
Abstract
Background
In Tsarang (at 3560 m), which is located in Mustang, 62.7% of the residents answered that they had a subjective medical history of arthritis, and 41.1% of the residents answered that their families had a subjective medical history of arthritis on a survey conducted in 2017. The expression of hypoxia-inducible factor (HIF) and its effects are deeply involved in hypoxic adaptation in Tibetan highlanders. At the same time, HIF is also related to the onset of rheumatoid arthritis. Therefore, the adaptive mechanism acquired by Tibetan highlanders may promote the development of rheumatoid arthritis. The prevalence of rheumatoid arthritis is estimated to be approximately 0.5–1.0% worldwide. The objective of this study was to estimate the prevalence of rheumatoid arthritis in Tsarang residents using existing diagnostic criteria and to explore its risk factors.
Methods
An epidemiological survey was conducted in Tsarang in 2019. Data obtained from anthropometry and questionnaires were statistically analyzed. Biochemical measurements using blood samples were also performed, and the results were used to assess arthritis status. Residents’ joint status was scored, and arthritis was assessed based on the clinical disease activity index and ACR/EULAR 2010 criteria.
Results
Twenty-seven males and 50 females participated in this survey. In Tsarang, ACR/EULAR 2010 classified 4.3% of males and 7.1% of females as having rheumatoid arthritis, indicating a very high estimated prevalence. We also performed a multivariate analysis to explore its risk factors, and two factors, older age (standardized parameter estimate = 4.84E−01, 95% CI = [9.19E−02, 8.76E−01], p = 0.0170) and a history of living in urban areas (standardized parameter estimate = − 5.49E−01, 95% CI = [− 9.21E−01, 1.77E−01], p = 0.0050), significantly contributed to the higher ACR/EULAR 2010 score in females. In addition, three factors, having no spouse (standardized parameter estimate = 3.17E−01, 95% CI = [5.74E−02, 5.77E−01], p = 0.0179), having a smoking habit (standardized parameter estimate = 2.88E−01, 95% CI = [1.71E−02, 5.59E−01], p = 0.0377), and a history of living in urban areas (standardized parameter estimate = − 3.69E−01, 95% CI = [− 6.83E−01, − 5.60E−02], p = 0.0219), resulted in significantly higher clinical disease activity index scores in females. Furthermore, smoking habits were found to significantly increase blood hyaluronic acid in both males (standardized parameter estimate = 6.03E−01, 95% CI = [3.06E−01, 9.01E−01], p = 0.0020) and females (standardized parameter estimate = 4.87E−01, 95% CI = [5.63E−02, 9.18E−01], p = 0.0291).
Conclusions
In this study, we evaluated the symptoms of arthritis and estimated the prevalence of rheumatoid arthritis using classification criteria for Tibetan highlanders who have adapted to the hypoxic environment and fostered their own culture. The high prevalence of rheumatoid arthritis among Tsarang residents suggests that the hypoxic adaptation mechanism involving HIF in Tibetan highlanders may promote the onset or exacerbation of rheumatoid arthritis. The high prevalence of rheumatoid arthritis among Tibetan highlanders may be related not only to the environmental factors analyzed in this study but also to hypoxic adaptation genes. Further investigation is needed to clarify the genetic factors involved.
Similar content being viewed by others
Background
A medical history of arthritis among Tsarang residents
Archeological studies suggest that humans entered the Tibetan Plateau 50,000 to 25,000 years ago [1, 2]. In addition, especially in Mustang, it is thought that human beings began to live there approximately 4500 years ago [3]. Mustang, which was the focus area for this research, is a mountainous area in the Annapurna Conservation Area, located approximately 206.1 km in a straight line from the capital Kathmandu [4]. Additionally, this district is a region where the Mustang kingdom was founded in 1440. The Tibetan highlanders currently live there. The Kingdom of Mustang survived as an autonomous kingdom until 2008 and is a rare area that has long restricted exchanges with foreign countries [5,6,7]. Therefore, people who live in Mustang are highly likely to inherit genes increasing adaptation to the hypoxic environment that were acquired by ancient Tibetan highlanders as a population.
While the hypoxic adaptation mechanism of these Tibetan highlanders enables environmental adaptation, it makes them vulnerable to aging and lifestyle changes, and a possibility of promoting the onset of diabetes has been reported [8]. An epidemiological study conducted in Tsarang in 2017 also revealed an increase in hemoglobin concentration with age in only females [9]. In Tsarang village (altitude 3560 m) in Mustang, residents’ health conditions have not been clarified because health surveys by the government have not been thoroughly conducted. In 2017, an epidemiological survey of Tibetan highlanders living in Tsarang was conducted to investigate health status, especially regarding noncommunicable diseases and their risk factors. As a result, in terms of questionnaires related to arthritis, 62.7% of the residents answered that they had a subjective medical history of arthritis, and 41.1% of the residents answered that their families had a subjective medical history of arthritis [10]. From this survey, it became clear that arthritis has become a health problem among the residents of Mustang.
Prevalence of rheumatoid arthritis and its pathology associated with hypoxia
The prevalence of rheumatoid arthritis is estimated to be approximately 0.5–1.0% worldwide [11,12,13]. On the other hand, in Southern Europe, including Greece, the prevalence rate is as low as 0.18–0.34% [14,15,16]. Conversely, the prevalence rate is as high as 5.3% [17] in native American Pima Indians and 6.8% in Chippewa Indians [18]. To date, it has been reported that genetic differences may affect the prevalence of rheumatoid arthritis [19], but differences in the classification criteria used in each survey also heavily contribute to differences in prevalence.
Rheumatoid arthritis is an autoimmune disease, and autoantibodies such as rheumatoid factor and anti-cyclic citrullinated peptide (CCP) antibody are involved in the onset of the disease. In the early stage, synovitis, bilateral joint swelling, and pain occur in the small joints. As the condition progresses, the joints become deformed, the inflamed areas spread to the wrists, knees, elbows, shoulders, etc., and this joint destruction has a great impact on the patient’s daily life [20, 21].
Relationship between hypoxic adaptation and HIF among Tibetan highlanders
The mutant endothelial per-ARNT-sim domain protein 1 (EPAS1) gene inherited from Denisovans is thought to enable Tibetan highlanders to adapt to hypoxic environments [22]. When people living in lowlands go to a hypoxic environment, HIF2 expressed by the EPAS1 gene is less likely to be degraded, and a hypoxic response is initiated. As a result, the body tries to adapt to hypoxia by increasing the amount of erythropoietin secretion and the concentration of hemoglobin in the blood [23]. On the other hand, many Tibetan high highlanders have mutations specific to the EPAS1 gene, and having this mutation increases the ability to increase blood NO levels and dilate blood vessels. It is also known that even in a hypoxic environment, the hemoglobin concentration is maintained at the same level as that of people in the lowlands, and the increase in hemoglobin concentration is suppressed. In other words, it is thought that the hypoxic adaptation of Tibetan highlanders improves oxygen circulation by enhancing the vasodilatory effect instead of suppressing the increase in blood hemoglobin concentration [24]. EPAS1 is the gene that expresses HIF-2α, which is also deeply involved in the pathophysiology of rheumatoid arthritis [25]. We suspect that the hypoxic adaptation mechanism acquired by Tibetan highlanders not only enables environmental adaptation but is also involved in promoting the onset of rheumatoid arthritis.
Hypothetical risk factors and objectives of this study
It has been reported that age, sex, smoking habits, etc. are risk factors for rheumatoid arthritis [26]. In addition, it has been reported that married people have a longer life expectancy than single people, suggesting that marriage also has some effect on health [27, 28]. Furthermore, when Tibetan highlanders come and go in urban areas (normal oxygen environment), the adaptive mechanism may be switched on and off, which may add excessive stimulation to HIF expression. We thought that such changes in life and irritation to the body, such as drinking habits in a hypoxic environment, may be risk factors for rheumatoid arthritis through disturbance of HIF expression.
We suspect that the hypoxic adaptation mechanism acquired by Tibetan highlanders not only enables environmental adaptation but is also involved in promoting the onset of rheumatoid arthritis. Therefore, in this study, to clarify the actual situation of rheumatoid arthritis, to estimate the prevalence of rheumatoid arthritis, and to explore its risk factors among Tibetan highlanders, we conducted an epidemiological survey in Tsarang.
Methods
Study population
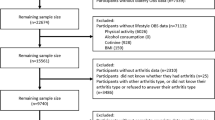
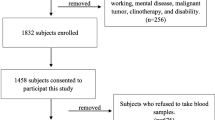
In June 2019, we conducted a cross-sectional study aimed at assessing arthritis status in Tibetan highlanders living in the village of Tsarang in the Mustang district of Nepal. The population of Tsarang is 452 people (217 males and 235 females), and among them, 179 males and 190 females are over the age of 18 years [29]. A venue was set up at the Health Post in Tsarang Village to conduct a survey. Children under the age of 18 years, pregnant females, patients with diseases such as cancer, and residents not born in the highlands were excluded. In this study, we hypothesize that Tibetan highlanders who have genetically acquired hypoxic adaptation over many years may be more likely to develop rheumatoid arthritis if they continue to be exposed to the hypoxic environment from when they were born. We planned the investigation based on this hypothesis. Therefore, we set such exclusion criteria to exclude nonhypoxic-adapted residents who were born and raised in the lowlands and migrated to the highlands.
Questionnaire survey
In the questionnaire survey, we investigated the basic attributes of the subjects, the consumption of cigarettes and alcohol, and the status of outpatient medication and dysfunction due to arthritis. In addition, to calculate the score of the clinical disease activity index (CDAI), we collected data on joint symptoms such as the number and location of joints with swelling and tenderness, the degree of pain, bilateral disability, and the duration of joint pain [30]. The CDAI is an index that was originally used for evaluating the activity of patients diagnosed with rheumatoid arthritis, but in this study, it was used to evaluate the degree of joint damage. The score is calculated according to the number of tender joints, the number of swollen joints, the subject’s visual analog scale (VAS), and the doctor’s VAS. Interviews using these questionnaires were conducted by Nepali- and Tibetan-speaking doctors and nurses.
Anthropometric and biochemical measurements
Trained researchers and medical staff measured the subject’s height, weight, blood pressure, hemoglobin concentration, and saturation of peripheral oxygen (SpO2). A tape measure was attached to the wall to measure height, and the Health meter HA-851-BL (TANITA, Tokyo, Japan) was used to measure weight. An automatic sphygmomanometer (OMRON Model, HEM-7210, Kyoto, Japan) was used to measure blood pressure, an ASTRIM FIT health monitoring analyzer (Sysmex, Kobe, Japan) was used to measure hemoglobin concentration, and a pulse oximeter (Masimo Radical V 5.0, Masimo Corp, CA, USA) was used to measure SpO2. Body mass index (BMI) was calculated from height and weight (BMI = Weight (kg)/Height (m)2). The collected blood samples were centrifuged at 3000 rpm in Tsarang, and plasma was separated. Blood samples were transported to the Institute of Tropical Medicine, Nagasaki University according to the United Nations standards with UN3373 (Category B) containers, and the levels of rheumatoid factor (RF), anti-CCP antibody, C-reactive protein (CRP), and hyaluronic acid were measured by the outsourcing examination company (SRL, Inc. Tokyo, Japan).
The positive criteria for RF and anti-CCP antibody were > 15 IU/mL and ≥ 4.5 U/mL, respectively, and the high value criteria for CRP and hyaluronic acid were > 0.3 mg/dL and ≥ 50.0 ng/mL, respectively. In addition, for RF and anti-CCP antibody, more than 3 times the standard was considered very high. Furthermore, rheumatoid arthritis was classified according to the ACR/EULAR 2010 classification criteria based on biochemical measurement results, the degree of joint damage, and the duration of arthritis [31].
Although there are no major fluctuations, the cutoff values to be set vary by country and facility [32, 33]. In fact, the international classification standard ACR/EULAR2010 used in this study stipulates that “the positive standard exceeds the normal value for each facility” [34]. It also stipulates that “high positive is more than 3 times the upper limit of normal value.” Therefore, in this study, classification was performed according to the SRL criteria that were serologically tested.
Statistical analysis
Data were analyzed by Fisher’s exact tests, Welch’s t tests, and Cochrane-Armitage tests for comparison of the rates of each variable and shown as the mean ± standard deviation (SD) or percentage (%). In addition, to explore factors related to the increase in CDAI score and ACR/EULAR2010 score, we performed Spearman’s rank correlation coefficient analysis, linear regression analysis, and multivariate analysis using sociological variables and tobacco/alcohol consumption status as explanatory variables for each objective variable.
Sociological variables included marital status (married or unmarried), alcohol consumption habits (no drinking experience, past drinking history, drinking less than once a week, or drinking more than once a week), smoking habits (no smoking experience, past smoking history, smoking less than once a week, or smoking more than once a week), and living in an urban area (never or past experience living in Kathmandu or Pokhara). Kathmandu (altitude: 1400 m) is the capital city, and Pokhara (altitude: 822 m) is the second largest city in Nepal. Finally, to explore the association between smoking and the development of arthritis, Spearman’s rank correlation coefficient, linear regression analysis, and multivariate analysis were conducted using the data about daily activity restriction, small joint disorders, large joint disorders, or the values for serological factors. In addition, considering that sex is one of the risk factors for rheumatoid arthritis, all analyses were performed by sex in this study. The significance level was set to a p value of less than 0.05. R (version 3.5.3), and R studio was used for these statistical analyses.
Results
Subjects’ sociological and physiological characteristics
Twenty-seven males and 50 females participated in the field survey at Tsarang. In this study, we set exclusion criteria for subjects, but not all participants were applied to the exclusion criteria. Of the residents who participated, 23 males and 42 females agreed to donate blood, and blood tests were also conducted using blood samples for a total of 65 people. Subjects were classified according to basic attributes and cigarette and alcohol intake, and the numbers for each item and proportions are summarized in Table 1. The ages of males and females were 53.5 ± 11.3 and 51.2 ± 11.8 years, respectively, and there was no significant difference (p = 0.3981). Regarding education history, we classified the subjects into 4 groups (no educational history, elementary school, junior high school, high school or more), and the proportion of males and females in each group was denoted. Although a significant sex difference in the four groups of educational history was not identified (p = 0.0507), the proportion of non-educated subjects was higher among females (86.0%) than among males (59.3%). The employment rate (male: 25.9%, female: 12.0%, p = 0.2004), marital rate (male: 92.6%, female: 86.0%, p = 0.4814), and single marriage rate (not polygamy, male: 92.6%, female: 82.0%, p = 1.0000) were higher in males than in females. However, there were no statistically significant sex differences. In addition, 85.2% of males and 86.0% of females had experience working in cities (Kathmandu and Pokhara), and there was no significant sex difference (p = 1.0000). The prevalence of alcohol consumption was 81.5% for males and 58.0% for females, which was a significant sex difference (p = 0.0015), and smoking history was 66.7% for males and 60.0% for females, with no significant sex difference (p = 0.6281).
Table 2 summarizes the physiological values of the subjects. The mean systolic blood pressure was 135.7 ± 26.2 mmHg for males and 116.4 ± 22.6 mmHg for females, which was a significant sex difference (p = 0.0023). However, for other values, such as BMI (male: 23.8 ± 3.1, female: 23.7 ± 4.2, p = 0.9017), diastolic blood pressure (male: 84.6 ± 13.4 mmHg, female: 78.3 ± 13.1 mmHg, p = 0.0517), hemoglobin (male: 13.9 ± 1.9 g/dL, female: 14.4 ± 2.2 g/dL, p = 0.3839), and SpO2 (male: 89.2 ± 3.2%, female: 88.6 ± 5.1%, p = 0.5616), there were no significant sex differences.
The effects of arthritis on daily life, use of medications, and hospital visits
The proportion of subjects who felt that arthritis interfered with their daily lives was 68.0% among females and 44.4% among males, but no statistically significant difference was observed (p = 0.0543) (Table 3). Regarding the movement of their own joints, 22.2% of males and 26.0% of females answered that they were not satisfied, and there was no significant sex difference (p = 0.6825). The number of days of awareness of joint pain in the previous 7 days was 6–7 days in 34.0% of females and 25.9% of males and 0–2 days in 42.0% of females and 59.3% of males. No significant sex difference was found (p = 0.2248). Both the outpatient rate due to arthritis symptoms (male: 11.1%, female: 38.0%, p = 0.0163) and the medication rate (male: 11.1%, female: 34.0%, p = 0.0324) were higher in females.
Evaluation of arthritis by joint damage site and CDAI
Knees (55.6%), elbows (18.5%), and ankles (18.5%) were the joints most commonly affected by arthritis in males, and knees (56.0%), fingers (16.0%), elbows, and neck (14.0%) were the joints most commonly affected by arthritis in females (Fig. 1). The prevalence of subjects who had no symptoms of arthritis was 18.5% among males and 36.0% among females. In the evaluation of arthritis using CDAI, 88.9% of males and 64.0% of females had arthritis corresponding to remission or hypoactive rheumatoid arthritis. The proportion of males with moderate or severe arthritis was 11.0%, and the proportion of females was 36.0%. Thus, a significant sex difference was observed in the degree of joint damage (p = 0.0304) (Table 4).

Joint sites with swelling or tenderness by sex. The prevalence of subjects who had no symptoms of arthritis was 18.5% (n = 5) for males and 36.0% (n = 18) for females. No participants complained of hip, toe, or waist swelling or tenderness. Fingers include both hands and feet
Prevalence of rheumatoid arthritis by ACR/EULAR 2010 score
According to the RF measurement results, the subjects were classified as negative (male: 78.3%, female: 78.6%), weakly positive (male: 17.4%, female: 16.7%), or strongly positive (male: 4.3%, female: 4.8%). There were no significant sex differences in the proportions (p = 0.9940) (Table 5). The overall proportion of subjects who were positive for RF was 21.7% for males and 21.5% for females. The subjects were classified as negative (male: 100.0%, female: 95.2%) or strongly positive (male: 0.0%, female: 4.8%) according to the anti-CCP antibody level. No significant sex difference was found (p = 0.2878). In terms of the CRP positive rate, 30.4% of males were positive, and 21.4% of females were positive. In terms of the hyaluronic acid positive rate, 22.7% of males were positive, and 33.3% of females were positive, but neither measurement showed a significant sex difference (p = 0.5485, p = 0.5654). Furthermore, these criteria classified 4.3% of males and 7.1% of females as having rheumatoid arthritis, indicating a very high estimated prevalence.
Factors affecting ACR/EULAR 2010 score
Table 6 shows the correlation coefficient (r) between the ACR/EULAR2010 score and each explanatory variable, such as sociological factors and smoking habits and alcohol consumption, and the partial regression coefficient and p value from linear regression analysis. In males, the absolute value of the correlation coefficient between marriage status and smoking against the ACR/EULAR2020 score was over 0.2. In females, the absolute value of the correlation coefficient between age, drinking habits, and living in urban areas against the ACR/EULAR2020 score was over 0.2. In addition, in the linear regression analysis, neither factor had a significant linear relationship with the ACR/EULAR2020 score for males or females. Furthermore, multiple linear regression analysis was performed (Table 7). As a result, none of the factors were associated with ACR/EULAR 2010 scores in males. On the other hand, in females, two factors, older age (standardized parameter estimate = 4.84E−01, 95% CI = [9.19E−02, 8.76E−01], p = 0.0170) and history of urban residence (standardized parameter estimate = − 5.49E−01, 95% CI = [− 9.21E−01, 1.77E−01], p = 0.0050), significantly increased the ACR/EULAR 2010 score.
Factors affecting CDAI score
Table 8 shows the correlation coefficient (r) between the CDAI score and each explanatory variable, such as sociological factors and smoking habits and alcohol consumption, and the partial regression coefficient and p value by linear regression analysis. In males, the absolute value of the correlation coefficient between age, marriage status, drinking habits, and smoking habits against the CDAI score was over 0.2. In females, the absolute value of the correlation coefficient between age, marital status, and smoking habits against the CDAI score was over 0.2. In addition, in the linear regression analysis, marriage status, and smoking habits had a significant linear relationship with the CDAI score in females. Furthermore, multiple linear regression analysis was performed (Table 9). As a result, none of the factors were associated with CDAI scores in males. On the other hand, in females, three factors, having no spouse (standardized parameter estimate = 3.17E−01, 95% CI = [5.74E−02, 5.77E−01], p = 0.0179), smoking habits (standardized parameter estimate = 2.88E−01, 95% CI = [1.71E−02, 5.59E−01], p = 0.0377), and a history of urban residence (standardized parameter estimate = − 3.69E−01, 95% CI = [− 6.83E−01, − 5.60E−02], p = 0.0219), significantly increased CDAI scores.
Effects of smoking habits on joint symptoms
Table 10 shows the correlation coefficient (r) between smoking habits and each explanatory variable, such as activity limitation, joint disability, and serum data, and the partial regression coefficient and p value by linear regression analysis. In males, the absolute values of the correlation coefficients between large joint disability, CRP, and hyaluronic acid against smoking habits were over 0.2. In females, the absolute value of the correlation coefficient between CRP and hyaluronic acid was over 0.2. In addition, in the linear regression analysis, only hyaluronic acid had a significant linear relationship with smoking habits in males. Furthermore, multiple linear regression analysis was performed (Table 11). As a result, hyaluronic acid was significantly higher in both males (standardized parameter estimate = 6.03E−01, 95% CI = [3.06E−01, 9.01E−01], p = 0.0020) and females (standardized parameter estimate = 4.87E−01, 95% CI = [5.63E−02, 9.18E−01], p = 0.0291) who had a smoking habit.
Discussion
Characteristics of Tsarang residents
In terms of the use of alcohol and tobacco among the subjects, the alcohol consumption history of males was significantly higher than that of females, but there was no difference between males and females in smoking history. A survey of 2815 adults in the Pokhara district in 2013 found that 67.2% of males and 18.9% of females had consumed alcohol [35]. According to this study, the alcohol consumption rate of Tsarang residents is 81.5% for males and 42.0% for females, which may be higher than that in urban areas. In addition, the smoking rate in Nepal decreases annually, from 41% in 2000 to 35.5% in 2015 for males and from 28% in 2000 to 9% in 2015 for females [36]. In this study, 40.0% of females had a history of smoking, and highland females may have more opportunities to come into contact with tobacco than females in other regions in this country. Thus, it was suggested that females living in Mustang may have higher smoking and alcohol consumption rates than those living in urban areas. Smoking and drinking habits may be a public health problem, especially among high-altitude Mustang residents, because smoking habits have been reported to lead to vascular aging, reduced SpO2, and risk factors for rheumatoid arthritis [37,38,39].
Comparison of arthritis prevalence with other regions
In an American survey conducted between 2013 and 2015, 18.1% of males and 23.5% of females suffered from arthritis [40]. In a survey of arthritis in low- to middle-income countries, Russia had the highest rate of arthritis in the past year: 32.9% among males and 48.4% among females [41]. Comparison with these previous studies suggests that the high prevalence of arthritis in the Tsarang population may be a major public health problem.
Although no significant difference was observed between males and females in this study, the results suggest that females may be more strongly affected by arthritis in their daily lives. In fact, the proportion of people who went to the clinic or medical facility for arthritis and took medication was significantly higher among females than among males. Previous reports have shown that rheumatoid arthritis and osteoarthritis are more prevalent in females, and even infectious psoriatic arthritis is more likely to cause pain and dysfunction in females [42,43,44].
In this study, the knees were the most commonly impaired joints in both males and females. Upper Mustang is an area at one of the highest altitudes in the Mustang area. Many residents live in this area while farming or handling livestock, accounting for 45.2% of the total population in that region [45]. Since Tsarang, the study site, is located in Upper Mustang, it is considered that these types of physical labor place a burden on the knees. The next most common site of disability was the elbow in males and the finger in females. Males are more likely to be engaged in manual labor, and elbows and knees may be impaired. On the other hand, the proportion of females who had swelling or pain in the small joints of the fingers, which is a characteristic of rheumatoid arthritis, was higher than that of males. Therefore, it can be said that there was a sex difference in the characteristics of arthritis among Tsarang residents. Furthermore, in this study, the degree of disability associated with arthritis was evaluated using the CDAI. The CDAI is an index that was originally developed to evaluate the disease activity of patients diagnosed with rheumatoid arthritis, but in this study, the residents’ CDAI score was calculated to widely evaluate the presence or absence of arthritis and its severity among all participants, not limited to patients with rheumatoid arthritis. As a result, the rate of arthritis corresponding to moderate or high rheumatoid arthritis activity was significantly higher in females than in males.
Serological tests were conducted for rheumatoid factor, which increases in 50–80% of patients with rheumatoid arthritis, anti-CCP antibody, which has 98% specificity for rheumatoid arthritis diagnosis [46], CRP, which reflects a systemic inflammatory response, and hyaluronic acid, which increases in people who have experienced joint destruction [47]. A study of non-arthritic groups in Finland found an RF-positive rate of 2.1% and a strong positive rate of 1.0% [48]. In addition, a 2013 survey of the general population in Turkey found that 2.8% were RF-positive and 1% were anti-CCP antibody-positive [46]. Although these previous studies included data from younger people than this study because they targeted people aged 18 years and older, it was found that the positive rate of RF and anti-CCP antibodies in Tsarang residents was high.
Prevalence of rheumatoid arthritis
The standard currently used worldwide is the ACR/EULAR 2010, which was jointly created by the Rheumatoid Arthritis Society of the USA and Europe [34]. Many studies evaluating the prevalence of rheumatoid arthritis have used the 1987 or 2020 criteria, and comparing the prevalence of rheumatoid arthritis between such studies should be done carefully. However, even considering these differences in classification criteria, it was clear that the prevalence of rheumatoid arthritis in the Tsarang population obtained in this study was high. In a study that evaluated rheumatoid arthritis in Tibetan highlanders in Naku, China, using ACR/EULAR 2010, as in this study, it was reported that 4.86% of the subjects may have rheumatoid arthritis [49]. Studies comparing ancient human bone DNA with modern human DNA in the Annapurna Conservation Area, to which Mustang belongs, have previously reported that ancient human genes are still strongly inherited by the Mustang people [50]. In other words, the people of Mustang may strongly inherit the hypoxic adaptation genes of ancient Tibetan highlanders. Therefore, if the hypoxic adaptation mechanism of Tibetan highlanders promotes the development of rheumatoid arthritis through the expression of HIF, the prevalence of rheumatoid arthritis may be especially high in Tibetan highlanders living in Mustang. The relationship between the hypoxic adaptation gene and the onset of rheumatoid arthritis in Tibetan highlanders needs further verification from a genetic perspective.
Risk factors for rheumatoid arthritis among Tibetan highlanders
Previous studies have reported risk factors for rheumatoid arthritis, such as sex, age, heredity, smoking, exposure to particles of asbestos and silica, and obesity [20, 51]. In this study, we explored risk factors for rheumatoid arthritis in Tsarang residents by conducting linear multiple regression analysis using the ACR/EULAR 2010 score, which is a classification standard for rheumatoid arthritis, as the objective variable. It is not clear in this study how migrating to work in urban areas (lowlands) is a risk factor for rheumatoid arthritis. One possibility is that if highlanders born and raised in the highlands descend to the lowlands and then return to the highlands, the body will try to adapt to hypoxia again, and the expression level of HIF will temporarily increase. If so, highlanders who have lived in urban areas may be at increased risk of rheumatoid arthritis through overexpression of HIF.
Multiple regression analysis revealed that smoking, which has been reported as a risk factor for rheumatoid arthritis, may be widely involved in the development of arthritis, even at high altitudes. Furthermore, according to the results obtained by analyzing the relationship between the smoking habits of residents and joint disorders and biochemical factors in the blood, individuals with smoking habits tended to have higher blood hyaluronic acid levels among both males and females. Smoking was found to be a risk factor for arthritis in Tsarang residents.
The synovium is a loose connective tissue that constitutes the joint capsule. Synovial cells exist in the surface layer, and blood vessels and lymph vessels exist in the deep layer [52]. Therefore, the synovial fluid produced by the synovium is supplied to the joint cavity, and nutrients and oxygen are delivered to the cartilage where blood vessels are not distributed [52]. Inflammation of the synovium is considered to be one of the major pathologies of rheumatoid arthritis and results in severe tissue edema and overgrowth of approximately 10–15 layers of synovial cells [53]. In patients with rheumatoid arthritis, the expression of hypoxia-inducible factor (HIF) is elevated in fibroblast-like synovial cells (FLSs) and macrophage-like synovial cells (MLSs), which make up the inflamed hyperplastic synovium [54, 55]. In particular, FLSs, along with inflammatory cells, have been reported to be strongly involved in the onset and exacerbation of rheumatoid arthritis [56]. HIF-α has three isoforms (HIF-1α, HIF-2α, HIF-3α), and it has been reported that HIF-2α is mainly expressed in FLSs in the joint cavity of patients with rheumatoid arthritis [25, 57]. Therefore, smoking habits in the Tibetan Plateau may promote HIF production in the synovium and promote the development of rheumatoid arthritis. Further molecular biological verification is needed in the future.
Given that the primary purpose of evolution and adaptation is to leaving offspring, diseases such as rheumatoid arthritis, which often develop after the age of reproduction, have little effect on reproduction. Even if such disadvantages are inherent, it is considered that the selection that prioritizes adaptation to a hypoxic environment has been applied. It is possible that vulnerability against diseases such as rheumatoid arthritis have become apparent due to the increase in life expectancy and the introduction of tobacco among Tibetan highlanders.
Limitations of this study
In this study, we surveyed the inhabitants of Tsarang in the less populated Charang area. According to 2011 data, the population of the Charang region is reported to be 119 males and 131 females over the age of 35 [29]. No population data have been reported since then, but there have been no major fluctuations, and the population is still considered to be approximately the same. Although the representativeness in statistical analysis is not high, data and samples from the 1930s to the 1980s were acquired and analyzed. Having analyzed the characteristics of Tsarang populations, further research is needed to clarify their association with rheumatoid arthritis prevalence and hypoxic adaptation in Tibetan highlanders throughout Mustang.
Conclusions
In this study, we evaluated the symptoms of arthritis and estimated the prevalence of rheumatoid arthritis using classification criteria for Tibetan highlanders who have adapted to the hypoxic environment and fostered their own culture. The high prevalence of rheumatoid arthritis among Tsarang residents suggests that the hypoxic adaptation mechanism involving HIF in Tibetan highlanders may promote the onset or exacerbation of rheumatoid arthritis. The results of this study are valuable not only because of the anthropological characteristics of Tibetan highlanders but also because of the geographical isolation of Tsarang from urban areas. In addition, valuable results were obtained for both clinical patients with rheumatoid arthritis and the general population. In addition, this study is the first report describing the site of joint damage and its effect on daily life among Tibetan highlanders in detail. The high prevalence of rheumatoid arthritis among Tibetan highlanders may be related not only to the environmental factors analyzed in this study but also to hypoxic adaptation genes. Further investigation is needed to clarify the genetic factors involved.
Availability of data and materials
The datasets generated during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- CCP:
-
Cyclic citrullinated peptide
- CDAI:
-
Clinical disease activity index
- CRP:
-
C-reactive protein
- EPAS1:
-
Endothelial per-ARNT-sim domain protein 1
- FLSs:
-
Fibroblast-like synovial cells
- HIF:
-
Hypoxia-inducible factor
- MLSs:
-
Macrophage-like synovial cells
- SD:
-
Standard deviation
- SpO2 :
-
Saturation of peripheral oxygen
References
Meyer MC, Aldenderfer MS, Wang Z, Hoffmann DL, Dahl JA, Degering D, et al. Permanent human occupation of the central Tibetan Plateau in the early Holocene. Science. 2017;355(6320):64–7.
Zhang XL, Ha BB, Wang SJ, Chen ZJ, Ge JY, Long H, et al. The earliest human occupation of the high-altitude Tibetan Plateau 40 thousand to 30 thousand years ago. Science. 2018;362(6418):1049–51.
Aldenderfer M, Eng JT. Death and Burial among two ancient high-altitude communities of Nepal. A companion to South Asia in the past; 2016. p. 374–97.
Rome2rio. How to get from Kathmandu to Upper Mustang by bus, car or plane. 2021. https://www.rome2riocom/s/Kathmandu/Upper-Mustang. Accessed on 7 Jul 2021.
Darnal P. Significant heritages of Upper Mustang and issue of conservation. DJSA. 2017;11:1–23.
Dahal A. An investigation on vernacular architecture of Marpha, Mustang, Nepal and understanding the influences and changes in architecture and its sustainability. 2019. https://www.repositorieslibutexasedu/handle/2152/78406. Accessed on 1 Jul .
Erzurum SC, Ghosh S, Janocha AJ, Xu W, Bauer S, Bryan NS, et al. Higher blood flow and circulating NO products offset high-altitude hypoxia among Tibetans. Proc Natl Acad Sci U S A. 2007;104(45):17593–8.
Okumiya K, Sakamoto R, Ishimoto Y, Kimura Y, Fukutomi E, Ishikawa M, et al. Glucose intolerance associated with hypoxia in people living at high altitudes in the Tibetan highland. BMJ Open. 2016;6(2):e009728–e.
Arima H, Nakano M, Koirala S, Ito H, Pandey BD, Pandey K, et al. Unique hemoglobin dynamics in female Tibetan highlanders. Trop Med Health. 2021;49(1):2.
Koirala S, Nakano M, Arima H, Takeuchi S, Ichikawa T, Nishimura T, et al. Current health status and its risk factors of the Tsarang villagers living at high altitude in the Mustang district of Nepal. J Physiol Anthropol. 2018;37(1):20.
Silman AJ, Pearson JE. Epidemiology and genetics of rheumatoid arthritis. Arthritis Res Ther. 2002;4(3):S265.
Gabriel SE. The epidemiology of rheumatoid arthritis. Rheum Dis Clin North Am. 2001;27(2):269–81.
Alamanos Y, Voulgari PV, Drosos AA. Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Semin Arthritis Rheum. 2006;36(3):182–8.
Stojanović R, Vlajinac H, Palić-Obradović D, Janosević S, Adanja B. Prevalence of rheumatoid arthritis in Belgrade, Yugoslavia. Br J Rheumatol. 1998;37(7):729–32.
Drosos AA, Alamanos I, Voulgari PV, Psychos DN, Katsaraki A, Papadopoulos I, et al. Epidemiology of adult rheumatoid arthritis in northwest Greece 1987-1995. J Rheumatol. 1997;24(11):2129–33.
Cimmino MA, Parisi M, Moggiana G, Mela GS, Accardo S. Prevalence of rheumatoid arthritis in Italy: the Chiavari Study. Ann Rheum Dis. 1998;57(5):315–8.
Del Puente A, Knowler WC, Pettitt DJ, Bennett PH. High incidence and prevalence of rheumatoid arthritis in Pima Indians. Am J Epidemiol. 1989;129(6):1170–8.
Harvey J, Lotze M, Stevens MB, Lambert G, Jacobson D. Rheumatoid arthritis in a Chippewa Band. I. Pilot screening study of disease prevalence. Arthritis Rheum. 1981;24(5):717–21.
Danila MI, Reynolds RJ, Tiwari HK, Bridges SL Jr. Ethnic-specific genetic analyses in rheumatoid arthritis: incremental gains but valuable contributions to the big picture. Arthritis Rheum. 2013;65(12):3014–6.
Prevention CfDCa. Rheumatoid arthritis (RA). 2018. https://www.cdcgov/arthritis/basics/rheumatoid-arthritishtml. Accessed on 13 Apr 2021.
Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010;376(9746):1094–108.
Huerta-Sánchez E, Jin X, Asan BZ, Peter BM, Vinckenbosch N, et al. Altitude adaptation in Tibetans caused by introgression of Denisovan-like DNA. Nature. 2014;512(7513):194–7.
Majmundar AJ, Wong WJ, Simon MC. Hypoxia-inducible factors and the response to hypoxic stress. Mol Cell. 2010;40(2):294–309.
Beall CM. Andean, Tibetan, and Ethiopian patterns of adaptation to high-altitude hypoxia. Integr Comparative Biol. 2006;46(1):18–24.
Ryu J-H, Chae C-S, Kwak J-S, Oh H, Shin Y, Huh YH, et al. Hypoxia-inducible factor-2α is an essential catabolic regulator of inflammatory rheumatoid arthritis. PLoS Biol. 2014;12(6):e1001881.
Deane KD, Demoruelle MK, Kelmenson LB, Kuhn KA, Norris JM, Holers VM. Genetic and environmental risk factors for rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2017;31(1):3–18.
Rendall MS, Weden MM, Favreault MM, Waldron H. The protective effect of marriage for survival: a review and update. Demography. 2011;48(2):481–506.
Shurtleff D. Mortality and marital status. Public Health Rep. 1955;70(3):248–52.
Central_Bureau_of_Statistics. National population and housing census 2011 (National report). 2012; https://www.unstatsunorg/unsD/demographic/sources/census/wphc/Nepal/Nepal-Census-2011-Vol1pdf. Accessed on 25 June 2021.
Aletaha D, Nell VP, Stamm T, Uffmann M, Pflugbeil S, Machold K, et al. Acute phase reactants add little to composite disease activity indices for rheumatoid arthritis: validation of a clinical activity score. Arthritis Res Ther. 2005;7(4):R796–806.
Kay J, Upchurch KS. ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology (Oxford). 2012;51(Suppl 6):vi5–9.
Kameda H, Hirata A, Katagiri T, Takakura Y, Inoue Y, Takenaka S, et al. Prediction of disease flare by biomarkers after discontinuing biologics in patients with rheumatoid arthritis achieving stringent remission. Sci Rep. 2021;11(1):6865.
Taylor P, Gartemann J, Hsieh J, Creeden J. A systematic review of serum biomarkers anti-cyclic citrullinated Peptide and rheumatoid factor as tests for rheumatoid arthritis. Autoimmune Dis. 2011;2011:815038.
Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–81.
Adhikari TB, Rijal A, Kallestrup P, Neupane D. Alcohol consumption pattern in western Nepal: findings from the COBIN baseline survey. BMC Psychiatry. 2019;19(1):283.
Reduction GSoTH. Cigarettes in Nepal. 2020. https://www.gsthrorg/country/npl. Accessed on 27 Apr 2021.
Vold ML, Aasebø U, Melbye H. Low FEV1, smoking history, and obesity are factors associated with oxygen saturation decrease in an adult population cohort. Int J Chron Obstruct Pulmon Dis. 2014;9:1225–33.
MiYang J, HyeonCheol J, Lee K, Yim J. The acute effect of smoking a single cigarette on vascular status, SpO2, and stress level. Med Sci Monit. 2014;20:601–7.
Di Giuseppe D, Discacciati A, Orsini N, Wolk A. Cigarette smoking and risk of rheumatoid arthritis: a dose-response meta-analysis. Arthritis Res Ther. 2014;16:R61.
Prevention CfDCa. Arthritis. 2018. https://www.cdcgov/arthritis/data_statistics/national-statisticshtml. Accessed on 27 Apr 2021.
Brennan-Olsen SL, Cook S, Leech MT, Bowe SJ, Kowal P, Naidoo N, et al. Prevalence of arthritis according to age, sex and socioeconomic status in six low and middle income countries: analysis of data from the World Health Organization study on global AGEing and adult health (SAGE) Wave 1. BMC Musculoskelet Disord. 2017;18(1):271.
Zhang Y, Jordan JM. Epidemiology of osteoarthritis. Clin Geriatr Med. 2010;26(3):355–69.
Myasoedova E, Crowson CS, Kremers HM, Therneau TM, Gabriel SE. Is the incidence of rheumatoid arthritis rising?: results from Olmsted County, Minnesota, 1955-2007. Arthritis Rheum. 2010;62(6):1576–82.
Braaten TJ, Zhang C, Presson AP, Breviu B, Clegg D, Walsh JA. Gender differences in psoriatic arthritis with fatigue, pain, function, and work disability. J Psoriasis Psoriatic Arthritis. 2019;4(4):192–7.
Pandey R. The State of Food (In) Security in the Trans-Himalaya, Upper-Mustang, Nepal. DJSA. 2016;10:92–122.
Tasliyurt T, Kisacik B, Kaya SU, Yildirim B, Pehlivan Y, Kutluturk F, et al. The frequency of antibodies against cyclic citrullinated peptides and rheumatoid factor in healthy population: a field study of rheumatoid arthritis from northern turkey. Rheumatol Int. 2013;33(4):939–42.
Sawai T, Uzuki M. Serum hyaluronic acid level is a good marker for evaluating the process of joint destruction in rheumatoid arthritis. Int Congress Ser. 2001;1223:273–7.
Korpilähde T, Heliövaara M, Kaipiainen-Seppänen O, Knekt P, Aho K. Regional differences in Finland in the prevalence of rheumatoid factor in the presence and absence of arthritis. Ann Rheum Dis. 2003;62(4):353–5.
Zhang Q, Liu Q, Lin C, Baima Y, Li H, Gong H, et al. The prevalence of rheumatoid arthritis in middle-aged and elderly people living in Naqu City, Tibet, Autonomous Region of China. J Orthop Surg Res. 2020;15(1):338.
Jeong C, Ozga AT, Witonsky DB, Malmström H, Edlund H, Hofman CA, et al. Long-term genetic stability and a high-altitude East Asian origin for the peoples of the high valleys of the Himalayan arc. Proc Natl Acad Sci. 2016;113(27):7485.
Pradeepkiran JA. Insights of rheumatoid arthritis risk factors and associations. J Transl Autoimmun. 2019;2:100012.
Smith MD. The normal synovium. Open Rheumatol J. 2011;5:100–6.
McInnes IB, Schett G. The pathogenesis of rheumatoid arthritis. N Engl J Med. 2011;365(23):2205–19.
Hitchon C, Wong K, Ma G, Reed J, Lyttle D, El-Gabalawy H. Hypoxia-induced production of stromal cell-derived factor 1 (CXCL12) and vascular endothelial growth factor by synovial fibroblasts. Arthritis Rheum. 2002;46(10):2587–97.
Hua S, Dias TH. Hypoxia-inducible factor (HIF) as a target for novel therapies in rheumatoid arthritis. Front Pharmacol. 2016;7:184.
Li G-Q, Zhang Y, Liu D, Qian Y-Y, Zhang H, Guo S-Y, et al. PI3 kinase/Akt/HIF-1α pathway is associated with hypoxia-induced epithelial–mesenchymal transition in fibroblast-like synoviocytes of rheumatoid arthritis. Mol Cell Biochem. 2013;372(1):221–31.
Fan L, Li J, Yu Z, Dang X, Wang K. The hypoxia-inducible factor pathway, prolyl hydroxylase domain protein inhibitors, and their roles in bone repair and regeneration. Biomed Res Int. 2014;2014:239356.
Acknowledgements
We appreciate all the highlanders who participated in this research and the staff of Tsarang Health Post and Mustang District Hospital who kindly helped us. Additionally, we would like to thank Dr. Atsushi Kawakami and Dr. Mami Tamai for the helpful discussions.
Funding
This work was supported by Grants-in-Aid for Scientific Research (KAKENHI Grant Numbers 17H04659, 17H04731, and 19H05737) and the Program for Nurturing Global Leaders in Tropical and Emerging Communicable Diseases, Graduate School of Biomedical Sciences, Nagasaki University.
Author information
Authors and Affiliations
Contributions
Conceptualization: HA, SK, MN, and TY. Data curation: HA, SK, KN, MN, and TY. Formal analysis: HA and KN. Investigation: HA, SK, MN, HI, KMP, KP, BDP, and TY. Methodology: HA, SK, MN, and TY. Project administration: TY. Resources: TY and HI. Supervision: TY and BDP. Writing—original draft: HA. Writing—review and editing: HA, SK, MN, KP, and TY. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committees of the Nepal Health Research Council (Approval # 142/2016) and the Institute of Tropical Medicine, Nagasaki University (# 150226137-3). Each participant in this study was provided detailed information about the research objectives, data collection procedures, benefits, risks, and confidentiality before written informed consent was obtained. In addition, when explaining the research content, we stated that participation in this research is voluntary and that the participant could be excluded from the research at any time.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Arima, H., Koirala, S., Nema, K. et al. High prevalence of rheumatoid arthritis and its risk factors among Tibetan highlanders living in Tsarang, Mustang district of Nepal. J Physiol Anthropol 41, 12 (2022). https://doi.org/10.1186/s40101-022-00283-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40101-022-00283-3