
Abstract
Background
Dulaglutide is a once-weekly glucagon-like peptide-1 (GLP-1) receptor agonist approved for the treatment of type 2 diabetes mellitus (T2DM). However, the efficacy and safety of dulaglutide remain unclear in insulin-treated patients with T2DM on maintenance hemodialysis (HD).
Methods
Dulaglutide treatment was initiated, and the insulin dose was adjusted according to the needs of individual participants. Primary outcomes were changes in the mean and standard deviation (SD) of blood glucose (BG) levels and mean amplitude of glycemic excursions (MAGE) evaluated by continuous glucose monitoring (CGM) for six days, glycated albumin (GA), glycated hemoglobin (HbA1c), pre-dialysis blood glucose levels, and daily total insulin dose from the baseline over 24 weeks. Secondary outcomes were changes in treatment satisfaction and QOL levels from the baseline, measured by using the Diabetes Treatment Satisfaction Questionnaire (DTSQ) and the Diabetes Therapy-Related Quality of Life questionnaire (DTR-QOL) scores.
Results
The analysis was performed on the 12 participants who completed the study. The GA level (median − 1.8 [interquartile range − 6.6, − 0.3] %; p = 0.026) and daily total insulin dose (− 15.0 [− 24.5, − 9.4] U/day; p = 0.002) significantly decreased without increasing hypoglycemia (area over the glucose curve < 70 mg/dL: 0.0 [− 0.2, 0.0] mg·24 h/dl; p = 0.917). Four patients successfully withdrew from insulin therapy. The levels of HbA1c, SD of BG, and MAGE showed a decreasing tendency, but no significant improvement. Regarding treatment satisfaction and QOL, the total scores of DTSQ (8.0 [0.3, 12.5]; p = 0.041) and DTR-QOL (15.5 [− 1.8, 42.0]; p = 0.023) significantly improved.
Conclusion
Dulaglutide may help improve glycemic control, treatment satisfaction, and QOL without increasing hypoglycemia in insulin-treated patients with T2DM on maintenance HD.
Trial registration This study was registered with the University Hospital Medical Information Network-Clinical Trials Registry (UMIN-CTR) on October 11, 2016 (registration ID, UMIN000024283).
Similar content being viewed by others


Background
Dipeptidyl peptidase 4 (DPP-4) inhibitors, which are incretin-related drugs, have a lower risk of hypoglycemia, even in patients with renal failure and can be used relatively safely [1]. For this reason, it has been reported that DPP-4 inhibitors are also commonly used in dialysis patients, and their effectiveness has been reported [2, 3]. Dialysis patients, however, generally take a relatively large number of drugs, and so there are often problems with poor adherence [4, 5]. Insulin treatment is indispensable for strict control of blood glucose in dialysis patients, but it may affect quality of life (QOL), for example, frequent and painful injections and severe hypoglycemia [6, 7].
Dulaglutide is a weekly formulation of glucagon-like peptide-1 (GLP-1) receptor agonist launched in Japan in 2015. It is also an incretin-related drug like a DPP4 inhibitor. The features of dulaglutide are that it may be injected only once a week and that the injection is easy because there is no need to make a blank shot or match the number of units. These advantages of dulaglutide not only reduce the risk of misoperation and insulin dosing, but may also reduce the frequency of injection pain and ultimately improve adherence and QOL. In previous studies, the addition of a GLP-1 receptor agonist to insulin-using type 2 diabetic patients not only improved glycemic control without increasing the risk of hypoglycemia, but also their QOL also improved [8, 9]. There have been, however, few reports of studies in which dulaglutide was added to patients with maintenance hemodialysis who had type 2 diabetes and were taking insulin. Therefore, we conducted a study to add dulaglutide to adult patients on maintenance hemodialysis with type 2 diabetes who are currently receiving insulin therapy. We used continuous glucose monitoring (CGM) before and after the start of treatment to investigate the improvement of glycemic control and the reduction of insulin usage and further examined whether improvement of treatment adherence and improved QOL could be obtained.
Methods
Study participants
The study subjects were enrolled from November 2016 to August 2018 at seven dialysis facilities (Nagaoka Central General Hospital, Nagaoka City, Japan; Nagaoka Red Cross Hospital, Nagaoka City, Japan; Saiseikai Sanjo Hospital, Sanjo City, Japan; Nishikawa Municipal Hospital, Yamagata, Japan; Miura Internal Medicine Clinic, Shibata City, Japan; Maihira Clinic, Niigata City, Japan; Koyo Medical Clinic, Niigata City, Japan). The subjects were outpatients over the age of 20 who had been on hemodialysis for more than six months and had type 2 diabetes on insulin and were not using GLP-1 receptor agonist or DPP-4 inhibitors for more than eight weeks before the start of the study. The subjects who met any of the following criteria were excluded from the study: history of hypersensitivity to components of incretin-related drugs such as DPP-4 inhibitors and GLP-1 receptor agonists, severe ketosis, diabetic coma or precoma, active phase of serious infections, imminent or recent surgery, severe direct trauma, severe cardiac or hepatic dysfunction, pituitary or adrenal insufficiency, malnutrition, starvation, irregular dietary intake, insufficient or debilitated dietary intake, strenuous muscular exercise, excessive alcohol consumption, body mass index (BMI) < 18.5 kg/m2, pregnant, breastfeeding, may become pregnant, or any patient whom the attending physician deemed inappropriate for participation in this study.
Study design
This uncontrolled, open-label, exploratory study was approved by the institutional review boards of Niigata University and was performed in accordance with the principles embodied in the Declaration of Helsinki. All participants provided written informed consent. The Ethics Committee of the Niigata University School of Medicine approved the study (approval numbers: 2015–2573). Furthermore, the study was registered with the University Hospital Medical Information Network–Clinical Trials Registry (UMIN000024283).
Only a dose of 0.75 mg of dulaglutide is approved in Japan, and this was the dose used in this study. The attending physician appropriately reduced the insulin dose at the start of dulaglutide. At that time, the attending physician followed the protocol (Additional file 1) prepared with reference to the past reports on GLP-1 receptor agonists [10] based on the patient's glycemic control status. Subcutaneous injections of dulaglutide were given by the subject or the nurse at the end of a hemodialysis session at the beginning of the week. During the study period, the attending physician paid close attention to the onset of hypoglycemia and adjusted the insulin dose appropriately, that is, so that the blood glucose levels were within the range of 70–180 mg/dl as measured by self-monitoring of blood glucose (SMBG). In addition, as suggested by the Japanese Society of Dialysis, the blood glucose at the start of a hemodialysis session was controlled to less than 180–200 mg/dl. Regarding the adjustment of long-acting insulin usage, the insulin level was adjusted with reference to the protocol used in ATLAS study [11] (Additional file 2). During the period of this study, the attending physician did not add any oral anti-diabetic drugs. Drugs for complications other than anti-diabetic drugs (anti-platelet drugs, antihypertensive drugs, anti-dyslipidemia drugs, etc.) were not restricted, but the dose of the drug was not changed or added during the intervention period as much as possible.
Glucose levels were measured by a continuous glucose monitoring (CGM) system iPro2 (Medtronic MiniMed, USA) in a pre-observation period within one month before the start of dulaglutide. The following data also were collected during a day on hemodialysis at the beginning of the week: general blood biochemical measurements including glycated albumin (GA) and glycated hemoglobin (HbA1c) values, evaluation of body composition by impedance method (InBody) after a hemodialysis session, treatment satisfaction and QOL (the Diabetes Treatment Satisfaction Questionnaire [DTSQ] and the Diabetes Therapy-Related Quality of Life Questionnaire [DTR-QOL]). General blood biochemical measurements were performed monthly for 24 weeks after the start of dulaglutide. CGM and body composition analysis were performed four weeks after the start of dulaglutide. Twenty-four weeks after the start of dulaglutide, CGM, body composition analysis, and a questionnaire using DTSQ and DTR-QOL were conducted (Additional file 3).
The primary endpoints were: (i) changes in mean and standard deviation (SD) of blood glucose and glycemic variability using mean amplitude of glycemic excursions (MAGE) by CGM before and after the start of dulaglutide; (ii) changes in GA, HbA1c, and pre-dialysis blood glucose levels before and after the start of dulaglutide; and (iii) changes in total daily insulin usage before and after the start of dulaglutide. Secondary endpoints were: (i) changes in treatment satisfaction and QOL before and after the start of dulaglutide by DTR-QOL and DTSQ; (ii) changes in body composition using InBody (body fat mass, skeletal muscle mass) before and after the start of dulaglutide; and (iii) changes in interdialytic weight gain (IDWG) before and after the start of dulaglutide. Safety endpoints were: (i) incidence of serious adverse events associated with dulaglutide use and (ii) hypoglycemia rate (by comparison of area over the glucose curve < 70 mg/dL per 24 h [AOC < 70] in CGM before and after the use of dulaglutide).
Laboratory investigations
Body mass index (BMI) was calculated by dividing the average weight (kg) after HD by the square of height (m). Pre-HD venous blood samples were taken at the beginning of the week. General blood biochemical tests were analyzed in each facility's laboratory. GA and HbA1c were measured at SRL Co., Ltd. (Tokyo, Japan). Body composition was measured in a unified posture using a body composition analyzer (InBody470, InBodyJapan, Japan). Bioimpedance was measured for each of the five parts of the right arm, left arm, trunk, right leg, and left leg using these three frequencies: 5 kHz, 50 kHz, and 250 kHz. Body weight, body water, body fat mass, muscle mass, skeletal muscle mass (SMM), and body fat percentage were measured using the same body composition analyzer.
DTR-QOL consists of 29 questions and has four major domains (D): D1 is “burden on social activities and daily activities” (13 items); D2 is “anxiety and dissatisfaction with treatment” (eight items); D3 is “hypoglycemia” (four items); and D4 is “satisfaction with treatment” (four items). Answers were scored on a Likert-type scale ranging from 1 (strongly agree) to 7 (strongly disagree), but an inverted scale was used in questions 26–29, with 7 representing the highest quality of life score. The domain score is calculated by the total scale of each domain, and the higher the score, the higher the QOL [12]. DTSQ consists of eight questions and two different elements. The first element evaluates treatment satisfaction and consists of six questions (Q1, 4, 5, 6, 7, 8). Respectively, these six questions ask about “satisfaction with current treatment,” “flexibility,” “convenience,” “understanding of diabetes,” “recommend treatment to others,” and “willingness to continue.” The patient’s scores range from 0 (“very dissatisfied,” “very inconvenient”) to 6 (“very satisfied,” “very convenient”). The second element consists of two questions (Q2, 3), each scoring the burden of hyperglycemia and hypoglycemia from 0 (“none of the time”) to 6 (“most of the time”). Treatment satisfaction is evaluated by the sum of the scores of the six questions regarding the first factor; the higher the score, the higher the treatment satisfaction [13].
Continuous glucose monitoring
Patient glucose data were evaluated using the iPro 2 CGM system. The device was worn on a day of hemodialysis at the beginning of the week and removed the following week. When evaluating the data, we excluded the data on days of putting on and removing the device and used the data for a total of six days (Day 2–7) (Additional file 3). MAGE was calculated as the arithmetic mean difference between consecutive blood glucose peaks (between meals) and nadirs (between the peaks) when differences were > 1 standard deviation of the mean glucose value in the same 24 h period. We defined the range of blood glucose in time in range (TIR) as 70–180 mg/dL [14]. We also defined the glucose level in CGM from 0:00 to 6:00 as the nocturnal blood glucose level [15] and evaluated the nocturnal glucose control of two consecutive non-dialysis days over the weekend before and after the start of dulaglutide.
Statistical methods
Data are presented as median with interquartile range (IQR). The Wilcoxon signed-ranks test was used to compare the values before and after the start of dulaglutide and each measurement point. P values less than 0.05 were considered significant. All statistical analyses were performed using IBM SPSS Statistics for Windows ver. 21.0 (IBM Corp., Armonk, NY).
Results
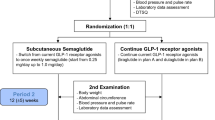
Fifteen patients agreed to the study, but one was hospitalized after obtaining consent and was excluded due to difficulty in following up, so fourteen patients started the study. One participant was eliminated after abdominal symptoms made it difficult for the patient to continue. In addition, another participant deviated from the protocol. The remaining 12 subjects who completed the study were the subjects of the present study (Fig. 1). The clinical background of the participants who completed the trial is shown in Table 1. The median age was 70.0 years, the median duration of diabetes was 25.5 years, and the median duration of dialysis was 4.3 years. One participant was taking α-glucosidase inhibitor. Regarding the diseases causing dialysis, one subject had an MPO-ANCA-related disease; all others had diabetic nephropathy. The median values of GA and HbA1c were 22.9% and 6.8%, respectively, and the median daily insulin usage was 24.5 units (Table 2).

Flowchart of study participants throughout the trial
The changes in each primary endpoint are shown in Table 2 and Fig. 2. After 24 weeks, change in GA was significant (median − 1.8 [IQR − 6.6, − 0.3] %; p = 0.026), and change in HbA1c (− 0.4 [− 1.2, 0.2] %; p = 0.172) showed an improving tendency. Insulin usage decreased (− 15.0 [− 24.5, − 9.4] U/day; p = 0.002) after six months, and four out of 12 patients (33.3%) were able to discontinue insulin use (Fig. 3 and Additional file 4). Furthermore, in the examination by CGM, the change in mean blood glucose level (− 18.8 [− 42.0, 17.2] mg/dl; p = 0.158) and the change in blood glucose variability showed an improving tendency as follows: SD of BG (− 10.6 [− 20.2, 5.9] mg/dl; p = 0.099), MAGE (− 21.7 [− 47.7, 14.1] mg/dl; p = 0.209), AUC > 180 (− 58.6 [− 141.0, 26.8] mg·24 h/dl; p = 0.117). The change in AOC < 70 was showing no significant change (0.0 [− 0.2, 0.0] mg·24 h/dl; p = 0.917) (Table 2). Although we also evaluated BG data using CGM with % coefficient of variation (− 2.0 [− 6.7, 2.8] %; p = 0.308) and TIR (16.1 [− 9.1, 29.5] %; p = 0.117), no significant differences were found (Additional file 5). In addition, we evaluated glycemic fluctuations during HD days, HD sessions, and six hours after HD session (Additional file 6), and there was a tendency for improvements in the levels of median SD of BG (− 5.9 [− 26.4, 6.6] mg/dl; p = 0.084) and MAGE (− 18.3 [− 66.7, 4.4] mg/dl; p = 0.084) on the dialysis days, although there was no clear significant difference in the levels of mean blood glucose. Furthermore, in an analysis on two consecutive non-dialysis days over the weekend before and at the end of the study, the change in nocturnal blood glucose levels between 0:00 and 6:00 was significant (− 22.8 [− 70.6, − 1.1] mg/dl; p = 0.023) (Fig. 4).

Changes in GA and HbA1c values during this study. GA and HbA1c values showed a tendency to decrease from four weeks after the start of the use of dulaglutide. Data are presented as median with an interquartile range. Δ indicates changes from baseline to each month. Number of subjects available for 0, 4, 8, 12, 16, 20, 24 week-measurements was 12, 10, 12, 10, 12, 11, and 12 for GA and 11, 11, 11, 11, 10, 11, and 9 for HbA1c, respectively. GA, glycated albumin; HbA1c, glycated hemoglobin

Changes in insulin dose during this study. Most participants have gradually reduced their insulin doses since the start of dulaglutide. Four out of 12 participants were able to stop using insulin

Daily variation of glucose levels in two consecutive non-dialysis days over the weekend. The nocturnal glucose level (median glucose level in CGM from 0:00 to 6:00) was significantly decreased during the study period (p = 0.023): median [IQR] values of the change in the nocturnal glucose level from 0 to 24 week were − 22.8 [− 70.6, − 1.1] mg/dl. CGM, continuous glucose monitoring; HD, hemodialysis; and IQR, interquartile range
Next, the changes in the secondary endpoints are shown in Table 3. Changes in BMI (− 0.4 [− 1.0, − 0.3] %; p = 0.003), fat ratio (− 4.8 [− 8.2, − 1.7] %; p = 0.022), and fat mass (− 2.6 [− 5.5, − 1.3] kg; p = 0.037) were indicating significant change. On the other hand, the change in SMM (0.5 [− 0.4, 1.6] kg; p = 0.285) and skeletal muscle mass indexes (SMI) (0.2 [− 0.2, 0.7] kg/m2; p = 0.203) was showing no significant change. Regarding treatment satisfaction evaluation, in terms of changes in DTSQ, convenience (1.0 [0.0, 3.0]; p = 0.039), likelihood of recommending the treatment to others (1.0 [1.0, 2.0]; p = 0.004), and continuation (1.0 [0.0, 3.0]; p = 0.026), scores were also significantly improved from the baseline, respectively. The total score was also significantly improved (8.0 [0.3, 12.5]; p = 0.041) from the baseline. The dissatisfaction scores for hyperglycemia (− 1.0 [− 4.0, 0.0]; p = 0.073) and hypoglycemia (− 0.5 [− 2.0, 0.0]; p = 0.065) tended to improve from the baseline, respectively. Regarding DTR-QOL, the total score improved (15.5 [− 1.8, 42.0]; p = 0.023) significantly from the baseline; in individual items, scores for the burden on social activities and daily life (10.5 [1.5, 54.3]; p = 0.013) and anxiety and burden of treatment (15.5 [− 3.8, 40.5]; p = 0.041) were significantly improved. Also, the score of hypoglycemia showed a tendency to improve (27.0 [− 12.8, 54.0]; p = 0.062) from the baseline.
Discussion
In this study, we added the GLP-1 receptor agonist dulaglutide to HD patients with type 2 diabetes who were on insulin treatment. We investigated whether this treatment could improve glycemic control and reduce insulin usage, treatment adherence, and QOL. Regarding blood glucose control, the GA value was significantly improved, and the mean blood glucose of CGM and SD, MAGE, and AUC > 180 showed a decreasing tendency. On the other hand, no significant change was observed in AUC < 70, and no exacerbation of hypoglycemia was observed. Insulin dose was also significantly reduced, and four of the fourteen patients were able to discontinue insulin use. Regarding changes in body composition, BMI, body fat percentage, and fat mass decreased significantly, but SMM did not decrease. Furthermore, regarding treatment satisfaction, improvement in total score was observed for both DTSQ and DTR-QOL.
One of the problems with diabetes treatment for hemodialysis diabetic patients is that the types of oral anti-diabetic agents that can be used are limited, and therefore insulin treatment is often required. There are, however, many cases where injecting insulin is difficult due to visual impairment and other complications; hypoglycemia is likely to occur due to the use of insulin [16]. Therefore, it is necessary to have a treatment method that enables good blood glucose control without increasing the risk of hypoglycemia, reduces the amount of insulin used and the frequency of injections, and obtains higher adherence. Dulaglutide, a GLP-1 receptor agonist, is a once-weekly formulation, is easy to use, and does not require adjustment of the number of units. Dulaglutide has been shown to be effective in non-HD patients with type 2 diabetes not only in glycemic control, but also in body composition changes, treatment satisfaction, and tolerability [17,18,19,20,21]. Regarding the tolerability of dulaglutide in patients with impaired renal function, it was reported that dulaglutide obtained glycemic control equivalent to insulin glargine in type 2 diabetic patients with chronic kidney disease stages 3–4 [22]. However, few reports targeted dialysis patients. Recently, the results of using dulaglutide in HD patients have been reported, showing improvement in glycemic control and changes in body composition [23, 24]. Yajima et al. reported that the addition of dulaglutide reduced GA and insulin use in hemodialysis patients taking insulin [23, 24]. Similar results were shown in this study, confirming the effectiveness of dulaglutide in glycemic control.
A major feature of this study was that it targeted HD patients undergoing insulin treatment and evaluated glycemic control for 24 weeks, which was relatively longer than previously reported using CGM. Furthermore, we were investigating changes in treatment satisfaction and QOL using DTSQ and DTR-QOL. Feng-fei Li et al. reported the changes in insulin dose to maintain glycemic control after 24 weeks of vildagliptin, a DPP-4 inhibitor, treatment for type 2 diabetes patients using insulin. In that report, subjects in the additional vildagliptin therapy group did not show a significant difference in the total insulin dose required to maintain glycemic control compared to the control group [25]. In our study, dulaglutide, which is the same incretin-related drug, significantly reduced insulin dose even in hemodialysis patients with type 2 diabetes, indicating that insulin use could be discontinued in some cases. For hemodialysis patients with type 2 diabetes who wish to discontinue insulin injections, the addition of GLP-1 receptor agonists may be better than DPP-4 inhibitors. On the other hand, Baptist et al. reported that when dulaglutide 1.5 mg or 0.75 mg was added to patients who were also taking oral anti-diabetic agents or insulin treatment, not only an improvement in HbA1c, but also a significant improvement in fasting blood glucose level were observed [26]. In addition, Johan et al. reported that the addition of dulaglutide to type 2 diabetes patients using insulin improved not only postprandial blood glucose, but also nocturnal blood glucose levels [27]. The CGM analysis of our study also showed improvement of nocturnal blood glucose levels on non-dialysis days. The nocturnal and postprandial blood glucose variability shown by CGM at 26 and 52 weeks in the report by Johan et al. was similar to our results. Regarding hypoglycemia, it has been reported that the use of GLP-1 receptor agonists such as liraglutide and dulaglutide in hemodialysis patients with type 2 diabetes did not show a significant increase in hypoglycemia [24, 28]. Before and after the use of dulaglutide in our study, there was no significant change in AOC < 70 mg · 24 h/dL, which indicates hypoglycemia. These results suggest that the addition of dulaglutide in patients on maintenance hemodialysis with type 2 diabetes on insulin may improve glycemic control without increasing the risk of hypoglycemia.
Takase et al. divided 31 non-dialysis type 2 diabetes patients using once-daily liraglutide into two groups, one that continued to use liraglutide and one that changed to once-weekly dulaglutide and continued treatment 12 weeks later, and they assessed treatment satisfaction by using DTSQ and DTR-QOL [29]. As a result, the dulaglutide group showed an improvement in the total DTSQ score compared to the liraglutide group, and the subscale score also showed a higher improvement in “convenience” and “flexibility” in the dulaglutide group than in the liraglutide group. In DTR-QOL, the total score of the dulaglutide group was significantly improved compared to that of the liraglutide group; significant improvement was observed in domain 1 and 2. In this study, we targeted hemodialysis patients, and both total DTSQ and DTR-QOL scores were also significantly improved; in the DTSQ subscale, there were significant improvements in “convenience,” “flexibility,” “recommend,” and “continue,” and in the domain of DTR-QOL, domains 1 and 2 were significantly improved. These were almost the same results as in the reports mentioned above. It has been suggested that in diabetic patients on insulin use, decreased insulin dose and injection frequency are closely associated with improved treatment satisfaction in patients [30, 31]. From the results of our study, it is considered that the treatment satisfaction in DTSQ and DTR-QOL improved due to the decrease in insulin amount and insulin injection frequency even in hemodialysis patients with type 2 diabetes.
In the above-mentioned report by Yajima et al., BMI, fat mass, SMM, and SMI were all decreased in changes in body composition. In our study, however, although BMI and fat mass decreased, there was no significant decrease in muscle mass. Regarding fat mass, GLP-1 has been reported to induce lipolysis by activating cyclic adenosine monophosphate (AMP) dependent protein kinase (PKA) and AMP-activated protein kinase (AMPK) in adipocytes [32]. It is possible that dulaglutide, a GLP-1 analog, enhanced the activation of PKA and AMPK, promoted lipolysis, and reduced BMI. On the other hand, regarding the decrease in SMM and SMI, Yajima et al. discussed the following factors that were likely to cause sarcopenia in these subjects: The median age of registered patients was higher than 65 years old; they had renal failure; the median BMI was 24 kg/m2, lower than in previous studies. The subjects in our study, however, were hemodialysis patients with an average age of 68.4 years and a BMI value of 24.7 kg/m2; under almost the same conditions, no decrease in SMM or SMI was observed. In previous papers, it was reported that GLP-1 receptor agonists also suppressed myostatin and muscular atrophy factors in vitro and in vivo, and by enhancing myogenic factors through GLP-1 receptor-mediated signaling pathways, it improved muscle atrophy [33]. It was also reported that when dulaglutide was used for 12 weeks in non-dialysis type 2 diabetic patients and when body composition was measured before and after treatment, BMI was significantly reduced, but SMM was not changed [34]. Because there are reports that about 40% of dialysis patients have sarcopenia and type 2 diabetes can also cause sarcopenia [35], further studies are needed on changes in muscle mass in dialysis patients due to the use of dulaglutide.
There are several limitations in this study. The first is that the number of subjects was small. The second was that walking speed and grip strength included among the diagnostic criteria for sarcopenia were not evaluated. The third is that this study was exploratory and not a randomized controlled trial. Therefore, in order to verify the results of this study, a larger-scale randomized controlled trial will be required.
Conclusions
We added the GLP-1 receptor agonist dulaglutide to patients on maintenance hemodialysis who had type 2 diabetes on insulin, and 24 weeks after the start of use, we examined changes in glycemic indices including CGM-based blood glucose variability, treatment satisfaction, and QOL. Regarding glycemic control, the GA level and daily total insulin dose significantly decreased without increasing hypoglycemia. Further improvement in treatment satisfaction and QOL was also observed. It was suggested that dulaglutide may help improve glycemic control, treatment satisfaction, and QOL in patients with type 2 diabetes who require dialysis without increasing the risk of hypoglycemia with insulin treatment.
Availability of data and materials
All data generated or analyzed during this study are included in this article.
References
Nakamura Y, Hasegawa H, Tsuji M, Udaka Y, Mihara M, Shimizu T, et al. Diabetes therapies in hemodialysis patients: Dipeptidase-4 inhibitors. World J Diabetes. 2015;6(6):840–9.
Wada N, Mori K, Nakagawa C, Sawa J, Kumeda Y, Shoji T, et al. Improved glycemic control with teneligliptin in patients with type 2 diabetes mellitus on hemodialysis: evaluation by continuous glucose monitoring. J Diabetes Complications. 2015;29(8):1310–3.
Terawaki Y, Nomiyama T, Takahashi H, Tsutsumi Y, Murase K, Nagaishi R, et al. Efficacy of dipeptidyl peptidase-4 inhibitor linagliptin in patients with type 2 diabetes undergoing hemodialysis. Diabetol Metab Syndr. 2015;7:44.
Kothawala P, Badamgarav E, Ryu S, Miller RM, Halbert RJ. Systematic review and meta-analysis of real-world adherence to drug therapy for osteoporosis. Mayo Clin Proc. 2007;82(12):1493–501.
Lee A, Song X, Khan I, Belozeroff V, Goodman W, Fulcher N, et al. Association of cinacalcet adherence and costs in patients on dialysis. J Med Econ. 2011;14(6):798–804.
Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, Davis M, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977–86.
Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837–53.
Ishii H, Niiya T, Ono Y, Inaba N, Jinnouchi H, Watada H. Improvement of quality of life through glycemic control by liraglutide, a GLP-1 analog, in insulin-naive patients with type 2 diabetes mellitus: the PAGE1 study. Diabetol Metab Syndr. 2017;9:3.
Lind M, Jendle J, Torffvit O, Lager I. Glucagon-like peptide 1 (GLP-1) analogue combined with insulin reduces HbA1c and weight with low risk of hypoglycemia and high treatment satisfaction. Prim Care Diabetes. 2012;6(1):41–6.
Lane W, Weinrib S, Rappaport J, Hale C. The effect of addition of liraglutide to high-dose intensive insulin therapy: a randomized prospective trial. Diabetes Obes Metab. 2014;16(9):827–32.
Group AS. Titration of insulin glargine in patients with type 2 diabetes mellitus in Asia: physician- versus patient-led? Rationale of the Asian Treat to Target Lantus Study (ATLAS). Diabetes Technol Ther. 2011;13(1):67–72.
Mita T, Hiyoshi T, Yoshii H, Chimori H, Ikeda K, Shimizu M, et al. The effect of linagliptin versus metformin treatment-related quality of life in patients with type 2 diabetes mellitus. Diabetes Ther. 2019;10(1):119–34.
Saisho Y. Use of diabetes treatment satisfaction questionnaire in diabetes care: importance of patient-reported outcomes. Int J Environ Res Public Health. 2018;15(5):947.
Battelino T, Danne T, Bergenstal RM, Amiel SA, Beck R, Biester T, et al. Clinical targets for continuous glucose monitoring data interpretation: recommendations from the international consensus on time in range. Diabetes Care. 2019;42(8):1593–603.
Kawaguchi Y, Sawa J, Kumeda Y. Efficacy and safety of tofogliflozin and ipragliflozin for patients with type-2 diabetes: a randomized crossover study by flash glucose monitoring. Diabetes Ther. 2020;11(12):2945–58.
Abbatecola AM, Maggi S, Paolisso G. New approaches to treating type 2 diabetes mellitus in the elderly: role of incretin therapies. Drugs Aging. 2008;25(11):913–25.
Giorgino F, Benroubi M, Sun JH, Zimmermann AG, Pechtner V. Efficacy and safety of once-weekly dulaglutide versus insulin glargine in patients with type 2 diabetes on metformin and glimepiride (AWARD-2). Diabetes Care. 2015;38(12):2241–9.
Da Porto A, Casarsa V, Colussi G, Catena C, Cavarape A, Sechi L. Dulaglutide reduces binge episodes in type 2 diabetic patients with binge eating disorder: a pilot study. Diabetes Metab Syndr. 2020;14(4):289–92.
Reaney M, Yu M, Lakshmanan M, Pechtner V, van Brunt K. Treatment satisfaction in people with type 2 diabetes mellitus treated with once-weekly dulaglutide: data from the AWARD-1 and AWARD-3 clinical trials. Diabetes Obes Metab. 2015;17(9):896–903.
Pozzilli P, Norwood P, Jódar E, Davies MJ, Ivanyi T, Jiang H, et al. Placebo-controlled, randomized trial of the addition of once-weekly glucagon-like peptide-1 receptor agonist dulaglutide to titrated daily insulin glargine in patients with type 2 diabetes (AWARD-9). Diabetes Obes Metab. 2017;19(7):1024–31.
Kaneko S, Oura T, Matsui A, Shingaki T, Takeuchi M. Efficacy and safety of subgroup analysis stratified by baseline HbA1c in a Japanese phase 3 study of dulaglutide 0.75 mg compared with insulin glargine in patients with type 2 diabetes. Endocr J. 2017;64(12):1165–72.
Tuttle KR, Lakshmanan MC, Rayner B, Busch RS, Zimmermann AG, Woodward DB, et al. Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7): a multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol. 2018;6(8):605–17.
Yajima T, Yajima K, Takahashi H, Yasuda K. The effect of dulaglutide on body composition in type 2 diabetes mellitus patients on hemodialysis. J Diabetes Complic. 2018;32(8):759–63.
Yajima T, Yajima K, Hayashi M, Takahashi H, Yasuda K. Improved glycemic control with once-weekly dulaglutide in addition to insulin therapy in type 2 diabetes mellitus patients on hemodialysis evaluated by continuous glucose monitoring. J Diabetes Complic. 2018;32(3):310–5.
Li FF, Shen Y, Sun R, Zhang DF, Jin X, Zhai XF, et al. Effects of vildagliptin add-on insulin therapy on nocturnal glycemic variations in uncontrolled type 2 diabetes. Diabetes Ther. 2017;8(5):1111–22.
Gallwitz B, Dagogo-Jack S, Thieu V, Garcia-Perez LE, Pavo I, Yu M, et al. Effect of once-weekly dulaglutide on glycated haemoglobin (HbA1c) and fasting blood glucose in patient subpopulations by gender, duration of diabetes and baseline HbA1c. Diabetes Obes Metab. 2018;20(2):409–18.
Jendle J, Testa MA, Martin S, Jiang H, Milicevic Z. Continuous glucose monitoring in patients with type 2 diabetes treated with glucagon-like peptide-1 receptor agonist dulaglutide in combination with prandial insulin lispro: an AWARD-4 substudy. Diabetes Obes Metab. 2016;18(10):999–1005.
Osonoi T, Saito M, Tamasawa A, Ishida H, Tsujino D, Nishimura R, et al. Effect of hemodialysis on plasma glucose profile and plasma level of liraglutide in patients with type 2 diabetes mellitus and end-stage renal disease: a pilot study. PLoS ONE. 2014;9(12):e113468.
Takase T, Nakamura A, Yamamoto C, Nomoto H, Miya A, Dannoura M, et al. Improvement in treatment satisfaction after switching from liraglutide to dulaglutide in patients with type 2 diabetes: A randomized controlled trial. J Diabetes Investig. 2019;10(3):699–705.
Miya A, Nakamura A, Miyoshi H, Cho KY, Nagai S, Kurihara Y, et al. Satisfaction of switching to combination therapy with lixisenatide and basal insulin in patients with type 2 diabetes receiving multiple daily insulin injection therapy: a randomized controlled trial. J Diabetes Investig. 2018;9(1):119–26.
Ishii H, Anderson JH, Yamamura A, Takeuchi M, Ikeda I. Improvement of glycemic control and quality-of-life by insulin lispro therapy: assessing benefits by ITR-QOL questionnaires. Diabetes Res Clin Pract. 2008;81(2):169–78.
Kato H, Nagai Y, Ohta A, Tenjin A, Nakamura Y, Tsukiyama H, et al. Effect of sitagliptin on intrahepatic lipid content and body fat in patients with type 2 diabetes. Diabetes Res Clin Pract. 2015;109(1):199–205.
Hong Y, Lee JH, Jeong KW, Choi CS, Jun HS. Amelioration of muscle wasting by glucagon-like peptide-1 receptor agonist in muscle atrophy. J Cachexia Sarcopenia Muscle. 2019;10(4):903–18.
Seko Y, Sumida Y, Tanaka S, Mori K, Taketani H, Ishiba H, et al. Effect of 12-week dulaglutide therapy in Japanese patients with biopsy-proven non-alcoholic fatty liver disease and type 2 diabetes mellitus. Hepatol Res. 2017;47(11):1206–11.
Mori K, Nishide K, Okuno S, Shoji T, Emoto M, Tsuda A, et al. Impact of diabetes on sarcopenia and mortality in patients undergoing hemodialysis. BMC Nephrol. 2019;20(1):105.
Acknowledgements
The authors thank Ryota Kobayashi, Koichi Komochi, Taeko Endo, Nanako Sugita, Maiko Daisaka, Ryohei Kaseda for technical assistance; Emiko Kono, Aya Takeyama, Takayoshi Miura, Hirokazu Fujikawa, Masahiro Sugai, Hajime Yamazaki, Hiroki Sasage, Ikuo Aoike, Yoshiaki Miura for recruiting and following the subjects in the study. We also thank Shido Co., Ltd. for Medical English editing.
Funding
No funding or sponsorship was received for this study.
Author information
Authors and Affiliations
Contributions
DU, MH, HK, NT, YY, YS, and AS were responsible for the conception and design of the study. DU was the chief investigator and was responsible for data analysis. MH, HK, and NT were responsible for data analysis. DU, MH, and HK were responsible for data acquisition. DU, MH, HK, YY, YS, and AS were responsible for data interpretation. DU and MH were responsible for drafting the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of the Niigata University School of Medicine approved the study (approval numbers: 2015-2573). Written informed consent was obtained from each participant.
Consent for publication
Not applicable.
Competing interests
MH and AS received lecture fees and donations for research from Eli Lilly Japan K. K. and Sumitomo Dainippon Pharma Co., Ltd.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Insulin reduction protocol at the start of the study.
Additional file 2
. Insulin reduction protocol after starting dulaglutide.
Additional file 3
. Outline of the trial protocol.
Additional file 4
. Type of dialysis, dialysate, and changes in insulin dose.
Additional file 5
. %CV and TIR in CGM.
Additional file 6
. The blood glucose profiles on HD day in CGM.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ugamura, D., Hosojima, M., Kabasawa, H. et al. An exploratory clinical trial on the efficacy and safety of glucagon-like peptide-1 receptor agonist dulaglutide in patients with type 2 diabetes on maintenance hemodialysis. Ren Replace Ther 8, 26 (2022). https://doi.org/10.1186/s41100-022-00409-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-022-00409-4