
Abstract
Background
In patients on maintenance dialysis, increased serum calcium levels are known to be associated with a poor prognosis. However, it is not known whether serum calcium levels at dialysis initiation have an impact on subsequent prognosis.
Methods
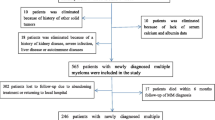
The subjects were patients who were newly initiated dialysis at the 17 Aichi Cohort Study of Prognosis in Patients Newly Initiated into Dialysis (AICOPP) group centers. The study included 1524 patients who were at least 20 years old, had CKD, and provided written consent. We excluded one patient whose serum adjusted calcium was not assessed and six patients whose outcomes were unknown. Thus, we enrolled 1517 subjects into the study. The patients were divided into the following five groups: (1) G1 with a serum adjusted calcium level <7.0 mg/dL, (2) G2 with 7.0 to <8.0 mg/dL, (3) G3 with 8.0 to <9.0 mg/dL, (4) G4 with 9.0 to <10.0 mg/dL, and (5) G5 with ≥10.0 mg/dL. The study outcomes included: (1) comparisons of all-cause mortality rates in the five groups; (2) extraction of factors influencing all-cause mortality.
Results
There were 268 deaths during the follow-up period (G1, 9 cases; G2, 30 cases; G3, 91 cases; G4, 110 cases; G5, 28 cases). Significant differences were observed between the five groups’ cumulative survival rates (Logrank test p = 0.005) by using Kaplan-Meier method. There were significant differences in the incidence of either aortic or cardiac valve calcification among the five groups (aortic calcification: p = 0.006, cardiac valve calcification: p = 0.008). Moreover, lower Barthel Index, which evaluated activities of daily living, were associated with higher serum adjusted calcium levels (p < 0.001). Multivariate Cox proportional hazard analysis using the stepwise method indicated that increasing serum adjusted calcium was associated with all-cause mortality (every 1 mg/dL increase, HR = 1.267, 95% CI = 1.092 − 1.470, p = 0.002). In addition, high mortality was associated with advanced age, male gender, low systolic blood pressure, history of cardiovascular disease, and no prior use of calcium carbonate.
Conclusions
Serum adjusted calcium levels at dialysis initiation were demonstrated to be associated with all-cause mortality after dialysis initiation.
Trial registration
UMIN 000007096. Registered 18 January 2012.
Similar content being viewed by others

Background
In patients newly starting dialysis, advanced age and concurrent cardiovascular diseases (CVDs) are major problems which are strongly associated with survival prognosis. The concept of chronic kidney disease-mineral and bone disorders (CKD-MBD) focuses on survival prognosis rather than bone lesions, and management of serum phosphorus and calcium levels is considered to be especially important [1]. In patients on dialysis, serum phosphorus levels have been shown to have a U-shaped association with mortality [2–7]. As for serum calcium levels, although it is not clear whether low levels are detrimental, high levels are known to be associated with a poor prognosis [3, 4, 8]. Given these background conditions, each guideline provides target values for serum phosphorus and calcium levels when managing patients on dialysis [1, 9].
Increased serum calcium levels reportedly cause vascular calcification and carry a risk of CVD [10–12]. However, serum calcium levels often tend to decrease during the predialysis stage of CKD including the period immediately before dialysis initiation [13]. Although secondary hyperparathyroidism has already manifested in this stage, it rarely progresses to nodular hyperplasia and is unlikely to cause hypercalcemia. Doi et al. documented a serum calcium level >8.5 mg/dL at dialysis initiation to be associated with outcomes at one year after dialysis initiation [14], but only a few other reports have described similar findings. Whether the association observed in patients on maintenance dialysis between serum calcium levels and survival prognosis is also present in patients starting dialysis merits investigation.
Thus, the present study aimed to elucidate the association between serum calcium levels at dialysis initiation and subsequent prognosis.
Methods
Subjects
The subjects were patients who were newly initiated dialysis at the 17 Aichi Cohort Study of Prognosis in Patients Newly Initiated into Dialysis (AICOPP) group centers from October 2011 to September 2013 [15]. Patients who were withdrawn from dialysis while hospitalized, died while hospitalized, or did not agree to be registered were excluded. The study included 1524 patients who were at least 20 years old, had CKD, and provided written consent. We excluded one patient whose serum adjusted calcium was not assessed and six patients whose outcomes were unknown, as determined by a survey conducted at the end of March 2015. Thus, we enrolled 1517 subjects into the study.
Patient characteristics and data when dialysis was initiated (baseline)
Body mass index (BMI) was measured at the first dialysis session. Diabetes was defined as a fasting blood glucose ≥126 mg/dL, casual blood glucose ≥200 mg/dL, HbA1c (NGSP) ≥6.5%, use of insulin, or use of oral hypoglycemic agents. History of cardiovascular disease (CVD) was defined as a history of heart failure requiring hospitalization, coronary artery disease requiring coronary artery intervention or heart bypass surgery, stroke, aortic disease requiring surgery, or peripheral artery disease requiring hospitalization. The period of nephrology care was established, based on patients’ medical records, as the period from referral to the nephrologist until the initiation of dialysis. Medication use referred to the drugs taken at dialysis initiation. Blood tests were performed on samples taken before the first dialysis session. Blood pressure was measured before the first dialysis session.
Group assignment according to serum adjusted calcium levels
The serum calcium levels at dialysis initiation of patients with a serum albumin level <4.0 g/dL were adjusted employing the Payne formula. According to adjusted serum calcium levels, the patients were divided into the following 5 groups: (1) G1 with a serum adjusted calcium level <7.0 mg/dL, (2) G2 with 7.0 to <8.0 mg/dL, (3) G3 with 8.0 to <9.0 mg/dL, (4) G4 with 9.0 to <10.0 mg/dL, and (5) G5 with ≥10.0 mg/dL.
Assessment of aortic and cardiac valve calcification
Aortic calcification was assessed according to the presence or absence of aortic arch calcification on plain frontal chest radiographs taken immediately before dialysis initiation. Cardiac valve calcification was assessed according to the presence or absence of a calcified aortic or mitral valve determined by B-mode echocardiography during the 1-month periods before and after dialysis initiation.
Assessment of activities of daily living with the Barthel index
The BI is composed of 10 items: (1) eating, (2) transferring between the bed and wheelchair, (3) grooming, (4) using the toilet, (5) bathing, (6) walking on a flat surface, (7) climbing and descending stairs, (8) dressing, (9) controlling bowel movements, and (10) controlling urination. Each item is evaluated on a 2-point (0 and 5) to 4-point (0, 5, 10, and 15) scale, and the total score (0−100 in increments of 5) is used for assessment [16]. In the present study, experienced nurses assessed the patients to determine the BI on discharge for dialysis initiation.
Survey of survival prognosis
Survival prognosis as of March 31, 2015 was determined by surveying medical records. For patients who were transferred to other institutions, information was obtained by mailing out survey forms.
Outcomes
The study outcomes included (1) comparisons of all-cause mortality rates in the five groups as categorized by serum adjusted calcium level; (2) extraction of factors, which included serum adjusted calcium, influencing all-cause mortality.
Statistical processing
The easy R (EZR) was used for statistical processing [17]. Comparisons of characteristics and baseline data between the five groups of patients were performed using the analysis of variance (ANOVA) for continuous variables and chi-square test for nominal variables. All-cause mortality rates were compared using the log-rank test for the Kaplan-Meier curves. Factors contributing to the all-cause mortality rates were examined using univariate Cox proportional hazard regression analysis. In addition to the serum adjusted calcium level, factors that were significant in the univariate analysis served as explanatory variables for the multivariate Cox proportional hazard analysis using the stepwise method (i.e., serum adjusted calcium, age, gender, BMI, SBP, DBP, CTR, history of CVD, use of calcium carbonate, hemoglobin, serum albumin, eGFR, PTH, and CRP). In stratified analyses, all-cause mortality rates were compared by Cox proportional hazard models adjusted for the factors used in the above-described step-wise analysis. Comparisons of aortic or cardiac valve calcification between the five groups of patient were performed using the chi-square test. Comparisons of Barthel index score between the five groups of patient were performed the analysis of variance (ANOVA). P values less than 5% were considered statistically significant.
Results
Comparison of patient characteristics and baseline data
Table 1 shows the patient characteristics and baseline data in the five groups. Significant differences between the five groups were observed in age, gender, BMI, DBP, prevalence of diabetes mellitus, history of CVD, BI, rate of beta blockers use, rate of ESAs use, hemoglobin level, serum albumin level, blood urea nitrogen (BUN) level, eGFR, serum creatinine level, serum phosphorus level, serum PTH level, and C-reactive protein (CRP) level.
Comparison of all-cause mortality
Figure 1 shows Kaplan-Meier curves for the cumulative survival rates of the five groups. There were 268 deaths during the follow-up period (G1, 9 cases; G2, 30 cases; G3, 91 cases; G4, 110 cases; G5, 28 cases). Significant differences were observed between the five groups’ cumulative survival rates (p = 0.005).

Comparison of all-cause mortality among the five groups. Significant differences were observed between the five groups’ cumulative survival rates (p = 0.005). G1 with a serum-adjusted calcium level <7.0 mg/dL, G2 with 7.0 to <8.0 mg/dL, G3 with 8.0 to <9.0 mg/dL, G4 with 9.0 to <10.0 mg/dL, and G5 with ≥10.0 mg/dL)
Factors affecting all-cause mortality
The results of univariate Cox proportional hazard regression analysis are presented in Table 2. The increase in serum adjusted calcium levels was associated with the survival prognosis (every 1 mg/dL increase, hazard ratio [HR] = 1.332, 95% confidence interval [CI] = 1.185 − 1.498, p < 0.001). In addition, high mortality was associated with advanced age, male gender, low BMI, low blood pressure, presence of cardiomegaly, history of CVD, no prior use of renin angiotensin system (RAS) inhibitors, no prior use of vitamin D receptor activator (VDRA), no prior use of calcium carbonate, no prior ESA use, presence of anemia, presence of hypoalbuminemia, high BUN level, high eGFR, low serum creatinine level, low serum phosphorus level, low PTH level, and high CRP level.
The results of multivariate Cox proportional hazard analysis using the stepwise method are shown in Table 3. Increasing serum adjusted calcium was associated with survival prognosis (every 1 mg/dL increase, HR = 1.267, 95% CI = 1.092−1.470, p = 0.002). In addition, high mortality was associated with advanced age, male gender, low systolic blood pressure, history of CVD, and no prior use of calcium carbonate.
Association of serum adjusted calcium levels with aortic and cardiac valve calcification
The five groups based on serum adjusted calcium levels at dialysis initiation were compared for aortic and cardiac valve calcification. There were significant differences in the incidence of either aortic or cardiac valve calcification among the five groups (aortic calcification p = 0.006, cardiac valve calcification p = 0.008). The incidence of calcification was especially low for G1 (Fig. 2).

Comparison of aortic and cardiac valve calcification among the five groups. Significant differences were observed between the five groups’ frequency of aortic and cardiac valve calcification (p = 0.006 and p = 0.008). G1 with a serum adjusted calcium level <7.0 mg/dL, G2 with 7.0 to <8.0 mg/dL, G3 with 8.0 to <9.0 mg/dL, G4 with 9.0 to <10.0 mg/dL, and G5 with ≥10.0 mg/dL
Association between serum adjusted calcium levels and the Barthel index
BI scores were compared among the five groups based on serum adjusted calcium levels at dialysis initiation. Lower BI scores were associated with higher serum adjusted calcium levels (p < 0.001) (Fig. 3).

Comparison of Barthel index score among the five groups. Significant differences were observed between the five groups’ Barthel index score (p < 0.001). G1 with a serum adjusted calcium level <7.0 mg/dL, G2 with 7.0 to <8.0 mg/dL, G3 with 8.0 to <9.0 mg/dL, G4 with 9.0 to <10.0 mg/dL, and G5 with ≥10.0 mg/dL. ANOVA, analysis of variance
Stratified analysis
The association between serum adjusted calcium levels and all-cause mortality was assessed with stratification by age, gender, history of CVD, BI score, VDRA use, calcium carbonate use, eGFR, and the PTH level. A significant association between serum adjusted calcium levels and all-cause mortality was observed in male patients age 70 years and older, a history of CVD, the full score of BI, VDRA use, no prior use of calcium carbonate, and an eGFR ≥5 mL/min/1.73 m2 (Fig. 4).

Stratified risk factors affecting all-cause mortality associated with serum adjusted calcium. Adjusted for serum adjusted calcium, age, gender, BMI, SBP, DBP, CTR, history of CVD, use of ACEIs or ARBs, use of VDRAs, use of calcium carbonate, use of ESAs, hemoglobin, serum albumin, BUN, eGFR, serum phosphorus, PTH, and CRP. VDRA; vitamin D receptor activator, CC; calcium carbonate, eGFR; estimated glomerular filtration rate, PTH; parathyroid hormone
Discussion
The present results revealed serum adjusted calcium levels at dialysis initiation to be associated with all-cause mortality after dialysis initiation. Moreover, multivariate analysis identified a high serum adjusted calcium level as an independent risk factor for poor survival prognosis. Severe hypocalcemia is highly likely to occur during the early period after dialysis initiation. On the other hand, we found that high serum adjusted calcium levels were associated with poor outcomes. In other words, pathological conditions that inhibit the decrease in serum adjusted calcium levels might have been associated with poor survival prognosis.
We considered that renal function at dialysis initiation influenced serum adjusted calcium levels. As the glomerular filtration rate (GFR) decreases, serum phosphorus and fibroblast growth factor 23 levels increase, followed by a decrease in the serum activated vitamin D level. As a consequence, the serum calcium level decreases. Thus, if dialysis is initiated in patients with a high GFR, their serum calcium may still be elevated. Regarding the association between renal function at dialysis initiation and survival prognosis, there is reports describing the survival prognosis as being rather poor when dialysis is initiated in patients with a high eGFR [18, 19]. This is considered to be attributable to many patients who begin dialysis in the early stage being elderly, and also to early initiation of dialysis being inevitable in some patients because of concurrent CVDs. The present study also showed higher adjusted serum calcium levels at dialysis initiation to be associated with higher eGFR, more advanced age, and/or a greater likelihood of concurrent CVDs. Because stratified analysis by eGFR revealed high serum adjusted calcium levels to be associated with poor survival prognosis, regardless of renal function level at dialysis initiation, higher serum adjusted calcium levels with respect to renal function might be a clinical issue. Common causes of hypercalcemia include (1) hyperparathyroidism, (2) malignancy, (3) chronic granulomatous disease, (4) drugs (e.g., activated vitamin D preparations, thiazide diuretics, and teriparatide), (5) hyperthyroidism, (6) adrenal insufficiency, (7) immobility, (8) total parenteral nutrition, and (9) milk-alkali syndrome [20]. We considered that among above causes of hypercalcemia, drugs or immobility led to increase in serum adjusted calcium level inconsistent with renal function. Because many reports have recently indicated that the use of calcium-containing phosphate binders in patients with dialysis worsens survival prognosis [21–23], we additionally examined drugs affecting serum calcium levels. The rate of using thiazide diuretics, VDRA, or calcium-containing phosphate binders did not differ significantly among the groups. After the patients were stratified based on the use of VDRA or calcium-containing phosphate binders, the effects of these drugs on survival prognosis were assessed. Regardless of the use of these drugs, high serum adjusted calcium levels were generally associated with poor survival prognosis. Thus, when these serum calcium-elevating drugs are used, it would apparently be important to maintain the serum adjusted calcium concentration at “a level commensurate with renal function”. The use of calcium carbonate was unexpectedly associated with better prognosis in the present study. Comparison of serum adjusted calcium and phosphorus levels between use and no use of calcium carbonate groups showed no significant differences (Additional file 1: Figure S1). In other word, patients who took more amount of phosphorus intake were likely administered calcium carbonate. We suspected that those of patients probably took sufficient dietary protein after dialysis initiation. Therefore, good nutritional status led to better prognosis during the relatively short term follow up period.
In the present study, patients with a high serum adjusted calcium level at dialysis initiation included many elderly as well as those with a low BI score, which reflects ADL. Thus, increased serum calcium levels due to immobility, one of the above-described causes of hypercalcemia, might have contributed to our results. Immobility promotes bone resorption via mobilization of calcium from bone, which in turn causes hypercalcemia [24, 25]. Consequently, PTH levels are suppressed. In the present study, PTH levels decreased as serum adjusted calcium levels rose. This result appears to be consistent with the known effects of immobility.
Elevated serum calcium is known to be a factor promoting vascular calcification [26]. Moreover, vascular calcification is an important pathological condition that affects survival prognosis [27]. The results of the present study revealed the prevalence of aortic and cardiac valve calcification to be higher in patients with higher serum-adjusted calcium levels. This suggests that the poor survival prognosis in patients with higher serum adjusted calcium levels might be attributable to advanced organ dysfunction due to vascular calcification. However, it is also possible that such ectopic calcification is strongly associated with age-related factors.
The present study has the following limitations. First, because of the observational study design, there were differences in patient characteristics and baseline data among the groups, although the data were adjusted for several of these factors. We could not exclude the bias because several factors including age, gender, BMI, diabetes, and history of CVD were strongly associated mortality in general. Second, there was difference in the number of patients among the five groups. Hence, we conducted comparison of all-cause mortality between five groups classified by quintile of serum adjusted calcium. We considered that the bias was at minimum because the results were similar (Additional file 2: Figure S2). Third, the extent to which low BI scores reflect bone resorption due to immobility is unknown. The subjects of the present study were limited to patients who could be discharged to home or transferred to another facility after dialysis initiation. Thus, there were only a few patients with very low ADL who were bedridden 24 h a day. In this situation, it is not certain whether the physical activity levels of the patients can be regarded as “immobility.” Fourth, neither vascular nor cardiac valve calcification was assessed quantitatively. As the severity calcification was not considered, i.e., cases with mild to severe calcifications were handled equally in performing the analyses, this study lacks sufficient objectivity to identify calcification as a cause of poor prognosis.
Conclusions
Serum-adjusted calcium levels at dialysis initiation were demonstrated to be associated with all-cause mortality after dialysis initiation.
References
Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2009;113:S1–130.
Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol. 2004;15(8):2208–18.
Stevens LA, Djurdjev O, Cardew S, Cameron EC, Levin A. Calcium, phosphate, and parathyroid hormone levels in combination and as a function of dialysis duration predict mortality: evidence for the complexity of the association between mineral metabolism and outcomes. J Am Soc Nephrol. 2004;15(3):770–9.
Taniguchi M, Fukagawa M, Fujii N, Hamano T, Shoji T, Yokoyama K, Nakai S, Shigematsu T, Iseki K, Tsubakihara Y, Committee of Renal Data Registry of the Japanese Society for Dialysis Therapy. Serum phosphate and calcium should be primarily and consistently controlled in prevalent hemodialysis patients. Ther Apher Dial. 2013;17(2):221–8.
Kalantar-Zadeh K, Kuwae N, Regidor DL, Kovesdy CP, Kilpatrick RD, Shinaberger CS, McAllister CJ, Budoff MJ, Salusky IB, Kopple JD. Survival predictability of time-varying indicators of bone disease in maintenance hemodialysis patients. Kidney Int. 2006;70(4):771–80.
Floege J, Kim J, Ireland E, Chazot C, Drueke T, de Francisco A, Kronenberg F, Marcelli D, Passlick-Deetjen J, Schernthaner G, Fouqueray B, Wheeler DC, ARO Investigators. Serum iPTH, calcium and phosphate, and the risk of mortality in a European hemodialysis population. Nephrol Dial Transplant. 2011;26(6):1948–55.
Tentori F, Blayney MJ, Albert JM, Gillespie BW, Kerr PG, Bommer J, Young EW, Akizawa T, Akiba T, Pisoni RL, Robinson BM, Port FK. Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2008;52(3):519–30.
Lin YC, Lin YC, Hsu CY, Kao CC, Chang FC, Chen TW, Chen HH, Hsu CC, Wu MS, Taiwan Society of Nephrology. Effect Modifying Role of Serum Calcium on Mortality-Predictability of PTH and Alkaline Phosphatase in Hemodialysis Patients: An Investigation Using Data from the Taiwan Renal Registry Data System from 2005 to 2012. PLoS One. 2015;10(6):e0129737.
Fukagawa M, Yokoyama K, Koiwa F, Taniguchi M, Shoji T, Kazama JJ, Komaba H, Ando R, Kakuta T, Fujii H, Nakayama M, Shibagaki Y, Fukumoto S, Fujii N, Hattori M, Ashida A, Iseki K, Shigematsu T, Tsukamoto Y, Tsubakihara Y, Tomo T, Hirakata H, Akizawa T, CKD-MBD Guideline Working Group; Japanese Society for Dialysis Therapy. Clinical practice guideline for the management of chronic kidney disease-mineral and bone disorder. Ther Apher Dial. 2013;17(3):247–88.
Moldovan D, Rusu C, Kacso IM, Potra A, Patiu IM, Gherman-Caprioara M. Mineral and bone disorders, morbidity and mortality in end-stage renal failure patients on chronic dialysis. Clujul Med. 2016;89(1):94–103.
Chen NX, Moe SM. Pathophysiology of Vascular Calcification. Curr Osteoporos Rep. 2015;13(6):372–80.
Ossareh S. Vascular calcification in chronic kidney disease: mechanisms and clinical implications. Iran J Kidney Dis. 2011;5(5):285–99.
Hutchison AJ. Predialysis management of divalent ion metabolism. Kidney Int Suppl. 1999;73:S82–4.
Doi T, Yamamoto S, Morinaga T, Sada KE, Kurita N, Onishi Y. Risk Score to Predict 1-Year Mortality after Hemodialysis Initiation in Patients with Stage 5 Chronic Kidney Disease under Predialysis Nephrology Care. PLoS One. 2015;10(6):e0129180.
Hishida M, Tamai H, Morinaga T, Maekawa M, Aoki T, Tomida H, Komatsu S, Kamiya T, Maruyama S, Matsuo S, Inaguma D. Aichi cohort study of the prognosis in patients newly initiated into dialysis (AICOPP): baseline characteristics and trends observed in diabetic nephropathy. Clin Exp Nephrol. 2016 Feb 23. [Epub ahead of print]
Mahoney FI, Barthel DW. Functional Evaluation: The Barthel Index. Md State Med J. 1965;14:61–5.
Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–8.
Hwang SJ, Yang WC, Lin MY, Mau LW, Chen HC, Taiwan Society of Nephrology. Impact of the clinical conditions at dialysis initiation on mortality in incident hemodialysis patients: a national cohort study in Taiwan. Nephrol Dial Transplant. 2010;25(8):2616–24.
Rosansky SJ, Eggers P, Jackson K, Glassock R, Clark WF. Early start of hemodialysis may be harmful. Arch Intern Med. 2011;171(5):396–403.
Khairallah W, Fawaz A, Brown EM, El-Hajj FG. Hypercalcemia and diabetes insipidus in a patient previously treated with lithium. Nat Clin Pract Nephrol. 2007;3(7):397–404.
Borzecki AM, Lee A, Wang SW, Brenner L, Kazis LE. Survival in end stage renal disease: calcium carbonate vs. sevelamer. J Clin Pharm Ther. 2007;32(6):617–24.
Block GA, Raggi P, Bellasi A, Kooienga L, Spiegel DM. Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Kidney Int. 2007;71(5):438–41.
Jamal SA, Vandermeer B, Raggi P, Mendelssohn DC, Chatterley T, Dorgan M, Lok CE, Fitchett D, Tsuyuki RT. Effect of calcium-based versus non-calcium-based phosphate binders on mortality in patients with chronic kidney disease: an updated systematic review and meta-analysis. Lancet. 2013;382(9900):1268–77.
Stewart AF, Adler M, Byers CM, Segre GV, Broadus AE. Calcium homeostasis in immobilization: an example of resorptive hypercalciuria. N Engl J Med. 1982;306(19):1136–40.
Alborzi F, Leibowitz AB. Immobilization hypercalcemia in critical illness following bariatric surgery. Obes Surg. 2002;12(6):871–3.
Razzaque MS. The dualistic role of vitamin D in vascular calcifications. Kidney Int. 2011;79(7):708–14.
Blacher J, Guerin AP, Pannier B, Marchais SJ, London GM. Arterial calcifications, arterial stiffness, and cardiovascular risk in end-stage renal disease. Hypertension. 2001;38(4):938–42.
Acknowledgements
We acknowledge the support provided by the following investigators and members of the Aichi Cohort study of Prognosis in Patients Newly Initiated Into Dialysis (AICOPP), who participated in this study: Akihito Tanaka, Minako Murata, Hibiki Shinjo, Yasuhiro Otsuka, Asami Takeda (Japanese Red Cross Nagoya Daini Hospital), Hirofumi Tamai (Anjo Kosei Hospital), Tomohiko Naruse (Kasugai Municipal Hospital), Kei Kurata (Tosei General Hospital), Hideto Oishi (Komaki City Hospital), Isao Aoyama (Japanese Community Healthcare Organization Chukyo Hospital), Hiroshi Ogawa (Shinseikai Daiichi Hospital), Hiroko Kushimoto (Chita City Hospital), Hideaki Shimizu (Chubu-Rosai Hospital), Junichiro Yamamoto (Tsushima City Hospital), Hisashi Kurata (Toyota Kosei Hospital), Taishi Yamakawa (Toyohashi Municipal Hospital), Takaaki Yaomura (Nagoya Medical Center), Hirotake Kasuga (Nagoya Kyouritsu Hospital), Shizunori Ichida (Japanese Red Cross Nagoya Daiichi Hospital), Shoichi Maruyama (Nagoya University Graduate School of Medicine), Seiichi Matsuo (Nagoya University Graduate School of Medicine), and Noritoshi Kato (Nagoya University Graduate School of Medicine).
Funding
Not applicable.
Availability of data and materials
Not applicable.
Authors’ contributions
DI participated in the design of the study and interpretation of the data. DI, SK, and HH participated in writing the manuscript. All authors were involved in drafting, reviewing, and approving the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was conducted by following the Ethical guidelines for Clinical Research by the Japanese Ministry of Health, Labor, and Welfare (created July 30, 2003; full revision December 28, 2004; full revision July 31, 2008) and the Helsinki Declaration (revised 2013) and was approved by the clinical research ethics committees at each AICOPP group facility (the approval number: 20110823-3). The subjects received oral and written explanations of the purpose of the study and provided their consent in writing.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional files
Additional file 1: Figure S1.
Comparison of serum adjusted calcium and phosphorus level between use and no use of calcium carbonate groups. No significant differences were observed between the two groups’ serum mineral levels (p = 0.071 and p = 0.634) by t test. (TIF 40 kb)
Additional file 2: Figure S2.
Comparison of all-cause mortality among the five groups classified by quintile of serum adjusted calcium. Significant differences were observed between the five groups’ cumulative survival rates (p < 0.001). Q1 with the lowest serum adjusted calcium level, Q5 with the highest serum adjusted calcium level. (TIF 42 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Inaguma, D., Koide, S., Takahashi, K. et al. Relationship between serum calcium level at dialysis initiation and subsequent prognosis. Ren Replace Ther 3, 2 (2017). https://doi.org/10.1186/s41100-016-0087-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-016-0087-2