
Abstract
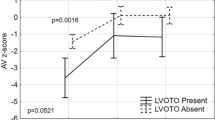
Left ventricular outflow tract obstruction (LVOTO) remains a significant complication after primary repair of interrupted aortic arch with ventricular septal defect (IAA-VSD). Clinical and echocardiographic predictors for LVOTO reoperation are controversial and procedures to prophylactically prevent future LVOTO are not reliable. However, it is important to identify the patients at risk for future LVOTO intervention after repair of IAA-VSD. Patients who underwent single-stage IAA-VSD repair at our center 2006–2021 were retrospectively reviewed, excluding patients with associated cardiac lesions. Two-dimensional measurements, LVOT gradients, and 4-chamber (4C) and short-axis (SAXM) strain were obtained from preoperative and predischarge echocardiograms. Univariate risk analysis for LVOTO reoperation was performed using unpaired t-test. Thirty patients were included with 21 (70%) IAA subtype B and mean weight at surgery 3.0 kg. Repair included aortic arch patch augmentation in 20 patients and subaortic obstruction intervention in three patients. Seven (23%) required reoperations for LVOTO. Patient characteristics were similar between patients who required LVOT reoperation and those who did not. Patch augmentation was not associated with LVOTO reintervention. Patients requiring reintervention had significantly smaller LVOT AP diameter preoperatively and at discharge, and higher LVOT velocity, smaller AV annular diameter, and ascending aortic diameter at discharge. There was an association between LVOT-indexed cross-sectional area (CSAcm2/BSAm2) ≤ 0.7 and reintervention. There was no significant difference in 4C or SAXM strain in patients requiring reintervention. LVOTO reoperation was not associated with preoperative clinical or surgical variables but was associated with smaller LVOT on preoperative echo and smaller LVOT, smaller AV annular diameter, and increased LVOT velocity at discharge.

Similar content being viewed by others

Abbreviations
- AV:
-
Aortic valve
- BSA:
-
Body surface area
- CSA:
-
Cross-sectional area
- DORV:
-
Double outlet right ventricle
- IAA:
-
Interrupted aortic arch
- LVOT(O):
-
Left ventricular outflow tract (obstruction)
- PDA:
-
Patent ductus arteriosus
- STE:
-
Speckle-tracking echocardiography
- TGA:
-
Transposition of the great arteries
- VSD:
-
Ventricular septal defect
References
Lapar DJ, Baird CW (2018) Surgical considerations in interrupted aortic arch. Semin Cardiothorac Vasc Anesth 22(3):278–284
Riggs KW, Tweddell JS (2019) How small is too small? Decision-making and management of the small aortic root in the setting of interrupted aortic arch. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 22:21–26
Chen PC et al (2013) Predictors of reintervention after repair of interrupted aortic arch with ventricular septal defect. Ann Thorac Surg 96(2):621–628
Salem MM et al (2000) Predictors of left ventricular outflow obstruction following single-stage repair of interrupted aortic arch and ventricular septal defect. Am J Cardiol 86(9): 1044–1047, A11.
Apfel HD et al (1998) Usefulness of preoperative echocardiography in predicting left ventricular outflow obstruction after primary repair of interrupted aortic arch with ventricular septal defect. Am J Cardiol 82(4):470–473
Hirata Y et al (2010) Impact of aortic annular size on rate of reoperation for left ventricular outflow tract obstruction after repair of interrupted aortic arch and ventricular septal defect. Ann Thorac Surg 90(2):588–592
Geva T et al (1993) Echocardiographic predictors of left ventricular outflow tract obstruction after repair of interrupted aortic arch. J Am Coll Cardiol 22(7):1953–1960
Abarbanell G et al (2018) Preoperative echocardiographic measures in interrupted aortic arch: which ones best predict surgical approach and outcome? Congenit Heart Dis 13(3):476–482
Harrington JK et al (2021) Normal left ventricular systolic and diastolic strain rate values in children derived from two-dimensional speckle-tracking echocardiography. J Am Soc Echocardiogr 34(12):1303–1315.e3
Chang JC et al (2020) Echocardiographic strain analysis reflects impaired ventricular function in youth with pediatric-onset systemic lupus erythematosus. Echocardiography 37(12):2082–2090
Harrington JK et al (2019) Serial changes in right ventricular systolic function among rejection-free children and young adults after heart transplantation. J Am Soc Echocardiogr 32(8):1027–1035.e2
Sun JP et al (2019) Echocardiographic strain in hypertrophic cardiomyopathy and hypertensive left ventricular hypertrophy. Echocardiography 36(2):257–265
Cvijic M, Voigt JU (2020) Application of strain echocardiography in valvular heart diseases. Anatol J Cardiol 23(5):244–253. https://doi.org/10.14744/AnatolJCardiol.2020.09694. (PMID:32352410; PMCID:PMC7219305)
Alsoufi B et al (2016) Selective management strategy of interrupted aortic arch mitigates left ventricular outflow tract obstruction risk. J Thorac Cardiovasc Surg 151(2):412–421.e2
Jijeh A, Ismail M, Alhabshan F (2017) Growth of left ventricular outflow tract and predictors of future re-intervention after repair for ventricular septal defect and aortic arch obstruction. Cardiol Young 27(7):1323–1328
Mayor JM et al (2019) Sex-based differences in ten-year nationwide outcomes of carotid revascularization. J Am Coll Surg 229(1):38–46.e4
Author information
Authors and Affiliations
Contributions
HM and DB conceptualized the study and collected data. JH and NP reviewed echocardiographic studies and performed measurements. EB, DK, and SL assisted in development of measurement guidelines and criteria, as well as expert review and input critical for formation of the project. HM completed all analysis, wrote the main manuscript text, and prepared all tables and figure.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
McMullen, H.L., Harrington, J.K., Blitzer, D. et al. Clinical Outcomes and Echocardiographic Predictors of Reintervention After Interrupted Aortic Arch Repair. Pediatr Cardiol 45, 967–975 (2024). https://doi.org/10.1007/s00246-024-03419-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-024-03419-7