
Abstract
Background
Valve repair is the treatment of choice for native mitral valve regurgitation. The feasibility of repair when the defect is caused by acute infective endocarditis (IE) is debated. This study aims to compare the outcome of repair and replacement procedures, to report the rate of repair in a single surgical center, and to review the literature on this topic.
Results
We retrospectively analyzed 108 patients with native mitral IE, potentially eligible for surgical repair. Of these 108, 90 (83%) underwent surgery, and 18 were treated conservatively. Among the 90 surgical patients, 57 (63%) underwent valve replacement and 33 valve repair (37%). The mean follow-up duration was 3 years. The two primary endpoints were mortality and freedom from recurrent endocarditis. Secondary endpoints were the post-operative incidence of major adverse events (hospitalization for any cause, pacemaker implantation, new onset of atrial fibrillation, sternal dehiscence), left ventricular systolic function (LVSF), and valvular function at 1-year echocardiographic follow-up. All-cause mortality was lower for valve repair, although not significantly (p = 0.86), as well as nonfatal adverse events (p = 0.92) and relapse rate (p = 0.20) at 3 years. We did not find differences between the two groups at echocardiographic follow-up, neither for left ventricular systolic function (p = 0.22), nor for valvular continence (p = 0.28).
Conclusions
In our experience, the mid-term outcome of repair in IE is comparable to valve replacement and should be considered whenever possible, as in degenerative valve disease. The review of the literature supports this strategy.
Similar content being viewed by others
Background
Treatment of infective endocarditis (IE) is surgical in patients with complications: heart failure, a paravalvular extension of the infection, sepsis unresponsive to antibiotics, systemic embolism despite appropriate antibiotic therapy, and occasionally for large vegetation. While the treatment of choice for degenerative mitral valve regurgitation is valve repair, this is often challenging in IE because of structural damage and concerns regarding durability. For eradication of infection, all grossly infected tissue must be removed, limiting the possibility of repair. In expert hands, however, it can be approached by different techniques.
In patients undergoing surgery for mitral, several studies and meta-analyses have suggested a more favorable survival following valve repair, compared to replacement [1,2,3,4,5,6,7,8]. These data derive from small, retrospective observational studies, and a selection process triaging milder patients for repair represents a likely bias. On the other hand, randomized trials appear scarcely feasible in this setting, owing to the rarity of IE and different clinical profiles of candidates for the two procedures. Thus, there is still a need for further single-center investigation in this field that is the base for future meta-analyses. We assessed the feasibility and outcomes of valve repair in a consecutive series of IE patients seen in a surgical center in Florence and provided 1-year echocardiographic follow-up.
Methods
Patient selection
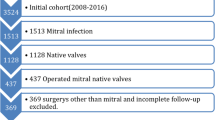
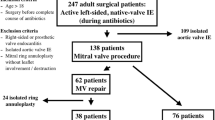
During the last 3 years, we have collected all the cases admitted to our department between January 2013 and December 2019 with a definite diagnosis of IE, according to modified Duke University criteria [9]. In this way, we have generated a single-center registry of IE, consisting now of 363 patients and 294 variables. Among these 363 cases, we retrospectively selected 108 consecutive patients with a definite diagnosis of native mitral valve IE. Of these 108, 90 were treated surgically and constituted our study cohort: 57 underwent valve replacement (63%) and 33 valve repair (37%) (Fig. 1). Of these 90 patients, 20 also had a second infected valve (19 aortic and one tricuspid): aortic valves were replaced in all cases, while the tricuspid one was repaired (Fig. 2).

Study flow chart

Echocardiographic images of the patient with mitral and tricuspid IE. a 3D transesophageal view of mitral valve. b 2D transesophageal view of mitral valve. c Transthoracic four chamber view before surgery. d Transthoracic four chamber view after surgery. Vegetation is marked with arrows in each view
Data collection method, diagnostic work-up, and surgical indications are reported in another study conducted on the same registry, focusing on embolic risk stratification in patients with IE [10].
Operative technique
Surgical planning was re-evaluated intraoperatively, based on direct valve inspection. Underlying valve disease in patients treated with valve repair and replacement is reported in Table 1 and the surgical procedures for valve repair for each specific lesion are listed in Table 2. An example of mitral repair is reported in Fig. 3.

Mitral endocarditis with perforation of the anterior leaflet. a, b After careful debridement and removal of the infected tissue, a large hole is left in the body of the anterior mitral leaflet. The perforation is repaired with an appropriate size fresh autologous pericardial patch (c). The final test with saline demonstrates a perfectly competent mitral valve (d)
Follow-up and study endpoints
The follow-up duration was calculated from the time of IE diagnosis to the final contact. A structured phone interview was implemented to update the follow-up of all patients to December 2019. In a subset of 32 patients, 1-year echocardiographic follow-up was performed (13 repairs, 19 replacements). The two primary endpoints were mortality and freedom from recurrent endocarditis, comparing repair and replacement procedures. Secondary endpoints were the post-operative incidence of major adverse events (hospitalization for any cause, pacemaker implantation, new onset of atrial fibrillation, sternal dehiscence), left ventricular systolic function (LVSF), and valvular function at 1-year echocardiographic follow-up of the two procedures. LVSF was measured through left ventricular ejection fraction (LVEF) at 1-year follow-up and normalized for pre-operative EF; the logarithm of the ratio of LVEF at follow-up and LVEF had a normal distribution. Valvular regurgitation was estimated by the PISA method (Proximal Isovelocity hemispheric Surface Area).
Statistical analysis
We used the chi-square test to compare proportions, the Mann-Whitney test to compare continuous variables with non-normal distribution, and the two-tailed Student’s t test for continuous variables with normal distribution. We performed univariable and multivariable analyses using logistic regression and general linear models. We used the Kaplan-Meier method to estimate the univariate cumulative incidence of events and event-free survival. All tests were 2-sided, and statistical significance was defined as a p value < 0.05. Analyses were performed with SPSS 23.0 package.
Results
The mean age at the time of surgery was 63.6 ± 13.5 years. Of 90 operated patients, seven had undergone previous surgical valve repair. The mean vegetation length was 11.6 ± 7.7 mm. Blood cultures were positive in 81% of cases (Streptococci 31%, Staphylococcus aureus 19%, negative coagulase staphylococci 11%, enterococci 13%, Gram-negative, fungi, and other Gram-positive 6%). IE was at its first occurrence in 83 patients (92%) and relapse in seven (8%). Embolic events were reported at the time of admission in 45 patients (50%), in 23 of whom involving the central nervous system. Early surgery (within 2 weeks of diagnosis) was performed in 70 patients (78%), with valve replacement in 57 (63%) and valve repair in 33 (37%). The repair was performed more frequently in patients with IE involving two valves (12/33 vs. 8/57, p = 0.014), in patients with a first episode of IE (33/33 vs 50/57, p = 0.036), and in patients affected by spondylodiscitis (7/33 vs 4/57, p = 0.048). Moreover, vegetation length was significantly smaller in patients undergoing repair (p = 0.001; best predictive threshold for replacement at ROC analysis 8.5 mm, AUC 0.78; Fig. 4). The presence of endocarditis involving two valves, the combination of endocarditis and spondylodiscitis, having a first episode of IE rather than a relapse, and the vegetation length were not associated with a higher mortality at Kaplan-Meyer survival analysis nor with a higher relapse rate.

ROC curve of vegetation dimension for replacement; AUC 0.78, p = 0.001
The other baseline clinical characteristics were similar in the repair and replacement groups (Table 3).
At multivariable analysis, variables independently associated with repair procedure were vegetation length (OR 0.78, 95% CI 0.69–0.87, p = 0.000), male gender (OR 5.0, 95% CI 1.2–20.7, p = 0.025), and severe valvular dysfunction (OR 0.10, 95% CI 0.02–0.48, p = 0.004).
At echocardiographic follow-up, the logarithm of the ratio of LVEF at follow-up and basal was not statistically different between the two groups (p = 0.22). Severe valvular regurgitation was reported only in 1 patient that had undergone repair, due to residual tethering in severe ventricular dysfunction, without significant difference between the two groups (p = 0.28).
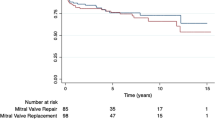
We registered 19 deaths among 90 surgical patients (21%). Three of them were drug abusers and died from complications related to the abuse. The EuroSCORE 2 of the remaining 16 dead patients was 17.3 (SD 13.9, maximum 56.2). Since the follow-up duration was different among patients of our cohort, mortality was extrapolated from Kaplan-Meyer curves. All-cause short-term (30 days, 3 ± 3% vs 4 ± 2% for repair and replacement, respectively) and long-term (3 years, 26 ± 9 vs. 36 ± 11%) mortality was lower for valve repair (Fig. 5), although not significantly (p = 0.86), as well as nonfatal adverse events (15 ± 4 vs. 20 ± 2%, p = 0.92) and relapse rate (1 ± 1% vs. 3 ± 1%, p = 0.20) at 3 years. The absence of statistical significance probably depends on the relatively small size of the sample.

Survival probability (± 95% CI) after repair and replacement procedure in IE
Discussion
The feasibility of mitral valve repair in patients with infective endocarditis is still a matter of debate, since it seems to vary significantly among different centers [11,12,13,14,15,16,17,18,19,20,21,22]. Although most studies agree about the benefits of repair, any single experience adds strength to recommend this strategy.
The main value of the present study is therefore to share a single-center experience that can be useful for future meta-analyses; moreover, we seized the opportunity to review the recent literature about this topic.
Our data reinforce the preference for mitral repair over replacement in IE, not only for the good results in terms of mid-term mortality and relapse rate, but also for 1-year echocardiographic results. More than one third of patients with native mitral valve IE could be managed (in most cases early after diagnosis) with valve repair, with mid-term outcomes (3 years) similar to those obtained with replacement, but with potentially better long-term results. LVEF and valvular continence at follow-up are surrogate endpoints that reflect long-term durability and safety of valve repair.
In our experience, selection for repair was largely based on the qualitative assessment of valvular damage by experienced cardiologists and surgeons.
The repair was particularly favored in the presence of spondylodiscitis to lower the risk of relapse in a subset of patients with an active infective focus. The presence of spondylodiscitis, which may act as a persisting infective focus, should be considered one further reason to attempt at valve repair in IE whenever anatomically feasible, in order to possibly reduce the risk of early relapse.
Notably, most of the baseline features were similar in repair and replacement cohorts.
At multivariable analysis, the main independent predictors of the feasibility of repair were vegetation dimension that was significantly smaller in the repair group, and the entity of mitral regurgitation, where severe regurgitation was inversely associated with the procedure of repair, so we can conclude that the ultimate decision could not be foreseen a priori. While guidelines and algorithms are desirable for IE, these findings suggest that there is no real substitute for direct clinical experience in IE management.
During the last 20 years, many attempts have been undertaken to repair the mitral valve in IE, avoiding the insertion of prosthetic material in infected tissue; the review of the literature shows that an ever-increasing percentage of mitral IE has been judged amenable to valve repair worldwide in the last years, especially if surgery was performed in an early stage (Table 4).
Reconstructive surgery in inflammatory tissue may be hard, and the feasibility of repairing infected mitral valves for acute IE has been reported to vary considerably [11,12,13,14,15,16,17,18]. In a systematic review of 24 studies on this issue, Feringa et al. [3] observed that valve repair was possible in approximately 39% of patients presenting with mitral valve IE, but some recent experiences report a higher feasibility rate, even over 80% [19,20,21].
The repair rate in our study was similar to that reported in the review of Feringa et al., but clearly lower than the feasibility reported by Defauw et al. of 66% [21] or by de Kerchove et al. of 80% [22]; on the other hand, we registered a lower in-hospital mortality (4%) than the latter two, who reported 15.4% and 16%, respectively. We favored safety, at the price of a lower rate of complex repair procedures, with similar long-term survival rate.
Similar to the degenerative MR experience, valve repair recently became the procedure of choice in IE, as confirmed by several studies [18,19,20,21,22]. Patients who undergo mitral valve repair need significantly fewer reinterventions during the early post-operative period and long-term follow-up and have less long-term IE relapses and cerebrovascular events.
The hard task of the surgeon is to balance the risks connected with repair failure with the numerous advantages of a successful repair. This challenge probably gives the reason for the high variability of repair feasibility in the literature.
Okada et al. [20] reported even 86% rate of mitral valve repair, with an in-hospital mortality of 0.7%. However, 67% of patients undergoing valve repair had healed at the time of surgery, and only 33% had active infective endocarditis. For this reason, their valuable experience does not fully answer the query of the feasibility of valve repair in IE. Moreover, in order to prevent embolic events, early surgery is generally preferred over delayed surgery, which is recommended only for conditions that may increase operative mortality, such as large volume (> 2 cm) intracranial hemorrhage.
Solari et al. [17] recently showed that an early repair-oriented surgical approach can achieve high repair rates with a good long-term durability of the repair and a very low rate of recurrence of endocarditis.
In a recent multicentric study in New York and California states, Toyoda et al. [23] reported a mitral repair rate of 19% in 1970 patients with IE; this percentage is probably more representative of the real world. Consistently with the literature, their experience confirmed that repair was associated with better survival and lower risk of recurrent infection compared with valve replacement. Radical removal of all infected material and inflamed tissue is a key issue for successful operative technique, using the broad spectrum of surgical armamentarium to recreate a normal-functioning valve with the available vital tissue. Patching of perforations, vegetectomy, and resection of the involved leaflet and leaflet patching with an autologous or bovine pericardium, commissural debridement, and reconstruction, left ventricular abscess debridement with annular patch reconstruction and leaflet re-suspension with artificial chordae, sliding plasty, flip-over technique, and ring annuloplasty can all be employed to obtain a perfect functional result [22]. Finally, when a repair is not possible and replacement becomes mandatory, the choice between mechanical and bioprosthetic valves should be made based on usual clinical considerations.
The main limitations to be acknowledged for our study are its retrospective nature, based on a single-center experience, and consequently on a relatively small cohort. However, since our hospital is the referral center, our population covers the entire spectrum of IE in the region and is, therefore, representative of real-world experience. As discussed, criteria for repair are largely based on expert consensus and operative strategy has to be confirmed or changed after direct inspection by an expert surgeon, and no pre-specified criteria exist. This may limit the generalizability of our results to other centers and populations, but we all are aware that prospective studies would be useful but hardly feasible due to practical considerations.
Conclusions
Outcome of repair in IE guarantees a more favorable outcome than valve replacement and should be considered whenever possible in IE as in degenerative valve disease. Identifying patients who will benefit from surgery, operating them timely and following technically individualized surgical approach may decrease the mortality and morbidity of mitral valve IE.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- IE:
-
Infective endocarditis
- LVSF:
-
Left ventricular systolic function
- LVEF:
-
Left ventricular ejection fraction
- PISA:
-
Proximal Isovelocity hemispheric Surface Area
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
References
Hendren WG, Morris AS, Rosenkranz ER, Lytle BW, Taylor PC, Stewart WJ, Loop FD, Cosgrove DM Mitral valve repair for bacterial endocarditis. J Thorac Cardiovasc Surg 1992 103(1):124–128 discussion 128-129
Podesser BK, Rodler S, Hahn R, Eigenbauer E, Vodrážka M, Moritz A, Laufer G, Simon P, Wolner E (2000) Mid-term follow up of mitral valve reconstruction due to active infective endocarditis. J Heart Valve Dis 9(3):335–340
Feringa H, Shaw LJ, Poldermans D, Hoeks S, Van der Wall E, Dion R, Bax J (2007) Mitral valve repair and replacement in endocarditis: a systematic review of literature. Ann Thorac Surg 83(2):564–570
Ishikawa S, Kawasaki A, Neya K, Abe K, Suzuki H, Koizumi S, Shibuya H, Horikawa M, Ueda K (2009) Surgical treatments for infective endocarditis involving valve annulus. Ann Thorac Cardiovasc Surg 15(6):378–381
Huang XS, Xie JS, You B, Gu CX, Wang SY, Zhang JQ Clinical outcome of mitral valve repair in primary infective endocarditis with mitral insufficiency. Zhonghua Wai Ke Za Zhi 2009 47(16):1236–1238
Omoto T, Tedoriya T, Oi M, Nagai N, Miyauchi T, Ishikawa N (2011) Significance of mitral valve repair for active-phase infective endocarditis. Asian Cardiovasc Thorac Ann 19(2):149–153
Evans CF, Gammie JS (2011) Surgical management of mitral valve infective endocarditis. Semin Thorac Cardiovasc Surg 23(3):232–240
Chang HW, Kim KH, Hwang HY, Kim JS (2014) Role of mitral valve repair in infective endocarditis. J Heart Valve Dis 23(3):350–359
Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, Delgheru R, El Khoury G, Erba PA, Iung B, Miro JM, Mulder BJ, Plonska-Gosciniak B, Price S, Roos-Hesselink J, Snygg-Martin U, Thuny F, Mas PT, Vilacosta I, Zamorano JL (2015) ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC). Eur Heart J 36:3075–3128
Scheggi V, Alterini B, Olivotto I, Del Pace S, Zoppetti N, Tomberli B, Bartalesi F, Brandi L, Ceschia N, Andrei V, Suardi LR, Marchionni N, Stefàno PL. Embolic risk stratification and prognostic impact of early surgery in left-sided infective endocarditis. Eur J Intern Med. 2020;78:82–87
Zhao D, Zhang B (2014) Are valve repairs associated with better outcomes than replacements in patients with native active valve endocarditis? Interact Cardiovasc Thorac Surg 19(6):1036–1039
Mick SL, Keshavamurthy S, Gillinov M (2015) Mitral valve repair versus replacement. Ann Cardiothorac Surg 4(3):230–237
Rostagno C, Carone E, Stefàno PL (2017) Role of mitral valve repair in active infective endocarditis: long term results. J Cardiothorac Surg 12(1):29
Hu YN, Wan S (2018) Repair of infected mitral valves: what have we learned? Surg Today 48(10):899–908
Liu JZ, Li XF, Miao Q, Zhang CJ (2018) Surgical treatment of active native mitral infective endocarditis: a meta-analysis of current evidence. J Chin Med Assoc 81(2):147–154
Thitipong T, Chartaroon R, Apichat T, Noppon T, Surin W, Suphachai C, Weerachai N (2019) Comparison between mitral valve repair and replacement in active infective endocarditis. Gen Thorac Cardiovasc Surg 67(12):1030–1037
Solari S, De Kerchove L, Tamer S, Aphram G, Baert J, Borsellino S, Mastrobuoni S, Navarra E, Noirhomme P, Astarci P, Rubay J, El Khoury G (2019) Active infective mitral valve endocarditis: is a repair-oriented surgery safe and durable? Eur J Cardiothorac Surg 55(2):256–262
Harky A, Hof A, Garner M, Froghi S, Bashir M Mitral valve repair or replacement in native valve endocarditis? Systematic review and meta-analysis. J Card Surg 2018 33(7):364–371
Lee HA, Cheng YT, Wu VC, Chou AH, Chu PH, Tsai FC, Chen SW. Nationwide cohort study of mitral valve repair versus replacement for infective endocarditis. J Thorac Cardiovasc Surg. 2018 Oct;156(4):1473-1483.e2.
Okada Y, Nakai T, Muro T, Ito H, Shomura Y (2020) Mitral valve repair for infective endocarditis: Kobe experience. Asian Cardiovasc Thorac Ann 28:384
Defauw RJ, Tomšič A, van Brakel TJ, Marsan NA, Klautz RJM, Palmen M (2020) A structured approach to native mitral valve infective endocarditis: is repair better than replacement? Eur J Cardiothorac Surg 58(3):544–550
De Kerchove L, Price J, Tamer S, Glineur D, Momeni M, Noirhomme P, ElKhoury G (2012) Extending the scope of mitral valve repair in active endocarditis. J Thorac Cardiovasc Surg 143(4 Suppl):S91–S95
Toyoda N, Itagaki S, Egorova NN, Tannous H, Anyanwu AC, El-Eshmawi A, Adams DH, Chikwe J. Real-world outcomes of surgery for native mitral valve endocarditis. J Thorac Cardiovasc Surg. 2017 Dec;154(6):1906-1912.e9.
Acknowledgements
Not applicable
Funding
None to declare
Author information
Authors and Affiliations
Contributions
VS projected the study, analyzed and interpreted the data, and wrote the manuscript. NZ carried out the statistical analysis. PLS performed the surgical interventions and was a major contributor in writing the manuscript. NM and IO revised the final version of the manuscript. SDP and BA performed clinical follow-up and contributed to collecting the data for analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the local ethics committee (Comitato Etico Regionale per la Sperimentazione Clinica della Regione Toscana, Sezione: AREA VASTA CENTRO, n 12113_oss). Written informed consent was acquired in all patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Scheggi, V., Olivotto, I., Del Pace, S. et al. Feasibility and outcome of mitral valve repair in patients with infective endocarditis. Cardiothorac Surg 28, 27 (2020). https://doi.org/10.1186/s43057-020-00037-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43057-020-00037-w