
Plain English summary
People with osteoarthritis desire high quality care, support and information. However, the quality of care for people with OA in general practice is not routinely collected. Quality Indicators can be used to benefit patients by measuring whether minimum standards of quality care are being met from a patient perspective.
The aim of this study was to describe how a Research User Group (RUG) worked alongside researchers to co-produce a set of self-reported quality indicators for people with osteoarthritis when visiting their general practitioner or practice nurse (primary care). These were required in the MOSAICS study, which developed and evaluated a new model of supported self-management of OA to implement the NICE quality standards for OA.
This article describes the public involvement in the MOSAICS study. This was 1) the co-development by RUG members and researchers of an Osteoarthritis Quality Indicators United Kingdom (OA QI (UK)) questionnaire for use in primary care, and 2) the comparison of the OA QI (UK) with a similar questionnaire developed in Norway.
This study shows how important and effective a research user group can be in working with researchers in developing quality care indicators for osteoarthritis for use in a research study and, potentially, routine use in primary care. The questionnaire is intended to benefit patients by enabling the assessment of the quality of primary care for osteoarthritis from a patient’s perspective. The OA QI (UK) has been used to examine differences in the quality of osteoarthritis care in four European countries.
Abstract
Background
People with osteoarthritis (OA) desire high quality care, support and information about OA. However, the quality of care for people with OA in general practice is not routinely collected. Quality Indicators (QI) can be used to benefit patients by measuring whether minimum standards of quality care (e.g. NICE quality standards) are being met from a patient perspective. A Research User Group (RUG) worked with researchers to co-produce a set of self-report, patient-generated QIs for OA. The QIs were intended for use in the MOSAICS study, which developed and evaluated a new model of supported self-management of OA to implement the NICE guidelines. We report on 1) the co-development of the OA QI (UK) questionnaire for primary care; and 2) the comparison of the content of the OA QI (UK) questionnaire with a parallel questionnaire developed in Norway for the Musculoskeletal Pain in Ullensaker (MUST) study.
Methods
Researchers were invited to OA RUG meetings. Firstly, RUG members were asked to consider factors important to patients consulting their general practitioner (GP) for OA and then each person rated their five most important. RUG members then discussed these in relation to a systematic review of OA QIs in order to form a list of OA QIs from a patient perspective. RUG members suggested wording and response options for a draft OA QI (UK) questionnaire to assess the QIs. Finally RUG members commented on draft and final versions of the questionnaire and how it compared with a translated Norwegian OA-QI questionnaire.
Results
RUG members (5 males, 5 females; aged 52–80 years) attended up to four meetings. RUG members ranked 20 factors considered most important to patients consulting their GP for joint pain. Following discussion, a list of eleven patient-reported QIs for OA consultations were formed. RUG members then suggested the wording and response options of 16 draft items – four QIs were split into two or more questionnaire items to avoid multiple dimensions of care quality within a single item. On comparison of this to the Norwegian OA-QI questionnaire, RUG members commented that both questionnaires contained seven similar QIs. The RUG members and researchers agreed to adopt the Norwegian OA-QI wording for four of these items. RUG members also recommended adopting an additional seven items from the Norwegian OA-QI with some minor word changes to improve their suitability for patients in the UK. One other item from the draft OA QI (UK) questionnaire was retained and eight items were excluded, resulting in a 15-item final version.
Conclusions
This study describes the development of patient-reported quality indicators for OA primary care derived by members of a RUG group, working in partnership with the research team throughout the study. The OA QI (UK) supports the NICE quality standards for OA and they have been successfully used to assess the quality of OA consultations in primary care in the MOSAICS study. The OA QI (UK) has the potential for routine use in primary care to assess the quality of OA care provided to patients.
Ongoing research using both the UK and Norwegian OA-QI questionnaires is assessing the self-reported quality of OA care in different European populations.
Similar content being viewed by others



Background
Osteoarthritis (OA) is a leading cause of joint pain and years lived with disability worldwide causing considerable detrimental impact on daily activities and quality of life [1–4]. OA is one of the main reasons for musculoskeletal consultations with a general practitioner by older adults [5].
High quality care is described as clinically effective, personal and safe, which is delivered to all users of a health service in all aspects of care [6]. However, previous studies have shown that the quality of care provided to patients with OA in primary care is suboptimal [7–11] and varies according to patient age and OA severity [12]. Research has shown that patients with OA need more information and education about the condition, diet, exercise, aids, and better support for self-management [13]. However, core recommended treatments such as exercise, weight loss and the provision of written information is underused for patients with OA [7]. Furthermore many core treatment are initiated by the patients themselves rather than doctor initiated [7, 14].
Several international guidelines exist which provide recommendations for the management of OA [3, 4, 15, 16]. International quality standards for OA have also been developed such as those recently published by the National Institute for Health & Care Excellence (NICE) [17], and the European Musculoskeletal Conditions Surveillance and Information Network (eumusc.net) [18]. Yet there are no robust or routinely collected measures used currently in general practice to monitor the quality of care for people with OA [19], although an OA e-template for use during consultations in primary care has recently been developed and tested [20, 21].
Quality indicators (QI) are ‘specific and measurable elements of practice that can be used to assess the quality of care’ [22]. They are used to assess care quality according to defined standards of care (e.g. NICE [17], eumusc.net [18]). QIs typically assess the processes of care given to patients [23] by measuring what the provider can offer patients and examining whether standards of care are being implemented.
A systematic review identified 15 QIs which are broadly applicable with current international guidance for the assessment of non-pharmacological and pharmacological management of OA in primary care [8]; however the authors recommended an increased use of QIs in primary care from the patient perspective.
The Management of OSteoArthritis In ConsultationS (MOSAICS) study [24] developed and evaluated a new model of supported self-management of OA to implement the NICE guidelines for OA in primary care [3]. The MOSAICS study aimed to evaluate the new model of supported self-management for OA in primary care, in terms of the quality of care from both a clinical and a patient perspective (see Additional file 1 for more information about the MOSAICS study). The findings of the MOSAICS study are subject to other papers in production. However, at the time of designing the MOSAICS study, there was a lack of evidence regarding the experiences of patients with OA in primary care and there were few appropriate quality indicators that captured the quality of primary care for OA from the patient perspective. Active and meaningful patient and public involvement (PPI) is increasingly viewed and encouraged as integral part of the research process to improve its quality and relevance [25–28]. Therefore the collaboration between the researchers and the RUG described in this article led to development of patient reported QIs for the MOSAICS model of self-support in primary care.
During the course of the MOSAICS study, the research team became aware of a questionnaire capturing the patient perspective of the quality of OA primary care being developed in Norway. The OsteoArthritis Quality Indicator (OA-QI) has since been validated for use to measure the quality of primary care for OA in a Norwegian population [29]. The Norwegian OA-QI, comprises 17 questions related to patient education and information, regular provider assessments, referrals, and pharmacologic treatment. The tool was developed by team of researchers and OA clinicians, with input from two patient partners who gave feedback on the content of the finalised questionnaire. The results of the validation study are reported elsewhere [29].
We report on the co-production of a set of self-report, RUG-generated QIs to capture the quality of primary care management of OA. We also compare the RUG-generated OA QI (UK) questionnaire with a Norwegian OA-QI questionnaire developed in parallel, leading to a final recommended OA QI (UK) questionnaire.
The manuscript was written using the Guidance for Reporting Involvement of Patients and Public (GRIPP) checklist for reporting Patient and Public Involvement (PPI) in research [30]. This checklist provides a structure for improving the quality of reporting of the PPI and is designed for studies that have included some form of patient and public involvement in research. The authors have referred to the checklist to ensure all the relevant aspects of PPI in this study were reported.
PPI good practice
The PPI described in this article took place at the Arthritis Research UK Primary Care Centre, Keele University. This institution takes an explicit and systematic approach to involvement of patients and the public in research [31]. Formed in 2006, a Research User Group (RUG) was established to embed PPI across the whole of the Centre’s research activities and is supported by a dedicated PPI team and core funding. Currently, the RUG has over 60 members actively involved on over 60 projects, recruited on a basis of ‘expertise by experience’ of musculoskeletal and other long term conditions. Some RUG members have more experience in involvement in research than other members, though all provide the lay perspective of their health condition. Our approach to patient involvement draws on previous experience [32–35] and recommendations for the good practice of PPI [25, 30, 36, 37] so that RUG members can provide meaningful contributions to the research process (see Additional file 2 for more information about the RUG).
Our good practice principles include holding meetings in accessible venues at convenient times; allocated parking; meeting and greeting on arrival; training and support; inclusion of regular breaks during meetings; payment for RUG members’ time and contribution (if wanted); and reimbursement of expenses. Meetings between researchers and RUG members are made actively ‘jargon-free’ and any technical terms are explained in plain English.
Methods
The MOSAICS study investigated whether a new way of supporting self-management, delivered during an OA consultation in primary care, could offer a clinically practical approach to implementing the core NICE recommendations [24]. We describe here the development of the OA QI (UK) questionnaire by the RUG group for use in the MOSAICS study in Stage 1, the comparison of this with a Norwegian OA-QI questionnaire in Stage 2, and review of the finalised OA QI (UK) questionnaire in Stage 3. Figure 1 provides an overview of the process.

Overview of the stages of development of the OA QI
Patient and public involvement in this study
In 2009, RUG members with OA were invited to form an OA PPI group to work in partnership with researchers throughout the MOSAICS study, including the development of patient-reported QIs, set within a wider five year programme of research into OA [24, 38]. Furthermore, two members (AH: a former member of the wider Research User group and now PPI Support Worker/Coordinator; and RT: Lay member of the OA Research User Group) have co-authored this article, including writing the plain English and providing detailed comments on the manuscript prior to the final submission.
During the course of the MOSAICS study, members of the research team met with RUG members to co-produce the OA QI (UK) questionnaire for use in the MOSAICS study. The discussion meetings were facilitated by the Centre’s PPI Support Worker/Coordinator, the MOSAICS study Chief Investigator and a trial coordinator. The PPI Support Worker/Coordinator provided a key role by attend the meetings with RUG members to provide assistance and support, prior, during and after meetings. The MOSAICS study Chief Investigator (KD) has collaborated with the RUG on numerous research studies and is currently the senior academic lead for PPI in the Centre. All trial coordinators at the Centre have a responsibility for ensuring PPI in their respective studies and have lots of experience of collaborating with RUG members.
Discussion notes from the meetings were recorded on flip charts and in meeting minutes. Following each meeting, a summary of the outcomes and decisions written in plain English was sent to the RUG members to acknowledge their contribution and verify that all views had been captured. RUG members were also given the opportunity for further comment at the start of the next meeting.
It was not intended to formally evaluate the PPI interaction and the RUG members’ experience in the process. However, the impact of the RUG members is described in this article in the form of the co-produced OA QI (UK) questionnaire for use in the MOSAICS study.
Ethical approval for the PPI activities was not sought because the RUG members were acting as specialist advisers, providing valuable knowledge and expertise based on their experience of a health condition or public health concern and their involvement did not raise any ethical concerns [39]. However, the full MOSAICS research programme was approved by the North West 1 Research Ethics Committee, Cheshire, UK (REC reference: 10/H1017/76) [24].
Stage 1: development of the OA QI questionnaire
Members of the OA RUG group (n = 10) were invited to a series of four discussion groups with the research team to develop the patient-reported QIs for patients with OA treated in primary care. The discussion groups took place over a three year period from 2009–2012. The objectives of the discussion groups were i) to understand the aims of MOSAICS and roles and expectations of the RUG members, ii) to identify important and relevant quality indicators for patients with OA when consulting in primary care, and iii) to develop wording and response options for a self-report OA QI (UK) questionnaire to assess the identified quality indicators (Fig. 1).
-
i)
Understanding the aims of MOSAICS and roles and expectations of the RUG members
In the first meeting, a plain English summary of the MOSAICS study was introduced to set the context for the meetings and outline roles of the RUG members.
-
ii)
Identifying important and relevant quality indicators of OA in primary care consultations from a patient’s perspective
During facilitated discussions, RUG members identified factors they considered to be important to patients with OA consulting their general practitioner (GP) to help identify potential QIs for OA consultations. Each RUG member then ranked (1 to 5) the top five factors they considered the most important. Any factors not selected as ‘most important’ by at least one RUG member were excluded from further discussions.
The research team then presented RUG members with five QIs identified from a previous systematic review [8] (Fig. 2). These QIs were selected on the basis of their relevance for the MOSAICS model OA consultation of supported self-management and were used to stimulate discussion within the RUG group. The QIs included whether during GP consultations, patients have been offered education and advice about their disease, exercise and weight loss, and offered pain relief in the form of paracetamol and topical (skin applied) non-steroidal anti-inflammatory drugs (NSAIDS). RUG members were asked to 1) consider each QI alongside the initial list of important factors when consulting their GP for OA and add other factors as necessary, and 2) suggest potential QIs and questions which could capture the quality of care from a patient perspective.
Fig. 2 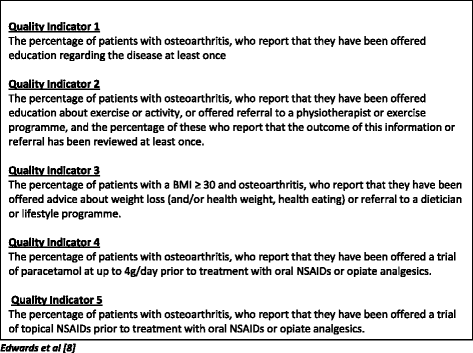
Five quality indicators identified from a systematic review used to stimulate discussion with the RUG members
-
iii)
Developing the wording and response options for a self-report OA QI (UK) questionnaire
Based on the list of important factors suggested by RUG members, an initial set of patient-reported OA QIs were generated. From this list, wording for questionnaire items to assess the QIs were drafted for an OA QI (UK) questionnaire. Over a further two meetings, RUG members and the research team worked together to refine and finalise the questions so they were suitable for use in a research trial. (See Fig. 3 for an outline of the process). Feedback and suggestions on the wording of the items and the scoring method (response options) were given on documents mailed to the RUG members between meetings.
Fig. 3 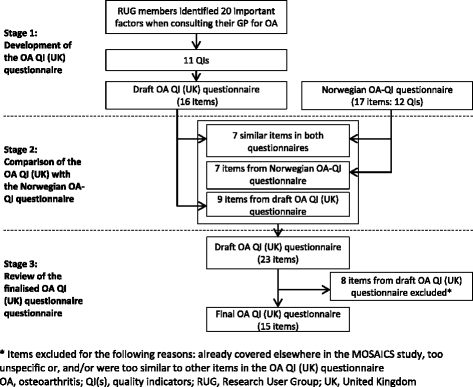
Overview of the OA QI (UK) questionnaire item development


Stage 2: comparison of the OA QI (UK) with the Norwegian OA-QI questionnaire
The RUG group and MOSAICS study team had not planned to test the measurement (or psychometric) properties of the OA QI (UK) questionnaire. As mentioned earlier in this article, a similar OA QI questionnaire was being developed for use in primary care in Norway (the Norwegian OA-QI) [29].
In order to establish the measurement properties of the OA QI (UK) questionnaire, the Norwegian developers (NO, KH) produced an English translation of a draft version of the Norwegian OA-QI for item content and scoring comparison. RUG members reviewed this and compared its content with the OA QI (UK) questionnaire during the third meeting. Based on this comparison, RUG members suggested how the OA QI (UK) questionnaire could be refined and modified to include items in the validated Norwegian OA-QI. Where QIs in each questionnaire were similar, RUG members considered the appropriateness of the wording used in the Norwegian OA-QI for potential use.
Stage 3: review of the finalised OA QI (UK) questionnaire
During the last meeting, the RUG reviewed, commented and suggested refinements to the OA QI (UK) questionnaire for primary care. RUG members were also asked to assess the face validity of the questionnaire by commenting further on its appearance and layout, ease of completion, and to identify anything ambiguous or difficult to understand. The research team also compared the content of the OA QI (UK) questionnaire with the other questionnaires and data collected in the MOSAICS to check for unnecessary duplication.
Results
Patient and public involvement
All of the RUG members (males 5, females 5) had OA and were aged 52–80 years. Four meetings were held during the three year period. All meetings were attended by between three and ten members.
Stage 1: development of the OA quality indicators
Identifying important and relevant quality indicators of OA in primary care consultations from a patient’s perspective
RUG members initially discussed and identified 30 factors considered important and relevant to patients consulting their GP for OA. From this list, RUG members chose 20 factors as ‘most important’ (Table 1), which were grouped into the following domains: information about OA; information about treatment for OA; information about self-management for OA; advice about using medications to relieve joint pain; information about exercise and activities; referrals to activity or exercise programmes, and the quality of the consultation with the GP. These domains formed an initial list of seven patient-reported QIs for OA consultations. Following the review of the five quality indicators identified from a systematic review [8], an additional four QIs appropriate from a patient perspective (‘patient has received a follow-up review of his/her joint problem’; ‘patient has received a referral for physiotherapy’; ‘patient has received advice about body weight and joint pain’, ‘patient has received a referral for weight loss services’) were added. Therefore, 11 unique QIs were identified (Table 1).
Developing the wording and response options for a self-report OA QI (UK) questionnaire
Using the list of eleven self-reported QIs for OA consultations, RUG members suggested questionnaire wording and response options to assess each QI. RUG members stated that the 3-month recall period, as determined by the MOSAICS trial design, was an appropriate period to have had at least one consultation with their GP for a joint problem. They also suggested that the response options should be a simple 3-level response format for all questions for the draft questionnaire: “Yes”, “No”, and “Don’t know”.
The RUG members’ suggestions were drafted into a questionnaire. Views of the overall quality of the consultation were captured in other parts of the MOSAICS study, so this item was not included in the questionnaire. To avoid multiple dimensions of care within a single question, one QI (advice about using medications to relieve joint pain) was split into four questions, two QIs (information about self-management for OA; advice about exercise or activities) into three items, and one other QI (follow up review) was split into two questions, respectively.
The resultant draft OA QI (UK) questionnaire comprised 16 items. In the second group meeting, RUG members reviewed the draft questionnaire and worked with the research team to refine its content. RUG members provided further comments on the ease of understanding and relevance of the questions. They suggested wording for the questionnaire instructions and changes to improve the clarity, specificity and order of the questions. RUG members suggested changing the wording for the ‘don’t know’ response option where relevant if the respondent could not remember, if they had not received an aspect of care, or if the question was not applicable.
Stage 2: comparison of the OA QI (UK) with the Norwegian OA-QI questionnaire
After reviewing both questionnaires, RUG members suggested that the draft OA QI (UK) questionnaire and the draft Norwegian OA-QI were similar. Seven items in the draft OA QI (UK) questionnaire capturing six quality indicators: (information about OA, information about treatment for OA, information about self-managing OA, advice about exercise or activities for OA, referral to exercise or activity programmes for OA, advice about the use of medications to relieve joint pain) used comparable wording to those included in the draft Norwegian OA-QI (Table 2). Of these, RUG members and the research team agreed to retain the wording used in the draft OA QI (UK) questionnaire for three items and adopt all or some of wording in the draft Norwegian OA-QI for the other four items for the final questionnaire. Both questionnaires used similar three-level response options.
RUG members recommended that a further seven items (capturing six QIs) included in the Norwegian OA-QI were relevant and should be added to the UK questionnaire. They suggested minor changes to wording to make them more appropriate for the UK (Table 2). Three other items from the Norwegian OA-QI questionnaire (advice about changing lifestyle; assessment of daily activities; assessment of pain) were captured elsewhere in the MOSAICS study and therefore not required for the OA QI (UK) questionnaire. Nine items from the draft OA QI (UK) that were not present in the Norwegian OA-QI were retained at this stage. Therefore, at the end of Stage 2, the draft version of the OA QI (UK) questionnaire contained 23 items (Fig. 3).
Stage 3: review of the finalised OA QI (UK) questionnaire
The iterative process of redrafting and reviewing the questionnaire continued into the fourth meeting until the RUG members and researchers agreed on the final draft version. Along with subtle changes to item wording suggested by RUG members, the research team and RUG members agreed to retain one item from the draft OA QI (UK) (on support for self-managing OA). Eight items from the draft OA QI (UK) (support from ‘surgery’ or other health care professionals to help you manage your joint problem; follow up review received (2 items); current participation in exercise; exercise programme suggested; referral for physiotherapy; advice about taking paracetamol received; advice about taking capsaicin cream received) were either covered elsewhere in the MOSAICS study [24], too generic or were too similar to other items (Table 2). Therefore, these eight items were not included in the final 15-item OA QI (UK) questionnaire (see Additional file 3). RUG members and researchers agreed that the length of the final version of the questionnaire was appropriate to capture important quality indicators of OA in primary care consultations from a patient’s perspective without overburdening those who complete it.
Discussion
This study describes the development of patient-reported quality indicators questionnaire for the primary care of osteoarthritis, which were derived by members of a Research User Group, working in partnership with researchers. The OA QI (UK) has been successfully used in a large randomized control trial of a new model of supported self-management of OA (the MOSAICS study) [22] and a study to audit the quality of OA primary care practice in the United Kingdom, Norway, Denmark and Portugal. While the full results of these studies are subject to other papers in production, the focus of this article is on the role and impact of PPI to develop the OA QI (UK).
The active, meaningful and on-going involvement of patients as partners in the research process is a strength of this study. The perspectives of patients may differ from the perspectives of healthcare professionals or information recorded by professionals in medical records [40, 41]. Therefore, the unique perspectives of patients with OA based on their experience of the condition and past consultations in primary care has enhanced the development of patient-centred quality indicators for use in OA primary care. We acknowledged that the PPI input in this study incorporated the perspectives of a small group of patients, as small as three people for one meeting. Also, the RUG membership was not greatly diverse, in terms of age, ethnicity, and physical abilities. While obtaining a range of perspectives is the objective of PPI in research and not necessarily ‘representativeness’, it is possible however that the OA QI (UK) does not cover the full range of quality indicators relevant to the population of patients with OA. Nevertheless, the sequential and iterative development of the OA QI (UK) allowed the researchers and RUG members to review and critique earlier suggestions made by the RUG.
The RUG group identified important factors related to the quality of OA care provided by a primary care healthcare professional and suggested item wording for a questionnaire. By comparing the OA QI (UK) questionnaire with a similar one developed in Norway, the RUG members helped redraft and refine the final questionnaire. The RUG collaborated with the research team throughout the development of the OA QI (UK) but were also involved on other aspects of the MOSAICS study such as developing a self-management guidebook for patients with OA and participant information sheets [33, 42]). Regular meetings were set up for these. Though there were extended gaps between meetings regarding the OA QI (UK) development, the timings of the meetings were governed by the MOSAICS study timeline. However, RUG members were provided with feedback of the meeting and given the opportunity to comment. This process built upon existing working relationships and trust between the RUG and researchers.
The research team embraced the contribution of the RUG members and implemented many of their suggestions. The concepts included in the finalised OA QI (UK) were generated by the RUG members. Working in collaboration the RUG members and the research team shaped the items in survey questions suitable for use in a research trial. The Chief Investigator did not make decisions on the final content of the questionnaire without the fully informed RUG and explained if information was already captured elsewhere in the MOSAICS study. For example, RUG members did identify eight other important and relevant QIs not included in the final version of the OA QI (UK). So, to avoid repetition and participant burden in the MOSAICS study, these eight items were not included in the final 15-item OA QI (UK) questionnaire. These decisions were fully explained to the RUG members. Therefore, the RUG members' contribution ensured that the resulting OA QI (UK) incorporated issues relevant to patients with OA, written in a language that patients found easy to understand.
The OA QI (UK) was developed to assess the uptake of treatment recommended by NICE [3] and complements the new NICE Quality Standards of Care for OA [15]. Using evidence from a systematic review [8], the OA QI (UK) is a 15-item questionnaire that covers treatments offered by healthcare professionals in primary care. The OA QI (UK) supports the recently published NICE Quality Standards of Care for OA [17] and the European Musculoskeletal Conditions Surveillance and Information Network (eumusc.net) recommendations for the OA Standards of Care across European member states [43]. For example, it captures five of the eight NICE quality statements either fully or partially from a patient’s viewpoint. The OA QI (UK) and the Norwegian OA-QI also sit alongside established outcome measures of OA management and provide process measures of the quality of OA care. The eumusc.net has developed OA health care quality indicators (HCQI-OA) and an accompanying audit tool for clinicians and health care providers [44]. The OA QI (UK) and HCQI-OA both include six similar quality indicators. This questionnaire, if used in routine practice, will have the patients’ perspectives embedded in an evaluation of care quality. Though developed for use across primary care settings, the OA QI (UK) may be further refined to meet the specific needs and priorities of local health care settings, if required.
Establishing the measurement properties of a questionnaire is an important step in its development. The use of scientifically sound and decision-relevant measures allows the collection of evidence on the benefits of intervention (or care practices) from a patients’ perspective [45]. The OA QI (UK) and the Norwegian OA-QI were developed in parallel. Given the similarity between the construct and wording of the two questionnaires and the direct additions of items from the Norwegian OA-QI, the UK version ‘adopted’ the measurement properties of the validated Norwegian version. The comparison of the questionnaires used a translated, draft version of the Norwegian OA-QI. However, the Norwegian OA-QI was further refined with some changes to the item wording before validity and reliability testing. Though they are very similar in content and wording, the finalised, validated Norwegian OA-QI was published after the OA QI (UK) was produced and implemented in the MOSAICS study. The measurement properties of the OA QI (UK) was not tested because the 14 (out of the 15 items) were identical or contained subtle changes in wording to items in the validated Norwegian questionnaire. Therefore, conducting a full validation study on the OA QI (UK) questionnaire was not justified at this stage. However, the assumption that the measurement properties of the two questionnaires are similar may need further exploration.
The overall positive feedback from RUG members on the Norwegian OA-QI enabled adaptations to the OA QI (UK) to be made with confidence. The development of the both questionnaires was coincidental. Although there was differences in how they were developed (one mainly patient-led and the other mainly researcher/clinician derived), this study has demonstrated that patients and researchers have similar expectations about what constitutes good quality care in OA in different European countries. It also highlights the value of the active, meaningful and useful contribution of patients in the research process. Furthermore, the consistency of quality indicators for OA consultations in two European countries has now provided a unique opportunity to compare QIs across European countries [46]. This may lead to the development of a single, combined questionnaire for use in routine clinical practice to assess the quality of OA care provided to patients.
Conclusion
This study has demonstrated that active involvement of patients in research, working in partnership with researchers, identified important and relevant OA quality indicators, and developed a self-reported questionnaire to measure them. The OA QI (UK) questionnaire aligns with current national and international standards and process measures of OA care (e.g. NICE, eumusc.net) and is consistent with quality indicators validated for Norwegian OA consultations. The development of two OA quality indicator questionnaires was coincidental but has led to further research to compare patient-reported OA QIs across European countries. Following this work, a single refined OA QI questionnaire for use in routine clinical practice is planned.
Abbreviations
- eumusc.net:
-
European musculoskeletal conditions surveillance and information network
- GP:
-
general practitioner
- GRIPP:
-
guidance for reporting involvement of patients and public
- HCQI-OA:
-
health care quality indicators for osteoarthritis
- MOSAICS:
-
Management of OSteoArthritis In ConsultationS
- NICE:
-
National Institute for Health and Care Excellence
- OA:
-
osteoarthritis
- PPI:
-
patient and public involvement
- QI(s):
-
quality indicator(s)
- RUG:
-
research user group
- UK:
-
United Kingdom
References
Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–223.
Arthritis Research UK. Osteoarthritis in general practice: Data and perspectives. http://www.arthritisresearchuk.org/~/media/Files/Policy%20files/Policy%20pages%20files/la=en. Accessed 22 December 2014.
National Institute for Health and Care Excellence. CG177 osteoarthritis: Care and management in adults. https://www.nice.org.uk/guidance/cg177. Accessed 23 December 2014.
Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72:1125–35.
Cook C, Pietrobon R, Hegedus E. Osteoarthritis and the impact on quality of life health indicators. Rheumatol Int. 2007;27:315–21.
Darzi A. High Quality Care for all: NHS Next Stage Review Final Report. London: The Stationery Office; 2008.
Porcheret M, Jordan K, Jinks C. P. Croft in collaboration with the Primary Care Rheumatology Society. Primary care treatment of knee pain—a survey in older adults. Rheumatology. 2007;46:1694–700.
Edwards JJ, Khanna M, Jordan KP, Jordan JL, Bedson J, Dziedzic KS. Quality indicators for the primary care of osteoarthritis: a systematic review. Ann Rheum Dis. 2015;74:490–8.
Ganz DA, Chang JT, Roth CP, Guan M, Kamberg CJ, Niu F, et al. Quality of osteoarthritis care for community-dwelling older adults. Arthritis Care Res. 2006;55:241–7.
Steel N, Maisey S, Clark A, Fleetcroft R, Howe A. Quality of clinical primary care and targeted incentive payments: an observational study. Br J Gen Pract. 2007;57:449–54.
Steel N, Bachmann M, Maisey S, Shekelle P, Breeze E, Marmot M, et al. Self reported receipt of care consistent with 32 quality indicators: national population survey of adults aged 50 or more in England. BMJ. 2008;337:a957.
Broadbent J, Maisey S, Holland R, Steel N. Recorded quality of primary care for osteoarthritis: an observational study. Br J Gen Pract. 2008;58:839–43.
Mann C, Gooberman-Hill R. Health care provision for osteoarthritis: concordance between what patients would like and what health professionals think they should have. Arthritis Care Res. 2011;63:963–72.
Jinks C, Ong BN, Richardson J. A mixed methods study to investigate needs assessment for knee pain and disability: population and individual perspectives. BMC Musculoskelet Disord. 2007;8:1–9.
Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012;64:465–74.
Zhang W, Moskowitz R, Nuki G, Abramson S, Altman R, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. 2008;16:137–62.
National Institute for Health and Care Excellence. Quality standard for osteoarthritis (QS87). https://www.nice.org.uk/guidance/qs87. Accessed June, 22 2015.
eumusc.net. Standards of care for people with osteoarthritis . http://www.eumusc.net/myUploadData/files/OA_Full_draft_FINAL[1].pdf. Accessed 03/09 2015.
Goodwin N, Curry N, Naylor C, Ross S, Duldig W. Managing people with long-term conditions. London: The Kings Fund; 2010.
Edwards JJ, Jordan KP, Peat G, Bedson J, Croft PR, Hay EM, et al. Quality of care for OA: the effect of a point-of-care consultation recording template. Rheumatology (Oxford). 2015;54:844–53.
Keele University. The osteoarthritis (OA) e-template. http://www.keele.ac.uk/pchs/disseminatingourresearch/researchtools/oae-template/. Accessed 23 July 2015.
Marshall M, Campbell S, Hacker J, Roland M. Quality Indicators for General Practice. A Practical Guide for Health Professionals and Managers. London: Royal Society of Medicine Press Ltd; 2002.
Raleigh V, Foot C. Getting the measure of quality: Opportunities and challenges. London: The King's Fund; 2010.
Dziedzic KS, Healey EL, Porcheret M, Ong B, Main CJ, Jordan KP, et al. Implementing the NICE osteoarthritis guidelines: a mixed methods study and cluster randomised trial of a model osteoarthritis consultation in primary care - the Management of OsteoArthritis In Consultations (MOSAICS) study protocol. Implement Sci. 2014;9:95.
INVOLVE. Briefing note three: Why involve members of the public in research? http://www.invo.org.uk/posttyperesource/why-should-members-of-the-public-be-involved-in-research/. Accessed 23 December 2014.
National Institute for Health Research. Public involvement in your research. http://www.nihr.ac.uk/funding/public-involvement-in-your-research.htm. Accessed 23 December 2014.
National Institutes of Health. Get Involved at NIH. http://www.nih.gov/about-nih/what-we-do/get-involved-nih. Accessed 23 December 2014.
INVOLVE. Briefing note eight: Ways that people can be involved in the research cycle. http://www.invo.org.uk/posttyperesource/where-and-how-to-involve-in-the-research-cycle/. Accessed 3 October 2015.
Østerås N, Garratt A, Grotle M, Natvig B, Kjeken I, Kvien TK, et al. Patient-reported quality of care for osteoarthritis: development and testing of the OsteoArthritis quality indicator questionnaire. Arthritis Care Res. 2013;65:1043–51.
Staniszewska S, Brett J, Mockford C. The GRIPP checklist:strengthening the quality of patient and public invovlement in research. Int J Technol Assess Health Care. 2011;27:391–9.
Jinks C, Carter P, Rhodes C, Beech R, Dziedzic K, Hughes R, et al. Sustaining patient and public involvement in research: a case study of a research centre. J Care Serv Manage. 2013;7:146–54.
Jinks C, Ong BN, O'Neill TJ. The Keele community knee pain forum: action research to engage with stakeholders about the prevention of knee pain and disability. BMC Musculoskelet Disord. 2009;10:85.
Grime J, Dudley B. Developing written information on osteoarthritis for patients: facilitating user involvement by exposure to qualitative research. Health Expect. 2014;17:164–73.
Strauss VY, Carter P, Ong BN, Bedson J, Jordan KPJ, Jinks C. Public priorities for joint pain research: results from a general population survey. Rheumatology. 2012;51:2075–82.
Carter P, Beech R, Coxon D, Thomas MJ, Jinks C. Mobilising the experiential knowledge of clinicians, patients and carers for applied health-care research. Contemp Soc Sci. 2013;8:307–20.
Williamson T, Kenney L, Barker AT, Cooper G, Good T, Healey J, et al. Enhancing public involvement in assistive technology design research. Disabil Rehabil Assist Technol. 2014;10:258–65.
Gooberman-Hill R, Horwood J, Calnan M. Citizens' juries in planning research priorities: process, engagement and outcome. Health Expect. 2008;11:272–81.
NIHR. School for Primary Care Research. Patient and Public Involvement: Case Studies in Primary Care Research. Oxford: NIHR School for Primary Care Research; 2014.
National Research Ethics Committee, INVOLVE. Patient and public involvement in research and research ethics committee review. http://www.invo.org.uk/posttypepublication/patient-and-public-involvement-in-research-and-research-ethics-committee-review/. Accessed 23 December 2014.
Hewlett SA. Patients and clinicians have different perspectives on outcomes in arthritis. J Rheumatol. 2003;30:877–9.
Asadi-Lari M, Tamburini M, Gray D. Patients' needs, satisfaction, and health related quality of life: towards a comprehensive model. Health Qual Life Outcomes. 2004;2:32.
Higginbottom A, Jinks C, Bird J, Rhodes C, Blackburn S, Dziedzic K. From Design to Implementation – Patient and Public Involvement in an Nihr Research Programme in Osteoarthritis in Primary Care. Ann Rheum Dis. 2015;74:69.
eumusc.net. Musculoskeletal conditions health care quality indicators (WP6). http://www.eumusc.net/workpackages_wp6.cfm. Accessed 23 December 2014.
eumusc.net. Audit tool OA. http://eumusc.net/myUploadData/files/Audit%20HCQI_OA_1-12.pdf. Accessed 23 December 2014.
Porcheret M, Grime J, Main C, Dziedzic K. Developing a model osteoarthritis consultation: a Delphi consensus exercise. BMC Musculoskelet Disord. 2013;14:25.
Østerås N, Jordan K, Clausen B, Cordeiro C, Dziedzic K, Edwards J, et al. Self-reported quality care for knee osteoarthritis; comparisons across Denmark, Norway, Portugal and United Kingdom. RMD Open. 2015;1:e000136.
Acknowledgements
This work presented in this paper was paper presents independent research commissioned by the National Institute for Health Research (NIHR) Programme Grant (RP-PG-0407-10386). The views expressed in this paper are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. We are grateful to the Primary Care Research Consortium Board and by Arthritis Research UK for their support of the RUG. The authors would especially like to thank the OA Research User Group (Jo Bird, Brian Dudley, Teresa George, John Murphy, Chris Pope, Jeannette Shipley, Alan Sutton, Robert Taylor, Christine Walker, Anne Worral) for all their support and assistance with this study. We are also thankful to Carol Rhodes and June Handy for their time and effort supporting and working with the RUG. Time for CJ and KD was part funded by the National Institute for Health Research (NIHR) Collaborations for Leadership in Applied Research and Care West Midlands. KD is part-funded by Knowledge Mobilisation Fellowships from the NIHR (KMRF-2014-03-002).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
K.D. has been an invited speaker to the European League Against Rheumatism (EULAR) conference and a member of the NICE OA guideline development group. Keele University has received payments and reimbursements of travel and other expenses related to these activities. K.D. has no financial relationships with any organizations that may have an interest in the submitted work in the previous 3 years. J.J.E. provides general medical services and benefits financially from the Quality & Outcomes Framework of the General Medical Services contract; he has also been an invited speaker to the European League Against Rheumatism (EULAR) conference. All other authors have declared no conflicts of interest.
Authors’ contribution
SB and KD wrote the first draft of the paper; AH and RT (Lay members of the OA Research User Group) wrote the plain English summary. AH, RT, JB, NØ, KB, JE, KJ, CJ gave detailed comments for the final submission. All authors read and approved the final manuscript.
Additional files
Additional file 1:
Overview of the Managing Osteoarthritis in Consultations (MOSAICS) study. (DOCX 12 kb)
Additional file 2:
Overview of Patient and Public Involvement in the Institute of Primary Care and Health, Keele University. (DOCX 12 kb)
Additional file 3:
The Osteoarthritis Quality Indicators (UK) Questionnaire. (DOCX 56 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Blackburn, S., Higginbottom, A., Taylor, R. et al. Patient-reported quality indicators for osteoarthritis: a patient and public generated self-report measure for primary care. Res Involv Engagem 2, 5 (2016). https://doi.org/10.1186/s40900-016-0019-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40900-016-0019-x