
Abstract
Background
This study aimed to compare the effects of Linagliptin and Empagliflozin on renal function and glycaemic control in patients with type 2 diabetes mellitus (DM).
Method
We conducted a randomized, double-blind, parallel trial on patients aged 30 to 80 years with type 2 DM and HbA1c ≤ 9%, regardless of background medical therapy, to compare the effects of Empagliflozin and Linagliptin on albuminuria, FBS, HbA1c, and eGFR. Participants were given the mentioned drugs for 12 weeks. Statistical analysis was performed using appropriate tests in IBM™SPSS® statistics software for windows version 24.
Results
In total, 60 patients participated in the study, thirty patients in each group. The mean age of participants was 56.8 (SD = 8.15) in the Empagliflozin group and 60.9 (SD = 7.22) in the Linagliptin group. Before the intervention, FBS, HbA1C, and albuminuria values were significantly higher in the Empagliflozin group than those in the Linagliptin group (P < 0.05), but there was no significant difference between groups regarding eGFR (P = 0.271). Changes in the FBS, HbA1C, and eGFR were not significantly different between groups (P > 0.05), but there was more decrease in albuminuria in the Empagliflozin group compared to the Linagliptin group (P = 0.001, Cohen’s d = 0.98).
Conclusions
Regardless of baseline albuminuria, eGFR, or HbA1c, Empagliflozin 10 mg daily significantly reduced albuminuria at 12 weeks compared to Linagliptin 5 mg daily in patients with type 2 diabetes.
Trial registration
Iranian Registry of Clinical Trials, IRCT20200722048176N1. Registered 3 August 2020.
Similar content being viewed by others

Background
Diabetes Mellitus (DM) is a debilitating metabolic disorder characterized by impaired insulin function, leading to chronic hyperglycemia [1]. Two main types of DM are type 1, insulin-dependent, and type 2, insulin-independent, and insulin resistance plays a crucial role in type 2 DM [2]. In 2017, it was estimated that the global prevalence of type 2 DM is about 6.28%, with about 462 million people being affected [3]. Additionally, approximately 193 million diabetic patients worldwide remain undiagnosed, putting them at risk of untreated chronic hyperglycemia complications [4]. Chronic hyperglycemia can cause microvascular and macrovascular complications. Several metabolic and structural alterations contribute to these vascular complications, such as the accumulation of glycation end products, improper stimulation of signal pathways like protein kinase C and hemodynamic regulatory mechanism of the renin–angiotensin–aldosterone system (RAAS), and excessive production of reactive oxygen species (ROS) [5].
Diabetic nephropathy (DN) is one of the most common and severe microvascular complications of DM, occurring in about 20–30% of diabetic patients [6, 7], which is typically defined as increased excretion of protein in the urine [8]. However, in some countries, as high as 45% of patients with type 2 DM are reported to have DN [9]. One of the major consequences of DN is kidney failure, leading to end-stage renal disease (ESRD), advanced cardiovascular disease, and death [10]. Even with extensive lifestyle and drug interventions [11], DN still accounts for the majority of cases of ESRD and triple the risk of dying from it [12].
A growing concern during the course of type 2 DM is the prevention or delay of the progression of DN, especially with its increasing incidence each year. Early-stage DN causes glomerulosclerosis, compensatory hypertrophy, and late-stage DN leads to gradual atrophy [13]. Treatment of DN consists of different interventions, including changes in lifestyle, glycaemic control, and pharmaceutical treatments [14]. Poor glycaemic control is associated with more severe DN [15], with glycaemic control can prevent the incidence of DN and slow its progression [16]. Glycemic control can also, in the long term, reverse some kidney histological changes in patients with type 2 DM [17]. Therefore, glycaemic control is one of the cornerstones of type 2 DM treatment [14]. Sodium-glucose cotransporter-2 inhibitors (SGLT2i) are one of the suggested pharmaceutical agents for glycaemic control in patients with diabetes, and concurrent DN, especially those with an estimated glomerular filtration rate (eGFR) of higher than 30 ml/min, high risk of hospitalization due to heart failure or atherosclerotic cardiovascular diseases [18]. In addition to glycaemic control, SGLT2 inhibitors can prevent glomerular injury. There are some hypotheses regarding the mechanisms of these beneficial effects of SGLT2 inhibitors on renal function, including their positive effects on risk factors of DN, reducing glomerular capillary pressure, decreasing inflammation, activating renin-angiotensin system (RAS), and decreasing podocyte damage; however, the exact mechanism is unknown [19]. Empagliflozin is an SGLT2i that has anti-fibrotic and anti-inflammatory effects and can slow the progression of DN [20,21,22].
Dipeptidyl peptidase-4 (DPP-4) inhibitors are another group of medications used for glycaemic control and treatment of DN in patients with type 2 DM [23, 24]. DDP-4 enzymes are suggested to have roles in the progression of kidney injury in patients with DN considering their inflammatory functions [25]. Therefore, inhibiting DDP-4 function is one of the therapeutic targets in patients with DN; however, there are controversies regarding the effects of DDP-4 inhibitors on kidney injury in these patients [25]. Linagliptin is one of the DDP-4 inhibitors which has been utilized for the treatment of DN. In a study by Groop et al., 5 mg of Linagliptin per day in combination with a renin–angiotensin–aldosterone system (RAAS) inhibitor had positive impacts on albuminuria and Hemoglobin A1C (HbA1C) levels in patients with type 2 DM compared to RAAS inhibitor alone [26]. However, Linagliptin did not have similar efficacy on the renal function when used alone [27].
To summarize, Empagliflozin and Linagliptin are two medications of different classes that have been used mainly for glycaemic control in patients with type 2 DM. Besides, Empagliflozin is one of the agents that has beneficial effects on renal function and has been used for this purpose. However, studies on the efficacy of Linagliptin are limited, and there are controversies in this regard. Therefore, to address these controversies on Linagliptin effects, this study aimed to compare the effects of Linagliptin and Empagliflozin on renal function and glycaemic control in patients with type 2 DM.
Methods
We ran a randomized, double-blind, parallel trial (Iranian Registry of Clinical Trials identifier: IRCT20200722048176N1) to compare the effects of Emplagiflozin 10 mg once daily and Linagliptin 5 mg once daily on albuminuria, fasting blood sugar (FBS), HbA1c, and eGFR in patients with type 2 DM. All patients were informed in detail about the study, and verbal and written informed consent were obtained. The study design entirely was approved by the Human Ethics Committee of the Arak University of Medical Sciences (ethics code: 1399.127.REC.ARAKMU.IR).
Trial population
The current study was conducted on patients with type 2 diabetes mellitus in Amir-al-Momenin hospital, Arak city, Iran, from September 2020, to May 2021. Patients aged 30 to 80 years and HbA1c ≤ 9% regardless of any background anti-diabetic therapy were eligible for inclusion. The dose of the background glucose-lowering drug was required to be unchanged at least 12 weeks before randomization. Exclusion criteria were: history of myocardial infarction or congestive heart failure less than three months before the study, hematuria, presence of urinary foley catheter, active urinary tract infection, and any renal diseases resulting in albuminuria at the time of inclusion.
Intervention
Patients were divided into two groups. One group received Empagliflozin 10 mg once daily, and the other group received Linagliptin 5 mg once daily. Both medications were added to the patients’ previous anti-glycemic agents, and patients in both groups received these medications for 12 weeks. The dosage of medications was determined based on the recommendations for the treatment of patients with DM [28, 29].
Primary and secondary outcomes
In our study, primary outcomes were changes in albuminuria and eGFR, and secondary outcomes were changes in HbA1c and FBS after 12 weeks of treatment. The subjects were required to fast for 8 to 10 h before collecting the blood samples to evaluate FBS, creatinin for calculation of GFR, and HbA1C. Also, we used a spot morning urine sample for evaluation of albuminuria. The following formula was used for the calculation of GFR based on the creatinine levels. The calculated value was multiplied by 0.85 if the patient was female.:
Blinding and randomization
For the purpose of blinding, drugs were removed from their original packages and were re-packed in look-alike packages, and neither the patients nor the instructors were informed about the contents of the packages. Patients were randomized 1:1 in a block size of 6 to receive either Empagliflozin 10 mg once daily or Linagliptin 5 mg once daily, and treatment allocation was performed by a random sequence generated by a computer. However, no allocation concealment was done.
Statistical Analysis
We calculated the mean and standard deviation (SD) for continuous variables. We used Kolmogorov–Smirnov (KS) test to evaluate the distribution of values of each variable. We used non-parametric tests, including the Mann–Whitney U test and Wilcoxon signed ranks test, to compare the FBS, HbA1C, and albuminuria between groups as they were not distributed normally (P < 0.05). For other variables, we used parametric tests, such as the T-test, as they were distributed normally (P > 0.05). We used univariate analysis of variances to assess the effects of confounders. We calculated Cohen’s D to evaluate the effects of medications where we find significant differences in the changes of variables between groups. We considered P ≤ 0.05 as statistically significant. We used IBM™SPSS® statistics software for windows version 24 for statistical analysis of the data.
Results
In total, 73 patients were assessed for the eligibility criteria, and 12 individuals were excluded as they did not meet the eligibility criteria, and one declined to participate in the study. Therefore, 60 patients were randomized into two intervention groups (Fig. 1). In both groups, nine patients were male, and 21 were female. The basic characteristics of participants are shown in Table 1. Patients who received Empagliflozin had significantly higher body mass index (BMI) than those in the Linagliptin roup (P = 0.049), but there were no other differences between groups regarding the basic characteristics, including age and gender (P > 0.05).

Flow diagram of participants enrollment
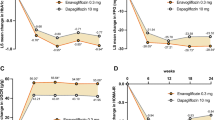
Clinical characteristics of participants are shown in Table 2. Before the intervention, FBS, HbA1C, and albuminuria values were significantly higher in the Empagliflozin group than those in the Linagliptin group (P < 0.05). After the intervention, no significant differences were seen between groups regarding the outcomes (P > 0.05).
GFR, albuminuria, FBS, and HbA1C values were significantly improved in patients who received Empagliflozin (P < 0.001). In the Linagliptin group, GFR was significantly decreased after the intervention (P < 0.001). Also, FBS and albuminuria did not significantly change after the treatment (P > 0.05). The only significant improvement in the Linagliptin group was in the HbA1C values, as HbA1C values were significantly decreased after the course of treatment (P = 0.002).
The decrease in albuminuria was greater in the Empagliflozin group compared to the Linagliptin group (P = 0.001, Cohen’s d = 0.98).). After adjusting for baseline values of albuminuria and HbA1C, changes in the albuminuria were significantly different between groups in favor of the Empagliflozin group (P < 0.001). Changes in GFR, FBS, and HbA1C were not significantly different between groups (P > 0.05).
Discussion
In this double-blind, randomized clinical trial comparing the effectiveness of Empagliflozin and Linagliptin in patients with type 2 DM, Empagliflozin emerged superior in efficacy regarding reducing albuminuria in the short term follow up of 12 weeks, regardless of their pre interventional renal function, BMI, and HbA1C, which is in line with previous studies. In a study by Lee et al., comparing the adverse kidney outcomes in patients with type 2 DM who received Empagliflozin or Linagliptin, it was found that decline in GFR was slower in patients who received Empagliflozin compared to those who received Linagliptin [30]. Also, they found that the risk of acute kidney injury (AKI) is lower in patients who receive Empagliflozin compared to those who received Linagliptin [30]. These findings indicate that Empagliflozin might be superior than Linagliptin in the management of DN not only in the trial condition, but also in the real-world situation.
In 2017 Groop et al. conducted a randomized clinical trial, MARLINA, comparing the effectiveness of Linagliptin versus placebo in reducing the albuminuria in patients with type 2 DM in a more extended period of follow up, 24 weeks [31]. In their study, no superiority was found in favor of Linagliptin in reducing albuminuria. However, in another randomized trial, CARMELINA, after a median follow-up of 2.2 years, Linagliptin reduced the albuminuria compared to placebo [32]. Although it has been reported that Linagliptin can prevent the progression of albuminuria in 2.2 years in different studies [33, 34], its efficacy in reducing albuminuria in the short term is still controversial. In a retrospective analysis of four randomized trials, significant efficacy of Linagliptin in lowering the albuminuria 24 weeks after randomization was found [26]. Han et al. in 2017 enrolled patients with an estimated eGFR of 15–59 in a randomized clinical trial to compare the efficacy of Linagliptin with Empagliflozin. After 40 weeks: they observed no statistically significant change in albuminuria in either group in this period [35].
Glycoprotein DPP-4, which has been found in healthy individuals in two forms of circulating soluble and membrane-bound with a predominancy in proximal convoluted tubules [36], was also expressed in glomeruli as an adaptive mechanism in patients with chronic kidney disease [37]. So a hypothesis was brought out of the renoprotective role of DPP-4 inhibitors and later demonstrated a reduction in albuminuria in mice with type 2 DM [38]. As a DPP-4 inhibitor, Linagliptin has shown to act as a renoprotective agent through the prevention of endothelial to mesangial transition [39] and its anti-fibrotic effects [40, 41]. For example, in an experimental study in 2016 in mice, using Linagliptin, a DPP-4 inhibitor, was associated with upregulation of stromal cell-derived Factor-1, which contributes as an antioxidative and anti-fibrotic agent in the pathophysiology of diabetic nephropathy [42]. Another study investigating the role of DPP-4 in kidney disease suggested Linagliptin as an inhibitor of podocyte growth, which could reduce albuminuria with Linagliptin in the long term [43].
On the other hand, SGLT2, a transport protein in proximal convoluted tubules contributing to sodium-glucose reabsorption, can be inhibited by Empagliflozin, mediating the reduction in blood pressure intraglomerular filtration, which seems to lead to a reduction in albuminuria in a short time. Beyond alleviation of patients’ hemodynamic status, histopathologic effects of SGLT-2 inhibitors could mediate a reduction in their albuminuria. In 2020, Klimontov et al. administered Empagliflozin to diabetic mice. As well as a reduction of urinary albumin-to-creatinine ratio, it showed a reduction in kidney hypertrophy, mesangial expansion, basement membrane thickening, and podocytopathy of glomeruli [44] that could explain its long-term efficacy in patients with DN.
Beyond Empagliflozin association with eGFR preservation and reduced risk of major adverse kidney events reported in a cohort study of 379,033 participants [45] and EMPA-REG trial [46], several studies have been designed to evaluate its efficacy in reducing albuminuria. Cherney et al. in 2017 evaluated the efficacy of Empagliflozin compared to placebo in reducing albuminuria in a median treatment duration of 2.6 years, and in line with the current study, they found the reduction in UACR occurs as early as week 12 [47]. Furthermore, a post hoc analysis of the EMPA-REG OUTCOME trial revealed a sustained reduction in UACR after a median follow-up of 3.1 years [48].
An intriguing conclusion was brought out of the EMPA-REG trial regarding the importance of early albuminuria reduction, where each 30% reduction of UACR was associated significantly with a lower hazard for major cardiovascular events [49]. In this regard, decreasing albuminuria in diabetic patients as early as possible could be very beneficial. To the best of our knowledge, this current study is the first clinical double-blind trial that revealed the superiority of Empagliflozin to Linagliptin. In a randomized trial by Cooper et al. in 2018, it was shown that Linagliptin did not change the hemodynamic status of patients with Type 2 DM in a period of 24 weeks [50], while some other studies, including a clinical trial of patients with Type 2 DM [51] and a post hoc analysis of two cohorts of randomized trials in patients with Type 2 DM [52], showed the Empagliflozin reducing effect on both systolic and diastolic blood pressure at weeks 8, 12, and 24, respectively.
There was a heterogeneity regarding the FBS, HbA1C, and albuminuria values between the groups, which should be considered in the interpretation of the current study’s findings. We used blocked randomization in our study to ensure the same number of participants would be enrolled in each group. However, there is a risk of imbalance regarding the prognostic factors while using block randomization, which might be even increased in the context of our study considering the small number of our sample size [53]. Adjusting for baseline values of albuminuria and HbA1C before comparing changes in the albuminuria between groups was a strategy used in this study to overcome this limitation. Also, baseline characteristics of participants indicated poorer diabetes control in individuals in the Empagliflozin group, which might be due to less adherence to treatment or being in more advanced stages of diabetes. Therefore, observing the effectiveness of Empagliflozin compared to Linagliptin even in patients with poorer conditions might be another factor in favor of Empagliflozin. Also, we did not perform allocation concealment due to limitations in resources for conducting this study in our center, which is another factor that should be considered in the interpretation of the findings as due to lack of allocation concealment, our study might be subject to selection bias [54].
This study has several limitations suggested to be considered in future studies. First of all, it is better to follow up patients for more extended periods to meet the albuminuria-lowering effects of Linagliptin and their probable adverse complications. On the other hand, stratified randomized sampling according to potential confounders would yield more reliable findings, and a larger sample size with various ethnicities could enhance the power of the study. Also, we did not record the anti-glycemic agents that patients were taking before participating in this study, which can be a confounder for our results. Future studies evaluating pre-enrollment medications may be useful for more careful comparison of the effects of these medications. Finally, we did not perform allocation concealment and did not record the side effects in this study, and future well-designed controlled trials are needed to compare the effects of Empagliflozin and Linagliptin better.
Conclusion
Regardless of baseline albuminuria, eGFR, or HbA1c, Empagliflozin 10 mg daily significantly reduced albuminuria at 12 weeks compared to Linagliptin 5 mg daily in patients with type 2 diabetes.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body Mass Index
- DM:
-
Diabetes Mellitus
- DN:
-
Diabetic Nephropathy
- DPP-4:
-
Dipeptidyl Peptidase-4
- eGFR:
-
Estimated Glomerular Filtration Rate
- ESRD:
-
End-Stage Renal Disease
- FBS:
-
Fasting Blood Sugar
- HbA1C:
-
Hemoglobin A1C
- KS:
-
Kolmogorov–Smirnov
- RAAS:
-
Renin–Angiotensin–Aldosterone System
- RAS:
-
Renin-Angiotensin System
- ROS:
-
Reactive Oxygen Species
- SD:
-
Standard Deviation
- SGLT2i:
-
Sodium-Glucose Cotransporter-2 inhibitors
References
National Diabetes Statistics Report. Centers for Disease Control and Prevention, US Dept of Health and Human Services 2017. 2017.
Zaccardi F, Webb DR, Yates T, Davies MJ. Pathophysiology of type 1 and type 2 diabetes mellitus: a 90-year perspective. Postgrad Med J. 2016;92(1084):63–9.
Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al KJ. Epidemiology of type 2 diabetes–global burden of disease and forecasted trends. J Epidemiol Global Health. 2020;10(1):107.
Chawla A, Chawla R, Jaggi S. Microvasular and macrovascular complications in diabetes mellitus: Distinct or continuum? Indian J Endocrinol Metabolism. 2016;20(4):546–51.
Braunwald E. Diabetes, heart failure, and renal dysfunction: The vicious circles. Prog Cardiovasc Dis. 2019;62(4):298–302.
Murea M, Ma L, Freedman BI. Genetic and environmental factors associated with type 2 diabetes and diabetic vascular complications. Rev Diabetic Stud : RDS. 2012;9(1):6–22.
Koye DN, Shaw JE, Reid CM, Atkins RC, Reutens AT, Magliano DJ. Incidence of chronic kidney disease among people with diabetes: a systematic review of observational studies. Diabetic Med : J Br Diabetic Assoc. 2017;34(7):887–901.
Rieg T, Masuda T, Gerasimova M, Mayoux E, Platt K, Powell DR, et al. Increase in SGLT1-mediated transport explains renal glucose reabsorption during genetic and pharmacological SGLT2 inhibition in euglycemia. Am J Physiol Renal Physiol. 2014;306(2):F188–93.
Aldukhayel A. Prevalence of diabetic nephropathy among Type 2 diabetic patients in some of the Arab countries. Int J Health Sci. 2017;11(1):1.
Lim A. Diabetic nephropathy - complications and treatment. Int J Nephrol Renov Dis. 2014;7:361–81.
Muskiet MH, Tonneijck L, Smits MM, Kramer MH, Heerspink HJ, van Raalte DH. Pleiotropic effects of type 2 diabetes management strategies on renal risk factors. Lancet Diabetes Endocrinol. 2015;3(5):367–81.
Rao KondapallySeshasai S, Kaptoge S, Thompson A, Di Angelantonio E, Gao P, Sarwar N, et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N Engl J Med. 2011;364(9):829–41.
Glassock RJ, Rule AD. The implications of anatomical and functional changes of the aging kidney: with an emphasis on the glomeruli. Kidney Int. 2012;82(3):270–7.
Selby NM, Taal MW. An updated overview of diabetic nephropathy: Diagnosis, prognosis, treatment goals and latest guidelines. Diabetes Obes Metab. 2020;22:3–15.
Dr M, DR H, Atkinson A, Johnston H, Kennedy L. The relationship between long-term glycaemic control and diabetic nephropathy. QJM: Int J Med. 1992;82(1):53–61.
Alaveras A, Thomas S, Sagriotis A, Viberti G. Promoters of progression of diabetic nephropathy: the relative roles of blood glucose and blood pressure control. Nephrol Dial Transplant. 1997;12:71–4.
Fioretto P, Steffes MW, Sutherland DE, Goetz FC, Mauer M. Reversal of lesions of diabetic nephropathy after pancreas transplantation. N Engl J Med. 1998;339(2):69–75.
Li J, Albajrami O, Zhuo M, Hawley CE, Paik JM. Decision algorithm for prescribing SGLT2 inhibitors and GLP-1 receptor agonists for diabetic kidney disease. Clin J Am Soc Nephrol. 2020;15(11):1678–88.
Barutta F, Bernardi S, Gargiulo G, Durazzo M, Gruden G. SGLT2 inhibition to address the unmet needs in diabetic nephropathy. Diabetes Metab Res Rev. 2019;35(7):e3171.
Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323–34.
Ojima A, Matsui T, Nishino Y, Nakamura N, Yamagishi S. Empagliflozin, an inhibitor of sodium-glucose cotransporter 2 exerts anti-inflammatory and anti-fibrotic effects on experimental diabetic nephropathy partly by suppressing AGEs-receptor axis. Horm Metab Res. 2015;47(09):686–92.
Inzucchi SE, Fitchett D, Jurišić-Eržen D, Woo V, Hantel S, Janista C, et al. Are the cardiovascular and kidney benefits of empagliflozin influenced by baseline glucose-lowering therapy? Diabetes Obes Metab. 2020;22(4):631–9.
Sato Y, Kamada T, Yamauchi A. The role of dipeptidyl peptidase 4 (DPP4) in the preservation of renal function: DPP4 involvement in hemoglobin expression. J Endocrinol. 2014;223(2):133–42.
Deacon CF. Physiology and pharmacology of DPP-4 in glucose homeostasis and the treatment of type 2 diabetes. Front Endocrinol. 2019;10:80.
Nistala R, Savin V. Diabetes, hypertension, and chronic kidney disease progression: role of DPP4. Am J Physiol-Renal Physiol. 2017;312(4):F661–70.
Groop P-H, Cooper ME, Perkovic V, Emser A, Woerle H-J, Von Eynatten M. Linagliptin lowers albuminuria on top of recommended standard treatment in patients with type 2 diabetes and renal dysfunction. Diabetes Care. 2013;36(11):3460–8.
McGill JB, Sloan L, Newman J, Patel S, Sauce C, Von Eynatten M, et al. Long-term efficacy and safety of linagliptin in patients with type 2 diabetes and severe renal impairment: a 1-year, randomized, double-blind, placebo-controlled study. Diabetes Care. 2013;36(2):237–44.
Deeks ED. Linagliptin Drugs. 2012;72(13):1793–824.
Sizar O, Podder V, Talati R. Empagliflozin. StatPearls. 2020.
Lee Y-T, Hsu C-N, Fu C-M, Wang S-W, Huang C-C, Li L-C. Comparison of adverse kidney outcomes with empagliflozin and linagliptin use in patients with type 2 diabetic patients in a real-world setting. Front Pharmacol. 2021;12(12):781379.
Groop PH, Cooper ME, Perkovic V, Hocher B, Kanasaki K, Haneda M, et al. Linagliptin and its effects on hyperglycaemia and albuminuria in patients with type 2 diabetes and renal dysfunction: the randomized MARLINA-T2D trial. Diabetes Obes Metab. 2017;19(11):1610–9.
Wanner C, Cooper ME, Johansen OE, Toto R, Rosenstock J, McGuire DK, et al. Effect of linagliptin versus placebo on cardiovascular and kidney outcomes in nephrotic-range proteinuria and type 2 diabetes: the CARMELINA randomized controlled trial. Clin Kidney J. 2021;14(1):226–36.
Inagaki N, Yang W, Watada H, Ji L, Schnaidt S, Pfarr E, et al. Linagliptin and cardiorenal outcomes in Asians with type 2 diabetes mellitus and established cardiovascular and/or kidney disease: subgroup analysis of the randomized CARMELINA((R)) trial. Diabetol Int. 2020;11(2):129–41.
Perkovic V, Toto R, Cooper ME, Mann JFE, Rosenstock J, McGuire DK, et al. Effects of Linagliptin on Cardiovascular and Kidney Outcomes in People With Normal and Reduced Kidney Function: Secondary Analysis of the CARMELINA Randomized Trial. Diabetes Care. 2020;43(8):1803–12.
Han SY, Yoon SA, Han BG, Kim SG, Jo YI, Jeong KH, et al. Comparative efficacy and safety of gemigliptin versus linagliptin in type 2 diabetes patients with renal impairment: A 40-week extension of the GUARD randomized study. Diabetes Obes Metab. 2018;20(2):292–300.
Groop PH, Cooper ME, Perkovic V, Hocher B, Kanasaki K, Haneda M, et al. Linagliptin and its effects on hyperglycaemia and albuminuria in patients with type 2 diabetes and renal dysfunction: the randomized MARLINA-T2D trial. Diabetes Obes Metab. 2017;19(11):1610–9.
Stiller D, Bahn H, August C. Demonstration of glomerular DPP IV activity in kidney diseases. Acta Histochem. 1991;91(1):105–9.
Sharkovska Y, Reichetzeder C, Alter M, Tsuprykov O, Bachmann S, Secher T, et al. Blood pressure and glucose independent renoprotective effects of dipeptidyl peptidase-4 inhibition in a mouse model of type-2 diabetic nephropathy. J Hypertension. 2014;32(11):2211–23 (discussion 23).
Shi S, Srivastava SP, Kanasaki M, He J, Kitada M, Nagai T, et al. Interactions of DPP-4 and integrin beta1 influences endothelial-to-mesenchymal transition. Kidney Int. 2015;88(3):479–89.
Tsuprykov O, Ando R, Reichetzeder C, von Websky K, Antonenko V, Sharkovska Y, et al. The dipeptidyl peptidase inhibitor linagliptin and the angiotensin II receptor blocker telmisartan show renal benefit by different pathways in rats with 5/6 nephrectomy. Kidney Int. 2016;89(5):1049–61.
Kanasaki K, Shi S, Kanasaki M, He J, Nagai T, Nakamura Y, et al. Linagliptin-mediated DPP-4 inhibition ameliorates kidney fibrosis in streptozotocin-induced diabetic mice by inhibiting endothelial-to-mesenchymal transition in a therapeutic regimen. Diabetes. 2014;63(6):2120–31.
Takashima S, Fujita H, Fujishima H, Shimizu T, Sato T, Morii T, et al. Stromal cell-derived factor-1 is upregulated by dipeptidyl peptidase-4 inhibition and has protective roles in progressive diabetic nephropathy. Kidney Int. 2016;90(4):783–96.
Miglio G, Vitarelli G, Klein T, Benetti E. Effects of linagliptin on human immortalized podocytes: a cellular system to study dipeptidyl-peptidase 4 inhibition. Br J Pharmacol. 2017;174(9):809–21.
Klimontov VV, Korbut AI, Taskaeva IS, Bgatova NP, Dashkin MV, Orlov NB, et al. Empagliflozin alleviates podocytopathy and enhances glomerular nephrin expression in db/db diabetic mice. World J Diabetes. 2020;11(12):596–610.
Xie Y, Bowe B, Gibson AK, McGill JB, Yan Y, Maddukuri G, et al. Comparative Effectiveness of the Sodium-Glucose Cotransporter 2 Inhibitor Empagliflozin Versus Other Antihyperglycemics on Risk of Major Adverse Kidney Events. Diabetes Care. 2020;43(11):2785–95.
Mayer GJ, Wanner C, Weir MR, Inzucchi SE, Koitka-Weber A, Hantel S, et al. Analysis from the EMPA-REG OUTCOME((R)) trial indicates empagliflozin may assist in preventing the progression of chronic kidney disease in patients with type 2 diabetes irrespective of medications that alter intrarenal hemodynamics. Kidney Int. 2019;96(2):489–504.
Cherney DZI, Zinman B, Inzucchi SE, Koitka-Weber A, Mattheus M, von Eynatten M, et al. Effects of empagliflozin on the urinary albumin-to-creatinine ratio in patients with type 2 diabetes and established cardiovascular disease: an exploratory analysis from the EMPA-REG OUTCOME randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017;5(8):610–21.
Ferreira JP, Verma S, Fitchett D, Ofstad AP, Lauer S, Zwiener I, et al. Metabolic syndrome in patients with type 2 diabetes and atherosclerotic cardiovascular disease: a post hoc analyses of the EMPA-REG OUTCOME trial. Cardiovasc Diabetol. 2020;19(1):200.
Waijer SW, Xie D, Inzucchi SE, Zinman B, Koitka-Weber A, Mattheus M, et al. Short-Term Changes in Albuminuria and Risk of Cardiovascular and Renal Outcomes in Type 2 Diabetes Mellitus: A Post Hoc Analysis of the EMPA-REG OUTCOME Trial. J Am Heart Assoc. 2020;9(18):e016976.
Cooper ME, Perkovic V, Groop PH, Hocher B, Hehnke U, Meinicke T, et al. Hemodynamic effects of the dipeptidyl peptidase-4 inhibitor linagliptin with renin-angiotensin system inhibitors in type 2 diabetic patients with albuminuria. J Hypertens. 2019;37(6):1294–300.
Cherney DZ, Perkins BA, Soleymanlou N, Har R, Fagan N, Johansen OE, et al. The effect of empagliflozin on arterial stiffness and heart rate variability in subjects with uncomplicated type 1 diabetes mellitus. Cardiovasc Diabetol. 2014;13:28.
Chilton R, Tikkanen I, Cannon CP, Crowe S, Woerle HJ, Broedl UC, et al. Effects of empagliflozin on blood pressure and markers of arterial stiffness and vascular resistance in patients with type 2 diabetes. Diabetes Obes Metab. 2015;17(12):1180–93.
Lim C-Y, In J. Randomization in clinical studies. Korean J Anesthesiol. 2019;72(3):221.
Attia A. Bias in RCTs: confounders, selection bias and allocation concealment. Middle East fertility society journal. 2005;10(3):258.
Acknowledgements
We would like to thank patients for their participation in this study.
Funding
This study was not funded.
Author information
Authors and Affiliations
Contributions
Conceptualization: All authors. Methodology: MAMG, NS, MRR. Formal analysis and investigation: ANA. Writing—original draft preparation: FA, PY, MA, ANA. Writing – review and editing: All authors. Resources: MAMG, NS, MRR. Supervision: MRR, NS. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and/or with the Helsinki Declaration of 1964 and later versions. Informed consent or substitute for it was obtained from all patients for being included in the study. The study design entirely was approved by the Human Ethics Committee of the Arak University of Medical Sciences (ethics code: 1399.127.REC.ARAKMU.IR).
Consent for publication
N/A
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mohammad zadeh Gharabaghi, M.A., Rezvanfar, M., Saeedi, N. et al. Comparison of effects of Empagliflozin and Linagliptin on renal function and glycaemic control: a double-blind, randomized clinical trial. Clin Diabetes Endocrinol 8, 5 (2022). https://doi.org/10.1186/s40842-022-00142-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40842-022-00142-1