421.21712.62
Sharkey PF, Hozack WJ, Rothman RH, Shastri S, Jacoby SM (2002) Insall Award paper. Why are total knee arthroplasties failing today? Clin Orthop Relat Res 404:7–13
Thiele K, Perka C, Matziolis G, Mayr HO, Sostheim M, Hube R (2015) Current failure mechanisms after knee arthroplasty have changed: polyethylene wear is less common in revision surgery. J Bone Joint Surg Am 97:715–720. doi:10.2106/JBJS.M.01534
Matsuda Y, Ishii Y, Noguchi H, Ishii R (2005) Varus-valgus balance and range of movement after total knee arthroplasty. J Bone Joint Surg Br 87:804–808. doi:10.1302/0301-620X.87B6.15256
D’Lima DD, Patil S, Steklov N, Colwell CW Jr (2007) An ABJS best paper: dynamic intraoperative ligament balancing for total knee arthroplasty. Clin Orthop Relat Res 463:208–212
Del Gaizo DJ, Della Valle CJ (2011) Instability in primary total knee arthroplasty. Orthopedics 34:e519–e521
Lombardi AV Jr, Berend KR, Adams JB (2014) Why knee replacements fail in 2013: patient, surgeon, or implant? Bone Jt J 96-B:101–104. doi:10.1302/0301-620X.96B11.34350
Wasielewski RC, Galat DD, Komistek RD (2005) Correlation of compartment pressure data from an intraoperative sensing device with postoperative fluoroscopic kinematic results in TKR patients. J Biomech 38:333–339. doi:10.1016/j.jbiomech.2004.02.040
Cross MB, Nam D, Plaskos C, Sherman SL, Lyman S, Pearle AD, Mayman DJ (2012) Recutting the distal femur to increase maximal knee extension during TKA causes coronal plane stability in mid-flexion. Knee 19:875–879. doi:10.1016/j.knee.2012.05.007
Ghosh KM, Blain AP, Longstaff L, Rushton S, Amis AA, Deehan DJ (2014) Can we define the envelope of stability during navigated knee arthroplasty? Knee Surg Sports Traumatol Arthrosc 22:1736–1743. doi:10.1007/s00167-013-2574-0
Incavo SJ, Schmid S, Sreenivas K, Ismaily S, Noble PC (2013) Total knee arthroplasty using anatomic alignment can produce mid-flexion stability. Clin Biomech (Bristol, Avon) 28:429–435. doi:10.1016/j.clinbiomech.2013.02.012
Laubenthal KN, Smidt GL, Kettelkamp DB (1972) A quantitative analysis of knee motion during activities of daily living. Phys Ther 52:34–43
Mikulak SA, Mahoney OM, dela Rosa MA, Schmalzried TP (2001) Loosening and osteolysis with the press-fit condylar posterior-cruciate-substituting total knee replacement. J Bone Jt Surg Am 83-A:398–403
O’Rourke MR, Callaghan JJ, Goetz DD, Sullivan PM, Johnston RC (2002) Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design: five to eight-year follow-up. J Bone Jt Surg Am 84-A:1362–1371
Hino K, Ishimaru M, Iseki Y, Watanabe S, Onishi Y, Miura H (2013) Mid-flexion stability is greater after posterior-stabilised total knee replacement than with cruciate-retaining procedures: a computer navigation study. Bone Jt J 95-B:493–497
Hino K, Kutsuna T, Oonishi Y, Watamori K, Kiyomatsu H, Iseki Y, Watanabe S, Ishimaru Y, Miura H (2016) Assessment of the midflexion rotational stability in posterior-stabilized total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 31:1–6. doi:10.1007/s00167-016-4175-1
Matsumoto T, Muratsu H, Kubo S, Matsushita T, Kurosaka M, Kuroda R (2011) Soft tissue tension in cruciate-retaining and posterior-stabilized total knee arthroplasty. J Arthroplasty 26:788–795. doi:10.1016/j.arth.2010.06.006
Minoda Y, Nakagawa S, Sugama R, Ikawa T, Noguchi T, Hirakawa M, Nakamura H (2014) Intraoperative assessment of midflexion laxity in total knee prosthesis. Knee 21:810–814. doi:10.1016/j.knee.2014.04.010
Tokuhara Y, Kadoya Y, Nakagawa S, Kobayashi A, Takaoka K (2004) The flexion gap in normal knees. An MRI study. J Bone Jt Surg Br 86:1133–1136
Okazaki K, Miura H, Matsuda S, Takeuchi N, Mawatari T, Hashizume M, Iwamoto Y (2006) Asymmetry of mediolateral stability of the normal knee. J Orthop Sci 11:264–266. doi:10.1007/s00776-006-1009-x
Nowakowski AM, Majewski M, Muller-Gerbl M, Valderrabano V (2012) Measurement of knee joint gaps without bone resection: “physiologic” extension and flexion gaps in total knee arthroplasty are asymmetric and unequal and anterior and posterior cruciate ligament resections produce different gap changes. J Orthop Res 30(4):522–527
Amis AA, Bull AM, Gupte CM, Hijazi I, Race A, Robinson JR (2003) Biomechanics of the PCL and related structures: posterolateral, posteromedial and meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc 11(5):271–281. doi:10.1007/s00167-003-0410-7
Grood ES, Noyes FR, Butler DL, Suntay WJ (1981) Ligamentous and capsular restraints preventing straight medial and lateral stability in intact human cadaver knees. J Bone Jt Surg Am 63:1257–1269
Krackow KA, Mihalko WM (1999) The effect of medial release on flexion and extension gaps in cadaveric knees: implications for soft-tissue balancing in total knee arthroplasty. Am J Knee Surg 12:222–228
Mullaji A, Sharma A, Marawar S, Kanna R (2009) Quantification of effect of sequential posteromedial release on flexion and extension gaps: a computer-assisted study in cadaveric knees. J Arthroplasty 24:795–805. doi:10.1016/j.arth.2008.03.018
Heyse TJ, Tucker SM, Lipman JD, Rajak Y, Imhauser CW, Kia M, Westrich GH (2015) Frontal plane stability following UKA in a biomechanical study. Arch Orthop Trauma Surg 135(6):857–865
Matziolis G, Brodt S, Windisch C, Roehner E (2017) Changes of posterior condylar offset results in midflexion instability in single-radius total knee arthroplasty. Arch Orthop Trauma Surg 137(5):713–717
Minoda Y, Ikebuchi M, Mizokawa S, Ohta Y, Nakamura H (2016) Mobile-bearing TKA improved the anteroposterior joint stability in mid-flexion range comparing to fixed-bearing TKA. Arch Orthop Trauma Surg 136(11):1601–1606
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
There is no funding source.
Conflict of interest
Kazunori Hino received research support from Teijin Nakashima Medical. Hiromasa Miura received research support from Senko Medical Instrument. Tatsuhiko Kutsuna, Kunihiko Watamori, Hiroshi Kiyomatsu, Yasumitsu Ishimaru, Jun Takeba, and Seiji Watanabe declare that they have no conflict of interest.
Ethical approval
The institutional review board of our university approved this study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hino, K., Kutsuna, T., Watamori, K. et al. Varus–valgus stability at 90° flexion correlates with the stability at midflexion range more widely than that at 0° extension in posterior-stabilized total knee arthroplasty. Arch Orthop Trauma Surg 137, 1429–1434 (2017). https://doi.org/10.1007/s00402-017-2779-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-017-2779-7