
Abstract
Recently, positron emission tomography (PET) imaging using PSMA-ligands has gained high attention as a promising new radiotracer in patients with prostate cancer (PC). Several studies promise accurate staging of primary prostate cancer and restaging after biochemical recurrence with 68Ga-PSMA ligand Positron emission tomography/computed tomography (PET/CT). However, prospective trials and clinical guidelines for this new technique are still missing. Therefore, we summarized our experience with 68Ga-PSMA ligand PET/CT examinations in patients with primary PC and biochemical recurrence. It focuses on the technical and logistical aspects of 68Ga-PSMA ligand PET/CT examination as well as on the specific background for image reading discussing also potential pitfalls. Further, it includes relevant issues on free-text as well as structured reporting used in daily clinical routine.
Similar content being viewed by others


Background
Prostate cancer (PC) represents the most common cancer in men and accounts for the third most cause for cancer-associated death in men [1]. Early detection of primary disease and its metastases is highly relevant in terms of prognosis and therapy management. Primary staging with conventional imaging modalities such as computed tomography (CT) or magnetic resonance imaging (MRI) is limited as these techniques focus on morphologic information and LN involvement is mainly assessed by size. Up to 50 % of all patients undergoing radical prostatectomy (RP) or radiotherapy (RT) for primary treatment of PC develop biochemical recurrence [2–4]. Therefore, precise diagnosis of recurrence is crucial for patient counselling and treatment selection. However, the limited accuracy of CT or MRI in the detection of local disease in patients with biochemical recurrence is well appreciated [5, 6].
Positron emission tomography/computed tomography (PET/CT) as a hybrid imaging technique combining functional and morphological information has been proven to exhibit high diagnostic accuracy and is increasingly established as the primary staging tool in PC and in patients with suspicious recurrent disease. Several radiotracers have been proposed for molecular imaging of PC including choline as a marker of membrane cell proliferation. For recurrent PC, choline based (i.e. either 18F-Choline or 11C-Choline) PET/CT is currently widely used in clinical routine, however, there have been numerous studies reporting a low sensitivity and specificity [7, 8]. Especially in patients with prostate-specific antigen (PSA)-values below 3 ng/ml the detection rate is reported to be only 40–60 % [9–11].
Other radiotracers evaluated for PC include 11C-Acetate and 18F-FACBC. 18F fluciclovine, a radiolabeled leucine analog (1-amino-3-fluorocyclobutane-1-carboxylic acid in the ‘anti’ configuration [18F FACBC]), is used to depict amino acid transportation and has been found to be successful in the assessment of primary and metastatic PC showing also statistically significant superior detection rates in comparison to 11C-Choline PET [12–14]. 11C-Acetate is used as a PET radiotracer for imaging PC via incorporation into intracellular phosphatidylcholine membrane microdomains in cancer cells.
Current clinical and scientific evidence for 68Ga-PSMA ligand PET/CT and potential indications
The prostate specific membrane antigene (PSMA) is a transmembrane protein with significantly elevated expression in PC cells compared to benign prostatic tissue. So far, several, mainly retrospective studies describe the value of 68Ga-PSMA ligand PET/CT in different clinical scenarios. All of them demonstrate a higher diagnostic efficacy of 68Ga-PSMA ligand PET/CT compared to conventional imaging including PET with other tracers (e.g. 18F-Choline, 11C-Choline) [7, 15–19]. In particular, 68Ga-PSMA ligand PET/CT promises accurate staging of primary PC and re-staging after biochemical recurrence. In a large study in primary intermediate to high-risk PC, 68Ga-PSMA-ligand imaging has been reported to clearly improve detection of lymph node metastases compared to morphological imaging thus potentially allowing for a more tailored therapeutic concept [16].
Similar encouraging results were obtained for patients with biochemical recurrence after radical prostatectomy [17]. Here, 68Ga-PSMA ligand PET imaging has been shown to increase detection of metastatic sites even at low PSA-values in comparison to conventional imaging or PET examination with different tracers [7]. More specifically, in a study of Afshar-Oromieh et al. 68Ga-PSMA ligand PET/CT detected 78 lesions characteristic for recurrent PC in 32 patients while 18F-fluoromethylcholine PET/CT detected only 56 lesions in 26 patients resulting in a significant higher detection rate for 68Ga-PSMA ligand PET/CT [7]. The advantage of 68Ga-PSMA ligand PET is especially evident in patients with low PSA levels (PSA below 1 ng/ml). A recent study reported a detection rate of 73 and 58 % in patients with biochemical recurrence after radical prostatectomy in a PSA-range of 0.5–1.0 ng/ml and 0.2–0.5 ng/ml, respectively [17]. This facilitates the use of salvage procedures (e.g. secondary lymphadenectomy, targeted radiation therapy) with a potentially curative intent [20]. Although 68Ga-PSMA ligand PET seems to have an edge over morphological imaging in patients with PC, the evaluation of PSMA-negative PC comprising around 8 % of the examined patients remains a challenge [16].
In nuclear medicine, bone imaging with 99mTc-phosphonates plays an important role in the management of PC patients according to current guidelines providing a fast whole-body overview evaluating the presence of bone metastases. Preliminary results from our department indicate that the detection rate of 68Ga-PSMA ligand PET/CT is clearly superior to traditional bone scan [21]. It has to be mentioned that in clinical practice often faint uptake in various regions of the skeleton, especially in the ribs is found. Caution has to be taken in these cases it remains unclear whether this uptake is really related to bone metastasis or might also constitute false positive findings. Nevertheless, in cases of moderate or intense uptake (see below) usually no doubts exist concerning the presence of bone metastases. Artigas et al. recently reported about an increased 68Ga-PSMA ligand uptake in a patient with Paget’s disease probably related to an overexpression of PSMA in areas with an abnormal bone remodelling and increased vascularity [22]. In addition, healing fractures e.g. ribs or pelvis are known to potentially show faint increased PSMA-ligand uptake [23]. Nevertheless, currently data from multicentric prospective trials creating a high level of evidence are still missing. Therefore and due to the novelty of this technique the implementation in clinical guidelines is still missing. In addition, the reimbursement by health-care providers is broadly varying as 68Ga-PSMA ligand PET is still considered experimental. However, according to the opinion of the authors of this article a summary of the potential and reasonable indications for PSMA-ligand PET/CT is provided in Table 1.
Furthermore, this review aims at helping physicians and physicists to execute, interpret and document hybrid 68Ga-PSMA ligand PET/CT examinations. It focuses on the technical and logistical issues as well as on the specific background for image reading with an emphasis on the PET-part since contrast enhanced computed tomography as the second part of a hybrid 68Ga-PSMA ligand PET/CT examination is an already very standardized and common imaging technique.
Synthesis, application and imaging protocol of 68Ga-PSMA ligand PET/CT
A number of different PSMA-targeted PET tracers have been developed [24–27]. The most widely used PSMA-ligand for PET-imaging in Europe is a 68Ga-labelled PSMA inhibitor Glu-NH-CO-NH-Lys(Ahx)-HBED-CC (68Ga PSMA HBED-CC) followed by the theranostic agent 68Ga-labelled PSMA I&T [26, 27]. Details on the synthesis of 68Ga-labelled PSMA HBED-CC and 68Ga-labelled PSMA I&T have been described previously [27, 28].
The 68Ga-PSMA ligand complex solution is applied to patients via an intravenous bolus with an activity of 1.8–2.2 MBq per kilogram bodyweight. Variation of injected radiotracer activity is caused by the short half-life of 68Ga and variable elution efficiencies obtained during the lifetime of the 68Ge/68Ga radionuclide generator. Low output of the 68Ge/68Ga radionuclide generator could pose a major problem in institutions with high-throughput as it can considerable lower the number of patients that can be examined per 68Ga-PSMA ligand synthesis. To optimize the number of patients it is recommended to either inject patients in parallel in the case several scanners are available at one site. In addition, in our experience it seems feasible that patients with already known diffuse metastatic disease (e.g. restaging after PSMA-radioligand therapy) are injected with only 2/3 of the usual activity. In these advanced cases, the images obtained still have reasonable quality allowing for adequate judgement of therapy response.
Administration of diuretics (furosemide 20 mg) at time of tracer injection is routinely used in our department to enhance diuresis and improve image quality by reducing artifacts due to high activity of 68Ga-PSMA ligand in the bladder and the urinary collection system. Thus, it is recommendable to ask the patient to empty the bladder directly prior to the PET-scan. Besides no published data on the image quality in examinations with and without the application of furosemide we have seen considerable “halo artefacts” around the parts of the urinary collection systems before starting to use diuresis. This seems to be even more relevant when PET/MRI is used [29]. Additionally, all patients receive diluted oral contrast (300 mg Telebrix) and facultative a rectal filling with a negative contrast agent (100–150 mL). The latter allows better anatomical delineation of the rectum and differentiating it from adjacent structures, e.g. seminal vesicles or lymph nodes. In our department (as in most other institutions) PET acquisition is started approximately 60 min after tracer injection. However, a study of Afshar-Oromieh et al. performing 68Ga-PSMA ligand PET/CT 1 h and 3 h p.i concluded that although suspicious PC lesions can be evaluated with an excellent contrast as early as 1 h p.i. late images (e.g. 3 h p.i.) may be help to further clarify unclear lesions due to a better tumour to background ratio [30]. Nevertheless, it would be more complicated to fit this approach in schedule of a busy PET department, as most of the other examination (mainly 18F-FDG) are also started 60 min p.i.
First a diagnostic CT scan is performed from base of the skull-base to midthigh in the portal venous phase 80 s after intravenous injection of contrast agent (1.5 ml per kilogram bodyweight, e.g. Imeron 300, maximum 120 ml) followed by the PET scan. Usually the PET-acquisition starts from the midthigh to the head to exploit the reduced 68Ga-PSMA ligand uptake in the urinary bladder directly after voiding. In addition, this minimizes misalignment especially for the bladder which tends to be filled up during the time of the examination. Technical and logistical details for the applied diagnostic CT-examination within a hybrid PET/CT-examination are described in Boellaard et al. [31].
In our institution, all PET scans are acquired in 3D-mode with an acquisition time of 3–4 min per bed position. Emission data are corrected for randoms, dead time, scatter, and attenuation and are reconstructed iteratively by an ordered-subsets expectation maximization algorithm (four iterations, eight subsets) followed by a postreconstruction smoothing Gaussian filter (5-mm full width at one-half maximum) as applied by the different vendors. Technical details on the reconstruction and post-processing of PET-imaging data using 68Ga-labelled compounds are described in Baum et al. [32].
Display of images
For image analysis all datasets are usually transferred to a dedicated postprocessing workstation (e.g. Syngo MMWP or Syngo Via, Siemens Medical Solutions, Germany; Hermes Hybrid Viewer, Hermes Medical Solutions, Sweden). The software packages for state-of-the-art PET/CT analysis allow for parallel visualisation of PET-, CT-, and PET + CT fusion images in the axial, coronal, and sagittal planes as well as maximum intensity projections in a 3D cine mode. In addition, they offer the possibility of changing the SUV-threshold to e.g. assess the uptake of PSMA-ligands in/or adjacent to organs with high background (e.g. urinary bladder, kidney). Morphological and functional imaging should be displayed at the same time and should be linked at the same table position. In addition, the diagnostic contrast-enhanced CT scan should be evaluated according to the established radiological criteria using a dedicated postprocessing workstation.
At our institution we routinely start reading the diagnostic CT scan, followed by a review of the accompanying 68Ga-PSMA ligand PET images with and without attenuation correction. Both uncorrected and attenuation-corrected images need to be assessed in order to identify artifacts caused by contrast agents, metal implants and/or patient motion. On all slices (of the attenuation corrected data) quantitative information with respect to size and 68Ga-PSMA ligand uptake can be derived. Additionally fused axial PET/CT images may be helpful for exact localization of PET positive findings.
Pattern recognition tips/common variants and artefacts
-
a)
Interpretation Criteria for 68Ga-PSMA ligand PET/CT
-
A physiological variable PSMA-ligand uptake can be observed in the following tissues: lacrimal gland, parotid gland, submandibular gland, liver, spleen, small intestine, colon and kidney as seen in Fig. 1. Within healthy organs, kidneys and the urinary collection system including the urinary bladder as well as salivary glands are showing the highest radiotracer uptake. However, especially in localizations where PC metastases mostly occur-the retroperitoneal fatty tissue, benign lymphatic as well as bone tissue-hardly any uptake is noted [33]. Care should be taken in heavily metastasized patients as here visceral metastases can occur. Due to high background activity in the liver potential liver metastases can be obscured. In addition, in advanced disease especially liver metastases tend to loose PSMA-expression—most likely due to de-differentiation. Therefore, in advanced disease the diagnostic CT scan is the mainstay for detection of liver metastases.
Fig. 1 
Maximum intensity protection (MIP) images of a patient with physiological distribution of 68Ga-PSMA ligand. Accumulation is seen in lacrimal and salivary glands, nasal mucosa, liver, spleen, bowel, kidneys and bladder
-
For 68Ga-PSMA ligand PET interpretation, first all PET positive lesions suspicious for PC are noted. In PET any focal uptake of 68Ga-PSMA ligand higher than the surrounding background and not associated with physiological uptake has to be considered suspicious for malignancy and judged and described below. As 68Ga-PSMA ligands are excreted via the kidneys and are highly accumulated in the urinary bladder, small local recurrences might be missed. Therefore it is especially important to evaluate PET images in axial as well as coronal and sagittal planes and to change the SUV-threshold to judge the PSMA-ligand uptake in soft-tissue structures near the urinary bladder. Examples of PC patients undergoing 68Ga-PSMA ligand PET/CT examination for primary staging and restaging are presented in Figs. 2 and 3.
Fig. 2 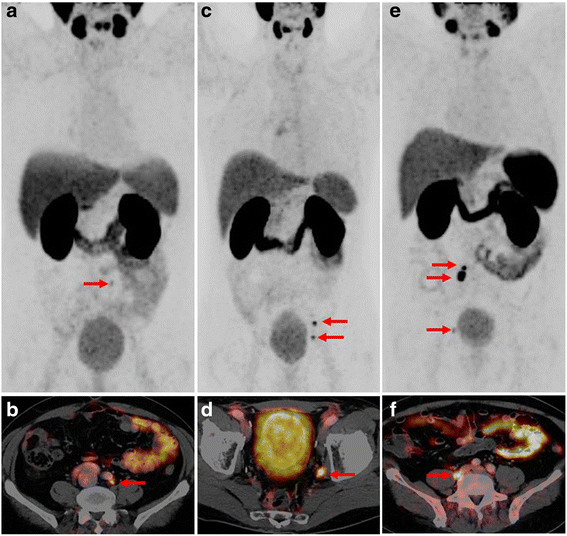
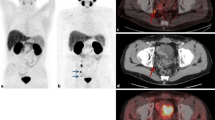
MIP a, c, e and fused 68Ga-PSMA ligand PET/CT b, d, f of a patient presenting with low 68Ga-PSMA ligand uptake in the left common iliac artery (A and B, SUV mean 3.5), a patient presenting with moderate 68Ga-PSMA ligand uptake in the left internal iliac artery (SUV mean 7,8) and in the left external iliac artery (C and D) and a patient presenting with intensive, focal 68Ga-PSMA ligand uptake behind the right common iliac vein twice (E and F, SUV mean 17,9), Note the low uptake adjacent to the urinary bladder on the right side in the MIP images (E)
Fig. 3 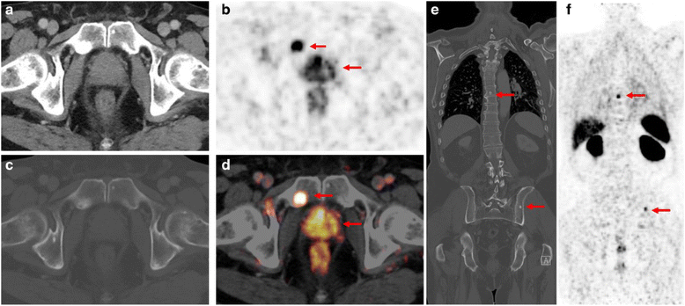
68Ga-PSMA ligand PET/CT in a 78-year old patient with primary PC (Gleason score 7, iPSA 34.3 ng/ml). The patient presented with intense, multifocal uptake in the prostate b, d without correlate on CT images a The CT examination with bone window setting c and e shows osteoblastic bone lesions in the left iliac bone as well as in the thoracic vertebrae with corresponding PSMA-ligand uptake in PET imaging f However, the focal PSMA-ligand uptake in the right symphysis (B, D) shows only a slight hypersclerosis (C) on corresponding CT images that might have been missed without PET. Note the physiological high uptake in the kidneys as well as moderate uptake in the liver and spleen (F)
-
Finally, it has to be noted that not all PC exhibit a significant PSMA overexpression. In a study of Maurer et al. about 8 % of patients with primary PC did not show PSMA overexpression—with currently no specific biological explanation [16]. Therefore, correct and careful interpretation of the diagnostic CT scan as part of the 68Ga-PSMA ligand PET/CT examination is of special importance.
-
-
b)
Pitfalls of 68Ga-PSMA ligand PET
-
As 68Ga-PSMA ligand PET/CT imaging is a relatively new imaging technique it is important to be aware that 68Ga-PSMA ligands are not completely specific for PC to avoid scan misinterpretation. So far, several case reports exist showing increased PSMA uptake in benign lesions such as thyroid adenoma, Paget’s disease, schwannoma, tuberculosis, adrenal adenoma or splenic sarcoidosis [22, 34–36]. Further, it is known that coeliac ganglia show a relevant 68Ga-PSMA uptake. In a study of Krohn et al. at least one ganglion with tracer uptake was found in 76/85 patients (89.4 %) undergoing 68Ga-PSMA ligand PET/CT examination which may mimic lymph node metastases in this area [37]. An example of a 68Ga-PSMA ligand PET/CT examination with focal uptake in the coeliac ganglion is presented in Fig. 4. Interestingly, PSMA expression has also been reported in the tumor neovasculature of some solid tumors (e.g. colon, breast, renal) and in newly formed blood vessels. Apart from PC, other malignant lesions presenting with increased PSMA expression have been reported for glioblastoma, hepatocellular carcinoma, lung cancer, renal cell carcinoma and thyroid cancer [38–42]. For example, differentiation between lung metastases and primary lung cancer which can also occur in elderly patients as secondary malignancy is a common clinical question. A study by Pyka et al. revealed that quantitative (SUV) analysis of 68Ga-PSMA ligand PET was not able to discriminate reliably between pulmonary metastases and primary lung cancer in PC patients as primary lung cancer lesions can also show high PSMA-expression by 68Ga-PSMA ligand PET. [41]. In summary, in unclear 68Ga-PSMA ligand PET positive lesions, morphological correlation, further clarification with other imaging techniques such as MRI, ultrasound or biopsy is mandatory.
Fig. 4 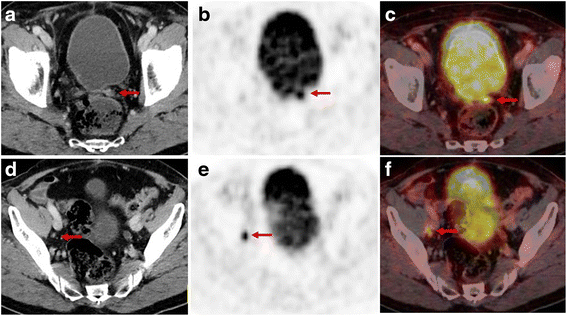
68Ga-PSMA ligand PET/CT examination of a 76-year old patient after radical prostatectomy (Gleason score 8, pT2b, pN1) followed by subsequent external beam radiation. 5 years later the patient presented with a rising PSA-value of 0.54 ng/ml. CT images show a 10 × 8 mm soft tissue formation in the former left prostatic bed a and a morphologically unsuspicious 4 mm lymph node (short axis) d dorsal of the right external iliac vein. Corresponding PET and fused PET/CT images show an intense, focal PSMA-ligand uptake in the former left prostatic bed b, c indicating a local recurrence as well as an intense, focal PSMA-ligand uptake in the small-sized lymph node dorsal of the right external iliac vein e, f indicating a lymph node metastasis
-




Formulating reports
At first, all important clinical data and technical details of the 68Ga-PSMA ligand PET/CT examination should be reported in a standardized way (Table 2). Reporting of imaging findings is usually performed in a structured way on a free text basis. We recommend the following information and details to be included in the section “findings” and “conclusion”.
Findings
Description of the localization, the extent and the intensity of pathological 68Ga-PSMA ligand accumulations related to normal tissue. Hereby, a standardized reporting should be pursued by reporting separately findings within the prostatic fossa, lymph nodes, bones or other visceral organs. 68Ga-PSMA ligand accumulation should be reported as low, moderate or intense by comparison to the background uptake in e.g. the liver parenchyma as seen in Fig. 5. For each suspicious lesion, corresponding SUVmax can be noted using a 3D isocontour VOI. However, as so far no evidence exists that specific SUV-thresholds aid in differentiation between benign and malignant lesions, at our institution quantitative SUVs are not generally reported.

Example of a 68Ga-PSMA ligand PET/CT examination with incidental finding of a moderate, focal PSMA-ligand uptake in a left-sided coeliac ganglion in PET b and fused PET/CT images c. Corresponding CT images a show a teardrop-shaped soft tissue formation between the left adrenal gland and the truncus coeliacus measuring about 9 × 3 mm, typical for a benign coeliac ganglion. Additionally, faint PSMA-ligand uptake in projection on a smaller right-sided coeliac ganglion can be noted
Relevant findings in CT and their relation to pathological 68Ga-PSMA ligand accumulations should be mentioned. However, the CT part of the 68Ga-PSMA ligand PET/CT report must describe all pathological findings (even in the case they are PET negative).
Conclusion
The conclusion should address the findings with respect to the clinical questions asked in the context of the 68Ga-PSMA ligand PET/CT examination. If possible, a definite diagnosis with regard to local tumor involvement, lymph node or bone metastases (and other if present) should be stated. Alternatively, an estimate of the probability of a diagnosis should be given. If relevant, differential diagnoses should be discussed. If appropriate, repeat examinations and/or additional examinations should be recommended to clarify or confirm findings.
However, there is growing evidence that the classical free-text reports of imaging studies have many possible flaws, like inconsistency between different readers, different nomenclature or incompleteness. Further, the narrative individual form leads to reports that do not always address key clinical questions, may contain clinically important errors and may contain ambiguous terms [43–45]. Besides, it is difficult to analyze information extracted from free-text reports.
There are large initiatives for structured reporting for different fields of imaging studies by several international societies [46]. Structured reporting assists in the clear, complete, and consistent communication of results by providing tools for physicians to adopt compliant reporting guidelines (e.g. checklists, clinical decision support). There are further efforts towards a unified reporting nomenclature (e.g. the RadLex initiative in Radiology) and towards information systems that support structured data storage and display report formats.
There have been publications for several tumor types (pancreatic cancer and rectal cancer) which showed improved satisfaction of referring physicians, higher completeness of reports when using specific report templates or checklists [47–49]. This form of reporting involves the presentation of a standard set of reporting items in a standard sequence. In urogenital radiology structured reporting is gaining more importance e.g. in the interpretation of multiparametric MRI of the prostate using the PIRADS classification [50, 51].
Based on these recent initiatives for structured reporting we developed a template for structured reporting of 68Ga-PSMA ligand PET/CT examination presented in Fig. 6. The proposed structured report divides into three categories: T-staging (primary tumor or local recurrence), N-staging (abdominopelvic or cervical/thoracic lymph nodes) and M-staging (bone). We used an online platform that allows creation of decision trees for certain examinations and concomitant report generation of semantic reports by linking text elements to the decision trees (https://www.smart-radiology.com).

Basic template for a decision tree for structured reporting of 68Ga-PSMA ligand PET/CT examinations. Please note that this decision tree only contains the structured elements for local tumor involvement (primary tumor and local recurrence) as well as possible lymph node and bone metastases as the most common findings in PC. Nevertheless all other potential malignant lesions/other pathological findings have to be noted but exceed the scope of this figure
Conclusions
PET imaging for PC using PSMA-ligands has gained high attention during the last years. However, so far, no guidelines exist how to review and report 68Ga-PSMA ligand PET/CT examinations in patients with PC. Therefore, in this review we have summarized our approach performing 68Ga-PSMA ligand PET/CT scans and reviewing the images. We discussed important pitfalls in the evaluation of 68Ga-PSMA ligand PET/CT examinations and outlined important aspects for free-text as well as structured reports in daily clinical routine. In addition, we have outlined potential indications with an emphasis on the estimated clinical benefit.
References
Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108.
Han M, Partin AW, Zahurak M, et al. Biochemical (prostate specific antigen) recurrence probability following radical prostatectomy for clinically localized prostate cancer. J Urol. 2003;169(2):517–23.
Chism DB, Hanlon AL, Horwitz EM, et al. A comparison of the single and double factor high-risk models for risk assignment of prostate cancer treated with 3D conformal radiotherapy. Int J Radiat Oncol Biol Phys. 2004;59(2):380–5.
Freedland SJ, Presti Jr JC, Amling CL, et al. Time trends in biochemical recurrence after radical prostatectomy: results of the SEARCH database. Urology. 2003;61(4):736–41.
Hovels AM, Heesakkers RA, Adang EM, et al. The diagnostic accuracy of CT and MRI in the staging of pelvic lymph nodes in patients with prostate cancer: a meta-analysis. Clin Radiol. 2008;63(4):387–95.
Briganti A, Abdollah F, Nini A, et al. Performance characteristics of computed tomography in detecting lymph node metastases in contemporary patients with prostate cancer treated with extended pelvic lymph node dissection. Eur Urol. 2012;61(6):1132–8.
Afshar-Oromieh A, Zechmann CM, Malcher A, et al. Comparison of PET imaging with a (68)Ga-labelled PSMA ligand and (18)F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging. 2014;41(1):11–20.
Schmid DT, John H, Zweifel R, et al. Fluorocholine PET/CT in patients with prostate cancer: initial experience. Radiology. 2005;235(2):623–8.
Krause BJ, Souvatzoglou M, Tuncel M, et al. The detection rate of [11C]choline-PET/CT depends on the serum PSA-value in patients with biochemical recurrence of prostate cancer. Eur J Nucl Med Mol Imaging. 2008;35(1):18–23.
Castellucci P, Picchio M. 11C-choline PET/CT and PSA kinetics. Eur J Nucl Med Mol Imaging. 2013;40 Suppl 1:S36–40.
Beer AJ, Eiber M, Souvatzoglou M, et al. Radionuclide and hybrid imaging of recurrent prostate cancer. Lancet Oncol. 2011;12(2):181–91.
Schuster DM, Taleghani PA, Nieh PT, et al. Characterization of primary prostate carcinoma by anti-1-amino-2-[(18)F]-fluorocyclobutane-1-carboxylic acid (anti-3-[(18)F] FACBC) uptake. Am J Nucl Med Mol Imaging. 2013;3(1):85–96.
Schuster DM, Savir-Baruch B, Nieh PT, et al. Detection of recurrent prostate carcinoma with anti-1-amino-3-18 F-fluorocyclobutane-1-carboxylic acid PET/CT and 111In-capromab pendetide SPECT/CT. Radiology. 2011;259(3):852–61.
Nanni C, Schiavina R, Brunocilla E, et al. 18 F-fluciclovine PET/CT for the detection of prostate cancer relapse: a comparison to 11C-choline PET/CT. Clin Nucl Med. 2015;40(8):e386–91.
Eiber M, Weirich G, Holzapfel K, et al. Simultaneous Ga-PSMA HBED-CC PET/MRI Improves the Localization of Primary Prostate Cancer. Eur Urol. 2016.
Maurer T, Gschwend JE, Rauscher I, et al. Diagnostic Efficacy of Gallium-PSMA Positron Emission Tomography Compared to Conventional Imaging in Lymph Node Staging of 130 Consecutive Patients with Intermediate to High Risk Prostate Cancer. J Urol. 2016;195(5):1436-43.
Eiber M, Maurer T, Souvatzoglou M, et al. Evaluation of hybrid (6)(8)Ga-PSMA ligand PET/CT in 248 patients with biochemical recurrence after radical prostatectomy. J Nucl Med. 2015;56(5):668–74.
Afshar-Oromieh A, Avtzi E, Giesel FL, et al. The diagnostic value of PET/CT imaging with the (68)Ga-labelled PSMA ligand HBED-CC in the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging. 2015;42(2):197–209.
Roethke MC, Kuru TH, Afshar-Oromieh A, et al. Hybrid positron emission tomography-magnetic resonance imaging with gallium 68 prostate-specific membrane antigen tracer: a next step for imaging of recurrent prostate cancer-preliminary results. Eur Urol. 2013;64(5):862–4.
Maurer T, Weirich G, Schottelius M, et al. Prostate-specific membrane antigen-radioguided surgery for metastatic lymph nodes in prostate cancer. Eur Urol. 2015;68(3):530–4.
M. Eiber TP, S. Okamoto, et al. 68Gallium-HBED-CC-PSMA PET compared to conventional bone scintigraphy for evaluation of bone metastases in prostate cancer patients. European Urology Supplements. March 2016;15(3).
Artigas C, Alexiou J, Garcia C, et al. Paget bone disease demonstrated on (68)Ga-PSMA ligand PET/CT. Eur J Nucl Med Mol Imaging. 2016;43(1):195–6.
Gykiere P, Goethals L, Everaert H. Healing Sacral Fracture Masquerading as Metastatic Bone Disease on a 68Ga-PSMA PET/CT. Clin Nucl Med. 2016 Apr 6 (Epub ahead of print).
Szabo Z, Mena E, Rowe SP, et al. Initial evaluation of [(18)F]DCFPyL for prostate-specific membrane antigen (PSMA)-targeted PET imaging of prostate cancer. Mol Imaging Biol. 2015;17(4):565–74.
Cho SY, Gage KL, Mease RC, et al. Biodistribution, tumor detection, and radiation dosimetry of 18 F-DCFBC, a low-molecular-weight inhibitor of prostate-specific membrane antigen, in patients with metastatic prostate cancer. J Nucl Med. 2012;53(12):1883–91.
Weineisen M, Schottelius M, Simecek J, et al. 68Ga- and 177Lu-labeled PSMA I&T: optimization of a PSMA-targeted theranostic concept and first proof-of-concept human studies. J Nucl Med. 2015;56(8):1169–76.
Eder M, Schafer M, Bauder-Wust U, et al. 68Ga-complex lipophilicity and the targeting property of a urea-based PSMA inhibitor for PET imaging. Bioconjug Chem. 2012;23(4):688–97.
Martin R, Juttler S, Muller M, et al. Cationic eluate pretreatment for automated synthesis of [(6)(8)Ga]CPCR4.2. Nucl Med Biol. 2014;41(1):84–9.
Afshar-Oromieh A, Haberkorn U, Schlemmer HP, et al. Comparison of PET/CT and PET/MRI hybrid systems using a 68Ga-labelled PSMA ligand for the diagnosis of recurrent prostate cancer: initial experience. Eur J Nucl Med Mol Imaging. 2014;41(5):887–97.
Afshar-Oromieh A, Malcher A, Eder M, et al. PET imaging with a [68Ga]gallium-labelled PSMA ligand for the diagnosis of prostate cancer: biodistribution in humans and first evaluation of tumour lesions. Eur J Nucl Med Mol Imaging. 2013;40(4):486–95.
Boellaard R, Delgado-Bolton R, Oyen WJ, et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2.0. Eur J Nucl Med Mol Imaging. 2015;42(2):328–54.
Baum R, Rösch F. Theranostics, Gallium-68, and Other Radionuclides. Recent Results in Cancer Research 194, Springer-Verlag Berlin Heidelberg 2013.
Silver DA, Pellicer I, Fair WR, et al. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin Cancer Res. 1997;3(1):81–5.
Kanthan GL, Drummond J, Schembri GP, et al. Follicular Thyroid Adenoma Showing Avid Uptake on 68Ga PSMA-HBED-CC PET/CT. Clin Nucl Med. 2016;41(4):331-2.
Kobe C, Maintz D, Fischer T, et al. Prostate-specific membrane antigen PET/CT in splenic sarcoidosis. Clin Nucl Med. 2015;40(11):897–8.
Rischpler C, Maurer T, Schwaiger M, et al. Intense PSMA-expression using (68)Ga-PSMA PET/CT in a paravertebral schwannoma mimicking prostate cancer metastasis. Eur J Nucl Med Mol Imaging. 2016;43(1):193–4.
Krohn T, Verburg FA, Pufe T, et al. [(68)Ga]PSMA-HBED uptake mimicking lymph node metastasis in coeliac ganglia: an important pitfall in clinical practice. Eur J Nucl Med Mol Imaging. 2015;42(2):210–4.
Schwenck J, Tabatabai G, Skardelly M, et al. In vivo visualization of prostate-specific membrane antigen in glioblastoma. Eur J Nucl Med Mol Imaging. 2015;42(1):170–1.
Verburg FA, Krohn T, Heinzel A, et al. First evidence of PSMA expression in differentiated thyroid cancer using [(6)(8)Ga]PSMA-HBED-CC PET/CT. Eur J Nucl Med Mol Imaging. 2015;42(10):1622–3.
Rowe SP, Gorin MA, Hammers HJ, et al. Imaging of metastatic clear cell renal cell carcinoma with PSMA-targeted (18)F-DCFPyL PET/CT. Ann Nucl Med. 2015;29(10):877–82.
Pyka T, Weirich G, Einspieler I, et al. 68GaPSMA-HBED PET for differential diagnosis of suspicious lung lesions in patients with prostate cancer. J Nucl Med. 2016;57(3):367-71.
Sasikumar A, Joy A, Nanabala R, et al. (68)Ga-PSMA PET/CT imaging in primary hepatocellular carcinoma. Eur J Nucl Med Mol Imaging. 2016;43(4):795-6.
Langlotz CP. Automatic structuring of radiology reports: harbinger of a second information revolution in radiology. Radiology. 2002;224(1):5–7.
Noumeir R. Benefits of the DICOM structured report. J Digit Imaging. 2006;19(4):295–306.
Bosmans JM, Neri E, Ratib O, et al. Structured reporting: a fusion reactor hungry for fuel. Insights Imaging. 2015;6(1):129–32.
Douglas PS, Hendel RC, Cummings JE, et al. ACCF/ACR/AHA/ASE/ASNC/HRS/NASCI/RSNA/SAIP/SCAI/SCCT/SCMR 2008 health policy statement on structured reporting in cardiovascular imaging. Endorsed by the society of nuclear medicine [added]. Circulation. 2009;119(1):187–200.
Brook OR, Brook A, Vollmer CM, et al. Structured reporting of multiphasic CT for pancreatic cancer: potential effect on staging and surgical planning. Radiology. 2015;274(2):464–72.
Tarulli E, Thipphavong S, Jhaveri K. A structured approach to reporting rectal cancer with magnetic resonance imaging. Abdom Imaging. 2015;40(8):3002–11.
Patel BN, Gupta RT, Zani S, et al. How the radiologist can add value in the evaluation of the pre- and post-surgical pancreas. Abdom Imaging. 2015;40(8):2932–44.
Weinreb JC, Barentsz JO, Choyke PL, et al. PI-RADS prostate imaging-reporting and data system: 2015, version 2. Eur Urol. 2016;69(1):16–40.
Hamoen EH, de Rooij M, Witjes JA, et al. Use of the prostate imaging reporting and data system (PI-RADS) for prostate cancer detection with multiparametric magnetic resonance imaging: a diagnostic meta-analysis. Eur Urol. 2015;67(6):1112–21.
ᅟ
ᅟ
Authors’ contributions
IR, TM, WPF, WHS, MS, ME: made substantial contributions to conception and design of this review, evaluation, interpretation and summarizing currently available literature . IR, TM, WPF, WHS, MS, ME: were involved in drafting the manuscript and revising it critically. IR, TM, WPF, WHS, MS, ME: read and gave final approval of the version to be published. IR, TM, WPF, WHS, MS, ME: agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Competing interest
All authors declare that they have no competing interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Rauscher, I., Maurer, T., Fendler, W.P. et al. 68Ga-PSMA ligand PET/CT in patients with prostate cancer: How we review and report. Cancer Imaging 16, 14 (2016). https://doi.org/10.1186/s40644-016-0072-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40644-016-0072-6