
Abstract
Background
Over 1 billion people suffer from chronic respiratory diseases such as asthma, COPD, rhinitis and rhinosinusitis. They cause an enormous burden and are considered as major non-communicable diseases. Many patients are still uncontrolled and the cost of inaction is unacceptable. A meeting was held in Vilnius, Lithuania (March 23, 2018) under the patronage of the Ministry of Health and several scientific societies to propose multisectoral care pathways embedding guided self-management, mHealth and air pollution in selected chronic respiratory diseases (rhinitis, chronic rhinosinusitis, asthma and COPD). The meeting resulted in the Vilnius Declaration that was developed by the participants of the EU Summit on chronic respiratory diseases under the leadership of Euforea.
Conclusion
The Vilnius Declaration represents an important step for the fight against air pollution in chronic respiratory diseases globally and has a clear strategic relevance with regard to the EU Health Strategy as it will bring added value to the existing public health knowledge.
Similar content being viewed by others


Background: chronic respiratory diseases are major chronic diseases across the life cycle
Over 1 billion people suffer from chronic respiratory diseases such as asthma, COPD, rhinitis and rhinosinusitis. Chronic respiratory diseases are major chronic diseases [1]. Asthma and allergic diseases occur along the life cycle from early childhood, affecting 30 million children and adults under 45 years of age in Europe. COPD has an estimated annual death rate of over 4 million people globally. The annual costs due to asthma (direct costs, indirect costs and loss of productivity) in the EU are estimated at 72 b€ and those due to COPD at 142 b€ [2]. Work productivity loss due to rhinitis is estimated at 30–50 b€ [3] and the disease has a major impact on sleep and anxiety [4]. Children with early onset asthma, active smoking, exposure to tobacco smoke and poverty are all risk factors of fixed airflow obstruction in adulthood [5,6,7].
The Polish Presidency of the EU Council (3051st Council Conclusions) made the prevention, early diagnosis and treatment of asthma and allergic diseases a priority to reduce health inequalities [8, 9]. The 3206th Cyprus Council Conclusions [10] recommended that the diagnosis and treatment of chronic diseases should be initiated as early as possible to improve active and healthy ageing (AHA). Several debates at the European Parliament recommended an early diagnosis and management of chronic respiratory diseases in children in order to promote AHA (Cyprus Presidency of the EU Council, 2012) [11], predictive medicine [12] and self-management strategies using mobile technology [13].
The Vilnius EU Summit on the prevention and management of chronic respiratory diseases (Vilnius, Lithuania, 23 March, 2018) followed these recommendations and attempted to provide a road map to prevent and control chronic respiratory diseases using integrated care pathways and the recent advances in mobile technology with a focus on air pollution.
Protective and risk factors
Chronic respiratory diseases and other chronic diseases often share risk factors (e.g. tobacco, including e-cigarettes, allergen exposure, nutrition, indoor and outdoor air pollution and sedentary lifestyle) [1, 14, 15], all leading to sustained local and systemic inflammation [16, 17] as well as ageing. Tobacco smoking is the best identified risk factor for many chronic diseases including chronic respiratory diseases. Allergens are of importance in rhinitis and asthma. Indoor and outdoor air pollution is another important risk factor for chronic respiratory diseases of increasing importance [18,19,20,21]. Ecosystems are impacted by air pollution, particularly sulphur and nitrogen emissions, and by ground-level ozone: these factors affect their ability to function and grow and have adverse effects on flora and fauna as well as on allergic diseases [22]. Moreover, these risk factors can interact to worsen chronic respiratory diseases and induce exacerbations [23].
Pre-natal and early-life events have a major impact on the development of chronic diseases in adults [24, 25] and older people. A better understanding of these links will enable the implementation of effective novel prevention strategies to promote AHA. The developmental origin of ageing is on the EU political agenda [9, 10, 26, 27].
Chronic disease prevention and control could be considered sequentially before the disease has been identified (i) to prevent its onset (health promotion and primary prevention), and (ii) after its onset, to better control and prevent its short- and long-term consequences (secondary and tertiary prevention and control). It should also be noted that early impairment of lung function is a marker of early all-cause systemic morbidity and mortality [23,24,25].
Health promotion and prevention should start at conception and continue steadily across the life cycle for healthy lungs and active and healthy ageing. They have been laid down from a political perspective to contribute to the goals of the Europe 2020 strategy of healthy and active ageing [28], the Sustainable Development Goals for 2030 (SDG) and the WHO strategy on chronic diseases. The strategy was also promoted by the Polish EU priority [8, 9]. Multi-sectoral prevention, including policy change, regulation, and market intervention, is of the highest priority.
There is a need to find novel health promotion strategies in chronic respiratory diseases and to promote value creation in order to promote AHA. Particular attention is required for tobacco smoke prevention and for air pollution mitigation strategies. It should be noted that there is ample evidence of the effectiveness of legislation to restrict smoking and reduce pollution, and that Governments should therefore be pushed to implement the best environmental policy.
Chronic respiratory diseases will be seriously impacted by climate change
Climate change is considered as a major threat for chronic respiratory diseases [29, 30]. Heat waves significantly increase morbidity and mortality in patients with chronic lung disease [31]. Climate change, mediated by greenhouse gases, causes adverse health effects to vulnerable chronic respiratory diseases patients including the elderly, children, and those in a distressed socioeconomic state [32]. Reducing greenhouse gas emission and improving air quality represent two global challenges [33].
Poor adherence to medication: a major factor in chronic respiratory disease-related burden and death
Public health measures play an essential role in improving outcomes, but, for conditions where effective medications are available, such as for non-severe asthma, patients are supported in taking their medication effectively. One important global cause of low adherence is that medications are not accessible or affordable [14], and this issue must be addressed across Europe, especially in middle-income countries. If medications are accessible, adherence is relatively high. This is a known important factor in asthma deaths [15]. Unfortunately, the education programmes that have been proposed over the past decades have not increased adherence. Innovative effective educational programmes using mobile technology and guided self-management appear to be crucial for the empowerment of patients and will increase and support their adherence to medications. However, evidence-based real-life studies should be proposed to confirm the importance of mHealth and lead to change management We need to develop evidence-based strategies to change the management of CRDs [34]. School-based interventions are also of great importance. Ensuring that practical support strategies are in place also represents an essential strategy for improving outcomes. On-demand strategies may be of great interest for the improvement of adherence [35, 36].
Prevention and treatment strategies at national or regional levels
Effective strategies are needed to reduce chronic respiratory disease burden. National programmes (Finnish, Czech, Portuguese Asthma or COPD Programmes) or national partnerships against chronic respiratory diseases (Italy, Netherlands, Lithuania, France, Romania, Belgium and Spain) can be cost-effective [37]. However, they are insufficiently implemented in many other EU countries, in particular in RIS countries [EIT Regional Innovation Scheme (EIT RIS)].
Integrated care pathways (ICPs) exist in some countries, such as the UK for COPD (QS10) (NICE) [38], France (HAS) and the Netherlands [39], but national ICPs for asthma or asthma and rhinitis comorbidity do not exist. Quality standards for asthma (QS25) have been published by NICE [40]. These are specific, concise statements that act as markers of high-quality and cost-effective patient care. Moreover, some initiatives are aimed at also incentivising good practice and improving implementation (i.e. remuneration based on performance indicators). In the UK, the Quality and Outcomes Framework (QOF) has 4 asthma-specific performance indicators which are explicitly linked to the subsequent remuneration of providers [41].
The Finnish Asthma 1994–2004 [42] and Allergy Programmes [43, 44] pioneered the field and have been found to be effective [45], demonstrating why public health problems need public health solutions. The programmes have been based on scientific innovations turned into practical actions. This has been possible in a country where the educational level of citizens is relatively high and where health care is efficiently organized and mainly funded by public money. Integration of the work of primary and secondary care physicians and nurses, pharmacists and caregivers has been the key for a better flow of information, education and patient care, while patient education and public awareness improved at the same time by organisations representing patients. However, the asthma programme has been successfully deployed in Europe [46] and developing countries [1, 37, 47]. The allergy programme has been deployed in Norway [48]. In asthma, improved detection of disease and recognizing asthma as an inflammatory disorder from the outset has led to early and effective management [49]. In the 2016 Pharmacy Barometer Survey, not more than 2.5% of Finnish asthma patients reported severe symptoms. In allergy, the turning avoidance into tolerance strategy, focusing on severe forms of disease and emphasizing health rather than mild problems, has encouraged a more rationale use of healthcare resources [3]. A nationwide cost analysis was also performed (Fig. 1) [50].

In 2013, direct and indirect asthma and allergy costs were €1.3–1.6 billion in Finland (population 5.5 million). From [50]
The Finish COPD programme has also been a success, the prevalence of smoking was reduced in both men and women, there was improved quality of diagnosis and reduction in hospitalizations (Fig. 2) [51].

Hospital admissions were reduced in Finland after initiation of the 10-year COPD programme (from Kinnula et al. [51])
The Finnish experience calls all European communities to take systematic and coordinated action to improve public health by lessening disability and costs caused by asthma and allergy. Inadequate care of these conditions seems to be a global problem delaying patient management and causing poor outcome [64]. Although many actions have already been taken in Europe [65], Lithuania and Baltic countries can speed up implementation and make it relevant to healthcare and society as a whole.
Multisectoral care pathways embedding guided self-management, mHealth and air pollution in chronic respiratory diseases
ICPs are structured multidisciplinary care plans which detail essential steps in the care of patients [52]. They promote the translation of guidelines into local protocols and their subsequent application to clinical practice [53]. They empower patients and their carers (health and social). ICPs differ from practice guidelines as they are utilised by a multidisciplinary team and have a focus on the quality and coordination of care. Multisectoral care pathways for multimorbid chronic respiratory diseases are needed [54] and should incorporate self-management and aerobiology to allow precision medicine with endotype-driven treatment [55].
A large number of chronic respiratory disease patients do not consult physicians because they think their symptoms are ‘normal’ and/or trivial. However, chronic respiratory diseases including rhinitis and asthma negatively impact social life, school and work productivity [56]. There is a clear role for the pharmacist for AR management in practice, through a guided change management process.
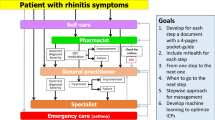
An example of an ICP has been proposed for allergic rhinitis (AR). Many rhinitis patients use over-the-counter (OTC) drugs [57] and only a fraction have had a medical consultation. The vast majority of patients who visit GPs or specialists have moderate/severe rhinitis [58,59,60,61,62]. GRADE-based guidelines are available for AR and their recommendations are similar [63,64,65]. However, they are based on the assumption that patients regularly use their treatment and are not tested with real-life data. Unfortunately, adherence to treatment is very low and real-life studies do not necessarily accord with all recommendations [66]. New-generation guidelines embedding real life data are needed.
Thus, ICPs should consider a multi-disciplinary approach as proposed by AIRWAYS ICPs (Fig. 3), using self-medication, shared decision making (SDM) and new-generation guidelines including messaging for increased adherence and information on aerobiology and air pollution.

Integrated care pathways for rhinitis and asthma multimorbidity embedding aerobiology
Self-care and shared decision making
Self-care is any necessary human regulatory function that is under individual control, deliberate and self-initiated. Chronic respiratory diseases require a long-term approach with emphasis on patient empowerment and appropriate support services stressing the importance of health literacy. In self-care, chronic disease patients make many day-to-day decisions. Self-management education complements traditional patient education. Self-care is learned, purposeful and continuous, otherwise it is dependent only on individuals’ specific circumstances, resources, beliefs, etc. Some important targets of self-care include the prevention of asthma and COPD exacerbations [67,68,69] but also the improvement of control of asthma, rhinitis or chronic rhinosinusitis [13, 70].
In shared decision making, both the patient and the health care professional contribute to the medical decision-making process, placing the patient at the centre of the decision [71]. For children, caregivers should contribute to the decision. Physicians explain treatments and alternatives to patients who can then choose the treatment option that best aligns with personal beliefs and goals and consider the benefits and risks [72]. In contrast to shared decision making, the traditional medical care system places physicians in a position of authority, with patients playing a passive role in care [73].
mHealth including messaging
mHealth has evolved from eHealth, the use of information and communication technology (ICT) for health services and information transfer. According to the World Health Organization (WHO) [74], mHealth “has the potential to transform the face of health service delivery across the globe. A powerful combination of factors is driving this change. These include rapid advances in mobile technologies and applications, a rise in new opportunities for the integration of mobile health into existing mHealth services, and the continued growth in coverage of mobile cellular networks.” The potential applications and benefits of mHealth are extensive and expanding [75]. mHealth may be of great value in self-care and shared decision making.
The potential for mHealth in chronic respiratory diseases is enormous [76] but implementing ICT innovations may also have adverse consequences. It is therefore important to test applicability in each individual situation [77]. Apps may be used to better understand and improve adherence, in particular using messaging, as well as to enable shared decision making and improve self-management of chronic diseases [78]. Patients, who are the final users of these apps, must be included not only in the testing phase, but also in the design and creation [79].
The Vilnius Declaration (VD)
The VD is an essential step for the fight against air pollution in chronic respiratory disease globally
A first meeting on air pollution in chronic respiratory diseases and mHealth was held during the 11th GARD meeting in Brussels (November 10, 2017). It paved the way for the VD.
-
POLLAR (Impact of Air POLLution on Asthma and Rhinitis) [80] is an EIT Health project that will propose strategies to predict and prevent air pollution peaks and chronic respiratory disease morbidity using mobile technology (Paris, January 2018).
-
The Vilnius EU Summit (March 2018) prepared the VD and proposed a meeting at the UN with the following objectives: (i) to tackle the future risk of air pollution and climate change in chronic respiratory diseases across the life cycle, (ii) to propose practical primary and secondary prevention strategies to meet this unprecedented public health challenge and (iii) to combat inequities.
-
The first ever WHO conference on air pollution and health was held in Geneva on October 30th–November 1st 2018, a clear sign that the problem is growing and that solutions are needed.
-
The 12th GARD meeting in Helsinki (August 2018) refined the VD for the UN High-Level Conference.
-
An ARIA-Masterclass (with Euforea) was the first teaching session on the subject and focussed on ICPs, self-management and shared decision making (Brussels, September 12 2018).
-
A meeting (HLC) was organized at the UN Assembly (September 27, 2018), the results of which led to an action plan for implementing recommendations.
-
A consensus meeting was organized (POLLAR, Paris, December 2018) to improve care pathway design in order to enhance patient participation, health literacy and self-care through technology-assisted ‘patient activation’ using rhinitis and asthma multimorbidity as a model of non-communicable disease. Pharmacy guidelines were included in this meeting.
-
With the results of POLLAR, a consensus meeting was organized (POLLAR, Paris, December 2019) to embed aerobiology and air pollution in ICPs.
The VD
The Vilnius Declaration was developed by the participants of the EU Summit on chronic respiratory diseases (Vilnius, March 23, 2018) under the leadership of Euforea (“Appendix”).
The expected impact of the VD
The VD has a clear strategic relevance with regard to the EU Health Strategy as it will bring added value to the existing public health knowledge:
-
To propose a common framework for integrated care pathways in chronic respiratory diseases (and their co-morbidities) for the entire EU which can be expanded to Eastern European and other regions and which will allow comparability and trans-national initiatives;
-
To help risk stratification in chronic respiratory disease patients with a common strategy;
-
To develop cost-effective policies, in particular strengthening those on smoking, including e-cigarettes, and environmental exposure;
-
To propose a common simulation tool for the entire EU to assist physicians in the segmentation of patients and choice of pathways;
-
To develop the interoperability of mHealth systems in Europe, including transborder interoperability in Eastern European regions (border between EU member states and associate EU countries);
-
To have a significant impact on the health of citizens in the short term (reduction of morbidity, improvement of education in children and of work in adults) and in the long term (healthy ageing).
Conclusions
The Vilnius Declaration represents an important step for the fight against air pollution in chronic respiratory diseases globally and has a clear strategic relevance with regard to the EU Health Strategy as it will bring added value to the existing public health knowledge.
Change history
17 November 2020
An amendment to this paper has been published and can be accessed via the original article.
Abbreviations
- AHA:
-
active and healthy ageing
- AR:
-
allergic rhinitis
- ARIA:
-
Allergic Rhinitis and its Impact on Asthma
- COPD:
-
chronic obstructive pulmonary disease
- EIT:
-
European Institute for Innovation and Technology
- EU:
-
European Union
- Euforea:
-
European Forum for Research and Education in Allergy
- GARD:
-
Global Alliance Against Chronic Respiratory Diseases
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
- ICP:
-
integrated care pathway
- ICT:
-
information and communication technology
- NICE:
-
National Insitute for Health and Care Excellence
- OTC:
-
over the counter
- POLLAR:
-
Impact of Air POLLution on Asthma and Rhinitis
- SDG:
-
Sustainable Development Goals
- VD:
-
Vilnius Declaration
- WHO:
-
World Health Organization
References
Bousquet J, Khaltaev N. Global surveillance, prevention and control of chronic respiratory diseases. A comprehensive approach. Global Alliance against Chronic Respiratory Diseases. World Health Organization. 2007. ISBN 978 92 4 156346 8.
Gibson GJ, Loddenkemper R, Lundback B, Sibille Y. Respiratory health and disease in Europe: the new European Lung White. Book. Eur Respir J. 2013;42(3):559–63.
Vandenplas O, Vinnikov D, Blanc PD, Agache I, Bachert C, Bewick M, et al. Impact of rhinitis on work productivity: a systematic review. J Allergy Clin Immunol Pract. 2017;6:1274–86.
Munoz-Cano R, Ribo P, Araujo G, Giralt E, Sanchez-Lopez J, Valero A. Severity of allergic rhinitis impacts sleep and anxiety: results from a large Spanish cohort. Clin Transl Allergy. 2018;8:23.
Svanes C, Sunyer J, Plana E, Dharmage S, Heinrich J, Jarvis D, et al. Early life origins of chronic obstructive pulmonary disease. Thorax. 2010;65(1):14–20.
Perret JL, Dharmage SC, Matheson MC, Johns DP, Gurrin LC, Burgess JA, et al. The interplay between the effects of lifetime asthma, smoking, and atopy on fixed airflow obstruction in middle age. Am J Respir Crit Care Med. 2013;187(1):42–8.
To T, Zhu J, Larsen K, Simatovic J, Feldman L, Ryckman K, et al. Progression from asthma to chronic obstructive pulmonary disease. Is air pollution a risk factor? Am J Respir Crit Care Med. 2016;194(4):429–38.
Samolinski B, Fronczak A, Wlodarczyk A, Bousquet J. Council of the European Union conclusions on chronic respiratory diseases in children. Lancet. 2012;379(9822):e45–6.
Samolinski B, Fronczak A, Kuna P, Akdis CA, Anto JM, Bialoszewski AZ, et al. Prevention and control of childhood asthma and allergy in the EU from the public health point of view: Polish Presidency of the European Union. Allergy. 2012;67:726–31.
Council conclusions on Healthy Ageing across the Lifecycle. 3206th Employment, social policy, ehalth and consumer affairs Council meeting. Brussels, 7 December 2012. 2012. http://www.consilium.europa.eu/uedocs/cms_data/docs/pressdata/en/lsa/134097.pdf. Accessed 7 Jan 2019.
Bousquet J, Tanasescu C, Camuzat T, Anto J, Blasi F, Neou A, et al. Impact of early diagnosis and control of chronic respiratory diseases on active and healthy ageing. A debate at the European Union Parliament. Allergy. 2013;68(5):555–61.
Muraro A, Fokkens WJ, Pietikainen S, Borrelli D, Agache I, Bousquet J, et al. European symposium on precision medicine in allergy and airways diseases: report of the European Union Parliament Symposium (October 14, 2015). Allergy. 2016;71(5):583–7.
Hellings PW, Borrelli D, Pietikainen S, Agache I, Akdis C, Bachert C, et al. European summit on the prevention and self-management of chronic respiratory diseases: report of the European Union Parliament Summit (29 March 2017). Clin Transl Allergy. 2017;7:49.
Bousquet J, Anto JM, Sterk PJ, Adcock IM, Chung KF, Roca J, et al. Systems medicine and integrated care to combat chronic noncommunicable diseases. Genome Med. 2011;3(7):43.
Peters MJ. E-cigarettes and airways’ disease: behind the smokescreen. Respirology. 2018;23(1):14–5.
Yanbaeva DG, Dentener MA, Creutzberg EC, Wesseling G, Wouters EF. Systemic effects of smoking. Chest. 2007;131(5):1557–66.
Petersen AM, Pedersen BK. The anti-inflammatory effect of exercise. J Appl Physiol. 2005;98(4):1154–62.
Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet. 2017;389(10082):1907–18.
Hansel NN, McCormack MC, Kim V. The effects of air pollution and temperature on COPD. COPD. 2016;13(3):372–9.
Sheehan WJ, Gaffin JM, Peden DB, Bush RK, Phipatanakul W. Advances in environmental and occupational disorders in 2016. J Allergy Clin Immunol. 2017;140(6):1683–92.
Peden DB. Impact of pollution on allergy/immunology. J Allergy Clin Immunol. 2018;141(3):878–9.
Ruokolainen L, Fyhrquist N, Haahtela T. The rich and the poor: environmental biodiversity protecting from allergy. Curr Opin Allergy Clin Immunol. 2016;16:421–6.
Schiavoni G, D’Amato G, Afferni C. The dangerous liaison between pollens and pollution in respiratory allergy. Ann Allergy Asthma Immunol. 2017;118(3):269–75.
Barker DJ, Bull AR, Osmond C, Simmonds SJ. Fetal and placental size and risk of hypertension in adult life. BMJ. 1990;301(6746):259–62.
Krauss-Etschmann S, Bush A, Bellusci S, Brusselle GG, Dahlen SE, Dehmel S, et al. Of flies, mice and men: a systematic approach to understanding the early life origins of chronic lung disease. Thorax. 2013;68(4):380–4.
Bousquet J, Tanasescu C, Camuzat T, Anto J, Blasi F, Neou A, et al. Impact of early diagnosis and control of chronic respriatory diseases on active and healthy ageing. A debate at the European Union Parliament. Allergy. 2013;68:555–61.
Bousquet J, Anto JM, Berkouk K, Gergen P, Antunes JP, Auge P, et al. Developmental determinants in non-communicable chronic diseases and ageing. Thorax. 2015;70(6):595–7.
Consultation on the pilot European Innovation Partnership on Active and Healthy Ageing. 2011. http://ec.europa.eu/information_society/activities/einclusion/deployment/ahaip/consultation/index_en.htm. Accessed 7 Jan 2019.
Hopkinson NS, Hart N, Jenkins G, Kaminski N, Rosenfeld M, Smyth A, et al. Climate change and lung health: the challenge for a new president. Thorax. 2017;72(4):295–6.
D’Amato G, Vitale C, Lanza M, Molino A, D’Amato M. Climate change, air pollution, and allergic respiratory diseases: an update. Curr Opin Allergy Clin Immunol. 2016;16(5):434–40.
Witt C, Schubert AJ, Jehn M, Holzgreve A, Liebers U, Endlicher W, et al. The effects of climate change on patients with chronic lung disease. A systematic literature Review. Dtsch Arztebl Int. 2015;112(51-52):878–83.
Gerardi DA, Kellerman RA. Climate change and respiratory health. J Occup Environ Med. 2014;56(Suppl 10):S49–54.
Erickson LE. Reducing greenhouse gas emissions and improving air quality: two global challenges. Environ Prog Sustain Energy. 2017;36(4):982–8.
Bousquet J, Hellings PW, Agache I, Amat F, Annesi-Maesano I, Ansotegui IJ, et al. ARIA Phase 4 (2018): change management in allergic rhinitis and asthma multimorbidity using mobile technology. J Allergy Clin Immunol. 2018. https://doi.org/10.1016/j.jaci.2018.08.049.
Bachert C, Bousquet J, Hellings P. Rapid onset of action and reduced nasal hyperreactivity: new targets in allergic rhinitis management. Clin Transl Allergy. 2018;8:25.
Bateman ED, Reddel HK, O’Byrne PM, Barnes PJ, Zhong N, Keen C, et al. As-needed budesonide-formoterol versus maintenance budesonide in mild asthma. N Engl J Med. 2018;378(20):1877–87.
Souza-Machado C, Souza-Machado A, Franco R, Ponte EV, Barreto ML, Rodrigues LC, et al. Rapid reduction in hospitalisations after an intervention to manage severe asthma. Eur Respir J. 2010;35(3):515–21.
Management of chronic obstructive pulmonary disease in adults in primary and secondary care (partial update). This guideline partially updates and replaces NICE clinical guideline 12. Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions. National Institute for Health and Clinical Excellence, NSH, UK. 2010. http://guidance.nice.org.uk/CG101. Accessed 7 Jan 2019.
Zorgstandaard for COP, Asthma in adults and asthma in children. 2012. http://www.longalliantie.nl/files/5113/7994/2952/LAN_Zorgstandaard_COPD-2013-juni.pdf, http://www.longalliantie.nl/files/4113/7335/4473/Zorgstandaard_Astma_Volwassenen.pdf, http://www.longalliantie.nl/files/9513/7335/4440/Zorgstandaard_Astma_Kinderen_en_Jongeren.pdf. Accessed 7 Jan 2019.
Asthma. Quality standards, QS25, February 2013 NICE. 2013. http://guidance.nice.org.uk/QS25. Accessed 7 Jan 2019.
QOF clinical indicators 2013/14: summary tables. 2013. http://www.eguidelines.co.uk/eguidelinesmain/external_guidelines/. Accessed 7 Jan 2019.
Haahtela T, Tuomisto LE, Pietinalho A, Klaukka T, Erhola M, Kaila M, et al. A 10 year asthma programme in Finland: major change for the better. Thorax. 2006;61(8):663–70.
Haahtela T, Valovirta E, Kauppi P, Tommila E, Saarinen K, von Hertzen L, et al. The Finnish Allergy Programme 2008–2018—scientific rationale and practical implementation. Asia Pac Allergy. 2012;2(4):275–9.
Haahtela T, von Hertzen L, Makela M, Hannuksela M. Finnish Allergy Programme 2008–2018—time to act and change the course. Allergy. 2008;63(6):634–45.
Haahtela T, Valovirta E, Bousquet J, Makela M, and the Allergy Programme Steering G. The Finnish Allergy Programme 2008–2018 works. Eur Respir J. 2017;49(6).
Selroos O, Kupczyk M, Kuna P, Lacwik P, Bousquet J, Brennan D, et al. National and regional asthma programmes in Europe. Eur Respir Rev. 2015;24(137):474–83.
Bousquet J, Dahl R, Khaltaev N. Global alliance against chronic respiratory diseases. Allergy. 2007;62(3):216–23.
Lodrup Carlsen KC, Haahtela T, Carlsen KH, Smith A, Bjerke M, Wickman M, et al. Integrated allergy and asthma prevention and care: report of the MeDALL/AIRWAYS ICPs meeting at the Ministry of Health and Care Services, Oslo, Norway. Int Arch Allergy Immunol. 2015;167(1):57–64.
Haahtela T, Herse F, Karjalainen J, Klaukka T, Linna M, Leskela RL, et al. The Finnish experience to save asthma costs by improving care in 1987–2013. J Allergy Clin Immunol. 2017;139(2):408–14.
Haahtela T, Valovirta E, Hannuksela M, Von Hertzen L, Jantunen J, Kauppi P, et al. Kansallinen allergiaohjelma 2008–2018 puolivälissä—suunnanmuutos tuo tuloksia. Suom Lääkäril. 2015;35(2):2165–72.
Kinnula VL, Vasankari T, Kontula E, Sovijarvi A, Saynajakangas O, Pietinalho A. The 10-year COPD Programme in Finland: effects on quality of diagnosis, smoking, prevalence, hospital admissions and mortality. Prim Care Respir J. 2011;20(2):178–83.
Campbell H, Hotchkiss R, Bradshaw N, Porteous M. Integrated care pathways. BMJ. 1998;316(7125):133–7.
Overill S. A practical guide to care pathways. J Integr Care. 1998;2:93–8.
Cingi C, Gevaert P, Mosges R, Rondon C, Hox V, Rudenko M, et al. Multi-morbidities of allergic rhinitis in adults: European Academy of Allergy and Clinical Immunology Task Force Report. Clin Transl Allergy. 2017;7:17.
De Greve G, Hellings PW, Fokkens WJ, Pugin B, Steelant B, Seys SF. Endotype-driven treatment in chronic upper airway diseases. Clin Transl Allergy. 2017;7:22.
Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63(Suppl 86):8–160.
Bosnic-Anticevich S, Costa E, Menditto E, Lourenço O, Novellino E, Bialek S, et al. Aria pharmacy 2018 “Allergic rhinitis care pathways for community pharmacy”. Allergy. 2018. https://doi.org/10.1111/all.13701.
Bousquet J, Neukirch F, Bousquet PJ, Gehano P, Klossek JM, Le Gal M, et al. Severity and impairment of allergic rhinitis in patients consulting in primary care. J Allergy Clin Immunol. 2006;117(1):158–62.
Bousquet J, Annesi-Maesano I, Carat F, Leger D, Rugina M, Pribil C, et al. Characteristics of intermittent and persistent allergic rhinitis: DREAMS study group. Clin Exp Allergy. 2005;35(6):728–32.
Bousquet PJ, Devillier P, Tadmouri A, Mesbah K, Demoly P, Bousquet J. Clinical relevance of cluster analysis in phenotyping allergic rhinitis in a real-life study. Int Arch Allergy Immunol. 2015;166(3):231–40.
del Cuvillo A, Montoro J, Bartra J, Valero A, Ferrer M, Jauregui I, et al. Validation of ARIA duration and severity classifications in Spanish allergic rhinitis patients—the ADRIAL cohort study. Rhinology. 2010;48(2):201–5.
Jauregui I, Davila I, Sastre J, Bartra J, del Cuvillo A, Ferrer M, et al. Validation of ARIA (allergic rhinitis and its impact on asthma) classification in a pediatric population: the PEDRIAL study. Pediatr Allergy Immunol. 2011;22(4):388–92.
Brozek JL, Bousquet J, Baena-Cagnani CE, Bonini S, Canonica GW, Casale TB, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126(3):466–76.
Dykewicz MS, Wallace DV, Baroody F, Bernstein J, Craig T, Finegold I, et al. Treatment of seasonal allergic rhinitis: an evidence-based focused 2017 guideline update. Ann Allergy Asthma Immunol. 2017;119(6):489–511.
Brozek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines—2016 revision. J Allergy Clin Immunol. 2017;140(4):950–8.
Bousquet J, Arnavielhe S, Bedbrook A, Alexis-Alexandre G, van Eerd M, Murray R, et al. Treatment of allergic rhinitis using mobile technology with real world data: The MASK observational pilot study. Allergy. 2018;73(9):1763–74.
Russell S, Ogunbayo OJ, Newham JJ, Heslop-Marshall K, Netts P, Hanratty B, et al. Qualitative systematic review of barriers and facilitators to self-management of chronic obstructive pulmonary disease: views of patients and healthcare professionals. NPJ Prim Care Respir Med. 2018;28(1):2.
Kessler R, Casan-Clara P, Koehler D, Tognella S, Viejo JL, Dal Negro RW, et al. COMET: a multicomponent home-based disease-management programme versus routine care in severe COPD. Eur Respir J. 2018;51(1):1701612.
Murphy LA, Harrington P, Taylor SJ, Teljeur C, Smith SM, Pinnock H, et al. Clinical-effectiveness of self-management interventions in chronic obstructive pulmonary disease: an overview of reviews. Chron Respir Dis. 2017;14(3):276–88.
Chronic asthma: management. London: National Institute for Health and Care Excellence (UK); 2017. November 2017.
Barry MJ, Edgman-Levitan S. Shared decision making—pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–1.
Florin J, Ehrenberg A, Ehnfors M. Clinical decision-making: predictors of patient participation in nursing care. J Clin Nurs. 2008;17(21):2935–44.
Buchanan A. Medical paternalism. Philos Public Aff. 1978;7(4):370–90.
mHealth. New horizons for health through mobile technologies. Global Observatory for eHealth series—Vol 3 WHO Library Cataloguing-in-Publication Data. 2011. http://www.who.int/goe/publications/goe_mhealth_web.pdf. Accessed 7 Jan 2019.
Stephani V, Opoku D, Quentin W. A systematic review of randomized controlled trials of mHealth interventions against non-communicable diseases in developing countries. BMC Public Health. 2016;16:572.
Bousquet J, Chavannes NH, Guldemond N, Haahtela T, Hellings PW, Sheikh A. Realising the potential of mHealth to improve asthma and allergy care: how to shape the future. Eur Respir J. 2017;49(5):1700447.
Mozaffar H, Cresswell KM, Williams R, Bates DW, Sheikh A. Exploring the roots of unintended safety threats associated with the introduction of hospital ePrescribing systems and candidate avoidance and/or mitigation strategies: a qualitative study. BMJ Qual Saf. 2017.
Bousquet J, Arnavielhe S, Bedbrook A, Bewick M, Laune D, Mathieu-Dupas E, et al. MASK 2017: ARIA digitally-enabled, integrated, person-centred care for rhinitis and asthma multimorbidity using real-world-evidence. Clin Transl Allergy. 2018;8:45.
Honkoop PJ, Simpson A, Bonini M, Snoeck-Stroband JB, Meah S, Fan Chung K, et al. MyAirCoach: the use of home-monitoring and mHealth systems to predict deterioration in asthma control and the occurrence of asthma exacerbations; study protocol of an observational study. BMJ Open. 2017;7(1):e013935.
Bousquet J, Anto JM, Annesi-Maesano I, Dedeu T, Dupas E, Pepin JL, et al. POLLAR: impact of Air POLLution on Asthma and Rhinitis; a European Institute of Innovation and Technology Health (EIT Health) project. Clin Transl Allergy. 2018;8:36.
Authors’ contributions
AV, JB and PH wrote the paper. All authors participated in the Vilnius meeting and gave a lecture. All authors read and approved the final manuscript.
Acknowledgements
None.
Competing interests
JB reports personal fees and other from Chiesi, Cipla, Hikma, Menarini, Mundipharma, Mylan, Novartis, Sanofi-Aventis, Takeda, Teva, Uriach, other from Kyomed, outside the submitted work. Dr. Chorostowska-Wynimko reports grants, personal fees and non-financial support from Grifols, CSL Behring, Angelini, Celon Pharma, Boehringer Ingelheim, Astra Zeneca, personal fees from Kamada, Novartis, GSK, outside the submitted work. Dr. Grigg reports personal fees from GSK, Vifor Pharmaceuticals, Novarits, outside the submitted work. Dr. Haahtela reports personal fees from Mundipharma, Novartis, and Orion Pharma, outside the submitted work.
Availability of data and materials
Not applicable.
Consent for publication
All authors gave their consent for publication.
Ethics approval and consent to participate
Not applicable.
Funding
Euforea, ARIA and IPOKRaTES Lithuania Funds and EAACI.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Appendix: the Vilnius Declaration
Appendix: the Vilnius Declaration
Introduction
-
1.
The European Forum for Research and Education in Allergy and Airway Diseases (Euforea) has developed the Vilnius Declaration as a statement to improve the guided self-management of chronic respiratory diseases using mHealth and giving special consideration to the impact of air pollution and climate change.
-
2.
The Declaration was elaborated and approved during the EU Summit on chronic respiratory diseases in Vilnius, Lithuania, on 23 March 2018, and addressed to health care personnel, policy makers and, most importantly, to patients suffering from chronic respiratory diseases.
-
3.
Over 1 billion people suffer from chronic respiratory diseases such as asthma, Chronic Obstructive Pulmonary Disease (COPD), rhinitis and rhinosinusitis. Chronic respiratory diseases are major chronic diseases.
-
4.
It is the duty of the medical community and health care systems to provide patients with tools to assist them with the most appropriate treatment and self-management of their condition.
Chronic respiratory diseases are major chronic diseases across the life cycle and are affected by environmental risk factors
-
5.
Chronic respiratory diseases and other chronic diseases often share environmental risk factors (e.g. tobacco use, including e-cigarettes, nutrition, indoor and outdoor air pollution and sedentary lifestyle), leading to sustained local and systemic inflammation as well as impaired ageing.
-
6.
Asthma and allergic diseases occur along the life cycle from early childhood, affecting 30 million children and adults under 45 years of age in Europe and more than 600 million people globally. COPD is responsible for an estimated 3 million deaths globally.
-
7.
Pre-natal and early-life events have a major impact on the development of chronic diseases in adults and older people. Early impairment of lung function is a marker of early all-cause systemic morbidity and mortality.
-
8.
Smoking is the most important risk factor for chronic respiratory diseases. Indoor and outdoor air pollution are other important risk factors of increasing importance. Allergens are of importance in rhinitis and asthma. Moreover, these risk factors can interact to worsen chronic respiratory diseases and induce exacerbations.
Prevention, control and self-management of chronic respiratory diseases
-
9.
Chronic disease prevention and control could be considered sequentially before the disease has been identified (i) to prevent its onset (health promotion and primary prevention), and (ii) after its onset, to better control and prevent its short- and long-term consequences (secondary and tertiary prevention and control).
-
10.
Tobacco smoking is the best identified risk factor for many chronic diseases including chronic respiratory diseases.
-
11.
Health promotion and prevention should start at conception and be steadily continued across the life cycle for healthy lungs and active and healthy ageing.
-
12.
A large number of chronic respiratory disease patients do not consult physicians because they think their symptoms are trivial. However, chronic respiratory diseases, including rhinitis and asthma, negatively impact social life, school and work productivity.
-
13.
Many rhinitis patients use over-the-counter (OTC) drugs and only a fraction have had a medical consultation. The vast majority of patients who visit general practitioners or specialists have moderate/severe rhinitis.
-
14.
Thus, Integrated Care Pathways should consider a multi-disciplinary approach including physicians, pharmacists and other health care personnel as proposed by AIRWAYS ICPs. Self-medication and shared decision making should be used as well as new-generation guidelines including messaging for increased adherence and information on aerobiology and air pollution.
-
15.
Chronic respiratory diseases require a long-term approach with emphasis on patient empowerment and appropriate support services stressing the importance of health literacy.
-
16.
Self-care is any necessary human regulatory function which is under individual control, deliberate and self-initiated.
-
17.
In shared decision making, both the patient and the physician contribute to the medical decision-making process, placing the patient at the centre of the decision. Physicians explain treatments and alternatives to patients who can then choose the treatment option that best aligns with personal beliefs and goals and consider the benefits and risks.
-
18.
The potential for mHealth in chronic respiratory diseases is enormous but implementing Information and Communication Technology (ICT) innovations may also have adverse consequences. It is therefore important to test applicability in each individual situation.
-
19.
Mobile Applications (Apps) may be used to better understand and improve adherence, in particular using messaging.
Health system strengthening and Sustainable Development Goals (SDG)
The Vilnius Declaration aims to contribute to the following actions:
-
20.
To propose a common framework for integrated care pathways in chronic respiratory diseases (and their co-morbidities) for the entire EU which can be expanded to Eastern European and other regions and which will allow comparability and trans-national initiatives.
-
21.
To extend the Finnish experience of population management models of long-term state chronic respiratory disease control programmes, especially in low to middle income countries.
-
22.
To help risk stratification in chronic respiratory disease patients with a common strategy.
-
23.
To develop cost-effective policies, in particular strengthening those on the reduction of smoking, including e-cigarettes, and environmental exposure.
-
24.
To propose a common simulation tool for the entire EU to assist physicians in the segmentation of patients and choice of pathways.
-
25.
To develop interoperability of mHealth systems in Europe, including transborder interoperability in Eastern European regions (border between EU member states and associate EU countries).
-
26.
To have a significant implication on the health of citizens in the short term (reduction of morbidity, improvement of education in children and of work in adults) and in the long term (healthy ageing).
-
27.
To achieve the goals of the Europe 2020 strategy of healthy and active ageing and of the UN Sustainable Development Goals to be reached in 2030.
European Forum for Research and Education in Allergy and Airway Diseases (Euforea) Ministry of Health of Lithuania Ministry of Health of Ukraine Ministry of Labour, Health and Social Affairs of Georgia Ministry of Health, Labour and Social Protection of Republic of Moldova Allergic Rhinitis and its Impact on Asthma (ARIA) Committee of Health of Lithuanian Seimas (Parliament) European Academy of Allergy and Clinical Immunology (EAACI) European Academy of Paediatrics (EAP/UEMS-SP) European Association of Allergy and Asthma Patients’ Associations (EFA) European Respiratory Society (ERS) European Rhinology Society (ERS) Lithuanian Academy of Sciences Reference Site Network of the European Innovation Partnership on Active and Healthy Ageing (RSCN-EIP on AHA) Vilnius University Medical Faculty Global Alliance Against Chronic Respiratory Diseases (GARD, WHO Alliance) World Health Organization (WHO) Lithuanian Office |
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Valiulis, A., Bousquet, J., Veryga, A. et al. Vilnius Declaration on chronic respiratory diseases: multisectoral care pathways embedding guided self-management, mHealth and air pollution in chronic respiratory diseases. Clin Transl Allergy 9, 7 (2019). https://doi.org/10.1186/s13601-019-0242-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13601-019-0242-2