
Abstract
Background
3D printing (3DP) has gained interest in many fields of medicine including cardiology, plastic surgery, and urology due to its versatility, convenience, and low cost. However, critical care medicine, which is abundant with high acuity yet infrequent procedures, has not embraced 3DP as much as others. The discrepancy between the possible training or therapeutic uses of 3DP in critical care and what is currently utilized in other fields needs to be addressed.
Objective
This narrative literature review describes the uses of 3DP in critical care that have been documented. It also discusses possible future directions based on recent technological advances.
Methods
A literature search on PubMed was performed using keywords and Mesh terms for 3DP, critical care, and critical care skills.
Results
Our search found that 3DP use in critical care fell under the major categories of medical education (23 papers), patient care (4 papers) and clinical equipment modification (4 papers). Medical education showed the use of 3DP in bronchoscopy, congenital heart disease, cricothyroidotomy, and medical imaging. On the other hand, patient care papers discussed 3DP use in wound care, personalized splints, and patient monitoring. Clinical equipment modification papers reported the use of 3DP to modify stethoscopes and laryngoscopes to improve their performance. Notably, we found that only 13 of the 31 papers were directly produced or studied by critical care physicians.
Conclusion
The papers discussed provide examples of the possible utilities of 3DP in critical care. The relative scarcity of papers produced by critical care physicians may indicate barriers to 3DP implementation. However, technological advances such as point-of-care 3DP tools and the increased demand for 3DP during the recent COVID-19 pandemic may change 3DP implementation across the critical care field.
Similar content being viewed by others


Introduction
The advantages of the use of 3-Dimensionl printing (3DP) technology in the medical field are numerous [1, 2]. The capability of 3DP technology to create high fidelity products has proved to be an asset in the production of patient specific models and prostheses (e.g. congenital heart disease models based on a patient’s radiological data) [3]. Moreover, the digital design of 3D models can be easily altered to fit its intended use by utilizing widely available software [4,5,6]. Its high output speed and affordability of materials enables 3DP to meet high demands during shortages. For instance, it was able to supply many healthcare institutions with the protective equipment they needed during the COVID-19 pandemic [7]. Over the past few decades, many medical subspecialties began using 3DP for a variety of purposes. For example, cardiac surgeons began using computed tomography scans to create 3DP models of patients’ hearts to help with surgical planning [8]. This widespread use of 3DP in medicine has become prevalent enough to create special interest groups to devise appropriateness criteria of 3DP utilization in clinical settings. Through these criteria, 3DP implementation in medicine can become better regulated and therefore more established [3].
Nevertheless, despite the aforementioned uses and advantages, 3DP technology has not been as heavily implemented in the field of critical care. This is noteworthy since critical care has many areas where 3DP could be applied. One such area is simulation training. Simulation has been shown by multiple studies to be at least as efficient as standard lectures and visual aids [9, 10]. Likewise, it has been shown that the “See One, Do One, Teach One” approach to medical education should be replaced by a model emphasizing constant practice in order to achieve a high level of competency [11]. In the critical care field, procedural competence is often hindered by the virtue of its many risky yet infrequent procedures (e.g. cricothyroidotomy). These procedures, while relatively infrequent, carry higher risk for patients if done inappropriately. Therefore, simulation models would help increase the physician’s comfort with the procedure without causing any harm to patients. However, many commercially available simulators are either expensive or depend on animal substitutes (which present additional storage and procurement issues). Simulation using 3DP models can evade these issues due to their lower cost and ease of production [12]. Manufacturing of tools and equipment can also improve through 3DP implementation. This is especially important in low resource settings where acquiring medical equipment may be economically or logistically challenging. 3DP can also be used to educate patients, staff, or caregivers [13, 14].
We conducted a literature review to summarize the current education and therapeutic uses of 3DP for critical care procedures or within critical care settings.
Methodology
The literature was collected by performing a comprehensive search of the PubMed database for all articles from inception until July 30th, 2019 containing the keywords used in literature to represent 3DP (e.g., 3D printing, three-dimensional print, additive manufacturing), and those used to represent critical care (e.g. critical care, emergency medicine, intensive care unit). The scarcity of the results led to the modification of the search strategy to include keywords representing the repertoire of skills of a critical care physician (Additional file 1). This modification was performed to include articles pertaining to the field of critical care but not necessarily by critical care physicians. With the assistance of a health sciences research librarian, terms and mesh categories for 3DP, critical care and skills required of a critical care physician were combined to create our search strategy (Additional file 1).
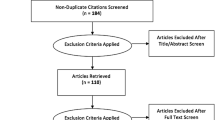
The search contributed 5846 results which were transported into Covidence (Veritas Health Innovation, Melbourne, Australia). The program found no duplicates. Papers were screened by title and abstract and disqualified if they had non-human subjects, implementations were not pertinent to critical care, or reviews. This created a list of 87 papers which were further reviewed for their applicability to the field of critical care by two critical care physicians (authors A.P. and J.G.). This left 35 papers which underwent full-text screening (Fig. 1). The papers were additionally examined for the degree of involvement of critical care in their production. Involvement in this study was defined as critical care physicians being part of the research team or research participants. Finally, the methodologies of the papers were divided into randomized control trials (RCT), technical reports, and quasi-experiments. Quasi-experiments were defined as studies that aim to demonstrate a causal relationship by introducing an intervention and control groups but without randomization [15].

Prisma flow diagram of the number of papers found at each stage of the study
Results
Our search produced 31 papers that described possible uses of 3DP in critical care which can be divided into three main themes: Medical education (Med-Ed), patient care, and clinical equipment modification (CEM) (Table 1). Topics under Med-Ed included: bronchoscopy (9 studies), congenital heart disease (CHD) (4 studies), cricothyroidotomy (3 studies), and medical imaging (3 studies). Some single study utilities within medical education involved: thoracotomy, chest tube insertion, epistaxis management, and pediatric intubation. Studies within the patient care category included wound care (1 study), personalized splints (2 studies), and patient monitoring (1 study). CEM involved a 3DP stethoscope (1 study) and laryngoscope adjustments (3 studies). The characteristics of the papers can be found in Table 2.
Med-Ed papers accounted for 74% of the studies found. Bronchoscopy was the most common topic with 39% of Med-Ed papers, followed by CHD at 17.4%. Med-Ed papers were mostly technical reports and quasi-experiments with only 21.7% of the studies containing RCTs. On the other hand, 65.2% and 52.2% of the Med-Ed papers included a technical report or quasi experiment, respectively.
Patient care papers comprised 17.4% of the total number of papers with half focusing on personalized splints. Moreover, patient care was the only topic that included a case study while the other three papers were either technical reports or quasi-experiments. CEM papers also made 17.4% of the total number of papers found; however, CEM was mostly comprised of laryngoscope modification projects (75%). All CEM papers included a technical report with only one using an RCT.
Comparing the involvement of critical care medicine in the papers, we found that only 13 of the papers had critical care contribution. Moreover, 12 papers were within Med-Ed while patient care and CEM having 0 and 1, respectively (Fig. 2).

Number of studies involving critical care within the major utilities of 3DP in critical care
Discussion
Results interpretation
This review shows that 3DP can have a variety of utilities in the field of critical care including medical education, patient care, and development of clinical equipment; however, Med-Ed takes the lead as the most common utility of 3DP with over 70% of the papers found discussing the use of 3DP models to train medical students and/or residents. This high percentage can be explained by the key findings of the papers. First, 3DP’s ability to create simulation models for numerous parts of the body including airways, shoulder girdle, and nasal cavity provides the opportunity to practice a large variety of skills. Such skills may be difficult to practice on real-life patients due to their high acuity and infrequency (e.g. cricothyroidotomy) [16,17,18,19,20,21,22, 32, 38]. Therefore, obtaining a model that can be used for frequent practice can be essential and life conserving [12]. Many of the studies showed that 3DP models were anatomically accurate and matched if not surpassed conventional models in their realism and student preference [18,19,20, 23, 28,29,30,31,32]. Moreover, the simulators were able to assess the difference in the proficiency between novices and experts by showing a clear correlation between the scores of the users and the number of years of experience [24]. This ability to discern between novices and experts enables the 3DP models to be used for assessing the competency of students as they progress in their training. In addition, the ability to help novice practitioners match experts after practicing on the simulator allows 3DP models to be useful training modules [22]. Another advantage of 3DP models is their ability to educate the user on both normal and variant/abnormal anatomy. For instance, 3DP models of congenital heart defects have been successfully used to increase the knowledge of participants of the anatomical issues and their consequences [25,26,27,28]. Normal anatomical variants have also been incorporated in many simulation models [17, 34].
Interestingly, the study by White and colleagues found that the 3DP group scored higher on the Tetralogy of Fallot test while the didactic class group scored better on the ventricular septal defect (VSD) test [28]. According to the authors, while VSD is simple enough to be learned through didactic learning, Tetralogy of Fallot is a complex case in which the tactile component may be advantageous to understanding the intricate anatomy. That is why the 3DP group were able to do better on that test than the classroom group. Therefore, for the optimum use of 3DP models in training, they should be used where a mix of visual and tactile information is beneficial.
Another noteworthy observation was that none of the papers we found discussed 3DP in critical care for adult cardiac disease. Although 3DP in cardiac medicine is a well-established field of research with various reviews [8, 47], 3DP utilization in adult cases mainly revolve around defect visualization, procedural planning, and surgical device innovation [47]. The scarcity of medical education utilities in adult cardiology is represented by both our results and those reported by Vukicevic and colleagues in their review of 3DP uses in cardiac medicine [47]. Considering the positive results of 3DP utilization in CHD for educating critical care physicians, similar training modules for the management of adult cases in cardiac intensive care units may prove beneficial.
The papers found under the categories of patient care and CEM represent the innovations possible through 3DP’s versatility. For example, the ability to create filaments of different characteristics allows for the production of more complex products. This was shown in the use of multiple materials to simulate the different tissue densities common to human structures [16, 33, 37, 38]. Furthermore, specially designed materials can be created for a particular utility. For instance, Muwaffak and colleagues were able to create specialized filaments containing silver, zinc, and copper and combine them into a personalized wound dressing that boasted the antimicrobial abilities of these metals [39]. Another source of versatility is the ability create 3DP molds of the desired structures. Using the sometimes-limited material properties offered by most 3DP technologies, 3DP molds can be used to shape silicon or gelatin to create anatomic structures that possess properties (e.g. mechanical) that more closely resemble tissue [20, 32]. 3DP molds were used with silicon in Risler and colleagues’ research to create the outer shoulder shell that provided feedback under ultrasound (US) that resembled human tissue [32]. 3DP versatility has also increased through personalization of therapeutic devices, such as splints to fit specifically to each patient. 3DP of personalized splints such as those described in Li et al. and Wu P-K et al. are made possible by hand-held 3D scanners that can capture the person’s exact measures within seconds, and which can then be used to custom-design the splint to fit the measured anatomy [40, 41].
Overall, 8 of the 31 studies specifically discussed that their 3DP models were either cheaper or of similar price to conventional models [16, 17, 31, 34, 35, 37, 38, 41]. This decrease in price can reach up to 250% which provides a strong motive for furthering the implementation of 3DP technology in critical care [17]. The expiration of the patent for various printers and the wide-spread availability of material has caused this decrease in cost and the increased availability of 3DP [48].
Despite the various advantages to 3DP implementation in critical care, only 13 of the 31 papers involved critical care physicians as authors or participants. This could be due to a variety of reasons from 3DP illiteracy, to lack of knowledge of possible implementations, to the fact that many 3D printed models are developed by surgeons or non-clinical researchers where the applications are more widespread. Another possible cause may be due to many physicians believing that the urgency of most critical care cases decreases the time available for designing and printing instruments. The relative difference in critical care papers found between the three topics supports this theory with 52% of Med-Ed papers involving critical care versus 25% and 0% in CEM and patient care respectively. This higher involvement in Med-Ed could be explained by the fact that education usually occurs in less urgent settings. However, with innovations such as 3DP wound dressings that can be made beforehand, printers that can produce splints in only a few hours, and the shortage of supplies mitigated by 3DP during the COVID-19 pandemic, we hope to see an increase in 3DP implementation in critical care tools and patient care [39, 40].
Strengths and limitations
Our search strategy was expanded by searching for the use of 3DP in skills pertaining to critical care. This allowed us to capture and describe results from both current and possible implementations of 3DP in critical care. Moreover, we have presented the details and key findings of each study (Table 2) which can help guide future research. Many of the papers discussed were technical reports of models and hence can be developed and researched further. Additionally, our results were supported by the findings of other larger reviews [1, 49, 50].
Nonetheless, there are a few limitations to this review. First, our results are restricted to the papers found on the PubMed database. Moreover, since our search was conducted before the COVID-19 pandemic, additional uses of 3DP may have emerged to battle instrument shortage. Nevertheless, we believe that any extra papers would still fall under the major topics of Med-Ed, patient care, and CEM. Another limitation is the low number of papers found in both CEM and patient care. Furthermore, many of the papers found did not test the clinical significance of their innovations. However, the positive results from every quasi-experiment and RCT reported here supports the hypothesis that uses of 3DP are clinically significant. Further research guided by our description of the benefits of 3DP in critical care will also help mitigate some of the issues caused by the low number of results found.
Future directions
With 3DP technology continuously improving, we expect a rise of new initiatives in the field of critical care. For instance, the ability of 3DP models to serve as simulation training modules for novice physicians will be crucial as the medical field begins its transition to competency-based learning. The versatility of 3DP raw materials makes it possible to create simulation models that cover an array of competencies and skills. For instance, researchers have been able to create high quality 3DP phantoms using different materials to resemble the physical characteristics of the distinctive tissue types [51]. These phantoms can be used to train novice critical care physicians on their imaging diagnostic skills as well as imaging-guided procedures [32, 33]. Nevertheless, further collaboration with 3DP companies is needed in the future to improve the fidelity of these phantoms through specially designed raw materials to more accurately depict the characteristics of human tissue [51]. With the continued development of 3DP simulation models, the authors hope that an open-source library with the printing files of the models can be made available so that physicians in resource-scarce regions can still maintain their training.
Furthermore, the tools used in critical care can benefit from the enhancements possible through 3DP. For example, biochemical research papers [52] have designed 3D printed materials that could be used to enhance wound healing. This ability can be applied to wound dressing manufacturing and tested in a critical care setting to determine the advantages they provide over commercially available dressings.
Another field in 3DP research that has been gaining attention is point-of-care testing (POCT). POCT is the field of diagnostic testing that can be done in real time generally outside of a laboratory and by untrained individuals [53]. This field has become essential for diagnosis both in the developing world and rural or resource scarce areas in the developed world [54]. Therefore, future research into 3DP POCT projects like ABO blood typing and wireless monitoring of key metabolites may be readily utilized in critical care settings [53, 55, 56].
The future implementation of 3DP in critical care has been affected greatly by the COVID-19 pandemic. The shortage of personal protective equipment and ventilation valves has supported the need for 3DP’s quick turnover and production rate [57]. Indeed, many research endeavours have utilized 3DP to overcome the scarcity of resources that faced many hospitals. For example, Callahan and colleagues were able to use 3DP to create nasal swabs that were comparable to the commercial ones [58]. Other uses of 3DP included production of face shields, N95 masks, ventilator valves, and environmental protection (ex. Hands-free door handles) [59, 60]. The pandemic was able to uncover the limitation of many of our hospitals when they were cut off their suppliers and faced shortage of necessary tools and equipments. However, this can be prevented in the future through two important steps. First, advocating for the development of 3DP labs within hospitals and the training of staff on the protocol for employment of 3DP tools during emergent situations may mitigate some of the effects of supply shortage. Moreover, the creation of a central depository for medical 3DP designs may help increase the access of hospitals to readily available products. Such a depository can also increase the number of trials a product undergoes which can hasten their development and improvement.
Conclusion
This narrative review has summarized the major uses of 3DP in the field of critical care which were found to be mainly within the realms of medical education (e.g. simulation models and training modules), patient care (e.g. wound care and personalized splints), and clinical equipment modification (e.g. 3DP laryngoscope handle). Moreover, our search found that most of the research endeavours, while discussing 3DP utilities applicable to the field of critical care, were not performed by critical care medicine. This fact represents the need for critical care-specific studies that consider the needs of the field and how 3DP can fulfill them. Finally, we looked at how some of the new innovations in 3DP like biochemically active 3DP raw material may be beneficial for the future of critical care. With these various advantages of 3DP and the clear demand for its role in a plethora of aspects of critical care, we expect to witness a greater involvement of critical care physicians in this field in the near future.
Availability of data and materials
Not Applicable.
Abbreviations
- 3DP:
-
Three-dimensional printing
- Med-Ed:
-
Medical Education
- MRI:
-
Magnetic resonance imaging
- CEM:
-
Clinical Equipment Modification
- CHD:
-
Congenital heart disease
- US:
-
Ultrasound
- RCT:
-
Randomized Control Trial
- VSD:
-
Ventricular septum defect
References
Mitsouras D, Liacouras P, Imanzadeh A, Giannopoulos AA, Cai T, Kumamaru KK, George E, Wake N, Caterson EJ, Pomahac B, Ho VB, Grant GT, Rybicki FJ. Medical 3D printing for the radiologist. Radiographics. 2015;35:1965–88.
Mitsouras D, Liacouras PC, Wake N, Rybicki FJ. RadioGraphics update: medical 3D printing for the radiologist. Radiographics. 2020;40(4):E21–3.
Chepelev L, Wake N, Ryan J, Althobaity W, Gupta A, Arribas E, Santiago L, Ballard DH, Wang KC, Weadock W, Ionita CN, Mitsouras D, Morris J, Matsumoto J, Christensen A, Liacouras P, Rybicki FJ, Sheikh A, RSNA Special Interest Group for 3D Printing. Radiological Society of North America (RSNA) 3D printing Special Interest Group (SIG): guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Print Med. 2018;4:11.
Giannopoulos AA, Chepelev L, Sheikh A, Wang A, Dang W, Akyuz E, Hong C, Wake N, Pietila P, Dydynski PB, Mitsouras D, Rybicki FJ. 3D printed ventricular septal defect patch: a primer for the 2015 Radiological Society of North America (RSNA) hands-on course in 3D printing. 3D Print Med. 2015;1:3.
Chepelev L, Hodgdon T, Gupta A, Wang A, Torres C, Krishna S, Akyuz E, Mitsouras D, Sheikh A, et al. 3D Print Med. 2016;2:5.
Chepelev L, Souza C, Althobaity W, Miguel O, Krishna S, Akyuz E, Hodgdon T, Torres C, Wake N, Alexander A, George E, Tang A, Liacouras P, Matsumoto J, Morris J, Christensen A, Mitsouras D, Rybicki F, Sheik A. Preoperative planning and tracheal stent design in thoracic surgery: a primer for the 2017 Radiological Society of North America (RSNA) hands-on course in 3D printing. 3D Print Med. 2017;3:14.
Swennen GR, Pottel L, Haers PE. Custom-made 3D-printed face masks in case of pandemic crisis situations with a lack of commercially available FFP2/3 masks. Int J Oral Maxillofac Surg. 2020;49:673–7.
Milano EG, Capelli C, Wray J, Biffi B, Layton S, Lee M, et al. Current and future applications of 3D printing in congenital cardiology and cardiac surgery. Br J Radiol. 2019;92:2018059.
Wang CL, Schopp JG, Petscavage JM, Paladin AM, Richardson ML, Bush WH. Prospective randomized comparison of standard didactic lecture versus high-Fidelity simulation for radiology resident contrast reaction management training. Am J Roentgenol. 2011;196:1288–95.
Daniels K, Arafeh J, Clark A, Waller S, Druzin M, Chueh J. Prospective randomized trial of simulation versus didactic teaching for obstetrical emergencies. Simulation Healthcare. 2010;5:40–5.
Vozenilek J. See one, do one, teach one: advanced Technology in Medical Education. Acad Emerg Med. 2004;11:1149–54.
Karakuş A, Duran L, Yavuz Y, Altintop L, Çalişkan F. Computer-based simulation training in emergency medicine designed in the light of malpractice cases. BMC Medical Education. 2014;14:155.
Loke Y-H, Harahsheh AS, Krieger A, Olivieri LJ. Usage of 3D models of tetralogy of Fallot for medical education: impact on learning congenital heart disease. BMC Medical Education. 2017;17.
Bernhard J-C, Isotani S, Matsugasumi T, Duddalwar V, Hung AJ, Suer E, et al. Personalized 3D printed model of kidney and tumor anatomy: a useful tool for patient education. World J Urol. 2015;34:337–45.
Harris AD, Mcgregor JC, Perencevich EN, Furuno JP, Zhu J, Peterson DE, et al. The use and interpretation of quasi-experimental studies in medical informatics. J Am Med Inform Assoc. 2006;13:16–23.
Ho BHK, Chen CJ, Tan GJS, Yeong WY, Tan HKJ, Lim AYH, et al. Multi-material three dimensional printed models for simulation of bronchoscopy. BMC Medical Education. 2019;19:236.
Bustamante S, Bose S, Bishop P, Klatte R, Norris F. Novel application of rapid prototyping for simulation of Bronchoscopic anatomy. J Cardiothorac Vasc Anesth. 2014;28:1122–5.
Al-Ramahi J, Luo H, Fang R, Chou A, Jiang J, Kille T. Development of an innovative 3D printed rigid bronchoscopy training model. Annals of Otology, Rhinology & Laryngology. 2016;125:965–9.
Hornung A, Kumpf M, Baden W, Tsiflikas I, Hofbeck M, Sieverding L. Realistic 3D-printed tracheobronchial tree model from a 1-year-old girl for pediatric bronchoscopy training. Respiration. 2017;93:293–5.
Deboer EM, Wagner J, Kroehl ME, Albietz J, Shandas R, Deterding RR, et al. Three-dimensional printed pediatric airway model improves novice Learnersʼ flexible bronchoscopy skills with minimal direct teaching from faculty. Simulation Healthcare. 2018;13:284–8.
Parotto M, Jiansen JQ, Abotaiban A, Ioukhova S, Agzamov A, Cooper R, et al. Evaluation of a low-cost, 3D-printed model for bronchoscopy training. Anestezjologia Intensywna Terapia. 2017;49:189–97.
Ghazy A, Vahl C, Dorweiler B. Development and evaluation of 3D-printed models of human tracheobronchial system for training in flexible bronchoscopy. Thorac Cardiovasc Surg. 2017;65:137–43.
Pedersen TH, Gysin J, Wegmann A, Osswald M, Ott SR, Theiler L, et al. A randomised, controlled trial evaluating a low cost, 3D-printed bronchoscopy simulator. Anaesthesia. 2017;72:1005–9.
Steinfort DP, Yong YH, Byrne T, Gorelik A, Colt H, Irving LB. Assessment of Bronchoscopic Dexterity and Procedural Competency in a Low-fidelity Simulation Model. J Bronchol Interventional Pulmonol. 2018;1:198–203.
Costello JP, Olivieri LJ, Su L, Krieger A, Alfares F, Thabit O, et al. Incorporating three-dimensional printing into a simulation-based congenital heart disease and critical care training curriculum for resident physicians. Congenit Heart Dis. 2014;10:185–90.
Olivieri LJ, Su L, Hynes CF, Krieger A, Alfares FA, Ramakrishnan K, et al. “Just-in-time” simulation training using 3-D printed cardiac models after congenital cardiac surgery. World J Pediatric Congenital Heart Surg. 2016;7:164–8.
Olivieri LJ, Zurakowski D, Ramakrishnan K, Su L, Alfares FA, Irwin MR, et al. Novel, 3D display of heart models in the postoperative care setting improves CICU caregiver confidence. World J Pediatric Congenital Heart Surg. 2018;9:206–13.
White SC, Sedler J, Jones TW, Seckeler M. Utility of three-dimensional models in resident education on simple and complex intracardiac congenital heart defects. Congenit Heart Dis. 2018;13:1045–9.
Doucet G, Ryan S, Bartellas M, Parsons M, Dubrowski A, Renouf T. Modelling and manufacturing of a 3D printed trachea for Cricothyroidotomy simulation. Cureus. 2017;9:e1575.
Hughes KE, Biffar D, Ahanonu EO, Cahir TM, Hamilton A, Sakles JC. Evaluation of an Innovative Bleeding Cricothyrotomy Model. Cureus. 2018;10(9):e3327.
Katayama A, Nakazawa H, Tokumine J, Lefor AK, Watanabe K, Asao T, et al. A high-fidelity simulator for needle cricothyroidotomy training is not associated with increased proficiency compared with conventional simulators. Medicine. 2019;98.
Risler Z, Magee MA, Mazza JM, Goodsell K, Au AK, Lewiss RE, et al. A Three-dimensional Printed Low-cost Anterior Shoulder Dislocation Model for Ultrasound-guided Injection Training. Cureus. 2018;10(11):e3536.
Javan R, Cho AL. An assembled prototype multimaterial three-dimensional–printed model of the neck for computed tomography– and ultrasound-guided interventional procedures. J Comput Assist Tomogr. 2017;41:941–8.
O’Reilly MK, Reese S, Herlihy T, Geoghegan T, Cantwell CP, Feeney RN, et al. Fabrication and assessment of 3D printed anatomical models of the lower limb for anatomical teaching and femoral vessel access training in medicine. Anat Sci Educ. 2015;9:71–9.
Yates E, Chirurgi R, Adamakos F, Habal R, Jaiswal R, Kalantari H, et al. Development and utilization of 3D printed material for thoracotomy simulation. Emergency Medicine International. 2018;2018:1–8.
Bettega AL, Brunello LFS, Nazar GA, Yuji G, De-Luca E, Sarquis LM, et al. Chest tube simulator: development of low-cost model for training of physicians and medical students. Rev Col Bras Cir. 2018;46:e2011.
Estomba CC, Fernández IG, Otero MI. How we do it: anterior and posterior nosebleed trainer, the 3D printing epistaxis project. Clin Otolaryngol. 2016;43:765–6.
Park L, Price-Williams S, Jalali A, Pirzada K. Increasing access to medical training with three-dimensional printing: creation of an endotracheal intubation model. JMIR Medical Education. 2019;5:e12626.
Muwaffak Z, Goyanes A, Clark V, Basit AW, Hilton ST, Gaisford S. Patient-specific 3D scanned and 3D printed antimicrobial polycaprolactone wound dressings. Int J Pharm. 2017;527:161–70.
Li J, Tanaka H. Rapid customization system for 3D-printed splint using programmable modeling technique – a practical approach. 3D Printing Med. 2018;4(1):5. https://doi.org/10.1186/s41205-018-0027-6. Epub 2018 May 25. PMID: 29882529; PMCID: PMC5970151.
Wu P-K, Shih Y-C, Chen C-M, Chen G, Chen W-M, Huang L-Y, et al. Printing a 3-dimensional, patient-specific splint for wound immobilization: a case demonstration. Ostomy Wound Management. 2018;64:8–17.
Gómez-Ramos JJ, Marín-Medina A, Prieto-Miranda SE, Dávalos-Rodríguez IP, Alatorre-Jiménez MA, Esteban-Zubero E. Determination of plasma lactate in the emergency department for the early detection of tissue hypoperfusion in septic patients. Am J Emerg Med. 2018;36:1418–22.
Aguilera-Astudillo C, Chavez-Campos M, Gonzalez-Suarez A, Garcia-Cordero JL. A low-cost 3-D printed stethoscope connected to a smartphone. 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC); 2016.
Kim S-H, Kwon J, Kim Y-J, Lee H-J, Seo H-C, Lim SB, et al. Impact of a custom-made 3D printed ergonomic grip for direct laryngoscopy on novice intubation performance in a simulated easy and difficult airway scenario—a manikin study. PLoS One. 2018;13:e0207445.
Dinsmore M, Doshi S, Sin V, Matava C. Design and evaluation of a novel and sustainable human-powered low-cost 3D printed thermal laryngoscope. J Med Syst. 2019;43:143.
Lee DW, Thampi S, Yap EPH, Liu EHC. Evaluation of a smartphone camera system to enable visualization and image transmission to aid tracheal intubation with the Airtraq® laryngoscope. J Anesth. 2016;30:514–7.
Vukicevic M, Mosadegh B, Min JK, Little SH. Cardiac 3D printing and its future directions. JACC Cardiovasc Imaging. 2017;10:171–84.
Schoffer F. How expiring patents are ushering in the next generation of 3D printing [Internet]. TechCrunch. TechCrunch; 2016 [cited 2020Jun5]. Available from: https://techcrunch.com/2016/05/15/how-expiring-patents-are-ushering-in-the-next-generation-of-3d-printing/.
Mardis NJ. Emerging technology and applications of 3D printing in the medical field. Sci Med. 2018;115:368–73.
Hoang D, Perrault D, Stevanovic M, Ghiassi A. Surgical applications of three-dimensional printing: a review of the current literature & how to get started. Ann Transl Med. 2016;4:456.
Filippou V, Tsoumpas C. Recent advances on the development of phantoms using 3D printing for imaging with CT, MRI, PET, SPECT, and ultrasound. Med Phys. 2018;45:e740–760.
Hafezi F, Scoutaris N, Douroumis D, Boateng J. 3D printed chitosan dressing crosslinked with genipin for potential healing of chronic wounds. Int J Pharm. 2019;560:406–9.
Songjaroen T, Primpray V, Manosarn T, Khumchanta W, Sakuldamrongpanich T, Kulkeratiyut S, et al. A simple and low-cost portable paper-based ABO blood typing device for point-of-care testing. J Immunoass Immunochem. 2018;39:292–307.
Chan HN, Tan MJA, Wu H. Point-of-care testing: applications of 3D printing. Lab Chip. 2017;17:2713–39.
Knowlton S, Joshi A, Syrrist P, Coskun AF, Tasoglu S. 3D-printed smartphone-based point of care tool for fluorescence- and magnetophoresis-based cytometry. Lab Chip. 2017;17:2839–51.
Basilotta F, Riario S, Stradolini F, Taurino I, Demarchi D, Micheli GD, et al. Wireless monitoring in intensive care units by a 3D-printed system with embedded electronic. 2015 IEEE Biomedical Circuits and Systems Conference (BioCAS) 2015.
Martin-Noguerol T, Paulano-Godino F, Menias CO, Luna A. Lessons learned from COVID-19 and 3D printing. Am J Emerg Med. 2020; S0735-6757(20)30693–8. https://doi.org/10.1016/j.ajem.2020.08.010. Epub ahead of print. PMID: 32829987; PMCID: PMC7428745.
Callahan CJ, Lee R, Zulauf KE, Tamburello L, Smith KP, Previtera J, et al. Open development and clinical validation of multiple 3D-printed nasopharyngeal collection swabs: rapid resolution of a critical COVID-19 testing bottleneck. J Clin Microbiol. 2020;58:1–4.
Ishack S, Lipner SR. Applications of 3D printing technology to address COVID-19–related supply shortages. Am J Med. 2020;133:771–3.
Tino R, Moore R, Antoline S, et al. COVID-19 and the role of 3D printing in medicine. 3D Print Med. 2020;6:11. https://doi.org/10.1186/s41205-020-00064-7.
Acknowledgements
The authors would like to acknowledge the uOttawa Health Librarian Majela Guzman for her contributions to the design of the search strategy used in this paper.
Funding
Not Applicable.
Author information
Authors and Affiliations
Contributions
M.B.: Conceptualization, Writing-original draft preparation, Visualization, Investigation, Formal Analysis. J.G.: Conceptualization, Writing-Reviewing and Editing. J.P.: Methodology, Writing-Reviewing and Editing. A.P.: Conceptualization, Writing-Reviewing and Editing, Supervision. All author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not Applicable.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Boshra, M., Godbout, J., Perry, J.J. et al. 3D printing in critical care: a narrative review. 3D Print Med 6, 28 (2020). https://doi.org/10.1186/s41205-020-00081-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41205-020-00081-6