
Abstract
Background
Diagnosis and treatment of stress fractures still remains to be a clinical and radiological challenge. Therapeutic options vary from conservative treatment to surgical treatment without a clear treatment concept. Recently the combination of PET and MRI has been introduced, aiming a superior diagnostic accuracy in clinical practice. Therefore the aim of our study was to analyse whether PET-MRI would be a feasible technique to recognize stress fractures of the foot and to analyse if our conservative treatment plan leads to a good clinical outcome.
Methods
Therefore, 20 patients with suspected stress fractures of the foot and ankle underwent plain radiography and 18F-Fluoride PET-MRI. Two blinded readers assessed in consensus both imaging techniques for the presence of stress fracture, stress reaction or osteoarthritis. Patients with stress fractures or stress reactions in the foot and ankle area underwent our conservative treatment plan, with immobilization in a VACO®ped cast for 6 weeks under partial weight bearing on forearm crutches. The benefit of our conservative therapeutic concept was evaluated by the patients on the basis of VAS and FAOS scoring systems before and after treatment.
Results
8 out of 20 patients underwent conservative treatment after diagnosis of either a stress fracture or a stress reaction of the foot and ankle area. PET-MRI identified four stress fractures and seven stress reactions. In all cases, no pathological findings were present on plain X-ray. FAOS and VAS significantly improved according to the patients’ records.
Conclusions
PET-MRI seems to be a useful modality to diagnose stress fractures and stress reactions of the foot and ankle area, especially when conventional modalities, such as plain radiographs fail. Conservative management is a promising therapeutic option for the treatment of stress fractures. To rule out the benefits compared to a surgical treatment plan, further studies are needed.
Similar content being viewed by others


Background
Due to the increasing number of recreational athletes, sports-related injuries represent a significant challenge in orthopaedic medicine [1, 2]. Among these injuries stress-related fractures (SFX) have gained increased attention in the recent past. Every loading exposes bone to internal forces of stress and deformation or strain. SFX occur due to repetitive overuse and/or overload, when stress-induced microfractures exceed the remodelling capacity of the bone and accumulate into macrofractures [3, 4]. Further factors contributing to SFX involve hormonal, metabolic and nutrition components [5]. Also anatomical predilections like leg length differences, pes planus/cavus and high Q-angle may increase the risk. SFX have been described in different parts of the human skeleton but are most common in the lower extremity areas of the tibia (23.6 %), navicular (17.6 %), metatarsals (16.2 %), femur (6.6 %) but are also reported in the fibula, navicular, sesamoid, sacrum (1.6 %) and ribs [4, 6]. Therefore SFX of the lower extremity account for 80–90 % of all SFX, representing between 0.7 and 20 % of all sports-related injuries. They are commonly observed among individuals who participate in endurance, high load-bearing activities with the highest incidences of up to 15 % observed in long-distance and track athletes followed by gymnasts and field athletes [5].
In orthopaedic sports medicine, the fracture site is crucial for the therapeutic management. Stress injuries are classified as either high-risk or low-risk injuries according to their location and the associated anatomic preconditions [5, 7]. Depending on the grading, the therapeutic options in case of SFX vary. Conservative treatment involves restriction of weight bearing, physical activity and, depending on severity, lasts from 6 weeks to over 6 months [3]. Operative treatment is only described as second choice in current literature [8, 9].
Besides the requirement of long periods of recovery, the functional outcome is often complicated by delays in diagnosis. Accurate diagnosis of SFX is based on the patient’s history, the anatomical area and different imaging techniques [10]. Regardless, early recognition is the optimal goal to minimize the potential for microfractures to turn into macrofractures. Standalone X-ray provides a sensitivity ranging from 12 to 56 %, while specificity ranges from 88 to 96 %, implying that many stress fracture diagnoses might be missed [3]. In contrast magnetic resonance imaging (MRI), the current gold standard in literature reveals a sensitivity of 68–99 %, while specificity ranges from 4 to 97 % [3, 6, 10]. Summarizing MRI currently is the most effective imaging modality for diagnosing SFX. However, it carries the potential of overdiagnosis and treatment, i.e. longer restriction of weight bearing in simple bone oedema or osteoarthritic degeneration.
Recently, positron emission tomography (PET) MRI, as a combination of morphological and functional imaging, has been introduced in clinical practice [9, 11, 12]. This new technique offers, besides the information on soft tissue and bone marrow pathology, an additional diagnostically relevant information on the bone metabolism when using 18F-Fluoride as a radiotracer.
Therefore, the aim of our study was to analyse, whether 18F-Fluoride PET-MRI would be a feasible technique to recognize stress fractures of the foot and to analyse if a conservative treatment plan leads to a good clinical outcome in patients suffering from foot and ankle pain due to acute fractures or stress reactions.
Methods
Patients
Between February 2012 and March 2013, 20 patients with suspected stress fractures of the ankle/foot were prospectively enrolled. Inclusion criteria were: localized pain in the foot and ankle area for at least 6 weeks without an adequate trauma in the patients’ history, X-rays of the affected area without verification of a fracture line and written informed consent to undergo 18F-Fluoride PET-MRI examination. The study was approved by the local institutional review board of Klinikum rechts der Isar (reference number: 2967/10). Exclusion criteria were: age under 18, pregnancy and contraindications for 18F-Fluoride PET-MR imaging. A comparison between 18F-Fluoride PET/MR and 18F-Fluoride PET/CT in these patients has been recently published [13]. However, this previously published study only showed theoretical aspects of the use of 18F-Fluoride PET/MR for the diagnosis of unclear foot pain, the present study examines the practical use of 18F-Fluoride PET/MR for the diagnosis of stress fractures, as a delayed diagnosis can lead to multiple complications like prolonged pain or non-unions [14].
Diagnostic and therapeutic regime
In case the patients matched the inclusion criteria and approved their written consent, the Foot and Ankle Outcome Score (FAOS) and the Visual Analogue Scale (VAS) were determined. The patients were then submitted to the department of nuclear medicine, where 18F-Fluoride PET-MR imaging was performed. PET-MR images were analysed in consensus by a dual-board-certified radiologist and nuclear physician with several years of experience in PET-imaging reading and a board-certified radiologist with special training in musculoskeletal radiology. The criteria for the diagnosis of osteoarthritis, stress reaction and stress fracture using 18F-Fluoride PET-MR were recently published [13].
After the analysis of the PET-MR scans, the patients were examined in the outpatient clinic, where the results were discussed. Only the patients who showed either stress fractures or stress reactions in the PET-MR scans underwent our conservative treatment plan, all other patients were not included in our follow-up examinations. Each patient with stress fractures/stress reactions in the 18F-Fluoride PET-MRI-Scan received a VACOped® cast and was mobilized with partial weight bearing (15–20 kg) with forearm crutches for 6 weeks. After 12 weeks, the patients were examined in the outpatient clinic again, the FAOS and VAS were determined for a second time.
Questionnaire
The Foot and Ankle Outcome Score (FAOS) consists of 42 Likert Scale questions. It is divided into five separate subscales: symptoms (7 questions), pain (9 questions), function (17 questions), sports performance (5 questions) and quality of life (4 questions). Results range from 0 to 100 points. A score of 0 indicates poor points, a score of 100 indicates the best score [15, 16].
18F-Fluoride PET-MRI
All of the 18F-Fluoride PET-MR examinations were conducted on a whole-body hybrid 18F-Fluoride PET-MR system (Biograph mMR; Siemens Healthcare, Erlangen, Germany). For attenuation correction, a coronal 2-point Dixon 3D volumetric interpolated examination (VIBE) T1-weighted (T1w) MR sequence was acquired. Together with the start of this Dixon MR sequence, the PET acquisition (20 min) started simultaneously in the same BP, thus ensuring optimal temporal and regional correspondence between MRI and PET data. Additionally, a dedicated MR protocol of the foot was defined depending on the localization of the maximum pain with the following parameters: slice thickness 3 mm, field of view (FoV) 120–225 mm, matrix: 320 × 256–384 × 384. The protocol consisted of at least one intermediate-weighted fat-saturated (PDfs) sequence in two planes and one T1- and T2-weighted turbo spin echo (TSE) sequence.
Statistical analysis
Data are given in mean values (arithmetic mean) and standard deviations. For the comparison of the FAOS score, the paired t test was performed with the software SigmaStat Version 3.5 (Systat Software, Inc., San Jose, California, USA).
Results
Between February 2012 and March 2013, 20 patients were included in our study. Eight patients of our study group were identified with either stress fractures or stress reactions by 18F-Fluoride PET-MRI. 7 of these 8 patients showed stress reactions and stress fractures at the same time, 1 patient showed an isolated stress fracture without a concomitant stress reaction. The priorly performed X-rays of these patients showed no pathological findings (see Table 1).
The other patients (n = 12) had no specific findings besides osteoarthrosis, neither in the PET-MRI nor in the other modalities. Eight patients of our study population underwent conservative treatment as described above. FAOS significantly improved from 35.9 ± 12.6 before treatment to 51.7 ± 12.5 after treatment (p ≤ 0.001). Pain also significantly improved from 3.6 ± 0.7 before treatment to 1.6 ± 0.74 after treatment (p ≤ 0.001) measured by to the Visual Analogue Scale (VAS) (see Table 1).
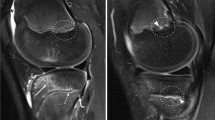
Diagnostic imaging of two patients who underwent conservative treatment is shown exemplarily in Figs. 1, 2. Figure 1 illustrates the X-ray (a), CT (b), MRI (c) and 18F-Fluoride PET-MRI (d) scans of a 58-year-old female patient. She complained about progressive pain in the calcaneocuboid joint and the dorsal calcaneus for several months, without an adequate trauma in her history. The pain had an intensity of 3 on the Visual Analogue Scale (VAS), the FAOS was 48.75 before treatment. No relevant medical findings were seen on the X-ray, the sagittal CT images (b) showed sclerotic lesions in the dorsal calcaneus and degenerative changes in the talonavicular region. With the help of 18F-Fluoride PET-MRI a stress fracture in the dorsal calcaneus and the mediodorsal parts of the cuboid, with little bone marrow oedema (c), coming along with a higher fluoride uptake in the 18F-Fluoride PET-MR (d) could be detected. After conservative treatment, the patients’ situation improved. Pain was reduced by two points (3 to 1) on the VAS and the FAOS increased up to 64.25 points. Figure 2 shows the X-ray and PET-MRI scans of a 45-year-old female patient with progressive pain in the third and fourth metatarsal bone (OMT) after operative treatment of a Weber B fracture of the same ankle. 10–12 weeks after the operation, when the patient started to be more active, the pain occurred without any signs of trauma. A VAS of 3 and a FAOS of 23.75 were described before treatment (see Table 1). The X-ray showed slight degenerative changes, whereas acute stress reactions in the OMT III and IV heads were detected by 18F-Fluoride PET-MR with high tracer uptake (see Fig. 2). With our conservative treatment, a reduction of pain (VAS 3 to VAS 1) and an increased FAOS (up to 35 points) could be achieved.

X-ray (a), CT scan (b), MRI scan (c) and 18F-Fluoride PET-MR (d) images of a 58-year-old female patient (patient no. 13). In the lateral X-ray (a) of the ankle region, neither acute stress fractures, nor degenerative lesions can be diagnosed. Sagittal CT images (b) show sclerotic lesions in the dorsal calcaneus (red arrow) and degenerative changes in the talonavicular region, no acute stress fractures are shown. Sagittal MRI images (c) show a fracture line in the dorsal calcaneus with little oedema (red arrow), due to an older stress fracture, coming along with a higher fluoride uptake in the 18F-Fluoride PET-MR (d, red arrow). Another stress fracture is shown in the mediodorsal parts of the cuboid with bone marrow oedema in the MRI scan (c, dotted arrow) and a higher fluoride uptake in the 18F-Fluoride PET-MR (d, dotted arrow)

X-ray (a) and 18F-Fluoride PET-MR (b) images of a 45-year-old female patient (patient no. 5). The a.p. X-ray (a) of the left foot shows no acute stress fractures, degenerative changes in the tarso-metatarsal and metatarsophalangeal joints are illustrated. 18F-Fluoride PET-MR (b) show high tracer uptake in OMT III/IV heads suitable to an acute stress reaction, no fracture lines can be detected
Discussion
Our study showed that 18F-Fluoride PET-MR can be useful in the diagnostics of stress fractures. 8 out of 20 patients with unclear foot/ankle pain were either diagnosed with “stress fractures” or with “stress reactions”. All of these patients underwent conservative treatment, following which a significant improvement of the FAOS and a pain reduction in the VAS could be achieved.
With the help of 18F-Fluoride PET-MRI, eight patients with relevant bony lesions could be identified in our study. Plain radiography showed no suspicious lesions in these cases. However, 18F-Fluoride PET-MR clearly illustrated even the small lesions directly due to a higher tracer uptake (18F-Fluoride PET-MR) and indirectly due to the bone marrow oedema, symbolizing large impact on the bone (MRI).
Looking at the current literature, different modalities such as plain radiography, computed tomography, scintigraphy and MRI are frequently used to diagnose stress fractures [6, 17, 18]. Even with the help of more than one single modality, diagnosis still remains a challenge [3]. Radiographs of the foot and ankle are often used as first-line diagnostic feature [19, 20]. Although X-rays are easy and fast to perform with only little amounts of radiation for the patient, there are limits when it comes to the diagnosis of small bony lesions. Especially in the early stages, only one-third of the fractures show typical radiographic signs [20, 21]. Local sclerosis and dense lines can only be observed as indirect fracture signs a few weeks after trauma with plain radiographs [17]. Therefore, additional imaging can be helpful.
Another widely accepted diagnostic feature—especially in the initial diagnostic phase—is computed tomography. Shearman et al. reviewed eight cases of longitudinal tibial stress fractures, respectively with respect to the ideal diagnostic modality. All of the patients had received normal plain radiographs initially. Additional CT imaging was performed in three cases and showed characteristic cortical lesions [20]. A high specificity of CT imaging in the diagnosis of stress reactions is also described by Gaeta et al. [19]. However, regarding the sensitivity of the diagnosis, MRI had advantages to CT [19, 22]. Fredericson et al. performed radiographs, scintigraphy (technetium bone scan) and MRI scans in fourteen runners with symptomatic leg pain and revealed that the MRI findings correlated with the scintigraphy, but the exact anatomical region of the lesion could be defined more precisely by MRI than by scintigraphy [23]. These findings are also confirmed by Miller et al. [24]. Scintigraphy itself shows a high sensitivity besides a very low specificity in the diagnosis of stress fractures [25]. Diagnosis of stress reactions remains to be a very big challenge. Apart from the high diagnostic effort, 18F-Fluoride PET-MRI, as an additional diagnostic tool, seems to be a suitable modality combining the high sensitivity of 18F-Fluoride PET with the high specificity of MRI in patients with suspected stress fractures.
After diagnosis, our patients underwent conservative treatment. They were immobilized in a VACOped® Cast for 6 weeks under partial weight bearing with 15–20 kg on forearm crutches. Although multiple different therapeutic strategies exist in current literature [3, 9], the ideal treatment of stress fractures still remains to be a big problem nowadays. Depending on the specific sites of occurrence, stress fractures can be classified into low-risk and high-risk fractures [5]. While low-risk stress fractures have a good chance to heal with conservative treatment, high-risk fractures are prone to delayed unions or non-unions more often [7]. An operative regimen with open reduction and internal fixation (ORIF) has been described by a few authors in current literature [26, 27]. Rongstad et al. showed the benefits of operative treatment of fourth metatarsal stress fractures in a retrospective study on 14 patients. 11 of the 14 patients chose operative treatment (ORIF) and returned to sports at an average of 12 weeks post surgery and would choose surgery for this kind of fracture again [27]. Nevertheless, an operative regimen is discussed controversially in current literature [10, 28] and a conservative regimen is preferred in most of the cases [1, 18, 29]. Operative treatment after failed fracture healing is described by Karthik et al. in a case of bilateral scapular spine stress fractures, where one side had united with conservative treatment and the other side had to be operated because of pain and non-union. The patient was asymptomatic at the final follow-up on both sides 2 years posttraumatically [30]. The ideal therapy of stress fractures is not found yet. We have good experiences with our conservative treatment regimen. Conservative therapy as first-line therapy is supported by many authors especially in low-risk stress fractures [1, 5, 7]. Operation after failed conservative treatment seems to be a good therapeutical concept.
Conclusions
Stress fractures pose a challenge for modern medicine. Modern imaging techniques such as 18F-Fluoride PET-MR seems to be useful for diagnosis, especially when conventional methods do not detect the reason for unclear foot pain. Depending on the fracture site, the functional claim and the age of the patient, the right treatment regimen should be determined. For evaluating the benefits of operative vs. non-operative treatment, further studies are needed.
Abbreviations
- CT:
-
computed tomography
- FAOS:
-
foot and ankle outcome score
- MRI:
-
magnetic resonance imaging
- OMT:
-
metatarsal bone
- ORIF:
-
open reduction internal fixation
- PET:
-
positron emission tomography
- SFX:
-
stress-related fractures
- VAS:
-
visual analogue scale
References
Changstrom BG, Brou L, Khodaee M, Braund C, Comstock RD. Epidemiology of stress fracture injuries among US high school athletes, 2005–2006 through 2012–2013. Am J Sports Med. 2015;43(1):26–33. doi:10.1177/0363546514562739.
Asano L, Duarte A Jr, Silva A. Stress fractures in the foot and ankle of athletes. Rev Assoc Med Bras. 2014;60(6):512–7. doi:10.1590/1806-9282.60.06.006.
Gehrmarnn R, Renard R. Current concepts stress fractures. Foot Ankle Int. 2006;27:750–7.
Mayer SW, Joyner PW, Almekinders LC, Parekh SG. Stress fractures of the foot and ankle in athletes. Sports Health. 2014;6(6):481–91. doi:10.1177/1941738113486588.
Boden BP, Osbahr DC, Jimenez C. Low-risk stress fractures. Am J Sports Med. 2001;29:100–11.
Daffner RH, Pavlov H. Stress fractures: current concepts. Am J Roentgenology. 1992;159:245–52.
Boden BP, Osbahr DC. High-risk stress fractures: evaluation and treatment. J Am Acad Orthop Surg. 2000;8:344–53.
Chen YT, Tenforde AS, Fredericson M. Update on stress fractures in female athletes: epidemiology, treatment, and prevention. Curr Rev Musculoskelet Med. 2013;6(2):173–81. doi:10.1007/s12178-013-9167-x.
Schmoz S, Voelcker AL, Burchhardt H, Tezval M, Schleikis A, Sturmer KM, et al. Conservative therapy for metatarsal 5 basis fractures—retrospective and prospective analysis. Sportverletzung Sportschaden: Organ der Gesellschaft fur Orthopadisch-Traumatologische Sportmedizin. 2014;28(4):211–7. doi:10.1055/s-0034-1385611.
Pegrum J, Dixit V, Padhiar N, Nugent I. The pathophysiology, diagnosis, and management of foot stress fractures. Phys Sports Med. 2014;42:87–99.
Yoo HJ, Lee JS, Lee JM. Integrated whole body MR/PET: Where are we? Korean J Radiol. 2015;16:32–49.
Rosenkrantz AB, Koesters T, Vahle AK, Friedman K, Bartlett RM, Taneja SS, et al. Quantitative graphical analysis of simultaneous dynamic PET/MRI For assessment of prostate cancer. Clin Nucl Med. 2015;40:236–40.
Rauscher I, Beer AJ, Schaeffeler C, Souvatzoglou M, Cronlein M, Kirchhoff C, et al. Evaluation of 18F-fluoride PET/MR and PET/CT in patients with foot pain of unclear cause. J Nucl Med Off Publ Soc Nucl Med. 2015;56(3):430–5. doi:10.2967/jnumed.114.150532.
Welck MJ, Hayes T, Pastides P, Khan W, Rudge B. Stress fractures of the foot and ankle. Injury. 2015. doi:10.1016/j.injury.2015.06.015.
van Bergen CJ, Sierevelt IN, Hoogervorst P, Waizy H, van Dijk CN, Becher C. Translation and validation of the German version of the foot and ankle outcome score. Arch Orthop Trauma Surg. 2014;134(7):897–901. doi:10.1007/s00402-014-1994-8.
Segal G, Elbaz A, Parsi A, Heller Z, Palmanovich E, Nyska M, et al. Clinical outcomes following ankle fracture: a cross-sectional observational study. J Foot Ankle Res. 2014;7:50.
Miltner O. Stress reactions in bones of the foot in sport: diagnosis, assessment and therapy. Der Unfallchirurg. 2013;116(6):512–6. doi:10.1007/s00113-013-2373-6.
Liong SY, Whitehouse RW. Lower extremity and pelvic stress fractures in athletes. Br J Radiol. 1016;2012(85):1148–56. doi:10.1259/bjr/78510315.
Gaeta M, Minutoli F, Mazziotti S, Visalli C, Vinci S, Gaeta F, et al. Diagnostic imaging in athletes with chronic lower leg pain. AJR Am J Roentgenol. 2008;191(5):1412–9. doi:10.2214/AJR.07.3379.
Shearman C, Brandser E, Parman L, El-Khoury G, Saltzman C, Pyevich M, et al. Longitudinal tibial stress fractures: a report of eight cases and review of the literature. J Comput Assist Tomogr. 1998;22:265–9.
Savoca C. Stress fractures. A classification of the earliest radiographic signs. Radiology. 1971;100:519–24.
Tins BJ, Garton M, Cassar-Pullicino VN, Tyrrell PN, Lalam R, Singh J. Stress fracture of the pelvis and lower limbs including atypical femoral fractures—a review. Insights Imaging. 2014. doi:10.1007/s13244-014-0371-z.
Fredericson M, Bergman A, Hoffman K, Dillingham M. Tibial stress reaction in runners: correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system. Am J Sports Med. 1995;23:472–81.
Miller TL, Harris JD, Kaeding CC. Stress fractures of the ribs and upper extremities: causation, evaluation, and management. Sports Med. 2013;43(8):665–74. doi:10.1007/s40279-013-0048-7.
Burke R, Chiang AL, Lomasney LM, Demos TC, Wu K. Multiple anterior tibial stress fractures complicated by acute complete fracture of the distal tibia. Orthopedics. 2014;37(4):217, 74–8. doi:10.3928/01477447-20140401-01.
Jacob KM, Paterson RS. Navicular stress fractures treated with minimally invasive fixation. Indian J Orthop. 2013;47(6):598–601. doi:10.4103/0019-5413.121589.
Rongstad KM, Tueting J, Rongstad M, Garrels K, Meis R. Fourth metatarsal base stress fractures in athletes: a case series. Foot Ankle Int. 2013;34(7):962–8. doi:10.1177/1071100713475613.
Mallee W, Weel H, van Dijk C, van Tulder M, Kerkhoffs G, Lin C. Surgical versus conservative treatment for high-risk stress fractures of the lower leg (anterior tibial cortex, navicular and fifth metatarsal base): a systematic review. Br J Sports Med. 2014;49:370–6.
Caesar BC, McCollum GA, Elliot R, Williams A, Calder JD. Stress fractures of the tibia and medial malleolus. Foot Ankle Clin. 2013;18(2):339–55. doi:10.1016/j.fcl.2013.02.010.
Karthik K, Lau J, Sinha J, Tavakkolizadeh A. Scapular spine stress fractures: to fix or not to fix, our experience in a patient with bilateral fractures and review of the literature. Int J Shoulder Surg. 2014;8:90–3.
Authors’ contributions
MC participated in the study design, conducted the literature search and drafted the manuscript. IR, ME, CS, GHS and CK assisted in the literature search and critical revisions of the manuscript for important intellectual content. MB and SH participated in the design of the study and performed the statistical analysis. AB, MS, ME, CS and PB conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We thank Fritz Seidl, M.A. Interpreting and translating, for professional language editing.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Crönlein, M., Rauscher, I., Beer, A.J. et al. Visualization of stress fractures of the foot using PET-MRI: a feasibility study. Eur J Med Res 20, 99 (2015). https://doi.org/10.1186/s40001-015-0193-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-015-0193-6