
Abstract
Purpose
Foot progression angle is a key factor for biomechanical knee load, which is associated with noncontact anterior cruciate ligament (ACL) injury during sports-specific tasks. The purpose of the present study was to assess the biomechanics of trunk, pelvis, and lower extremities during a cutting maneuver under different foot progression angles.
Methods
Nineteen male collegiate athletes (ages 18–24) participated in the present study. Cutting motion was analyzed using eight infrared cameras (250 Hz), two force plates (1250 Hz), and 44 reflective markers. Subjects performed 45-degree side cutting maneuvers under three foot progression angles, including 20 degrees (toe-out: TO), 0 degrees (neutral: TN), and − 20 degrees (toe-in: TI). Peak values of each biomechanical parameters in trunk, pelvis, hip, and knee within a first 40% stance phase and each parameter at the timing of the peak vertical ground reaction force were assessed. A statistical analysis was performed to compare data among the three-foot progression angles using the Friedman test.
Results
Peak angles of knee abduction, tibial internal rotation, hip internal rotation, and hip adduction were significantly greater for TI position than for TO position (p < 0.01). Peak moments of knee abduction and tibial internal rotation under TI position were also significantly larger than TO position (p < 0.01). Moreover, greater peak pelvis-trunk rotation was found for TI position than for TN and TO positions (p < 0.01).
Conclusion
From the present study, TI position could lead to an increased risk of ACL injury during a pre-planned cut maneuver, compared to TO position.
Similar content being viewed by others


Background
Noncontact anterior cruciate ligament (ACL) injury in athletes is commonly seen during deceleration, side-cutting, or landing tasks in various sports activities [15, 22, 25]. Knee valgus is an important biomechanical consideration for injury mechanism, based on previous three-dimensional biomechanical analysis [3, 11, 20, 22, 26, 28, 29]. For instance, a video imaging analysis reported that athletes exhibited knee valgus, extension, and an external rotation position at the time of several injury situations [5, 15]. In addition, an increased knee abduction angle during a drop landing task was characterized as a risk factor of noncontact ACL injury [28]. A prospective study assessed the kinetic parameters of a jump-landing task at baseline, and athletes who had sustained an ACL injury exhibited a 2.5-times knee valgus moment, compared with those who had an intact ACL [11]. ACL injured athletes showed greater knee internal rotation angle during cutting motion at baseline than control [39]. Prevention programs for ACL injury have focused on reducing knee valgus loading during sporting activities [6, 7, 12, 21]. The training program regarding modification of trunk motion and foot landing position was effective for the reduction of knee valgus loading during cutting motion [6]. Therefore, trunk, hip, and foot motion during sports movement are important as well as knee joint motion for ACL injury prevention [2, 9, 14, 24, 34, 35].
A cutting maneuver is a high-demand sports activity that has been recognized as a risky movement associated with noncontact ACL injuries [29]. According to previous reports, the cutting maneuvers produces an increased mechanical load at the knee joint, compared with hopping and drop landing [27, 36]. Foot progression angle at initial contact is also known to affect knee biomechanics during high demand activities. In term of cutting maneuver, Sigward et al. found that athletes with large knee valgus moment indicated increased internally rotation foot angle compared to those with normal knee valgus moment [33]. Jones et al. found that athletes with a larger knee valgus moment presented a more internally rotated foot progression angle than those with a smaller mean knee valgus moment [16]. Therefore, the foot progression angle is a key factor for the knee joint load during a cutting movements, and toe-in landing seems to be related to an increased knee valgus loading which is known as an ACL injury risk factor [16, 33]. Clinically, the kinematic chain mechanism of whole-body segments is extremely important to consider ACL injury prevention programs. However, few studies have been done to compare biomechanical differences, including trunk, pelvis, and lower extremities, in cutting maneuvers among different foot progression angles. Specifically, no previous study compared the biomechanical parameters between toe-in and toe-out positions during a cutting movement.
The purpose of the present study was to investigate and clarify whether difference of foot progression angles would affect the biomechanics of the trunk, pelvis, and lower extremities during a cutting maneuver. It was hypothesized that foot progression angles would change movements of trunk and pelvis as well as biomechanics of the hip and knee joints, and toe-in position could indicate the highest risk of noncontact ACL injury.
Methods
Study type
Cross-sectional study was conducted to investigate whether foot progression angle would affect biomechanical parameters of knee, hip, pelvis, and trunk during a cutting movement.
Subjects
A total of 16 subjects were needed to detect a significant difference of 3.5 degrees (standard deviation [SD] 6) for the knee abduction angle (β = 0.80, α = 0.05) based on power analysis of previous research examining the effects of toe angle [30]. In the present study, nineteen male collegiate athletes with a mean age of 20 ± 1.5 years, a mean height of 175 ± 5.4 cm, and a mean weight of 67 ± 6.5 kg were enrolled. Age of the subjects ranged from 18 to 24 years. The mean Tegner activity level scale was 7.0 ± 0.2 level, and the subjects in the current investigation consisted of twelve soccer players, five ice hockey players, one handball player, and one Judo player. The subjects were recruited in university sports club, and the inclusion criteria was more than Tegner activity score level 6. None of the subjects had a severe musculoskeletal injury in the trunk or lower extremities requiring surgery. All the subjects signed a written informed consent approved by university institutional review board.
Instrumentation
Three-dimensional motion analysis was performed using two ground reaction force (GRF) plates (sampling frequency, 1250 Hz; AM6110, Bertec, Columbus, OH, USA), eight infrared cameras (250 frames/s; Miqus, Qualisys, Sweden) and 44 retro-reflective markers. The GRF data was synchronized with the motion capture data. To define the local coordinate system for each segment, anatomical landmark markers were placed on bilateral acromion processes, xiphoid process, suprasternal notch, 7th cervical vertebra, 10th thoracic vertebra, bilateral anterior/posterior superior iliac spine, bilateral greater trochanters, bilateral lateral/medial epicondyles, bilateral lateral/medial malleoli, bilateral posterior heels, bilateral navicular bone, and bilateral heads of the first/fifth metatarsals. Four tracking markers were placed in squares on the anterior aspect of the thigh and shank.
Procedures
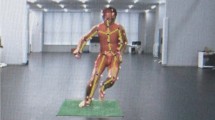
The participants were asked to sprint as fast as they can and then performed a 45-degree side cutting task to the side opposite to the tested limb at a self-selected speed with bare feet. In the present protocol, the cutting movement was done under three different foot progression angles, including 0 degrees (toe-neutral [TN]),− 20 degrees (toe-in [TI]), and 20 degrees (toe-out [TO]). The subjects were asked to aim their toe according to the signs attached to the force plate (Fig. 1). After participants performed the jogging and 45-degree side cutting task several times as a warm-up, two successful motion data sets were obtained for each pattern. The nondominant leg (1 right, 18 left) was chosen for the measurement. The dominant leg was defined as the leg with which each athlete preferred to kick a ball [1, 10].

Participants perform cutting maneuver on nondominant leg under toe-in, neutral, and toe-out landing. The peak values within the 40% stance phase equivalent to the loading acceptance and value at the timing of the peak Fz were compared among the neutral, toe-out, and toe-in positions
Data analysis
The three-dimensional kinematics of trunk, pelvis, hip and knee, and kinetics of hip and knee were calculated using Visual 3D (C-Motion Company, Rockville, MD). A low-pass filter was used to smooth the marker and GRF data at a cutoff frequency of 12 Hz, based on previous study [21]. Each parameter was normalized from zero to 100 between the initial contact and the toe off. External joint moments were calculated using inverse dynamics. The laboratory coordinate system was set to the right of progression direction as X-axis, progression direction as Y-axis, and vertical direction as Z-axis. The angle of the foot coordinate system with respect to the Z-axis of the laboratory coordinate system was defined as the toe angle (inward rotation: negative, outward rotation: positive). A positive value of pelvis lateral tilt was defined as an inclination toward the dominant leg side in the coronal plane. A positive value of trunk lateral bending was defined as an inclination toward the non-dominant leg side in the coronal plane. Pelvic and trunk rotations were evaluated as the angle relative to the jogging direction, and positive values were defined as rotation toward the nondominant leg side (measured side). The pelvis-trunk angle was calculated by the trunk motion relative to the pelvis. The peak values of the angle and moment within 40% after initial contact and at the timing of the peak vertical ground reaction force (vGRF) during the stance phase were analyzed as the weight acceptance phase, which is known to be a risky timing for noncontact ACL injury [4].
Statistical analysis
After Shapiro–Wilk test was performed to confirm normality assumption, the Friedman test was used to compare the differences among TI, TN and TO positions during a cutting movement using SPSS Statistics for Windows, Version 23.0 (IBM Corp., New York, USA). The average value of two successful trials for each foot progression angle was used in the statistical analysis. P values of < 0.05 were regarded as indicating significant differences. As a post-hoc test, the Wilcoxon signed-rank test was corrected using the Bonferroni method to compare the differences between foot progression angle patterns. Effect size was the difference of kinematics and kinetics between foot progression angle patterns, obtained from Wilcoxon signed-rank test.
Results
The toe angles at initial contact were − 12.6 (4.7) degrees, 2.3 (5.6) degrees and 19.5 (8.1) degrees in the TI, TN and TO positions, respectively. Significant differences were found among the three-foot progression angles (p < 0.001). The peak value of each parameter during the 40% stance phase is shown in Table 1. Peak knee abduction, internal rotation, hip adduction, internal rotation, and pelvis-trunk rotation angle were significantly greater for TI position than for TO position (p < 0.01). Peak pelvis-trunk flexion angle was smaller for TI position than TO position (p = 0.016). Peak knee abduction and internal rotation moment under TI position was larger than TO position (p < 0.01). Each biomechanical parameter at the timing of the peak Fz is shown in Table 2. TI position resulted in a significantly greater knee abduction, internal rotation, hip internal, rotation pelvis-trunk rotation angle than TO position (p < 0.01).
The three-dimensional kinematic waveforms of the knee joints and trunk-pelvis during the stance phase are shown in Figs. 2 and 3, and kinetic waveform of knee joint during the stance phase is shown in Fig. 4.

Waveforms showing the average knee flexion angle (a), knee abduction angle (b), and knee internal rotation angle (c) during the stance phase of the cutting maneuver

Waveforms showing the average pelvis-trunk flexion angle (a), pelvis-trunk lateral bending angle (b), and pelvis-trunk rotation angle (c) during the stance phase of the cutting maneuver

Waveforms showing the average knee flexion moment (a), knee abduction moment (b), and knee internal rotation moment (c) during the stance phase of the cutting maneuver
Discussion
The results of the current investigation supported the hypothesis that the foot progression angle would change the biomechanics of the trunk and pelvis, as well as the lower extremities. The main finding of the present study was that larger angles and moments of knee valgus and tibial internal rotation were observed for TI position, with biomechanical changes in the hip joint, trunk, and pelvis. Specifically, the kinematic chain mechanism including the knee, hip, pelvis, and trunk was affected by three different foot progression angles during the weight acceptance phase. The present study suggested that larger trunk torsion was related to larger knee abduction and tibial internal rotation with hip adduction and internal rotation under an internally rotated foot progression angle during a cutting movement, which was considered as risky movement of noncontact ACL injury [17, 18, 23, 31]. To our knowledge, this is the first study to assess differences in the cutting maneuver according to different foot progression angles.
Previous studies have investigated the relationship between the foot rotation angle and knee valgus loading during sports-specific tasks [13, 16, 21, 30, 33, 37, 38]. Sigward et al. found that the athletes with a high knee valgus moment produced a more internally rotated foot progression angle, compared with those with a normal knee valgus moment, during a cutting maneuver [33]. However, they showed no difference in the knee abduction angle between the subjects with and without high knee valgus moment. Unlike previous protocol, the foot progression angle was set at TI, TN, and TO with a difference 20 degree each in the current study, and the large difference between TI, TN, and TO might affect knee abduction motion during a cutting maneuver. In addition, preplanned foot progression angle in a jump-landing task was associated with knee valgus loading, and TI landing led to a larger knee valgus angle and moment than TO landing [13, 30]. These findings were consistent with the present study, since TI direction resulted in a larger knee abduction angle and moment than TN and TO directions in both parameters. The current results showed that TI remained in a knee abduction position during the 40% stance phase, while a knee adduction movement was observed during the early weight acceptance phase (0%-20%) in the TN and TO positions (Fig. 2). Knee abduction movement was associated with knee valgus moment during a cutting movement, therefore, the lack of knee adduction movement may contribute to the increase in the knee valgus moment during the weight acceptance phase (Fig. 4) [16, 21].
On the other hand, Kristianslund et al. indicated that the foot progression angle was not associated with the knee abduction moment during handball offensive cut [21]. Contrary to the current study, the previous protocol involved the subjects conducting a cutting maneuver in front of a virtual defender while holding a ball, which resulted in greater hip external rotation [21]. Presumably, differences in the trunk or hip joint movement patterns may affect the knee abduction moment. According to a previous study, the hip internal rotation angle during a cutting motion is a key predictor of the knee valgus moment [24, 32, 33]. In addition, hip adduction angle was associated with knee valgus moment [21]. In current results, greater peak hip adduction and internal rotation angle were shown in TI position than in TO position. Therefore, hip internal rotation and adduction with an internally rotated foot is a kinematic chain mechanism for knee abduction, and neuromuscular control training at the hip joint may reduce the knee valgus loading, which is considered as a risk of ACL injury.
An increased trunk torsion relative to the pelvis occurred for the TI position as a result of the compensation movements associated with the different foot progression angles. Simulated cutting movement with greater trunk rotation increased the knee internal rotation moment [7]. In addition, using a specimen model in a simulated jump-landing, the coupling moment of knee abduction and internal rotation resulted in a greater ACL strain, compared with that observed in individuals [17, 18, 23, 31]. Knee abduction and the internal rotation moment in both parameters increased for TI position than for TO position in the present study. Therefore, a cutting motion under TI direction was regarded as the ACL injury risk position, compared with TN and TO directions. The video analysis assessed the biomechanics at the ACL injury scenes of football games and showed that trunk torsion was increased, but the foot position was externally rotated [5]. Whereas inward foot rotation motion was observed in the injury situations of handball and basketball games [19]. Therefore, the results of the TI position more simulated injury situations with preplanned cut in handball and basketball.
The present study found that TI position led to greater knee abduction, hip internal rotation, and smaller trunk flexion as compared with TO position during cutting motion. The cutting movement assessment score (CMAS) shows that the pattern in this study increases the risk of ACL injury [8]. Therefore, the instruction to avoid TI position during cutting maneuver in the clinical situation by therapists and trainers is effective for ACL injury prevention.
Several limitations of the present study should be mentioned. First, all the subjects were male collegiate athletes. Generally, female athletes have a high noncontact ACL injury risk, compared with male athletes. Results obtained from female athletes may be different from the present results. Second, a cutting maneuver was assessed in different sport players. Thus, the influence of sports specificity on the present results is unknown. Third, balance and coordination abilities of athletes were not assessed prior to perform motion analysis in the current investigation. These abilities may affect kinematic and kinetic parameters during a cutting maneuver. Forth, preplanned cut motions under different foot progression angles were analyzed in the present study. The cutting motion was a simulation based on the limited movement freedom and thus may differ slightly from actual movement in games. Lastly, the actual TI angle was less than the preplanned angle. A 20-degree TI landing might be too large for athletes to perform during a cutting maneuver. However, the results of the current study provide valuable information when considering the influence of the foot progression angle on the kinematic chain that occurs during the cutting maneuver.
Conclusion
The kinematic chain mechanism was affected including the knee, hip, pelvis, and trunk by three different foot progression angles during a cutting movement. Significantly larger angles and moments of knee abduction and tibial internal rotation with biomechanical changes were observed for TI position, compared to TN and TO positions. Therefore, athletes should be aware of their foot progression angle during cutting movements to avoid ACL injury.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- TO:
-
Toe-out
- TN:
-
Neutral
- TI:
-
Toe-in
- vGRF:
-
Vertical ground reaction force
- GRF:
-
Ground reaction force
References
Brophy R, Silvers HJ, Gonzales T, Mandelbaum BR (2010) Gender influences: the role of leg dominance in ACL injury among soccer players. Br J Sports Med 44:694–697
Chijimatsu M, Ishida T, Yamanaka M, Taniguchi S, Ueno R, Ikuta R et al (2020) Landing instructions focused on pelvic and trunk lateral tilt decrease the knee abduction moment during a single-leg drop vertical jump. Phys Ther Sport 46:226–233
Cronström A, Creaby MW, Ageberg E (2020) Do knee abduction kinematics and kinetics predict future anterior cruciate ligament injury risk? A systematic review and meta-analysis of prospective studies. BMC Musculoskelet Disord 21:563
David S, Komnik I, Peters M, Funken J, Potthast W (2017) Identification and risk estimation of movement strategies during cutting maneuvers. J Sci Med Sport 20:1075–1080
Della Villa F, Buckthorpe M, Grassi A, Nabiuzzi A, Tosarelli F, Zaffagnini S et al (2020) Systematic video analysis of ACL injuries in professional male football (soccer): injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br J Sports Med 54:1423–1432
Dempsey AR, Lloyd DG, Elliott BC, Steele JR, Munro BJ (2009) Changing sidestep cutting technique reduces knee valgus loading. Am J Sports Med 37:2194–2200
Dempsey AR, Lloyd DG, Elliott BC, Steele JR, Munro BJ, Russo KA (2007) The effect of technique change on knee loads during sidestep cutting. Med Sci Sports Exerc 39:1765–1773
Dos’Santos T, McBurnie A, Donelon T, Thomas C, Comfort P, Jones PA (2019) A qualitative screening tool to identify athletes with “high-risk” movement mechanics during cutting: The cutting movement assessment score (CMAS). Phys Ther Sport 38:152–161
Frank B, Bell DR, Norcross MF, Blackburn JT, Goerger BM, Padua DA (2013) Trunk and hip biomechanics influence anterior cruciate loading mechanisms in physically active participants. Am J Sports Med 41:2676–2683
Hägglund M, Waldén M (2016) Risk factors for acute knee injury in female youth football. Knee Surg Sports Traumatol Arthrosc 24:737–746
Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG et al (2005) Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med 33:492–501
Imwalle LE, Myer GD, Ford KR, Hewett TE (2009) Relationship between hip and knee kinematics in athletic women during cutting maneuvers: a possible link to noncontact anterior cruciate ligament injury and prevention. J Strength Cond Res 23:2223–2230
Ishida T, Yamanaka M, Takeda N, Homan K, Koshino Y, Kobayashi T et al (2015) The effect of changing toe direction on knee kinematics during drop vertical jump: a possible risk factor for anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 23:1004–1009
Jamison ST, Pan X, Chaudhari AM (2012) Knee moments during run-to-cut maneuvers are associated with lateral trunk positioning. J Biomech 45:1881–1885
Johnston JT, Mandelbaum BR, Schub D, Rodeo SA, Matava MJ, Silvers-Granelli HJ et al (2018) Video Analysis of Anterior Cruciate Ligament Tears in Professional American Football Athletes. Am J Sports Med 46:862–868
Jones PA, Herrington LC, Graham-Smith P (2015) Technique determinants of knee joint loads during cutting in female soccer players. Hum Mov Sci 42:203–211
Kiapour AM, Demetropoulos CK, Kiapour A, Quatman CE, Wordeman SC, Goel VK et al (2016) Strain Response of the Anterior Cruciate Ligament to Uniplanar and Multiplanar Loads During Simulated Landings: Implications for Injury Mechanism. Am J Sports Med 44:2087–2096
Kiapour AM, Kiapour A, Goel VK, Quatman CE, Wordeman SC, Hewett TE et al (2015) Uni-directional coupling between tibiofemoral frontal and axial plane rotation supports valgus collapse mechanism of ACL injury. J Biomech 48:1745–1751
Koga H, Nakamae A, Shima Y, Bahr R, Krosshaug T (2018) Hip and Ankle Kinematics in Noncontact Anterior Cruciate Ligament Injury Situations: Video Analysis Using Model-Based Image Matching. Am J Sports Med 46:333–340
Koga H, Nakamae A, Shima Y, Iwasa J, Myklebust G, Engebretsen L et al (2010) Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med 38:2218–2225
Kristianslund E, Faul O, Bahr R, Myklebust G, Krosshaug T (2014) Sidestep cutting technique and knee abduction loading: implications for ACL prevention exercises. Br J Sports Med 48:779–783
Krosshaug T, Nakamae A, Boden BP, Engebretsen L, Smith G, Slauterbeck JR et al (2007) Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med 35:359–367
Markolf KL, Burchfield DM, Shapiro MM, Shepard MF, Finerman GA, Slauterbeck JL (1995) Combined knee loading states that generate high anterior cruciate ligament forces. J Orthop Res 13:930–935
McLean SG, Huang X, van den Bogert AJ (2005) Association between lower extremity posture at contact and peak knee valgus moment during sidestepping: implications for ACL injury. Clin Biomech (Bristol, Avon) 20:863–870
Montgomery C, Blackburn J, Withers D, Tierney G, Moran C, Simms C (2018) Mechanisms of ACL injury in professional rugby union: a systematic video analysis of 36 cases. Br J Sports Med 52:994–1001
Myer GD, Ford KR, Khoury J, Succop P, Hewett TE (2011) Biomechanics laboratory-based prediction algorithm to identify female athletes with high knee loads that increase risk of ACL injury. Br J Sports Med 45:245–252
Nedergaard NJ, Dalbø S, Petersen SV, Zebis MK, Bencke J (2020) Biomechanical and neuromuscular comparison of single- and multi-planar jump tests and a side-cutting maneuver: Implications for ACL injury risk assessment. Knee 27:324–333
Numata H, Nakase J, Kitaoka K, Shima Y, Oshima T, Takata Y et al (2018) Two-dimensional motion analysis of dynamic knee valgus identifies female high school athletes at risk of non-contact anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 26:442–447
Olsen OE, Myklebust G, Engebretsen L, Bahr R (2004) Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med 32:1002–1012
Sakurai A, Harato K, Morishige Y, Kobayashi S, Niki Y, Nagura T (2019) Effects of Toe Direction on Biomechanics of Trunk, Pelvis, and Lower-Extremity During Single-Leg Drop Landing. J Sport Rehabil. 29(8):1069–74. https://doi.org/10.1123/jsr.2019-00501-6
Shin CS, Chaudhari AM, Andriacchi TP (2011) Valgus plus internal rotation moments increase anterior cruciate ligament strain more than either alone. Med Sci Sports Exerc 43:1484–1491
Sigward SM, Cesar GM, Havens KL (2015) Predictors of Frontal Plane Knee Moments During Side-Step Cutting to 45 and 110 Degrees in Men and Women: Implications for Anterior Cruciate Ligament Injury. Clin J Sport Med 25:529–534
Sigward SM, Powers CM (2007) Loading characteristics of females exhibiting excessive valgus moments during cutting. Clin Biomech (Bristol, Avon) 22:827–833
Sugimoto D, Alentorn-Geli E, Mendiguchía J, Samuelsson K, Karlsson J, Myer GD (2015) Biomechanical and neuromuscular characteristics of male athletes: implications for the development of anterior cruciate ligament injury prevention programs. Sports Med 45:809–822
Tait DB, Newman P, Ball NB, Spratford W (2021) What did the ankle say to the knee? Estimating knee dynamics during landing - A systematic review and meta-analysis. J Sci Med Sport;https://doi.org/10.1016/j.jsams.2021.08.007
Tanikawa H, Matsumoto H, Komiyama I, Kiriyama Y, Toyama Y, Nagura T (2013) Comparison of knee mechanics among risky athletic motions for noncontact anterior cruciate ligament injury. J Appl Biomech 29:749–755
Teng PSP, Kong PW, Leong KF (2017) Effects of foot rotation positions on knee valgus during single-leg drop landing: Implications for ACL injury risk reduction. Knee 24:547–554
Tran AA, Gatewood C, Harris AH, Thompson JA, Dragoo JL (2016) The effect of foot landing position on biomechanical risk factors associated with anterior cruciate ligament injury. J Exp Orthop 3:13
Zebis MK, Aagaard P, Andersen LL, Hölmich P, Clausen MB, Brandt M, et al. (2021) First-time anterior cruciate ligament injury in adolescent female elite athletes: a prospective cohort study to identify modifiable risk factors. Knee Surg Sports Traumatol Arthrosc;https://doi.org/10.1007/s00167-021-06595-8
Acknowledgements
Not applicable.
Funding
This study was supported by Keio University Doctoral student Grant-in-Aid Program.
Author information
Authors and Affiliations
Contributions
KN designed the study. KN and SH acquired the motion data. KN, KH, and TH interpreted the processed data regarding joint angle and moment. KN and KH drafted manuscript preparation. TN and TO coordinated and managed the data collection. All authors contributed to reviewing and editing the manuscript. All authors read and agreed to the manuscript of the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study was approved by the institutional review board of Keio university (#20190116).
Consent for publication
We obtained consent for publication from participants in the present study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nishizawa, K., Hashimoto, T., Hakukawa, S. et al. Effects of foot progression angle on kinematics and kinetics of a cutting movement. J EXP ORTOP 9, 11 (2022). https://doi.org/10.1186/s40634-022-00447-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40634-022-00447-1