
Abstract
Background
In low-and-middle-income, including Ethiopia, high-risk fertility behavior is a major public health concern. High-risk fertility behavior has an adverse influence on maternal and child health, which hampered efforts to reduce maternal and child morbidity and mortality in Ethiopia. Therefore, this study aimed to assess the spatial distribution and associated factors of high-risk fertility behavior among reproductive-age women in Ethiopia using recent nationally representative data.
Methods
Secondary data analysis was done with a total weighted sample of 5865 reproductive-aged women using the latest mini EDHS 2019. The spatial distribution of high-risk fertility behavior in Ethiopia was determined using spatial analysis. Multilevel multivariable regression analysis was used to identify predictors of high-risk fertility behavior in Ethiopia.
Results
The prevalence of high-risk fertility behavior among reproductive-age women in Ethiopia was 73.50% (95% CI 72.36%, 74.62%). Women with primary education [AOR = 0.44; 95%CI; 0.37, 0.52], women with secondary and above education [AOR = 0.26; 95%CI; 0.20, 0.34], being Protestant religion followers [AOR = 1.47; 95%CI; 1.15, 1.89], being Muslim religion follower [AOR = 1.56; 95%CI; 1.20, 2.01], having television [AOR = 2.06; 95%CI; 1.54, 2.76], having ANC visit [AOR = 0.78; 95%CI; 0.61, 0.99], using contraception [AOR = 0.77; 95%CI; 0.65, 0.90], living in rural areas [AOR = 1.75; 95%CI; 1.22, 2.50] were significantly associated with high-risk fertility behavior. Significant hotspots of high-risk fertility behavior were detected in Somalia, SNNPR, Tigray region, and Afar regions of Ethiopia.
Conclusions
A significant proportion of women in Ethiopia engaged in high-risk fertility behavior. High-risk fertility behavior was distributed non-randomly across Ethiopian regions. Policymakers and stakeholders should design interventions that take into account the factors that predispose women to have high-risk fertility behaviors and women who reside in areas with a high proportion of high-risk fertility behaviors to reduce the consequences of high-risk fertility behaviors.
Similar content being viewed by others


Introduction
Maternal and child mortality is one of the major public health problems in the world, and it is particularly serious in developing countries [1]. Maternal high-risk fertility behavior is a risk factor that hinders efforts in lowering maternal and child morbidity and mortality [2,3,4]. High-risk fertility behavior (HRFB) remained to be a significant cause of neonatal and under-five mortality in low- and middle-income countries (LMICs) [5,6,7,8]. Several studies have revealed that high-risk fertility behavior has an adverse influence on maternal and child health [9,10,11]. The consequences of high-risk fertility behavior are more severe in LMICs, where healthcare is difficult to access and there is a high prevalence of unmet family planning needs [12,13,14].
Women's fertility behavior is measured by maternal age at delivery, birth spacing, and birth order, which have a significant impact on women's and children's well-being [12, 15]. High-risk fertility behavior constitutes too-early (< 18 years) or too-late(> 34 years) maternal age at delivery, short inter-pregnancy birth interval, and a higher number of live births of order three or higher [2, 16,17,18,19]. According to the WHO guidelines, a birth that occurred less than 24 months after a previous birth in two consecutive births was classified as having a short birth interval [20]. The age at first birth influences how many children a woman will have during her reproductive period [21], and childbirth by a very young or very old mother is associated with an increased risk of infant and child mortality [10, 22].
Like other LMICs in Ethiopia also, high-risk fertility behavior is a major public health concern causing poor birth and child outcomes [6, 13, 23]. Preterm births, intrauterine growth restriction, neonatal mortality, stillbirths, amniotic fluid embolism, chromosomal abnormalities, and low-birth-weight newborns are associated with late motherhood (> 34 years) [7, 24, 25]. Furthermore, high-risk fertility behavior in mothers increases the risk of chronic malnutrition in children [16].
Different previous studies across the world revealed factors such as residence [4, 9, 19, 26,27,28], educational status [4, 12, 29, 30], partner education [29], religion [27, 31], wealth index [28], health care access challenge [32], contraceptive use [27,28,29,30,31, 33, 34], ANC visit [4, 32], unwanted pregnancy[31], and history of abortion [32] were associated with high-risk fertility behavior (Fig. 1).

Conceptual framework of factors associated with high-risk fertility behavior developed from searching of literature
The majority of studies about HRFB in Ethiopia focused on determining the impact of HRFB on maternal and child health outcomes [23, 35]. Even though studies about high-risk fertility behavior in Ethiopia have been conducted based on EDHS 2016, assessing the spatial variation and determinants of high-risk fertility behavior using the most recent nationally representative data (2019 EDHS) is essential for providing updated information and designing geographically focused interventions in Ethiopia. Therefore, this study aimed to answer the following research questions. What was the magnitude of high-risk fertility behavior among women of reproductive age in Ethiopia in 2019 EDHS? What are the individual and community-level factors that contribute to high-risk fertility behavior? How do the spatial patterns of high-risk fertility behavior in Ethiopia appear? The study will provide timely information to program planners and policymakers to reduce the consequences of high-risk fertility behavior.
Methods
Data sources, sampling procedure, and populations
For our study, we used data from the 2019 mini EDHS, which was the second EMDHS and the fifth DHS implemented in Ethiopia from March 21, 2019, to June 28, 2019. Ethiopia is located in the Horn of Africa, between 3° and 15° north latitude and 33° and 48° east longitude. The source of the population in this study was all reproductive-age women in Ethiopia within 5 years of the surveys, whereas the study population was all reproductive-age women in the selected enumeration areas within 5 years of the survey.
A two-stage cluster sampling technique was used to collect and stratify the EDHS samples. After stratifying each region into urban and rural areas, 305 (93 urban and 212 rural) clusters or enumeration areas were chosen in the first stage. The second stage of selection involved selecting a fixed number of 30 households per cluster with an equal probability of systematic selection from the newly created household listing. The detailed sampling procedure was accessible on the Measure DHS [36]. Data were obtained from the DHS website: www.dhsprogram.com after a formal request. The individual record data set was used for this analysis. A total weighted sample of 5865 reproductive-age women was included in this study.
Variables of the study
The dependent variable was high-risk fertility which was a binary variable that was defined following the DHS guide [36]. A woman is considered to have high-risk fertility behavior if a woman is either under the age of 18 years or 34 years at the time of birth, has a birth interval of fewer than 24 months, or has the latest child of order three or higher which is coded as “1”, otherwise coded as “0” [36].
Relevant independent variables for this study were chosen based on previous literature. Individual level independent variables considered in the analysis include maternal educational level, religion, household wealth, having television, having a radio, sex of household head, ANC Visit, contraceptive use, child sex, and place of delivery. Residence, community-level poverty, community level of women's education, and region were included as community-level variables. Regions were classified into three categories; Amhara, Oromia, Tigray, and SNNP regions were categorized as a large central region; Harari, Addis Ababa, and Dire Dawa were categorized as metropolitan regions, and the others (Somali, Gambela, Afar, and Benishangul Gumuz region) were categorized as a small peripheral region [37, 38]. Because the data were not normally distributed, community poverty and literacy levels were classified as high or low, using the median value as the classification cutoff point. The poverty level in a community was categorized as high if the proportion of women in the two lowest wealth quintiles was greater than the median value, and low if the proportion was less than the median value [39]. The community level of women's education was categorized as high if the proportion of women with at least a primary level of education was greater than the median value, and low if it was less than the median value [40].
Data management and analysis
After accessing the data, it was cleaned and coded to make it suitable for analysis. Sample weights were used to restore the survey's representativeness and obtain valid statistical estimates. STATA version 16 was used to compute both descriptive and analytic statistics. We performed a multilevel logistic regression with a random effect at the cluster level, accounting for the clustered nature of the data as well as within and between community variations, and assuming that each community has a different intercept (β0) and fixed coefficient (β) [41]. Variables with p value < 0.2 in the bi-variable analysis for both individual and community-level factors were fitted in the multivariable model, and the Adjusted Odds Ratio (AOR) with a 95% Confidence Interval (CI) in the multivariable model was used to declare statistically significant associations with the outcome variable. The goodness of fit of our model was assessed using deviance information criteria (DIC) (− 2*log-likelihood value). The Variance Inflation Factor (VIF) was utilized to test for multicollinearity among the independent variables. ArcGIS version 10.7 and SaTScan version 9.6 software were utilized for spatial and SaTScan analysis.
Spatial analysis
Geographic variations in high-risk fertility behavior cases among EDHS clusters were assessed using spatial analysis. We computed the proportions of high-risk fertility behavior cases in the survey for each cluster and then appended the latitude and longitude coordinates of the selected EAS in the 2019 EDHS survey. The spatial autocorrelation (Global Moran's Index) statistic was utilized to determine whether high-risk fertility behavior among reproductive-age women in the study area was dispersed, clustered, or randomly distributed [42, 43] The maximum peak distance at which high-risk fertility behavior becomes more prominent was determined using incremental spatial autocorrelation [42].
Getis-Ord Gi* statistics were calculated to determine how spatial autocorrelation differs across study locations. Statistical output with a high GI* denotes a "hotspot," whereas a low GI* suggests a "cold spot" [44]. A “hotspot” area indicates a high prevalence of high-risk fertility behavior, while a “cold spot” area indicates a low prevalence of high-risk fertility behavior.
The ordinary Kriging spatial interpolation technique was used to predict areas that were not sampled based on sampled values. The spatial interpolation was performed under the assumption that spatially distributed objects are spatially correlated, and that objects that are close together are more likely to have similar properties [45, 46].
The spatial locations of statistically significant clusters for HRFB in Ethiopia were determined using Bernoulli-based model spatial scan statistics. A likelihood ratio test statistic and the p value were utilized to decide whether the number of observed high-risk fertility behavior within the potential cluster was significantly higher than expected.
Parameter estimation and model building
The fixed effects were used to calculate the odds ratio with a 95% confidence interval and a p value of < 0.05 for the correlation between HRFB and predictor variables. The likelihood of having HRFB was modeled as follows:
where πij = is the probability of having HRFB and 1-πij represents the probability of not having HRFB. The β’s are fixed coefficients indicating a unit increase in X can cause a β unit increase in the probability of having HRFB.\({X}_{1},{X}_{2}\)…., \({X}_{k}\) are the individual and community-level independent variables for the ith individual in community j, respectively. The \({\beta }_{0}\) represents the intercept, which is the effect on HRFB when all independent variables are excluded. The \({\mathrm{u}}_{j}\) represents the random effect, which is the community's effect on having HRFB for the jth community, and eij represents random error at the individual level.
The random effects were determined using Intra-Class Correlation (ICC), the median odds ratio (MOR), and the proportional change in variance (PCV), which measures the variation in high-risk fertility behavior across communities or clusters. The ICC measures the differences between clusters in HRFB among women of the reproductive age group, and it is computed as ICC = \(\frac{VA}{ VA+3.29}*100\), where VA = area-level variance [47,48,49]. When two clusters are chosen at random, the MOR represents the central value of the odd ratio between the highest and lowest risk regions. The MOR is calculated as MOR = e0.95 \(\surd VA\), where VA = area level variance [41, 50].
The PCV measures how much of the total observed individual variation can be attributed to cluster differences. The PCV is calculated as; \(\frac{V\mathrm{null}-VA}{V\mathrm{null}}*100\); whereas, Vnull represents the variance of the initial model, while VA represents the variance of the model with more terms [41, 50].
In multilevel analysis, four models were fitted. The first was a null model with no independent variables, which is fitted to assess the variability of HRFB in the community. The second (model I) hierarchical models contain individual-level variables, whereas the third (model II) contains community-level variables. In the fourth model (model III) both individual and community-level variables were fitted simultaneously.
Ethical consideration
All methods were carried out following relevant guidelines of the Demographic and Health Surveys (DHS) program. Informed consent was waived from the International Review Board of Demographic and Health Surveys (DHS) program data archivists after the consent paper was submitted to the DHS Program, a letter of permission to download the data set for this study. The data set was not shared or passed on to other bodies and has maintained its confidentiality.
Results
Characteristics of the study participants
A total weighted sample of 5865 women aged 15–49 was included in this study. The median age of women was 29 years, with an interquartile range of 24–36 years. Most of the study participants 4236 (72.25%) live in rural areas, and more than three quarters of these (3262 (77.00%) women have HRFB. Around half of the study participants, 3025 (51.59%) have no education, and out of these, around 2555 (84.47%) participants have high-risk fertility behavior. The overall prevalence of HRFB among reproductive-age women in Ethiopia was 73.50% (95% CI 72.36%, 74.62%) (Table 1).
The random effect analysis result
The ICC in the null model was 0.10, which means that about 10% of the variations in HRFB among reproductive-age women were due to cluster differences, while the remaining 90% were due to individual-level factors. The PCV value, 16.66%, in the final model indicates that about 16.66% of the variation in HRFB among reproductive-age women was attributed to both individual and community-level factors. The model with the lowest deviance was selected as the best-fitted model which was model III (4775). All variables had VIF values less than 10, and the final model's mean VIF value was 1.67, indicating the absence of multi-collinearity (Table 2).
Spatial analysis results
Spatial autocorrelation of high-risk fertility behavior among reproductive-age women in Ethiopia
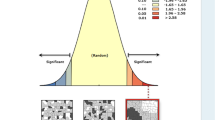
The Global Moran's Index value was 0.208, implying that there was a significant clustering variation of HRFB among reproductive-age women and children, with a p < 0.001. In addition, the Z scores of 4.61 indicated a clustered variation of high-risk HRFB among reproductive-age women across Ethiopian regions (Fig. 2). The incremental autocorrelation result revealed statistically significant z-scores at a maximum distance of 275.410 km 3.25 (distances; z-score) for HRFB.

Spatial autocorrelation analysis of high-risk fertility behavior among reproductive-age women in Ethiopia, 2019 Ethiopian Demographic and Health Survey
Hotspot analysis of high-risk fertility behavior among reproductive-age women in Ethiopia
We found substantial spatial variability in the distribution of HRFB among Ethiopian women of reproductive age with significant hotspots found in Somalia, SNNPR, Tigray region, and some parts of Afar regions indicated in red color. The significant cold spots were found in Addis Ababa, the Southern border of the Amhara region, and the Northwestern part of SNNPR regions indicated in blue color (Fig. 3).

Hot spot analysis of high-risk fertility behavior among reproductive-age women in Ethiopia, 2019 Ethiopian Demographic and Health Survey
Spatial interpolation of high-risk fertility behavior among reproductive-age women in Ethiopia
High-risk areas are indicated by red prediction zones, and women who live in such areas are more likely to have high-risk fertility behavior. The prevalence of predicted HRFB among women of reproductive age was highest in Somalia, Afar, northern SNNPR, Dire Dawa, northern Amhara, and southern Oromia regions, ranging from 81 to 88%. The lowest predicted area of HRFB was observed in Addis Ababa and the northwestern part of the SNNPR regions (Fig. 4).

Kriging interpolation of high-risk fertility behavior among reproductive-age women in Ethiopia, 2019 Ethiopian Demographic and Health Survey
Spatial scan statistical analysis of high-risk fertility behavior among reproductive-age women in Ethiopia
The SaTScan analysis result identified a total of 131 clusters of HRFB. The primary clusters detected in regions of Dire Dawa, Oromia, Northern SNNPR, and the southern border of Afar at 98.919051 N, 40.955418 E with a 111.22 km radius, with a relative risk of 1.25 and log-likelihood ratio (LLR) of 18.02 at a p value < 0.001. Women who lived within the spatial window had a 1.25 times higher chance of having high-risk fertility behavior as compared to those women outside the spatial window (Fig. 5).

Spatial scan statistics analysis of high-risk fertility behavior among reproductive-age women in Ethiopia, 2019 Ethiopian Demographic and Health Survey
Fixed effect analysis results
According to the final model result, women's education status, religion, having television, ANC visits, contraceptive use, and residence have significant associations with HRFB among reproductive-age women in Ethiopia.
Women who were Muslims and protestant religion followers were 1.56 (AOR = 1.56; 95% CI; 1.20, 2.01), and 1.47 (AOR = 1.47; 95% CI; 1.15, 1.89) times higher odds of having HRFB, respectively, than orthodox religion follower women. Women who have primary, and (secondary and higher education) were 56% (AOR = 0.44; 95% CI; 0.37, 0.52), and 74% (AOR = 0.26; 95% CI; 0.20, 0.34) times lower odds of having HRFB than women who have no education. The odds of having HRFB among women who use contraceptives were 23% (AOR = 0.77; 95% CI; 0.65, 0.90) less compared to their counterparts. The odds of having HRFB among women who have ANC visits were 22% (AOR = 0.78; 95% CI; 0.61, 0.99) less compared to those women who have no ANC visits. The odds of having HRFB among women who have television were 2.06 (AOR = 2.06; 95% CI; 1.54, 2.76) times higher than women who have no television. Women who live in rural areas were 1.75(AOR = 1.75; 95% CI; 1.22, 2.50) times more likely to have HRFB compared to women who live in urban areas (Table 3).
Discussion
Nearly three fourth of women in Ethiopia had high-risk fertility behavior. The result is higher than that of a study conducted in Bangladesh [31], a pooled study in nine East African countries [32], and lower than a previous study done in Ethiopia [4]. The possible reason for the discrepancy might be differences in participants' socio-demographic characteristics and the difference in health service availability across study areas. Moreover, high birth order is the most common single risk, with nearly half of all women reporting it. The short birth interval was the least common risk, affecting nearly one-third of all women.
The spatial distribution of HRFB among reproductive-age women in Ethiopia varied greatly across regions. Significant hotspots of HRFB among reproductive-age women were detected in Somalia, SNNPR, Tigray region, and some parts of the Afar regions of Ethiopia. The SaTScan analysis result identified primary clusters found in regions of Dire Dawa, Oromia, Northern SNNPR, and the southern border of Afar. The finding was supported by previous studies that indicated living in the Somalia region are more likely to engage in HRFB, whereas women in the Amhara region are less likely to engage in HRFB [4]. The possible reason might be due to variations in health care services access across regions of Ethiopia [51]. Another possible explanation for regional differences in high-risk fertility behavior hot spot areas could be differences in demographic, cultural, and socioeconomic factors [52]. Studies also indicated that there is a low proportion of modern contraceptive utilization in the Somali, Afar, Gambela, Tigray, and Benishangul-Gumuz regions of Ethiopia [53, 54]. Furthermore, pastoralists may have limited access to health information and modern family planning services due to their high mobility and a strong commitment to cultural and religious values [55,56,57].
A woman's HRFB is inversely associated with her educational level. Women who have primary and secondary education had a reduced risk of HRFB than women with no formal education. This finding was consistent with the study result in Ethiopia [4, 6], Nigeria [12], and Nepal [16]. The possible explanation would be that educated women are more aware of high-risk fertility behavior than uneducated women. Another possibility is that educated women may experience a delay in becoming pregnant due to reasons related to their career path [13].
According to this study, Muslim and protestant women in Ethiopia were more likely to engage in HRFB than orthodox religious followers. This finding is in line with a study done in Bangladesh [31], India [58], and Nepal [59]. Religion has enormous social and economic relevance in most societies, and each region has beliefs about marriage, reproductive behavior, and contraceptive use [60,61,62]. According to studies, the use of contraception is criticized in Islamic religious teachings, causing them to have a short birth interval and a high birth order [15].
Women having ANC visits are less likely to engage in HRFB than women not having ANC visits. The study's findings are similar to those of several other study results done in Ethiopia [4]. The possible reason might be that during ANC visits, a variety of essential services are provided to promote the health of the mother and newborn including information exchange and counseling women about birth preparation and family planning options for optimal birth intervals [63].
Contraceptive users were less likely to engage in HRFB than contraceptive nonusers. The finding is similar to a study done in Ethiopia [4], Bangladesh [31], and Sub-Saharan Africa [29]. As per study results, using contraception has a significant association with lowering the burden of these high-risk births, which reduces maternal and neonatal mortality [33]. Women having television are more likely to have HRFB than women who not having a television. This finding is contradictory to previous studies in Nepal [59]. Studies indicated that exposure to mass media (radio/TV) has a significant impact on reproductive behavior [59]. The difference could be because most studies define media exposure as the frequency of watching television, listening to the radio, or reading the newspaper, whereas our study only considers possession of television, which may not be an assurance for increasing awareness of HRFB. Since we have no information on the channels and serials broadcasted on television, as well as the frequency with which women watch television, we cannot be certain that owning a television plays a positive role in having high-risk fertility behavior.
Women who live in rural areas are more likely to participate in HRFB than women who live in urban areas. This finding is in line with a study done in Ethiopia [4, 6], and East African countries [32]. The possible explanation is that women in rural areas are severely underserved in terms of maternal health services, and the majority of women in rural areas may be uneducated, causing them to be less aware of the problems associated with high-risk fertility behavior.
The study's main strength was that it used nationally representative data with a large sample size and an appropriate statistical approach that took into account the data's hierarchical nature. However, this study had limitations in that the cross-sectional nature of the data makes it impossible to infer causality between the independent and dependent variables. Since this survey relies on respondents' self-report, there may be a chance of recall bias.
Conclusion
A significant proportion of women in Ethiopia engaged in high-risk fertility behavior. High-risk fertility behavior was distributed non-randomly across Ethiopian regions. Policymakers and stakeholders should design interventions that take into account the factors that predispose women to have high-risk fertility behaviors and women who reside in areas with a high proportion of high-risk fertility behaviors to reduce the consequences of high-risk fertility behaviors.
Availability of data and materials
The data sets used during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- ANC:
-
Antenatal care
- AOR:
-
Adjusted Odds Ratio
- CI:
-
Confidence Interval
- COR:
-
Crude odds ratio
- DHS:
-
Demographic and Health Survey
- EAs:
-
Enumeration Areas
- EDHS:
-
Ethiopian Demographic and Health Survey
- GIS:
-
Geographic Information System
- HRFB:
-
High-risk fertility behavior
- ICC:
-
Intra-class Correlation
- MOR:
-
Median Odd Ratio
- PCV:
-
Proportional Change in Variance
- SNNP:
-
Southern nation nationalities of people
- VIF:
-
Variance inflation factor
References
Hogan MC, Foreman KJ, Naghavi M, Ahn SY, Wang M, Makela SM, et al. Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards Millennium Development Goal 5. Lancet. 2010;375(9726):1609–23.
AmirudDin R, Naz L, Rubi A, Usman M, Ghimire UJB. Impact of high-risk fertility behaviours on underfive mortality in Asia and Africa: evidence from Demographic and Health Surveys. BMC Preg Childbirth. 2021;21(1):1–14.
Pal SK, Shekhar CJCE, Health G. Examining the role of high-risk fertility behaviour in chronic undernutrition among Indian married women age 15–49. Clin Epidemiol Global Health. 2021;11: 100739.
Tessema ZT, Tamirat KSJ. Determinants of high-risk fertility behavior among reproductive-age women in Ethiopia using the recent Ethiopian Demographic Health Survey: a multilevel analysis. Trop Med Health. 2020;48(1):1–9.
Finlay JE, Norton MK, Mejía-Guevara IJIJ. Adolescent fertility and child health: the interaction of maternal age, parity and birth intervals in determining child health outcomes. Int J Child Health Nutr. 2017;6(1):16–33.
Gurmu E, Tariku DJJ. Correlates of high risk fertility behaviour in Ethiopia: a multilevel analysis of the 2011 Ethiopian demographic and health survey data. J Health Med Nurs. 2017;2017(39):86–95.
Bhalotra S, Van Soest AJJ. Birth-spacing, fertility and neonatal mortality in India: Dynamics, frailty, and fecundity. J Econ. 2008;143(2):274–90.
Geronimus ATJP. On teenage childbearing and neonatal mortality in the United States. Popul Develop Rev. 1987;8:245–79.
Rahman M, Islam MJ, Haque SE, Saw YM, Haque MN, Duc NHC, et al. Association between high-risk fertility behaviours and the likelihood of chronic undernutrition and anaemia among married Bangladeshi women of reproductive age. Public Health Nutr. 2017;20(2):305–14.
Khan MA, Khan N, Rahman O, Mustagir G, Hossain K, Islam R, et al. Trends and projections of under-5 mortality in Bangladesh including the effects of maternal high-risk fertility behaviours and use of healthcare services. PLoS ONE. 2021;16(2): e0246210.
Rahman M, Hosen A, Khan MAJ. Association between maternal high-risk fertility behavior and childhood morbidity in Bangladesh: a nationally representative cross-sectional survey. Am J Trop Med Hyg. 2019;101(4):929.
Adiri F, Ibrahim HI, Ajayi V, Sulayman HU, Yafeh AM, Ejembi CLJA. Fertility behaviour of men and women in three communities in Kaduna state. Nigeria Afr J Reprod Health. 2010;14(3):97–105.
Fall CH, Sachdev HS, Osmond C, Restrepo-Mendez MC, Victora C, Martorell R, et al. Association between maternal age at childbirth and child and adult outcomes in the offspring: a prospective study in five low-income and middle-income countries (COHORTS collaboration). Lancet Glob Health. 2015;3(7):e366–77.
Jonas K, Crutzen R, van den Borne B, Sewpaul R, Reddy PJRh. Teenage pregnancy rates and associations with other health risk behaviours: a three-wave cross-sectional study among South African school-going adolescents. Reprod Health. 2016;13(1):1–14.
Asghar M, Murry B, Saraswathy KNA. Fertility behaviour and effect of son preference among the Muslims of Manipur. India J Anthropol. 2014;2014:1.
Rahman M, Haque SE, Zahan S, Islam J, Rahman M, Asaduzzaman M, et al. Maternal high-risk fertility behavior and association with chronic undernutrition among children under age 5 y in India, Bangladesh, and Nepal: do poor children have a higher risk? Nutrition. 2018;49:32–40.
Khan T, Ali Khan REJJ. Fertility behaviour of women and their household characteristics: A case study of Punjab. Pakistan J Hum Ecol. 2010;30(1):11–7.
Isabirye A. The effects of high risk fertility behavior on child survival in Uganda. Makerere: Makerere University; 2012.
Hammarberg K, Zosel R, Comoy C, Robertson S, Holden C, Deeks M, et al. Fertility-related knowledge and information-seeking behaviour among people of reproductive age: a qualitative study. Hum Fertil. 2017;20(2):88–95.
World Health Organization. Report of a WHO technical consultation on birth spacing. Geneva: World Health Organization; 2007.
Chowdhury S, Rahman M, Zayed NM, Shahi SK, Science S. Determinants of Age at First Birth of Bangladeshi Women: A Multivariate Approach on DHS 2014 Data. J Human Arts Soc Sci. 2020;4(2):118–25.
Maxwell L, Nandi A, Benedetti A, Devries K, Wagman J, García-Moreno CJB. Intimate partner violence and pregnancy spacing: results from a meta-analysis of individual participant time-to-event data from 29 low-and-middle-income countries. BMJ Glob Health. 2018;3(1):e000304.
Asresie MB, Dagnew GW. Association of maternal high-risk fertility behavior and under-five mortality in Ethiopia: Community-based survey. PLoS ONE. 2022;17(5):e0267802.
Favilli A, Pericoli S, Acanfora MM, Bini V, DiRenzo GC, Gerli SMF, et al. Pregnancy outcome in women aged 40 years or more. J Matern-Fetal Neonatal Med. 2012;25(8):1260–3.
Fretts RC, Usher RHJO. Causes of fetal death in women of advanced maternal age. Obstetr Gynecol. 1997;89(1):40–5.
Ndiaye K, Portillo E, Ouedraogo D, Mobley A, Babalola SJGHS. High-risk advanced maternal age and high parity pregnancy: tackling a neglected need through formative research and action. Global Health. 2018;6(2):372–83.
Tesema GA, Worku MG, Teshale ABJ. Duration of birth interval and its predictors among reproductive-age women in Ethiopia: Gompertz gamma shared frailty modeling. PLoS ONE. 2021;16(2):e0247091.
Chowdhury S, Singh A, Kasemi N, Chakrabarty M, Singh SJJ. Short birth interval and associated factors in rural India: A cross-sectional study. J Biosoc Sci. 2022;8:1–20.
Seidu A-A, Ahinkorah BO, Anjorin SS, Tetteh JK, Hagan JE, Zegeye B, et al. High-risk fertility behaviours among women in sub-Saharan Africa. J Public Health. 2021. https://doi.org/10.1093/pubmed/fdab381.
Roble AK, Osman MO, Ibrahim AM, Wedajo GT, Usman A, SJSom. Determinants of short birth interval among ever married reproductive age women living in Jigjiga, Eastern Ethiopia,. unmatched case–control study. SAGE Open Medicine. 2020;2021(9):20503121211067870.
Howlader M, Roshid HO, Kundu S, Halder HR, Chanda SK, Rahman MJRH. Determinants associated with high-risk fertility behaviours among reproductive aged women in Bangladesh: a cross-sectional study. Reprod Health. 2022;19(1):1–10.
Tamirat KS, Tesema GA, Tessema ZTJ. Determinants of maternal high-risk fertility behaviors and its correlation with child stunting and anemia in the East Africa region: A pooled analysis of nine East African countries. PLoS ONE. 2021;16(6):e0253736.
Brown W, Ahmed S, Roche N, Sonneveldt E, Darmstadt GL. Impact of family planning programs in reducing high-risk births due to younger and older maternal age, short birth intervals, and high parity. Seminars in perinatology; 2015: Elsevier.
Singer Babiarz K, Miller G, Valente C, Lee J, Tey NPJC. Family planning and fertility behavior: evidence from twentieth century Malaysia. In: Center for global development working paper. 2017. p. 470.
Fadl N, Ice GH, Haile ZTJN. Association between maternal high-risk factors and anemia among women in Ethiopia. Nutrition. 2021;91: 111404.
Croft T, Marshall AM, Allen CKJI. Guide to DHS Statistics 2018. 2019.
Abrha S, Shiferaw S, Ahmed KYJ. Overweight and obesity and its socio-demographic correlates among urban Ethiopian women: evidence from the 2011 EDHS. BMC Public Health. 2016;16(1):1–7.
Mare KU, Aychiluhm SB, Tadesse AW, Mohammed OAJ. Individual and community-level determinants of non-use of contraceptive among women with no fertility desire in Ethiopia: a multilevel mixed-effect analysis. Emerg Themes Epidemiol. 2022;19(1):1–10.
Liyew AM, Teshale ABJ. Individual and community level factors associated with anemia among lactating mothers in Ethiopia using data from Ethiopian demographic and health survey, 2016; a multilevel analysis. BMC Public Health. 2020;20(1):1–11.
Sisay D, Ewune HA, Muche T, Molla WJO, International G. Spatial Distribution and Associated Factors of Institutional Delivery among Reproductive-Age Women in Ethiopia: The Case of Ethiopia Demographic and Health Survey. 2022;2022.
Merlo J, Chaix B, Yang M, Lynch J, Råstam LJJ, Health C. A brief conceptual tutorial on multilevel analysis in social epidemiology: interpreting neighbourhood differences and the effect of neighbourhood characteristics on individual health. J Epidemiol Community Health. 2005;59(12):1022–9.
Waldhör TJSM. The spatial autocorrelation coefficient Moran’s I under heteroscedasticity. Statist Med. 1996;15(7–9):887–92.
Fischer MM, Getis A. Handbook of applied spatial analysis: software tools, methods and applications. Berlin: Springer; 2010.
Tsai P-J, Lin M-L, Chu C-M, Perng C. Spatial autocorrelation analysis of health care hotspots in Taiwan in 2006. BMC Public Health. 2009;9(1):1–13.
Franklin J. Mapping species distributions: spatial inference and prediction. Cambridge: Cambridge University Press; 2010.
Le ND, Zidek JVMA. Interpolation with uncertain spatial covariances: a Bayesian alternative to kriging. J Multivariate Anal. 1992;43(2):351–74.
Austin PC, Merlo JJS. Intermediate and advanced topics in multilevel logistic regression analysis. Stat Med. 2017;36(20):3257–77.
Sommet N, Morselli DJI. Keep calm and learn multilevel logistic modeling: A simplified three-step procedure using Stata, R, Mplus, and SPSS. Int Rev Soc Psychol. 2017;30:203–18.
Weinmayr G, Dreyhaupt J, Jaensch A, Forastiere F, Strachan DPJE. Multilevel regression modelling to investigate variation in disease prevalence across locations. Int J Epidemiol. 2017;46(1):336–47.
Merlo J, Chaix B, Ohlsson H, Beckman A, Johnell K, Hjerpe P, et al. A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Community Health. 2006;60(4):290–7.
CSA-Ethiopia I. International. Ethiopia Demographic and Health Survey. Key Indicators Report. USA: CSA and ICF; 2016. p. 2016.
Shifti DM, Chojenta C, Holliday EG, Loxton DJP. Application of geographically weighted regression analysis to assess predictors of short birth interval hot spots in Ethiopia. PLoS ONE. 2020;15(5):e0233790.
Tegegne TK, Chojenta C, Forder PM, Getachew T, Smith R, Loxton DJB. Spatial variations and associated factors of modern contraceptive use in Ethiopia: a spatial and multilevel analysis. BMJ Open. 2020;10(10):e037532.
Merera AM, Lelisho ME, Pandey DJJ, Disparities EH. Prevalence and Determinants of Contraceptive Utilization among Women in the Reproductive Age Group in Ethiopia. J Racial Ethnic Health Disparities. 2022;9(6):2340–50.
Kahsay ZH, Tegegne D, Mohammed E, Kiros GJP. Application of individual behavioral models to predict willingness to use modern contraceptives among pastoralist women in Afar region, Northern Ethiopia. PLoS ONE. 2018;13(5):e0197366.
Belda SS, Haile MT, Melku AT, Tololu AKJB. Modern contraceptive utilization and associated factors among married pastoralist women in Bale eco-region, Bale Zone, South East Ethiopia. BMC Health Serv Res. 2017;17(1):1–12.
Henok A, Takele EJE. Assessment of barriers to reproductive health service utilization among Bench Maji Zone Pastoralist Communities. Ethiop J Health Sci. 2017;27(5):523–30.
Mishra VK. Muslim/non-Muslim differentials in fertility and family planning in India. 2004.
Adhikari RJB. Demographic, socio-economic, and cultural factors affecting fertility differentials in Nepal. BMC Pregn Childbirth. 2010;10(1):1–11.
Balasubramanian KJAvjotGIoP, Economics PAvGASSDPTP. Hindu-Muslim differentials in fertility and population growth in India: role of proximate variables. journal of the Gokhale Institute of Politics and Economics, Poona (India)= Artha vijnana: Gokhale Artha Sastra Samstha Dvara Prakasita Traimesika Patrika. 1984;26:189–216.
Mistry M. THE ROLE OF RELIGION IN FERTILITY AND FAMILY PLANNING AMONG MUSLIMS IN INDIA. 1999.
Adioetomo SMJP. The role of religion in the construction of the small family norm in Java. Indonesia J Popul. 1995;1(1):107–29.
AbouZahr C, Wardlaw T. Antenatal care in developing countries: promises, achievements and missed opportunities-an analysis of trends, levels and differentials, 1990–2001. Antenatal care in developing countries: promises, achievements and missed opportunities-an analysis of trends, levels and differentials, 1990–20012003. p. 32.
Acknowledgements
We would like to acknowledge the MEASURE DHS program for providing us data set.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
The conception of the work, design of the work, acquisition of data, analysis, and interpretation of data was done by FMA. Data curation, drafting of the article, revising it critically for intellectual content, validation, and final approval of the version to be published was done by FMA, DC, DGB, MWM, AAK, AZA, and MHA. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out following relevant guidelines of the Demographic and Health Surveys (DHS) program. Informed consent was waived from the International Review Board of Demographic and Health Surveys (DHS) program data archivists after the consent paper was submitted to the DHS Program, a letter of permission to download the data set for this study. The data set was not shared or passed on to other bodies and has maintained its confidentiality.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aragaw, F.M., Chilot, D., Belay, D.G. et al. Spatial distribution and determinants of high-risk fertility behavior among reproductive-age women in Ethiopia. Trop Med Health 51, 14 (2023). https://doi.org/10.1186/s41182-023-00506-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41182-023-00506-y