
Abstract
Background
In addition to achieving good glycemic control, diabetes care management aims to improve the quality of life (QOL) in patients. Treatment-associated difficulties and side effects frequently cause deterioration in QOL. Liraglutide, a GLP-1 receptor agonist, is a novel injection drug that promotes insulin secretion. It is a user-friendly, once-daily injection with fewer hypoglycemic events. In this study, we aimed to examine the effect of liraglutide therapy on QOL in patients.
Methods
In total, 304 insulin- and liraglutide-naïve patients with type 2 diabetes were enrolled in this observational study; they received liraglutide therapy for 12 weeks. The main outcome measure was change in QOL from baseline, which was assessed using diabetes therapy-related QOL (DTR-QOL).
Results
At week 12, liraglutide significantly decreased HbA1c levels (8.7 ± 1.5 vs. 7.5 ± 1.3, p < 0.001) and BMI (27.9 ± 5.3 vs. 27.3 ± 5.2, p < 0.001). According to the QOL scores, although the treatment modality had changed from non-injection to injection therapy, liraglutide improved patient satisfaction with treatment. Significant correlations were found between change in HbA1c level and satisfaction with treatment, as well as between change in body weight and burden on social and daily activities, anxiety and dissatisfaction with treatment, and hypoglycemia.
Conclusions
Liraglutide significantly improved glycemic control and reduced the body weight without deteriorating QOL in obese patients with type 2 diabetes.
Trial registration UMIN-CTR: UMIN000007159
Similar content being viewed by others


Background
The prevalence of type 2 diabetes mellitus (T2DM) has been increasing worldwide. Japan is one of the countries with the highest prevalence rates in the world [1], which was promoted by the adoption of high-fat westernized diet patterns and sedentary lifestyle due to the rise of automation. The persistent elevation of blood glucose level causes microvascular and life-threatening macrovascular complications resulting in low quality of life (QOL) in patients with diabetes.
Recent evidence suggests that good glycemic control is necessary to prevent diabetic complications. However, many patients with T2DM have difficulty achieving and maintaining glycemic control. One of the obstacles is that patients have to stick to a daily routine for a long period to maintain good glycemic control [2]. Another possible barrier includes the side effects of medical treatment including hypoglycemia or weight gain or both, which may arouse anxiety [3], decrease motivation, and lower the QOL [4] in patients. Patients often fail to adhere to suitable diabetes treatment because of these psychological stressors, which lead to a downward spiral of neglected diabetes care [5]. In particular, most patients have a negative attitude towards insulin injection [6], and consider it a critical-state treatment [7]. They become hesitant about the initiation of insulin therapy despite the fact that it is a reliable means to control blood glucose [8], which may result in late insulin initiation [9]. Thus, it is very important to attain good glycemic control without reducing patient motivation or QOL.
Liraglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist. As GLP-1 receptor agonists promote insulin secretion in a blood glucose-dependent fashion, they cause fewer hypoglycemic episodes in comparison with sulfonylureas [10]. In addition, they can achieve long-term glycemic control with only one shot per day [11]. GLP-1 receptor agonists have other beneficial effects, such as suppression of appetite, delayed gastric emptying, and weight loss. These favorable features of liraglutide are expected to solve many of the unmet medical needs associated with T2DM treatment. However, it has been suggested that patients and physicians may be reluctant to implement liraglutide treatment because GLP-1 receptor agonists are injection drugs [4]. Therefore, it is important to elucidate the impact of liraglutide therapy on clinical parameters and QOL as well as its side effects in patients with T2DM.
We aimed to examine the effects of liraglutide on glycemic control, body weight, and QOL score in obese Japanese patients with T2DM in patient’s psychological attitude and glycemic control effectiveness by GLP-1 (PAGE1) study.
Methods
Research overview
We conducted a prospective, multicenter, pre-post observational study to examine the effect of liraglutide on QOL in Japanese patients with T2DM from February 2012 to September 2013 at 66 medical institutions in Japan listed in the Additional file 1. The inclusion criteria were (1) type 2 diabetes, (2) no prior use of insulin or liraglutide, and (3) aged 15 years and older. Patients with malignant tumors and pregnant or nursing women were excluded from this study. At the start of the study, only patients with dietary therapy, physical therapy, or sulfonylurea treatment were allowed to enroll because only they were allowed to use liraglutide under insurance coverage in Japan. During the course of the study, oral hypoglycemics other than sulfonylurea were reimbursed. Therefore, patients using those drugs were enrolled at later time points.
No pre-specified initiation or titration protocol for liraglutide was used. The participating physicians were allowed to determine the initial dose, maintenance dose, and timing of liraglutide administration by considering the patient’s condition and side effects. Clinical and laboratory parameters and diabetes therapy-related QOL (DTR-QOL) scores [12] were measured before (at baseline) and 12 weeks after the initiation of liraglutide therapy. In addition, at baseline and week 12, the hypoglycemic episodes that the patients experienced in the preceding four weeks were self-reported using the DTR-QOL questionnaire. The frequency of adverse events was evaluated to assess the safety of liraglutide therapy. The primary outcome measure was the change of DTR-QOL total score from baseline. Additionally, the correlation between changes in HbA1c and DTR-QOL scores was evaluated. Secondarily, correlations between changes in weight and DTR-QOL scores and those between changes in random blood glucose levels and DTR-QOL scores were evaluated.
The study protocol was registered with the University Hospital Medical Information Network (UMIN-CTR: UMIN000007159) prior to the commencement of the study. We adhered to the “Ethical Guidelines for Clinical Studies” issued by the Japanese government after receiving permission from the ethical committees at each of the participating medical facilities, and this study was conducted in accordance with the ethical standards laid down in the Declaration of Helsinki and its later amendments. All personal information was anonymized. The participation of patients with diabetes was obtained through an opt-out methodology. The patients were informed about the study and the ability to opt out via a poster. However, a written informed consent was given if directed by the institutional review board. To ensure data quality in this study, we contracted external entities for data collection, management, and statistical analysis.
DTR-QOL questionnaire
We used the DTR-QOL questionnaire for evaluating QOL. The reliability and validity of the questionnaire was verified psychometrically [12], and it can be used to assess all modalities of diabetic treatment including injections. The self-administered questionnaire comprises 29 questions, and the patient answers each question using the 7-point Likert scale ranging from “Strongly disagree” (−7) to “Strongly agree” (1). The score of each item was reversed so that “7” represented the highest QOL. When calculating the scores for DTR-QOL questions 26–29, the rating scores were reversed such that a higher score indicated better QOL. The assessment covers each of the following four domains: D1 “Burden on social activities and daily activities,” D2 “Anxiety and dissatisfaction with treatment,” D3 “Hypoglycemia,” and D4 “Satisfaction with treatment.” By comparing the DTR-QOL scores before and after initiation of a new treatment, the influence and effects of the new treatment on patient QOL can be assessed quantitatively. The total score and domain scores were converted to a scale of 0–100 as described previously [12]. The patients filled out the DTR-QOL questionnaire by themselves in private, to avoid any influence of physicians and medical care providers.
Statistical analysis
Patients were excluded from the analysis if data at baseline, week 12, or both time points were missing. We further excluded those who dropped out of the study or stopped liraglutide therapy owing to adverse effects. For the analysis of hypoglycemic events, we used all data, even when data for either of the two time points were missing. We calculated the total score and scores for each domain at both baseline and week 12, and compared them using a paired t test. All correlation analyses were performed using Spearman’s rank correlation coefficient. We conducted stratification analyses for DTR-QOL scores. DTR-QOL scores were compared using Student’s t test between the first and fourth groups stratified by quartiles of changes in HbA1c or body weight. The Wilcoxon signed-rank test was used to compare the scores of each question of the DTR-QOL questionnaire at baseline and week 12. The frequency of hypoglycemic events was compared between baseline and week 12 using the Chi squared test, and the number of hypoglycemic events per patient was compared using the Wilcoxon rank-sum test. A paired t test was used for comparing the clinical and biochemical characteristics at both time points.
Based on a previous study [12], power analysis was performed to detect a change of 7 points in the DTR-QOL total score (10% improvement), with two-sided alpha of 5% and beta of 7.5%. Assuming a DTR-QOL total score at baseline ±SD of 70 ± 15 and a dropout rate of 30%, we calculated that at least 300 patients were needed for this study. All statistical tests were two-sided with an alpha level of 0.05 and performed using the SAS 9.3 software.
Results
Subject characteristics
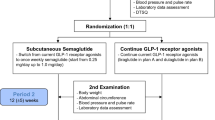
In total, 304 Japanese patients were enrolled in this study. After enrollment, five cases were found to meet the exclusion criteria, ten cases dropped out, 43 cases did not have questionnaire data either at baseline or week 12, and 42 cases deviated from the allowance period at week 12. Thus, we used data from 204 cases for analyses (Fig. 1). The ten dropouts included three patients who stopped hospital visits and seven who dropped out because of adverse events: four cases presented gastrointestinal symptoms (constipation, loss of appetite, gastritis, and bloating), one case showed hypersensitivity (hives), one showed hyperglycemia, and one showed depression. No dropouts due to hypoglycemia were noted. The mean age was 59.4 ± 12.3 years, mean weight was 73.9 ± 17.0 kg, mean BMI (body mass index) was 27.9 ± 5.3 kg/m2, mean HbA1c was 8.7 ± 1.5% (NGSP, National Glycohemoglobin Standardization Program; 71.6 ± 16.7 mmol/mol), and the mean duration of diabetes was 115.0 ± 88.8 months (9.6 ± 7.4 years). In total, 55.9% of subjects used combination therapy with sulfonylurea during this study (Table 1). The concomitant drugs used by these patients at baseline and week 12 are shown in Table 2, which indicated that their medication was not changed within 12 weeks. Concerning the dose of liraglutide, 91.8% of the patients started 0.3 mg/day at baseline, and 77.0% of the patients received 0.9 mg/day after 12 weeks (Table 3).

Flowchart of selection of patients with T2DM for the analysis
Effects of liraglutide on clinical and biochemical parameters, and incidence of hypoglycemia
The clinical and biochemical parameters at the two evaluated time points are shown in Table 4. The HbA1c change was −1.2 ± 0.1% (−13.0 ± 1.2 mmol/mol), demonstrating a significant improvement in glycemic control (p < 0.001). Body weight and BMI were significantly decreased (p < 0.001 for both) by −1.4 ± 0.3 kg and −0.5 ± 0.1 kg/m2, respectively. Significant decreases were also observed in total cholesterol (−8.4 ± 2.8 mg/dL [−0.2 ± 0.07 mmol], p = 0.003), uric acid (−0.2 ± 0.1 mg/dL [−11.9 ± 5.9 mmol], p = 0.025), and HDL-C (−1.2 ± 0.6 mg/dL [−0.03 ± 0.02 mmol], p = 0.041).
The proportion of patients experiencing hypoglycemic events during the 4 weeks prior to baseline and week 12 were 13.8 and 15.5% (p = 0.758), respectively. The number of hypoglycemic events per patient at both time points was 8.1 ± 8.5 and 5.3 ± 7.4 (p = 0.150), respectively (Additional file 2: Figure S1).
Effects of liraglutide on DTR-QOL scores
Changes in DTR-QOL total score and each of the four domain scores are shown in Table 5. The total score of 198 subjects at baseline was 61.9 ± 16.2, and it was significantly improved to 69.7 ± 16.8 (p < 0.001) at week 12. Significant improvement was also seen in all four domains (D1–D4; Table 5). The effect size [13] for the total score was 0.48. The effect sizes for the scores in domains D1, D2, D3, and D4 were 0.28, 0.48, 0.23, and 0.61, respectively. The effect size was the largest for D4, followed by total score and D2, which reflected moderate effect on QOL [14]. When assessing the effect for each individual question of the questionnaire, a significant improvement was observed for 24 of 29 questions (Table 6). However, significant decreases were found in the scores for Q12, “Pain due to my current diabetes treatment is uncomfortable,” and Q13, “Gastrointestinal symptoms (nausea, passing gas, diarrhea, abdominal pain) due to my current diabetes treatment are uncomfortable.” No significant changes were found for the following three questions: Q5, “It is a burden getting up at a certain time every morning for my current diabetes treatment,” Q15, “I worry about low blood glucose due to my current diabetes treatment,” and Q25, “I am concerned that if I continue my current diabetes treatment, the efficacy (effectiveness) may diminish.”
Correlations between changes in DTR-QOL scores and changes in HbA1c, body weight, and random blood glucose
We found a significant correlation between change in DTR-QOL total score and change in body weight (ρ = −0.24, p < 0.001), but not with change in HbA1c (ρ = −0.12, p = 0.102) and random blood glucose (ρ = 0.03, p = 0.702). With regard to changes in the four DTR-QOL domain scores, we detected significant correlations for the following parameters: HbA1c and D4 (ρ = −0.22, p = 0.002), and weight and D1 (ρ = −0.18, p = 0.010), D2 (ρ = −0.20, p = 0.006), and D3 (ρ = −0.22, p = 0.002; Additional file 3: Table S1). Stratification by HbA1c revealed significant changes between the first and fourth quartiles not only in D4 score (p = 0.008), but also in the total score (p = 0.027; Fig. 2). Similarly, significant differences were found in total, D1, D2, and D3 scores between the groups of the first and fourth quartiles of weight change (p = 0.003, 0.012, 0.019, 0.016, respectively).

Changes of DTR-QOL scores in each quartile of the change of HbA1c or body weight. The changes in the total DTR-QOL score and each domain score between baseline and 12 weeks after the initiation of liraglutide in each quartile of change in HbA1c and body weight are shown
Discussion
In this study, we showed the efficacy of liraglutide, and its influence on changes in DTR-QOL scores, and the correlations between changes in HbA1c/body weight/random blood glucose levels and DTR-QOL scores in T2DM patients who did not have prior experience with injection therapy. Liraglutide therapy decreased HbA1c level and body weights, and improved patient QOL as evidenced by the increase in scores for 24 of 29 questions, covering more than 82% of the DTR-QOL questionnaire.
When compared to patients who planned to start first-time insulin therapy [15] or those using oral hypoglycemic agents (OHA) alone [16], the following features were observed in this cohort: better glycemic control than patients considering insulin injections [15], but not better than those using OHA alone [16]; younger; shorter duration of T2DM; and higher BMI [19]. With regard to high BMI, obese T2DM patients with poor glycemic control in OHA therapy seemed to have been selected as candidates for this study in the hope of weight loss via liraglutide [17]. As expected, we observed a significant reduction in weight, BMI, and HbA1c at 12 weeks after liraglutide initiation. Notably, all four domains in DTR-QOL as well as the total score improved, which was rather unexpected because once-daily self-injection of liraglutide was supposed to pose a burden for patients or negatively influence their QOL [18]. We speculate that the improvement in clinical parameters by the liraglutide treatment changed the patients’ perception of T2DM treatment from negative to positive, even though they required additional self-injection of liraglutide, as is clear from Table 4 and Fig. 2. In other words, the difficulties of daily medication and additional liraglutide injection were overruled by the satisfaction associated with the beneficial outcomes generated by liraglutide. Another possibility is that patients felt that injection therapy turned out easier than expected. However, patients reported decreased QOL concerning side effects of liraglutide injection such as pain due to self-injection (Q12) and gastrointestinal symptoms (Q13). These results seem logical because gastrointestinal symptoms are well-known side effects of the drug, and the patients enrolled in our study were first-time users of self-injection therapy. Accordingly, we believe that the results of the DTR-QOL questionnaire represent not only subjective reality, but also objective reality in patients who started liraglutide treatment.
Among the four domains of DTR-QOL, marked improvements were observed for D2 (anxiety and dissatisfaction with treatment) and D4 (satisfaction with treatment), reflecting the achievement of satisfaction with improved clinical parameters. In particular, significantly improved scores were confirmed for all four questions in D4, indicating that patients with liraglutide treatment were satisfied and confident about glycemic control. A significant correlation was observed between the change in HbA1c and D4 score (ρ = −0.22, p = 0.002). Similarly, previous studies have demonstrated a correlation between changes in QOL score and HbA1c [19], with similar correlation coefficients [20, 21]. Furthermore, quartile-stratified analysis showed a large difference between groups of the first and fourth quartiles of change in HbA1c (Fig. 2), suggesting an association between the change of HbA1c and D4.
The combination of liraglutide therapy with OHA treatment was expected to increase the risk and fear of hypoglycemic events. In contrast, it resulted in the improvement of D3 (hypoglycemia). However, the number of patients who experienced hypoglycemic events, and the number of hypoglycemic events per patient did not change after the initiation of liraglutide therapy. We consider that the increase in D3 score was because of the improvement in clinical parameters without a rise in hypoglycemic events.
Weight change was negatively correlated with changes in the DTR-QOL total score and D1–D3, indicating that the greater the weight loss, the higher the QOL. Changes in these scores were as high as 8.6–14.8 in the first quartile groups of body weight change and as low as 0.8–4.6 in the fourth quartile groups (Fig. 2), strongly supporting the association between increase of QOL and body weight reduction.
There are several limitations to this study. First, it was a single-arm, pre-post observational study without control arm. Owing to this limitation, we do not know whether the results obtained include a placebo effect. A subset of patients might lose weight in response to the self-injection of placebo, and weight loss alone (independent of treatment) could provide combined improvement in HbA1c and QOL indicators seen in the study. Second, we excluded the data of 43 patients for whom we did not have data at both baseline and week 12. Therefore, it is difficult to extrapolate the findings of this study to all T2DM patients. Nonetheless, this study demonstrated that the injection of liraglutide along with OHA treatment reduced the body weight, BMI, and HbA1c level, and improved QOL, except for the gastrointestinal symptoms and pain associated with liraglutide injection, in obese T2DM patients. Physicians sometimes hesitate to initiate the use of injection therapies. However, this study revealed that self-injection does not necessarily deteriorate the patient’s QOL. Based on the routine subjective assessment of patient QOL, patients and physicians can select better treatment options.
Conclusions
In conclusion, liraglutide is an effective treatment option for obese T2DM patients, and it helps in reducing body weight and improving glycemic control without deteriorating QOL.
Abbreviations
- QOL:
-
quality of life
- DTR-QOL:
-
diabetes therapy-related QOL
- BMI:
-
body mass index
- T2DM:
-
type 2 diabetes mellitus
- NGSP:
-
National Glycohemoglobin Standardization Program
References
International Diabetes Federation. IDF diabetes atlas. 6th ed. Brussels: International diabetes federation; 2013.
Delahanty LM, Halford BN. The role of diet behaviors in achieving improved glycemic control in intensively treated patients in the diabetes control and complications trial. Diabetes Care. 1993;16:1453–8.
The DCCT Research Group. Epidemiology of severe hypoglycemia in the diabetes control and complications trial. Am J Med. 1991;90:450–9.
Rombopoulos G, Hatzikou M, Latsou D, Yfantopoulos J. The prevalence of hypoglycemia and its impact on the quality of life (QoL) of type 2 diabetes mellitus patients (The HYPO Study). Hormones (Athens). 2013;12:550–8.
Polonsky WH, Anderson BJ, Lohrer PA, et al. Assessment of diabetes-related distress. Diabetes Care. 1995;18:754–60.
Hunt LM, Valenzuela MA, Pugh JA. NIDDM patients’ fears and hopes about insulin therapy. The basis of patient reluctance. Diabetes Care. 1997;20:292–8.
Ratzmann KP. The psychological aspects of diabetics with the secondary failure of sulfonylurea therapy. Dtsch Med Wochenschr. 1991;116:87–90.
Nathan DM, Buse JB, Davidson MB, et al. Management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2006;29:1963–72.
Ishii H, Iwamoto Y, Tajima N. An exploration of barriers to insulin initiation for physicians in Japan: findings from the diabetes attitudes, wishes and needs (DAWN) Japan study. PLoS ONE. 2012;7:e36361.
Seino Y, Rasmussen MF, Zdravkovic M, Kaku K. Dose-dependent improvement in glycemia with once-daily liraglutide without hypoglycemia or weight gain: a double-blind, randomized, controlled trial in Japanese patients with type 2 diabetes. Diabetes Res Clin Pract. 2008;81:161–8.
Inoue K, Maeda N, Fujishima Y, et al. Long-term impact of liraglutide, a glucagon-like peptide-1 (GLP-1) analogue, on body weight and glycemic control in Japanese type 2 diabetes: an observational study. Diabetol Metab Syndr. 2014;6:95.
Ishii H. Development and psychometric validation of the diabetes therapy-related QOL (DTR-QOL) questionnaire. J Med Econ. 2012;15:556–63.
Fayers P, Machin D. Quality of life: assessment, analysis and interpretation. Chichester: Wiley; 2000.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: L Erlbaum Associate, Erlbaum; 1988.
Ishii H, Iwase M, Seino H, et al. Assessment of quality of life in patients with type 2 diabetes mellitus before and after starting biphasic insulin aspart 30 (BIAsp 30) therapy: IMPROVE study in Japan. Curr Med Res Opin. 2011;27:643–50.
Oishi M, Yamazaki K, Okuguchi F, et al. Changes in oral antidiabetic prescriptions and improved glycemic control during the years 2002–2011 in Japan (JDDM32). J Diabetes Investig. 2014;5:581–7.
Davies MJ, Bergenstal R, Bode B, et al. Efficacy of liraglutide for weight loss among patients with type 2 diabetes: the SCALE diabetes randomized clinical trial. JAMA. 2015;314:687–99.
The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86.
Ishii H, Anderson JH Jr, Yamamura A, et al. Improvement of glycemic control and quality-of-life by insulin lispro therapy: assessing benefits by ITR-QOL questionnaires. Diabetes Res Clin Pract. 2008;81:169–78.
Ming H, Zhiguang Z, Fang Z, et al. Effects of frequency of follow-up on quality of life of type 2 diabetes patients on oral hypoglycemics. Diabetes Technol Ther. 2012;14:777–82.
Bode BW, Testa MA, Magwire M, et al., for the LEAD-3 Study Group Patient-reported outcomes following treatment with the human GLP-1 analogue liraglutide or glimepiride in monotherapy: results from a randomized controlled trial in patients with type 2 diabetes. Diabetes Obes Metab. 2010;12:604–12.
Authors’ contributions
HI was the primary investigator, and was involved in all steps. All authors contributed to the study design, were involved at all stages of manuscript development, reviewed and edited the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to thank Akiko Matsumoto, Hisamoto Kuroda, Akira Yamauchi, Hiroaki Seino, Masako Togo, Masahiro Fukuda, Fuyuki Minagawa, Setsuya Sakagashira, Hideo Takahashi, Hitoshi Akiyama, Masayo Yamada, Yoko Matsuzawa, Ken Kurosaka, Toshiya Okamoto, Mitsuo Imura, Kumiko Hamano, Masahiro Iwamoto, Soichi Kurioka, Koji Kashima, Shin Furukawa, Hideki Nishimura, Hirofumi Matsuda, Nobuo Takahashi, Syuichi Takagi, Morio Aoyagi, Katsuyuki Yanagisawa, Mamiko Tsugawa, Hiromi Ogata, Tomoaki Yoshihara, Fumihiko Sato, Morio Aoyagi, Yasuyuki Ozawa, Satoru Okazaki, Miho Shimizu, Masae Toyonaga, Katsunori Manaka, Junko Saito, Masanori Nishino, Hitomi Fujii, Yoshimoto Kiyohara, Akitoshi Kawakubo, Kazuo Ikeda, Shingo Iwasaki, Keiji Nakayama, Kyuzi Kamoi, Kazuaki Yahata, Tomoko Nakagami, Tetsuji Yamashita, Yasumi Shintani, Munehide Matsuhisa, Atsuko Ashiba, Toru Hiyoshi, Ayumu Hoshi, Koji Nagayama, Hiroaki Sato, Etsuko Akita, Kenro Takahashi, Eri Kondo, Morio Aoyagi, Yasuhisa Yamamoto and Shinji Taneda for their participation in and contribution to this study. The authors also thank Yasuaki Hayashino for kindly reading and providing valuable comments on the manuscript. Hirokazu Yamada of Soiken, Inc. provided editorial assistance for this study, which was paid for by the Japan Society for Patient Reported Outcome.
Competing interests
HI received lecture fees from Astellas Pharma Inc., AstraZeneca K.K., Daiichi Sankyo Co., Ltd., Eli Lilly Japan K.K., Kowa Pharmaceutical Co., Ltd., Kyowa Hakko Kirin Co., Ltd., Mitsubishi Tanabe Pharma Co., MSD K.K., Nippon Boehringer Ingelheim Co., Ltd., Novartis Pharma K.K., Novo Nordisk Pharma Ltd., Sanofi K.K., Sumitomo Dainippon Pharma Co., Ltd., Takeda Pharmaceutical Co., Ltd., Taisho Toyama Pharmaceutical Co., Ltd., and grant/research support from Mitsubishi Tanabe Pharma Co., Ono Pharmaceutical Co., Takeda Pharmaceutical Co., Ltd., and Taisho Toyama Pharmaceutical Co., Ltd. Additionally, HI is the chief director of the Japan Society for Patient Report Outcome. TN has received lecture fees from Sanofi K.K., Novo Nordisk Pharma Ltd., Eli Lilly Japan K.K., Astellas Pharma Inc., Ono Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., Novartis Pharma K.K., Mitsubishi Tanabe Pharma Co., AstraZeneca K.K., MSD K.K., Shionogi & Co., Ltd., Taisho Toyama Pharmaceutical Co., Ltd., Bayer Yakuhin, Ltd., and Kissei Pharmaceutical Co., Ltd. Further, TN is a member of the Japan Society for Patient Report Outcome. HJ has received lecture fees from MSD K.K., Astellas Pharma Inc., Sanofi K.K., Novo Nordisk Pharma Ltd., Taisho Toyama Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Eli Lilly Japan K.K., and Nippon Boehringer Ingelheim Co., Ltd. and HJ is a member of the Japan Society for Patient Report Outcome. HW has received lecture fees from Astellas Pharma Inc., AstraZeneca K.K., Kowa Pharmaceutical Co., Ltd., Sanofi K.K., Takeda Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma Co., Novartis Pharma K.K., Novo Nordisk Pharma Ltd., Nippon Boehringer Ingelheim Co., Ltd., MSD K.K., Sumitomo Dainippon Pharma Co., Ltd., research funds from Novartis Pharma K.K., Eli Lilly Japan K.K., Taisho Pharmaceutical Co., Ltd., and grant/research support from MSD K.K., Astellas Pharma Inc., AstraZeneca K.K., Ono Pharmaceutical Co., Ltd., Kyowa Hakko Kirin Co., Ltd., Sanofi K.K., Daiichi Sankyo Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Takeda Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma Co., Terumo Co., Nippon Boehringer Ingelheim Co., Ltd., Novo Nordisk Pharma Ltd., Pfizer Japan Inc., Benefit one Health care Inc., Mochida Pharmaceutical Co., Ltd., Nitto Boseki Co., Ltd. HW is an endowed chair supported by a grant from MSD K.K., Takeda Pharmaceutical Co., Ltd., and a director of the Japan Society for Patient Report Outcome. All other authors declare that they have no competing interests.
Ethics approval and consent to participate
The study protocol was registered with the University Hospital Medical Information Network (UMIN-CTR: UMIN000007159) prior to the commencement of the study. We adhered to the “Ethical Guidelines for Clinical Studies” issued by the Japanese government, after receiving permission from the ethical committees at each of the participating medical facilities. Informed consent was obtained from all individual participants included in the study.
Funding
This study was funded by the Japan Society for Patient Reported Outcome that was operated by a research fund from Mitsubishi Tanabe Pharma Co., Ono Pharmaceutical Co., Ltd., Novo Nordisk Pharma Ltd., AstraZeneca K.K., Sanofi K.K., and Nippon Boehringer Ingelheim Co., Ltd.
Author information
Authors and Affiliations
Corresponding author
Additional files
13098_2016_202_MOESM3_ESM.docx
Additional file 3: Table S1. Table describing the correlation between domain scores and HbA1c, body weight, and random blood glucose.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Ishii, H., Niiya, T., Ono, Y. et al. Improvement of quality of life through glycemic control by liraglutide, a GLP-1 analog, in insulin-naive patients with type 2 diabetes mellitus: the PAGE1 study. Diabetol Metab Syndr 9, 3 (2017). https://doi.org/10.1186/s13098-016-0202-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-016-0202-0