
Abstract
Background
Montreal Cognitive Assessment test (MoCA) is a brief, sensitive test that has been recommended as a reliable tool to detect mild cognitive impairment. Associations between brain imaging measures and cognitive functioning have been observed in patients with multiple sclerosis (MS).
Objectives
To evaluate cognitive dysfunction and physical disability in MS patients by making correlation between magnetic resonance imaging (MRI), MoCA test, and Expanded Disability Status Scale (EDSS).
Methods
Fifty MS patients and 25 controls underwent clinical evaluation and assessment of cognitive functions using the MoCA test. In addition, all MS patients underwent conventional MRI brain and Expanded Disability Status Scale (EDSS).
Results
The scores for trail making test, memory, attention, serial seven subtractions, fluency, naming, and orientation in MS patients were significantly different from control (p < 0.05). There was significant inverse correlation between number of MS plaques in the temporal lobe and abstraction (p < 0.001, r = − 0.52). Less inverse correlation was found between total number of MRI plaques and concentration, total number of MRI plaques and abstraction, and infratentorial lesions and clock drawing test. No correlations were found between the number of MS plaques in frontal, parietal, occipital, corpus callosum, and neuropsychological tests.
Conclusion
Although conventional MRI techniques are crucial in the MS diagnostic workup, their accuracy in evaluating and predicting cognitive dysfunction is less relevant. The MoCA test would provide a brief screen for cognitive dysfunction in MS.
Similar content being viewed by others


Introduction
Multiple sclerosis (MS) has a variety of physical as well as cognitive signs and symptoms [1]. Cognitive dysfunction has a negative effect on social functions and quality of life with an important determinant of employment status and associated costs [2, 3].
Multiple sclerosis-associated cognitive impairment is a subcortical dementia subtype that affects mainly the speed of information processing [4]. In spite of the cognitive impairment in MS patients which has been correlated with both macro- and microscopic changes in brain anatomy, the pathogenesis of cognitive impairment in MS patient has not been fully understood [5].
Among the psychometric cognitive assessment that has been used commonly in research of MS, Montreal Cognitive Assessment test (MoCA) that has been recommended by the National Institute of Neurological Diseases and Stroke and Canadian Stroke Network (NINDS-CSN) was defined as a fast, reliable, accurate, and high-sensitivity test to detect mild cognitive impairment (MCI) and used as an alternative to the Mini-Mental Status Examination (MMSE) [6,7,8,9].
The effect of brain atrophy and lesion load was tested in different studies with different methodological assessment and variable results in MS patients [10,11,12,13,14,15].
The aim of this study was to test the relation between the clinical psychometric cognitive assessment and radiological finding by using conventional MRI brain and MoCA test in a cohort of MS patients. In addition, we used the Expanded Disability Status Scale (EDSS) to determine the physical disability in MS patients.
Subjects and methods
Subjects
This prospective, observational study was carried out during the period from May 2017 to June 2018 in the Neurology Department of Mansoura New General Hospital. The study included 50 MS patients and 25 age-, sex-, and education-matched healthy control subjects.
Inclusion criteria
-
1.
MS patients (relapsing–remitting “RR,” secondary progressive “SP,” and clinically isolated syndrome “CIS” according to “Revised Mc Donald criteria 2010” [16])
-
2.
Age ≥ 18 years
-
3.
No relapse for at least 3 months before the study
Exclusion criteria
-
1.
Primary progressive “PP” MS
-
2.
History of any neurological disorder other than MS
-
3.
Psychiatric disorder or other medical conditions that may affect the neuropsychological performance
-
4.
Any contraindication to MRI
Methods
Clinical evaluation
-
1.
Informed written consent was taken from all patients and control subjects
-
2.
History taking and complete neurological examination were done at the outpatient clinic at the Neurology Department of Mansoura New General Hospital
-
3.
All patients were diagnosed with MS according to “Revised McDonald criteria 2010” [16]
Assessment of cognitive functions
The MoCA was performed for all MS patients and control. The MoCA consists of 30 items divided into the domains of attention, language, memory, visuospatial, executive functions, and orientation. Score is a total of the points earned; an additional point was given for having 12 years or less of education. A score of 26 or above was considered normal [7].
Assessment of physical disability
Physical disability was determined using the Expanded Disability Status Scale (EDSS). The EDSS is used to describe disease progression in patient s with MS. It consists of an ordinal rating system ranging from zero (normal neurological status) to ten (death due to MS) [17].
MRI examintation
All patients underwent scanning with 1.5 T Siemens Magnetom Symphony Maestro Class, Syngo MR 2002B (Siemens Medical system Inc., Erlangen, Germany). T1-weighted (T1W), T2-weighted, and FLAIR image sets were acquired in the axial, sagittal, and coronal planes. The T1W sequence was TR, 500 ms; TE, 15 ms; matrix, 256 × 256 slices; slice thickness, 5 mm. The T2 sequence was TR, 3530 ms; TE, 81 and 70 ms; slice thickness, 5 mm. The FLAIR images were TR, 6000; TE, 140 ms; slice thickness, 5 mm.
To estimate the presence of MS plaques, we counted the number of plaques in different brain areas including frontal, parietal, temporal, and occipital lobes in addition to the corpus callosum and infratentorial plaques. Brain atrophy was determined using the qualitative method by recognition of an increase in cerebrospinal fluid spaces or a reduction in the size of parenchymal structures compared with the normal appearance for age [18].
Statistical analysis
The collected data were coded, processed, and analyzed using the SPSS (Statistical Package for Social Sciences) version 15 Windows (SPSS Inc., Chicago, IL, USA). Qualitative data was presented as number and percent. Comparison between groups was done by chi-square test. Quantitative data was presented as mean ± SD. Student’s t test was used to compare between the two groups. Non-parametric data was presented as min–max and median. Mann–Whitney test was used for comparison between groups. Spearman’s correlation coefficient was used to test the correlation between variables. p < 0.05 was considered to be statistically significant.
Results
Demographic results
Fifty MS patients and 25 normal control subjects participated in this study. The mean age of patients and control was 32.54 ± 6.64 and 29.88 ± 7.33, respectively (p = 0.11). Thirty-four of MS patients (68%) and 14 of the controls (56%) were women (p = 0.30). Thirty-one of patients (62%) had > 12 years of educations and 19 (38%) patients had < 12 years of educations while 12 (48%) of control group had > 12 years of educations and 13 (52%) had < 12 years of education (p = 0.24) (Table 1).
Clinical characteristics
According to the results of MoCA test, we classified our MS patients into two groups: cognitively abnormal group (32 patients “64%”, MoCA < 26) and cognitively normal group (18 patients“36%”, MoCA ≥ 26). The mean disease duration was 6.05 ± 4.08 years in cognitively abnormal group and 3.08 ± 2.83 years in the cognitively normal group. There were statistically significant differences between the two groups as regards the MS duration (p = 0.009).
Of the entire cognitively abnormal group, there were 27 (84.4%) relapsing–remitting (RR), four (12.5%) were secondary progressive (SP), and one (3.1%) with clinically isolated syndrome (CIS) whereas the cognitively normal group showed 13 (72.2%) with RR, 3 (16.7%) with SP, and 2 (11.1) with CIS. There were no statistically significant differences between the two groups as regards the MS phenotype (p = 0.45).
The most common presentation in the cognitively abnormal group was motor in 24 patients (75%), visual in 20 patients (62.5%), sensory in 17 patients (53.1%), cerebellar in 12 patients (37.5%), and speech in 6 patients (18.8%). The most common presentations in the cognitively normal group were sensory in 12 patients (66.7%), motor in 9 patients (50%), visual in 9 patients (50%), cerebellar in 3 patients (16.7%), and speech in 2 patients (11.1%). There were no statistically significant differences between the clinical presentations of both groups (p > 0.05).
The mean EDSS score was 4.36 ± 1.88 in the cognitively abnormal group and 2.81 ± 2.05 in the cognitively normal group. They were statistically significant differences between the EDSS of both groups (p = 0.009) (Table 2).
Montreal Cognitive Assessment test in MS and controls
MoCA test results of the patients and controls are shown in Table 3. The scores for trail making test, memory, attention, serial seven subtractions, fluency, naming, and orientation in MS patients were significantly different from control (p < 0.05). On the other hand, cube drawing, clock drawing, concentration, sentence repetition, and abstraction (similarities) showed non-significant differences between MS patients and control (p > 0.05).
MoCA test results of MS patients with normal and abnormal cognition showed a statistically significant correlation in all subtests (p < 0.05) except vigilance, concentration, and fluency (p > 0.05) Table 4.
MoCA test results of MS subtypes showed a statistically insignificant correlation in all subtests (p > 0.05) except digit span (sustained attention) which showed a highly statistically significant correlation (p = 0.001) Table 5.
MRI in cognitively normal and cognitively impaired patients
The presence of brain atrophy was more common in the cognitively abnormal group than in the cognitively normal group with statistically significant differences (p = 0.031). MS plaques in the temporal lobe were more common in the cognitively abnormal group than in the cognitively normal group with statistically significant differences (p = 0.048). Both the cognitively abnormal and cognitively normal groups showed no statistically significant differences regarding the total number of MS plaques as well as MS plaques in frontal, parietal, occipital, corpus callosum (CC), and infra-tentorial regions (p > 0.05) Table 6.
Correlation between MRI and the MoCA test
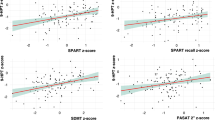
There was a significant inverse correlation between the number of MS plaques in the temporal lobe and abstraction (p < 0.001, r = − 0.52). Also, there were inverse correlations between the total number of MRI plaques and concentration (p = 0.048, r = − 0.28), total number of MRI plaques and abstraction (p = 0.005, r = − 0.38), and infra-tentorial lesions and clock drawing test (p = 0.001, r = − 0.44). No correlations were found between the number of MS plaques in frontal, parietal, occipital, and corpus callosum and the MoCA subtests (p > 0.05) (Table 7).
Discussion
MoCA is a well-established cognitive screen test. It is known to have discriminative power with high sensitivity and is widely validated for differentiating mild cognitive impairment from normal cognition and considered the short cognitive instrument of choice [19, 20].
The advantage of the MoCA over other cognitive screening measures is the breadth of cognitive domain coverage beyond memory, and it also detects individuals presenting with non-amnestic cognitive changes [21].
Many factors such as cognitive reserve, age, and level of education may have an effect on cognitive abilities and cause marked variability of cognitive impairment [22].
The aim of this study was to test the relation between the clinical psychometric cognitive assessment and radiological finding by using conventional MRI brain and MoCA test in a cohort of MS patients. In addition, we used the Expanded Disability Status Scale (EDSS) to determine the physical disability in MS patients.
In our study, 31 patients (62%) had > 12 years of educations and 19 patients (38%) had < 12 years of educations while 12 patients (48%) of control group had > 12 years of educations and 13 patients (52%) had < 12 years of education (p = 0.24).
In our work, 64% of MS patients were cognitively impaired and 36% were cognitively normal. This agreed with the study of Chiaravalloti and DeLuca as they found 40 to 70% of MS patients cognitively impaired [23] and disagreed with Guimaraes, who stated that overt dementia in MS patients was rare [24].
Our study showed longer disease duration in the cognitively impaired MS patients group than the disease duration in the non-cognitively impaired MS patients group (p = 0.009), and this matched with Achiron et al. [25] and Bagert et al. [26] who reported that the longer the duration of the disease, the more the progression of cognitive decline, and once cognitive impairment appears, it is unlikely to remit.
In our study, we concluded that cognitive impairment present in all MS phenotypes (RR, SP, and CIS) with no statistically significant differences (p > 0.05) except for digit span (sustained attention) which showed highly statistically significant correlation (p = 0.001). These findings were coping with Nocentini et al. [27], Portaccio et al. [28], and Khalil et al. [29], and they mentioned that cognitive dysfunction is often present in all MS subtypes and has been reported in the CIS.
In this study, when we compared the MS patients with the control group using the MoCA test, we found statistically significant differences in the digit span (p < 0.001), serial 7s (p < 0.001), delayed recall (p < 0.001), trail making test (p < 0.001), and fluency (p < 0.001). This is in agreement with several other studies; Sumowski et al. recognized deficits in episodic memory and processing speed as a debilitating symptom and prevalent of MS [30]. Rao et al. found that the MS patients were frequently impaired in recent memory, attention, and visuospatial functions [31]. Benedict et al. emphasized that the most affected domains in MS were verbal memory and executive function [32]. Deloire et al. observed differences between the MS patients and the control group as regards the memory, attention, and conceptualization [33].
In our study, we found that MS patients with cognitive impairment have a higher EDSS than MS patients with normal cognition with statistically significant differences between the EDSS of both groups (p = 0.009). This agreed with Ruano et al.; they found global cognitive impairment to be associated with higher EDSS in MS patients [34].
In our study, brain atrophy was more common in MS patients with abnormal cognition than MS patients with normal cognition with statistically significant differences (p = 0.031) This is in agreement with Camp et al.; they reported that cognitive impairment was correlated with total area/volume of MRI T2 lesions, cerebral volume, corpus callosum size, and third ventricle volume or width [35]. Benedict et al. concluded that ventricular enlargement (which is an index of brain atrophy) is associated with abnormalities on various cognitive tests [36]. Calabrese et al. showed a more severe cortical atrophy in RR–MS patients with cognitive impairment when compared with cognitively preserved patients [37]. According to Eijlers et al., brain atrophy is a predictor of cognitive decline in late relapsing–remitting and progressive MS [38].
Our study showed no statistically significant differences between the cognitively abnormal and cognitively normal MS patients as regards the lesion distribution in all the studied brain areas except temporal lobe. This is partially matching with Paul et al., as they did not detect differences in T1 and T2 lesion load between RRMS patients with or without cognitive impairment. These findings suggest that focal white matter lesions are not the sole feature influencing cognitive performance in MS and point to additional mechanisms such as damage to the normal-appearing white and gray matter [39].
Azevedo et al. [40], Nourbakhsh et al. [13], and Zivadinov et al. [41] reported that brain atrophy during MS course has become a well-recognized phenomenon. De Stefano et al. [42] and Fjell et al. [43] showed that brain atrophy has the strongest correlation with clinical disease progression, and increased atrophy over time is thought to predict worsening cognitive function and is known to occur in normal aging with an annual loss of brain volume of approximately 0.2–0.5%.
Vagberg et al. [44] reported that, in patients with MS, the atrophy rate is estimated to be 0.5–1.3% per year and appears commonly to be more prominent in patients with progressive MS than in those with RRMS. Other studies have shown that significant volume loss can already occur in patients with early RRMS and in patients with CIS [45, 46].
In our study, the total number of demyelinating plaques load showed no statistically significant differences between the cognitively abnormal and cognitively normal MS patients. Correlations between MRI findings and the neuropsychological assessment using MoCA test also showed no statistically significant differences except between number of MS plaques in the temporal lobe and abstraction (p < 0.001, r = − 0.52), total number of MRI plaques and concentration (p = 0.048, r = − 0.28), total number of MRI plaques and abstraction (p = 0.005, r = − 0.38), and infratentorial lesions and clock drawing test (p = 0.001, r = − 0.44). This agrees with several previous studies including Foong et al.; they did not find an association between frontal lesion load and impairment of executive skills [47]. Rossi et al. did not find an association between callosal lesions and the symbol digit modalities test [48]. Tiemann et al. did not find an association between the total lesion and seven neuropsychological variables [49]. Problems in abstract reasoning appear early in MS but may remain stable after many years. This type of cognitive impairment does not necessarily develop in parallel with other neurological deficits and may cause significant disturbances in everyday life [50].
Conclusions
Our study showed that the MoCA test would provide a brief screen for cognitive dysfunction in MS and is likely to be most useful in identifying those MS patients who may be at risk for cognitive impairment and warrant referral for full neuropsychological evaluation. Although conventional MRI techniques are crucial in the MS diagnostic workup, their accuracy in evaluating and predicting cognitive dysfunction is less relevant.
Availability of data and materials
The data supporting the results of this article are included within the article.
Abbreviations
- CC:
-
Corpus callosum
- CIS:
-
Clinically isolated syndrome
- EDSS:
-
Expanded Disability Status Scale
- MCI:
-
Mild cognitive impairment
- MMSE:
-
Mini-Mental Status Examination
- MoCA:
-
Montreal Cognitive Assessment test
- MS:
-
Multiple sclerosis
- NINSD-CSN:
-
National Institute of Neurological Diseases and Stroke and Canadian Stroke Network
- RR:
-
Relapsing–remitting
- SP:
-
Secondary progressive
- SPSS:
-
Statistical Package for Social Sciences
References
Uher T, Blahova-Dusankova J, Horakova D, et al. Longitudinal MRI and neuropsychological assessment of patients with clinically isolated syndrome. J Neurol. 2014;261:1735–44.
Blahova Dusankova J, Kalincik T, Dolezal T, et al. Cost of multiple sclerosis in the Czech Republic: the COMS study. Mult Scler. 2012;18:662–8.
Langdon DW. Cognition in multiple sclerosis. Curr Opin Neurol. 2011;24:244–9.
Cummings JL. Subcortical dementia. Neuropsychology, neuropsychiatry, and pathophysiology. Br J Psychiatry. 1986;149:682–97.
Morgen K, Sammer G, Courtney SM, Wolters T, Melchior H, Blecker CR, Oschmann P, Kaps M, Vaitl D. Evidence for a direct association between cortical atrophy and cognitive impairment in relapsing-remitting MS. Neuroimage. 2006;30:891.
Ashrafi F, Behnam B, Ahmadi MA, Taheri MS, Haghighatkhah HR, Pakdaman H, Kkarrazi AM. Correlation of MRI findings and cognitive funtion in multiple sclerosis patients using montereal cognitive assessment test. Med J Islam Repub Iran. 2016;30:357.
Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am GeriatrSoc. 2005;53:695–9.
Roalf DR, Moberg PJ, Xie SX, Wolk DA, Moelter ST, et al. Comparative accuracies of two common screening instruments for classification of Alzheimer's disease, mild cognitive impairment, and healthy aging. Alzheimers Dement. 2013;9:529–37.
Zadikoff C, Fox SH, Tang-Wai DF, Thomsen T, de Bie RM, et al. A comparison of the mini mental state exam to the Montreal cognitive assessment in identifying cognitive deficits in Parkinson's disease. MovDisord. 2008;23:297–9.
Benedict RH, Zivadinov R. Risk factors for and management of cognitive dysfunction in multiple sclerosis. Nat Rev Neurol. 2011;7:332–42.
Rocca MA, Amato MP, De Stefano N, et al. Clinical and imaging assessment of cognitive dysfunction in multiple sclerosis. Lancet Neurol. 2015;14:302–17.
Maghzi AH, Revirajan N, Julian LJ, et al. Magnetic resonance imaging correlates of clinical outcomes in early multiple sclerosis. Mult Scler Relat Disord. 2014;3:720–7.
Nourbakhsh B, Nunan-Saah J, Maghzi AH, et al. Longitudinal associations between MRI and cognitive changes in very early MS. Mult. Scler. Relat. Disord. 2016;5:47–52.
Hyncicova E, Vyhnalek M, Kalina A, et al. Cognitive impairment and structural brain changes in patients with clinically isolated syndrome at high risk for multiple sclerosis. J Neurol. 2017;264:482–93.
Mollison D, Sellar R, Bastin M, et al. The clinic-radiological paradox of cognitive function and MRI burden of white matter lesions in people with multiple sclerosis: a systematic review and meta-analysis. PLoS One. 2017;12:e0177727.
Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 2011;69:292–302.
Noseworthy JH, et al. Interrater variability with the Expanded Disability Status Scale (EDSS) and function systems (FS) in a multiple sclerosis trial. Neurology. 1990;110:971-5.
Bakshi R, Benedict RH, Bermel RA, Jacobs L. Regional brain atrophy is associated with physical disability in multiple sclerosis: Semiquantitative magnetic resonance imaging and relationship to clinical findings. J Neuroimaging. 2001;11:129–36.
Kang JM, Cho Y, Park S, Lee BH, Sohn BK, Choi CH, Choi J, Jeong HY, Cho S, Lee JH, Lee J, et al. Montreal cognitive assessment reflects cognitive reserve. MBC Geriatr. 2018:18-261. https://doi.org/10.1168/s12877-0951-8.
Damian A, Jacobsen S, Hentz J, Belden C, Shill H, Sabbagh M, Caviness J, Adler C. The Montreal Cognitive Assessment and the mini-mental state examination as screening instruments for cognitive impairment: item analyses and threshold scores. Dement Geriatr Cogn Disord. 2011;31:126–31.
Vogel SJ, Banks SJ, Cummings JL, Miller JB. Concordance of the Montreal cognitive assessment with standard neuropsychological measures. Alzheimer’s Dementia: Diagn Assess Dis Monit. 2015;1:289–94.
Horakova D, Kalincik T, Blahova Dusankova J, Dolezal O. Clinical correlates of grey matter pathology in multiple sclerosis. BMC Neurol. 2012;12:10.
Chiaravalloti ND, DeLuca J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008;7:1139–51.
Guimaraes J, SA MJ. Cognitive dysfunction in multiple sclerosis. Front Neurol. 2012;3:74.
Achiron A, Polliack M, Rao SM, et al. Cognitive patterns and progression in multiple sclerosis: construction and validation of percentile curves. J Neurol Neurosurg Psychiatry. 2005;76:744–9.
Bagert B, Camplair P, Bourdette D. Cognitive dysfunction in multiple sclerosis: natural history, pathophysiology and management. CNS Drugs. 2002;16:445–55.
Nocentini U, Pasqualetti P, Bonavita S, Bucafusca M, De Caro MF, Farina D. Et al. Cognitive dysfunction in patients with relapsing-remitting multiple sclerosis. Mult Scler 2006; 12:77–87.
Portaccio E, Stromillo ML, Goretti B, et al. Neuropsychological and MRI measures predict short-term evolution in benign multiple sclerosis. Neurology. 2009;73:498–503.
Khalil M, Enzinger C, Langkammer C. Cognitive impairment in relation to MRI metrics in patients with clinically isolated syndrome. Mult Sclera. 2011;17:173–80.
Sumowski JF, Benedict R, Enzinger C, Filippi M, et al. Cognition in multiple sclerosis: state of the field and priorities for the future. Neurology. 2018;90:278–88.
Rao SM, Leo GJ, Bernardin L, Unverzagt F. Cognitive dysfunction in multiple sclerosis: I: frequency, patterns, and prediction. Neurology. 1991;41:685–91.
Benedict RH, Cookfair D, Gavett R, et al. Validity of the minimal assessment of cognitive function in multiple sclerosis (MACFIMS). J Int Neuropsychol Soc. 2006;12:549–58.
Deloire MS, Ruet A, Hamel D, Bonnet M, Dousset V, Brochet B, et al. MRI predictors of cognitive outcome in early multiple sclerosis. Neurology. 2011;76(13):1161–7.
Lynch SG, Parmenter BA, Denney DR. The association between cognitive impairment and physical disability in multiple sclerosis. Mult Scler. 2005;11:469–76.
Camp SJ, Stevenson VL, Thompson AJ, et al. Cognitive function in primary progressive and traditional progressive multiple sclerosis: controlled study with MRI correlates. Brain. 1999;122:1341–8.
Benedict RH, Carone DA, Bakshi R. Correlating brain atrophy with cognitive dysfunction, mood disturbances, and personality disorder in multiple sclerosis. J Neuroimaging. 2004;14(3 Suppl):S36–45.
Calabrese M, Agosta F, Rinaldi F, et al. Cortical lesions and atrophy associated with cognitive impairment in relapsing-remitting multiple sclerosis. Arch Neurol. 2009;66(9):1144–50.
Eijlers AJC, Van Geest Q, Dekker I, Steenwijk MD, Meijer KA, Hulst HE, Barkhof F, Uitdehaag BM, Schoonheim MM, Geurts J, et al. Predicting cognitive decline in multiple sclerosis: a 5- year follow-up study. Brain. 2018;141(9):2605–18.
Paul F. Pathology and MRI: exploring cognitive impairment in MS. Acta Neurol Scand. 2016;134 (Suppl. 200:24–33.
Azevedo CJ, Pelletier D. Whole-brain atrophy: ready for implementation into clinical decision-making in multiple sclerosis? Curr Opin Neurol. 2016;29:237–42.
Bermel RA, Bakshi R. The measurement and clinical relevance of brain atrophy in multiple sclerosis. Lancet Neurol. 2006;5(2):158–70.
De Stefano N, Stromillo ML, Giorgio A, et al. Establishing pathological cut-offs of brain atrophy rates in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2016;87:93–9.
Fjell AM, Walhovd KB, Fennema-Notestine C, et al. One-year brain atrophy evident in healthy aging. J Neurosci. 2009;29:15223–31.
Vagberg M, Lindqvist T, Ambarki K, et al. Automated determination of brain parenchymal fraction in multiple sclerosis. AJNR Am J Neuroradiol. 2013;34:498–504.
De Stefano N, Iannucci G, Sormani MP, et al. MR correlates of cerebral atrophy in patients with multiple sclerosis. J Neurol. 2002;249:1072–7.
Dalton CM, Brex PA, Jenkins R, et al. Progressive ventricular enlargement in patients with clinically isolated syndromes is associated with the early development of multiple sclerosis. J Neurol Neurosurg Psychiatry. 2002;73:141–7.
Foong J, Rozewicz L, Quaghebeur G, et al. Executive function in multiple sclerosis. The role of frontal lobe pathology. Brain. 1997;120:15–26.
Rossi F, Giorgio A, Battglini M, et al. Relevance of brain lesion location to cognition in relapsing multile sclerosis. PLoS One. 2012;7:e44826.
Tiemann L, Penner IK, Haupts M, Schlegel U, Calabrese P. Cognitive decline in multiple sclerosis impact of topographic lesion distribution on differential cognitive deficit patterns. Mult Scler. 2009;15:1164–74.
Amato MP, Ponziani G, Pracucci G, et al. Cognitive impairment in early-onset multiple sclerosis: pattern, predictors, and impact on everyday life in a 4-year follow-up. Arch Neurol. 1995;52:168–72.
Acknowledgements
The authors are grateful to all patients and control subjects for their willingness to participate in this study.
Funding
There is no source of funding for the research.
Author information
Authors and Affiliations
Contributions
AAM, MEF, and CAZ carried out the work. AAM designed the study and collected the patients and gathered the clinical data. MEF did the statistical analysis. MEF was responsible for collecting the scientific data and writing of the initial draft of the manuscript. CAZ collected and reported the radiological data of all patients MRI. All authors read and approved the final version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The authors obtained permission to conduct this study from the Institutional Review Board, Mansoura Faculty of Medicine, Mansoura University (code-Number: R/18.11.332) on December 2018. An informed consent was obtained from all the patients studied.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Abou Elmaaty, A.A., Flifel, M.E. & Zarad, C.A. Correlation between brain magnetic resonance imaging, cognitive dysfunction and physical dysability in multiple sclerosis. Egypt J Neurol Psychiatry Neurosurg 55, 54 (2019). https://doi.org/10.1186/s41983-019-0100-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-019-0100-0