
Abstract
Background
Despite significant progress in drug treatment, the prognosis of patients with advanced pulmonary arterial hypertension (PAH) remains extremely poor. Many preclinical studies have reported the efficacy of stem cell (SC) therapy for PAH; however, this approach remains controversial. The aim of this systematic review and meta-analysis is to assess the potential efficacy of SC therapy for PAH.
Methods
The Medline, EMBASE, Cochrane Library, and Web of Science databases were searched from inception to August 12, 2018. Preclinical studies that evaluated the use of SC therapy for PAH were included. The primary outcome was pulmonary haemodynamics, as assessed by measurement of the right ventricular systolic pressure (RVSP), mean pulmonary arterial pressure (mPAP), and/or mean right ventricle pressure (mRVP). The secondary outcomes included the weight ratio of the right ventricle to the left ventricle plus septum (RV/LV+S), the right ventricle to body weight ratio (RV/BW), the percentage of pulmonary arteriole area index (WA), and/or the percentage of medial wall thickness of the pulmonary arteriole (WT). The quality of outcomes was evaluated using the SYstematic Review Centre for Laboratory animal Experimentation (SYRCLE) bias risk tool. The inverse-variance method with random-effects modelling was used to calculate pooled weighted mean differences (WMDs) and 95% CIs. Statistical analysis was performed with STATA 14.0.
Results
Twenty-eight eligible articles (722 animals) were included. SC therapy reduced the pooled WMDs (95% CIs) of RVSP, mPAP, mRVP, RV/LV+S, RV/BW, WA, and WT for animals with PAH, with values of − 14.12 (− 14.63, − 13.61), − 11.86 (− 12.35, − 11.36), − 17.33 (− 18.10, − 16.56), − 0.10 (− 0.10, − 0.09), 0.23 (0.21, 0.24), − 13.66 (− 15.71, − 11.62), and − 7.96 (− 7.99, − 7.93), respectively.
Conclusions
SC therapy is effective for PAH in preclinical studies. These results may help to standardise preclinical animal studies and provide a theoretical basis for clinical trial design in the future.
Systematic review registration
PROSPERO (http://www.crd.york.ac.uk/PROSPERO).
Similar content being viewed by others

Background
Pulmonary arterial hypertension (PAH) is a progressive chronic disease with a high mortality rate [1], and the median survival of patients with idiopathic PAH was estimated to be 2.8 years [2]. This disease is characterised by progressively increasing PAH and vascular remodelling [3], which ultimately leads to right heart failure and death [4]. The pulmonary vasculature is also remodelled, with increased pulmonary vascular resistance and over-proliferation of pulmonary artery endothelial cells [5, 6]. In recent decades, the treatment of PAH has progressed significantly, as a deeper understanding of the underlying pathogenesis has been achieved [7,8,9,10,11,12]. However, the mortality of PAH remains high [12, 13]. Therefore, there is a considerable unmet medical need in the management of PAH.
Recently, cell-based gene therapies have attracted increasing interest due to their beneficial roles in ameliorating the progression of PAH [14,15,16]. Stem cells (SCs) are multipotent progenitor cells, and mesenchymal SCs are the preferred seed cells for cell-based therapy because of their strong expansion ability in culture, their reproducible potential, and their capacity to differentiate into bone, cartilage, muscle, or vascular smooth muscle cells, as well as other connective tissues [17,18,19]. The ultimate goal of SC therapy is to inhibit pulmonary vascular remodelling and excessive cell proliferation, slowing the development of pulmonary hypertension and the occurrence of right heart failure to achieve clinical improvement of cardiopulmonary function without severe adverse effects.
Many animal studies of PAH have been reported, with heterogeneous designs and conflicting outcomes. Nevertheless, preclinical studies are needed to assess the risk of new therapies and to predict safety, feasibility, and efficacy. Moreover, such studies can offer guidance concerning unresolved issues related to clinical cell therapy (i.e., the choice of cell type and dose, the route and timing of delivery, and follow-up after cell transplantation). Thus, we performed a systematic review of the pertinent literature, including a quantitative meta-analytical pooling of the data, to assess the effects of SC therapy on animals with PAH.
Methods
The author declares that all supporting data are available within this article and its online supplementary files. The study protocol is registered through PROSPERO (http://www.crd.york.ac.uk/PROSPERO), and the registration number is CRD42018103854, which can be found online at https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=103854.
Data sources and search strategies
This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria [20]. The PRISMA 2009 checklist is shown in Additional file 11: Table S1. A systematic literature search was conducted for animal studies on SC therapy and PAH that were published until 12 August 2018, using the Medline (www.ncbi.nlm.nih.gov/pubmed), EMBASE (www.embase.com), Cochrane Library (www.cochranelibrary.com), and Web of Science (http://apps.webofknowledge.com/WOS_GeneralSearch_input.do?) databases. The detailed search strategy is shown in Additional file 12: Table S2. The search was limited to English. We also hand-searched the references of the included articles. Literature searches were performed independently by Huo-Yan Liang and Bo Yuan.
Eligibility criteria
Studies were considered suitable for inclusion in this meta-analysis if (1) all PAH animal models were subjected to SC treatment (all species and sexes), (2) saline-treated PAH animal models were used as controls, and (3) the studies included data on one or more outcomes, such as right ventricular systolic pressure (RVSP), mean pulmonary arterial pressure (mPAP), mean right ventricle pressure (mRVP), the weight ratio of the right ventricle to the left ventricle plus septum (RV/LV+S), the right ventricle to body weight ratio (RV/BW), the pulmonary arteriole area index (WA), and the wall thickness of the pulmonary arteriole (WT). The exclusion criteria were as follows: (1) all inclusion criteria were not fulfilled, (2) the animals had comorbidities, (3) the animal models did not have PAH, (4) animal models with PAH did not receive SC treatment, (5) the study was a case study, a crossover study, or a study without a separate control group, (6) the study was a duplicate report, or (7) weighted mean differences (WMDs) with 95% CIs were not provided or could not be calculated.
Study selection and data extraction
The titles and/or abstracts of studies retrieved using the search strategy and studies from additional sources were screened independently by Huo-Yan Liang and Bo Yuan to identify studies that potentially met the inclusion criteria outlined above. Key data interpretation was conducted independently by Li-Feng Li and Tian Wang. Any differences were resolved through discussions with Quan-Cheng Kan and Le-Xin Wang. The extracted information was as follows: author (year of publication), animal characteristics (species, gender, sample size, and model), intervention characteristics (source, dosage, route, and timing of SC therapy), follow-up (observation time of outcomes after SC administration), and measures relevant to our primary and secondary outcomes.
Assessment of risk of bias
The risk of bias of eligible studies was assessed using the SYstematic Review Centre for Laboratory animal Experimentation (SYRCLE) bias risk tool [21]. The SYRCLE tool was adapted from the Cochrane Risk of Bias Tool to assess methodological quality using criteria specific to animal studies. The items in this tool include assessments for selection bias (sequence generation, baseline characteristics, and allocation concealment), performance bias (random housing and blinding), detection bias (random outcome assessment and blinded outcome assessment), attrition bias (completeness of outcome data), and reporting bias. For each included study, results of no, yes, and unclear risk of bias were scored as high, low, and unclear risk of bias, respectively.
Primary and secondary outcomes
The current gold standard for the diagnosis and evaluation of clinical PAH is direct pulmonary haemodynamic measures, as assessed by measurement of RVSP, mPAP, and mRVP through right heart catheterization. RV remodelling is a precursor of right heart failure and is characterised by decreased function and dilatation of the RV, and this change is strongly correlated with prognosis and survival in PAH patients [22]. We collected morphometric data on RV remodelling expressed as the RV/LV+S and RV/BW. In addition, we also collected data from other non-invasive measures obtained by echocardiography to evaluate cardiac structure and pulmonary haemodynamics, such as WA and WT. In this meta-analysis, the primary outcomes included RVSP, mPAP, and mRVP after SC administration. Secondary outcomes included RV/LV+S, RV/BW, WA, and WT.
Statistical analysis
The estimated effect sizes of primary and secondary outcomes were determined by WMDs and 95% CIs. WMDs, an ideal measure for continuous data, were calculated by the mean (M), standard deviation (SD), and sample number (N) in each study. The pooled WMD of each study was conducted using a fixed-effects model (inverse-variance) or a random-effects model (I-V heterogeneity) to generate forest plots. In addition, the Q test and I2 test were used to measure heterogeneity, which was not considered significant if P > 0.1 or I2 < 50%. Potential sources of heterogeneity, if significant, were further investigated by stratified analysis and meta-regression. Begg’s funnel plot [23] and Egger’s linear regression [24] were used to assess potential publication bias. Funnel plots were visually assessed for asymmetry. For Egger’s tests, P < 0.1 was considered significant to confirm the presence of a small study size. All analyses were performed using Stata 14.0 statistical software (Stata Corp LP, College Station, Texas 77,845, USA, serial number: 401406267051). Differences for which P < 0.05 (two-sided) were considered statistically significant.
Results
Study selection
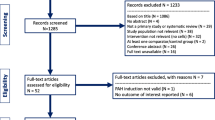
Using our search strategy, we initially identified 1342 records, and 1190 articles remained after duplicates were removed. After preliminary screening by title and abstract, 112 articles reporting the therapeutic potential of SCs for PAH were isolated for full-text review. However, 28 articles [14, 15, 25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50] enrolling 722 animals were ultimately included in this meta-analysis after study selection (Fig. 1).

Flow diagram of study selection
Study characteristics
The number of included articles reporting RVSP, mPAP, mRVP, RV/LV+S, RV/BW, WA, and WT was16 [14, 26, 28,29,30,31,32,33, 39, 40, 42, 45, 48,49,50], 12 [25, 30, 38, 41, 44, 47, 50], 14 [27, 34,35,36,37, 42, 50], 29 [25,26,27, 29,30,31, 33,34,35,36, 39,40,41, 43,44,45, 47, 48, 50], 16 [14, 29, 34,35,36,37, 42, 48, 50], 5 [27, 43, 44], and 23 [26, 27, 32,33,34,35,36,37, 40, 42,43,44, 49, 50], respectively. The animal model used in most studies was induced by surgical operation or by 40–60 mg/kg monocrotaline (MCT) administered intraperitoneally, subcutaneously, or via tail vein injection. The majority of the animals were male, 6-week-old, Sprague Dawley rats, and weighed 180–220 g. Regarding the intervention characteristics of the SCs, they mostly originated from human or rat bone marrow, adipose-derived mesenchymal tissue, or human umbilical cord blood-derived mesenchymal tissue. The doses of the interventions ranged from 105 to 107 SCs, which were injected intravenously, intratracheally, or intraperitoneally at least 3 days after induction of the PAH model. The observation time of the primary and secondary outcomes after SC administration was at least 1 week. In addition, several articles contained more than one study [34,35,36,37,38, 44]. The main characteristics of the 28 articles involved in this meta-analysis are shown in Tables 1 and 2.
Risk of bias
All 28 articles that met the inclusion criteria for this meta-analysis were included (Table 3). None of the experiments were judged as having a low risk of bias across all domains. All studies reported similar experimental and control groups at baseline, which reduced the risk of selection bias based on animal characteristics. Although the assignment of subjects to the experimental and control groups was random, none of the studies clearly described the method of random sequence generation. For this reason, the risk of bias in the sequence generation domain was judged as “unclear” in all studies. However, although none of the studies adequately described the method used to conceal allocation, the animals were randomly housed, the caregivers and investigators were blinded to the intervention each animal received, random outcome assessment was reported, and blinding of the outcome assessor was documented. Using the signalling questions provided, all studies were scored as having a low risk of attrition and reporting bias. Furthermore, we did not identify any additional sources of bias that were not already covered by the SYRCLE Risk of Bias tool.
Effect of SC therapy on PAH
The results of the primary outcomes in this meta-analysis are shown in Figs. 2, 3 and 4. The pooled WMDs (95% CIs) for RVSP, mPAP, and mRVP were 14.12 (− 14.63, − 13.61), − 11.86 (− 12.35, − 11.36), and − 17.33 (− 18.10, − 16.56), and the P values were all < 0.001, which indicated that compared to vehicle treatment, SC therapy was significantly associated with reduced RVSP, mPAP, and mRVP values in the animal model of PAH. A random-effects model was used to perform this meta-analysis, as there was significant heterogeneity (I2 = 94.0%, 90.1%, and 93.4%, respectively) among the studies.

Meta-analysis of overall pooled WMDs with 95% CIs across studies for primary outcomes in PAH. Forest plot showing that SC therapy significantly reduced the RVSP in animals with PAH from a random-effects model. Abbreviations: WMD, weighted mean difference; RVSP, right ventricular systolic pressure; PAH, pulmonary arterial hypertension

Meta-analysis of overall pooled WMDs with 95% CIs across studies for primary outcomes in PAH. Forest plot showing that SC therapy significantly reduced the mPAP in animals with PAH from a random-effects model. Abbreviations: WMD, weighted mean difference; mPAP, mean pulmonary arterial pressure; PAH, pulmonary arterial hypertension

Meta-analysis of overall pooled WMDs with 95% CIs across studies for primary outcomes in PAH. Forest plot showing that SC therapy significantly reduced the mRVP in animals with PAH from a random-effects model. Abbreviations: WMD, weighted mean difference; mRVP, mean right ventricle pressure; PAH, pulmonary arterial hypertension
The results of secondary outcomes in this meta-analysis are shown in Additional file 1: Figure S1, Additional file 2: Figure S2, Additional file 3: Figure S3, and Additional file 4: Figure S4. The pooled WMDs (95% CIs) for RV/LV+S, RV/BW, WA, and WT were 0.10 (− 0.10, − 0.09), 0.23 (0.21, 0.24), − 13.66 (− 15.71, − 11.62), and − 7.96 (− 7.99, − 7.93), respectively, and the P values were all < 0.001, which indicated that compared to vehicle treatment, SC therapy was also significantly associated with reduced RV/LV+S, RV/BW, WA, and WT values in the animal model of PAH. A random-effects model was also used to perform this meta-analysis, as there was moderate or significant heterogeneity (I2 = 93.2%, 99.8%, 67.9%, and 97.5%, respectively) among the studies. In summary, based on the results of forest plots of the primary and secondary outcomes, we concluded that SC therapy is effective for PAH in animal studies.
Stratified analysis and meta-regression analysis
Stratified analysis was conducted on the primary outcomes according to source, route, dose, and timing of SC treatment after PAH and follow-up. However, we could not find the source of heterogeneity. To further investigate the unexplained heterogeneity across these studies, meta-regression was performed to simultaneously examine the impact of all variables on the study effect. However, for RVSP, no significant sources of heterogeneity were found. For mPAP, the method of establishing the PAH model and the dose of MCT were the sources of heterogeneity (P = 0.046). For mRVP, the follow-up time was the significant source of heterogeneity (P = 0.007).
Publication bias
Funnel plots and Egger’s linear regression tests were performed to evaluate publication bias in RVSP, mPAP, mRVP, RV/LV+S, RV/BW, and WT individually (Additional file 5: Figure S5, Additional file 6: Figure S6, Additional file 7: Figure S7, Additional file 8: Figure S8, Additional file 9: Figure S9, and Additional file 10: Figure S10). As the number of included studies that measured WA was small (< 10), we did not construct a funnel plot, as it may not have detected publication bias [51]. No significant publication bias was found for mPAP (Begg’s test, P = 0.244; Egger’s test, P = 0.423; Additional file 6: Figure S6), mRVP (Begg’s test, P = 0.003; Egger’s test, P = 0.335; Additional file 7: Figure S7), RV/LV+S (Begg’s test, P = 0.129; Egger’s test, P = 0.155; Additional file 8: Figure S8), RV/BW (Begg’s test, P = 0.752; Egger’s test, P = 0.186; Additional file 9: Figure S9), or WT (Begg’s test, P = 0.492; Egger’s test, P = 0.050; Additional file 10: Figure S10) in PAH. However, significant publication bias was found for RVSP (Begg’s test, P = 0.013; Egger’s test, P = 0.000; Additional file 5: Figure S5).
Discussion
Systematic reviews play a critical role in applying preclinical data to clinical practice. When combined with a meta-analysis of these experiments, the results can be assessed in a more methodical and objective manner. In preclinical studies of PAH animal models, SCs have been shown to improve pulmonary pressure, RV hypertrophy, and pulmonary artery endothelium over-proliferation [52]. Investigators using animal models of PAH have reported similarly promising results. Progress in regenerative medicine has led to the first clinical trial to evaluate the safety of autologous endothelial progenitor cells in PAH [53], but to date, SCs have not been used for clinical treatment in patients with PAH. To our knowledge, this is the first attempt to systematically collect and evaluate the current preclinical evidence supporting the use of SCs in animal models of PAH. Based on the results of this meta-analysis, we prove that SCs do indeed have potential therapeutic efficacy for reducing pulmonary artery pressure and RV remodelling in PAH animal models. Furthermore, these results are applicable across a range of experimental conditions.
SCs significantly improved PAH and RV pressure. Our results showed that SCs could ameliorate pulmonary artery resistance and inhibit the over-proliferation of pulmonary epithelial cells, which is consistent with studies that used SCs to treat adult animal models of lung diseases. For instance, a meta-analysis performed by Zhao et al. [54] found a positive effect on pulmonary artery resistance in lung disease. In our study, the mPAP results yielded a WMD of − 11.86, which is comparable to the values obtained in the majority of studies but is different from the values obtained by Guo et al. [30]. Taken together, these findings support the potential use of SC therapy in preclinical studies of PAH.
This meta-analysis suggests that further studies should be performed to elucidate the ideal MSC dose, as the outcomes for mRVP suggested doses between 0.5 × 106 and 1 × 106 SCs, while the outcomes for mPAP and RVSP showed optimal doses between1 × 106 and 3 × 106. Similarly, there was a discrepancy regarding the most effective route of delivery, with the mPAP and RVSP results favouring the sublingual vein route, while the mRVP studies favoured external jugular vein injection. These variables are exceedingly relevant to future patient applications from a clinical perspective. As such, our findings should be used to guide future preclinical or clinical trials when determining the optimal SC characteristics for successful outcomes.
In all comparisons, significant heterogeneity in treatment effects was found among studies. This heterogeneity can be expected in studies such as ours that are based on a limited number of included studies and have potential bias in study selection. Funnel plots and Egger’s test reported the outcomes of RVSP and confirmed the presence of publication bias. Study quality may also be affected if our primary outcome measure was not the focus of the preclinical study. Such variations in study design could account for the heterogeneity found in this meta-analysis.
We performed a meta-regression analysis to assess the impact of these variables and consider sources of heterogeneity. The results of this analysis suggest that the mPAP, mRVP, and RVSP outcomes were indeed associated with moderator variables in the included study. However, it is also important to consider the limitations of meta-regression. In this meta-analysis, there are relatively few studies but many possible study characteristics that could explain the heterogeneity. Without significant power, it is possible to arrive at false-positive conclusions. Meta-regression is intended to generate hypotheses regarding heterogeneity rather than fully explain heterogeneity. For this reason, it is difficult to truly ascertain the variables with the most promising effects given the current collection of studies.
The SYRCLE Risk of Bias tool highlighted notable deficiencies in reporting across all studies. None of the 28 articles included in this meta-analysis were considered to have a low risk of bias based on the reporting domains included in this tool. As discussed, domains were scored as having a low risk of bias only if the authors specifically stated these details in their published manuscripts. Therefore, it is possible that the studies utilised such methods in their studies but simply failed to report them. This meta-analysis emphasises this widespread shortcoming and suggests a need for higher reporting standards when publishing, specifically for preclinical translational studies. We suggest using a checklist such as the SYRCLE Risk of Bias tool when designing future preclinical studies to minimise internal reporting bias.
The strengths of this meta-analysis are obvious. First, this is the first meta-analysis of the effect of SCs on PAH in animal models. Second, we conducted a systematic literature search and followed a published protocol to ensure a diligent and rigorous review process. Third, data from studies including large samples were pooled in this meta-analysis, increasing its robustness. Furthermore, our primary outcomes of pulmonary artery and RV pressure are widely applicable to future preclinical and clinical trials.
In addition, this meta-analysis has several limitations. For example, the included studies are limited only to studies that have already been published. Unpublished data may exist that would alter our results. While we have made every effort to thoroughly search the current literature, it is possible that we may have missed relevant studies. Additionally, this meta-analysis is limited by relatively small data sets due to strict inclusion criteria, with external publication bias across these studies. Our study did not include studies that used microvesiclesor medium-derived SCs. Finally, we are unable to comment on the clinical safety of SC therapy, as none of the included studies thoroughly investigated SC dose-effects on PAH in animal models. While immunogenicity is less of a concern with SC therapy, other significant risks exist. For instance, SCs, especially induced pluripotent stem cells (iPSCs), have been associated with malignant transformation, tumour growth, and a higher overall degree of metastasis [55,56,57]. Therefore, iPSCs should be considered carefully for the future treatment of PAH, although none of the studies indicated that iPSCs promoted tumourigenicity in PAH. Although complications have been observed in humans receiving SCs, meta-analysis has not shown a direct correlation between SCs and acute toxicity, systemic failure, malignancy, or death [58,59,60]. Although there have been clinical trials on the safety and efficacy of SCs for acute respiratory distress syndrome and other respiratory diseases, as well as progenitor cells for pulmonary hypertension, SCs have not yet been used to treat pulmonary hypertension. Therefore, further research is needed to define the dose of SCs for standardised preclinical studies or clinical trials. Despite these limitations, our results reflect the widespread tendencies in this field of research.
Conclusions
These findings highlight the effects of SCs on pulmonary artery and RV stress and pulmonary artery and RV remodelling in animal models. Furthermore, these results may help to standardise preclinical animal studies and provide a theoretical basis for future SC clinical trial designs.
Abbreviations
- mPAP:
-
Mean pulmonary arterial pressure
- mRVP:
-
Mean right ventricle pressure
- PAH:
-
pulmonary arterial hypertension
- RV/BW:
-
Right ventricle to body weight ratio
- RV/LV+S:
-
The weight ratio of the right ventricle to the left ventricle plus septum
- RVSP:
-
Right ventricular systolic pressure
- SCs:
-
Stem cells
- SYRCLE:
-
SYstematic Review Centre for Laboratory animal Experimentation
- WA:
-
Pulmonary arteriole area index
- WMD:
-
Weighted mean difference
- WT:
-
Wall thickness of pulmonary arteriole
References
Swaminathan AC, Dusek AC, McMahon TJ. Treatment-related biomarkers in pulmonary hypertension. Am J Respir Cell Mol Biol. 2015;52(6):663–73.
D'Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115(5):343–9.
Pereira SL, Kummerle AE, Fraga CA, Barreiro EJ, Rocha Nde N, Ferraz EB, et al. A novel Ca2+ channel antagonist reverses cardiac hypertrophy and pulmonary arteriolar remodeling in experimental pulmonary hypertension. Eur J Pharmacol. 2013;702(1–3):316–22.
Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J. 2009;30(20):2493–537.
Mori H, Park IS, Yamagishi H, Nakamura M, Ishikawa S, Takigiku K, et al. Sildenafil reduces pulmonary vascular resistance in single ventricular physiology. Int J Cardiol. 2016;221:122–7.
Fukumoto Y, Shimokawa H. Recent progress in the management of pulmonary hypertension. Circulation J. 2011;75(8):1801–10.
Channick RN, Simonneau G, Sitbon O, Robbins IM, Frost A, Tapson VF, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet (London, England). 2001;358(9288):1119–23.
Olschewski H, Simonneau G, Galie N, Higenbottam T, Naeije R, Rubin LJ, et al. Inhaled iloprost for severe pulmonary hypertension. N Engl J Med. 2002;347(5):322–9.
Simonneau G, Barst RJ, Galie N, Naeije R, Rich S, Bourge RC, et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med. 2002;165(6):800–4.
Galie N, Badesch D, Oudiz R, Simonneau G, McGoon MD, Keogh AM, et al. Ambrisentan therapy for pulmonary arterial hypertension. J Am Coll Cardiol. 2005;46(3):529–35.
Galie N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, Badesch D, et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med. 2005;353(20):2148–57.
Pulido T, Adzerikho I, Channick RN, Delcroix M, Galie N, Ghofrani HA, et al. Macitentan and morbidity and mortality in pulmonary arterial hypertension. N Engl J Med. 2013;369(9):809–18.
Benza RL, Miller DP, Barst RJ, Badesch DB, Frost AE, McGoon MD. An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL registry. Chest. 2012;142(2):448–56.
Kanki-Horimoto S, Horimoto H, Mieno S, Kishida K, Watanabe F, Furuya E, et al. Implantation of mesenchymal stem cells overexpressing endothelial nitric oxide synthase improves right ventricular impairments caused by pulmonary hypertension. Circulation. 2006;114(1 Suppl):I181–5.
Takemiya K, Kai H, Yasukawa H, Tahara N, Kato S, Imaizumi T. Mesenchymal stem cell-based prostacyclin synthase gene therapy for pulmonary hypertension rats. Basic Res Cardiol. 2010;105(3):409–17.
Chai S, Wang W, Liu J, Guo H, Zhang Z, Wang C, et al. Leptin knockout attenuates hypoxia-induced pulmonary arterial hypertension by inhibiting proliferation of pulmonary arterial smooth muscle cells. Transl Res. 2015;166(6):772–82.
Wang CH, Cherng WJ, Yang NI, Kuo LT, Hsu CM, Yeh HI, et al. Late-outgrowth endothelial cells attenuate intimal hyperplasia contributed by mesenchymal stem cells after vascular injury. Arterioscler Thromb Vasc Biol. 2008;28(1):54–60.
Westerweel PE, Verhaar MC. Directing myogenic mesenchymal stem cell differentiation. Circ Res. 2008;103(6):560–1.
Minguell JJ, Allers C, Lasala GP. Mesenchymal stem cells and the treatment of conditions and diseases: the less glittering side of a conspicuous stem cell for basic research. Stem Cells Dev. 2013;22(2):193–203.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Hooijmans CR, Rovers MM, de Vries RB, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol. 2014;14:43.
Vonk-Noordegraaf A, Haddad F, Chin KM, Forfia PR, Kawut SM, Lumens J, et al. Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. J Am Coll Cardiol. 2013;62(25 Suppl):D22–33.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101.
Stuck AE, Rubenstein LZ, Wieland D. Bias in meta-analysis detected by a simple, graphical test. Asymmetry detected in funnel plot was probably due to true heterogeneity. BMJ. 1998;316(7129):469. author reply 70–1
Baber SR, Deng W, Master RG, Bunnell BA, Taylor BK, Murthy SN, et al. Intratracheal mesenchymal stem cell administration attenuates monocrotaline-induced pulmonary hypertension and endothelial dysfunction. Am J Physiol Heart Circ Physiol. 2007;292(2):H1120–8.
Chen H, Yang H, Yue H, Strappe P, Xia P, Pan L, et al. Mesenchymal stem cells expressing eNOS and a Cav1 mutant inhibit vascular smooth muscle cell proliferation in a rat model of pulmonary hypertension. Heart Lung Circ. 2017;26(5):509–18.
Chen JY, An R, Liu ZJ, Wang JJ, Chen SZ, Hong MM, et al. Therapeutic effects of mesenchymal stem cell-derived microvesicles on pulmonary arterial hypertension in rats. Acta Pharmacol Sin. 2014;35(9):1121–8.
Chen Z, Huang JH, Liu XR, Liu JF. Mesenchymal stem cells transplantation improves functions of circulating endothelial progenitor cells in a rat model of pulmonary hypertension. Int J Clin Exp Med. 2016;9(2):2057–66.
Cheng G, Wang X, Li Y, He L. Let-7a-transfected mesenchymal stem cells ameliorate monocrotaline-induced pulmonary hypertension by suppressing pulmonary artery smooth muscle cell growth through STAT3-BMPR2 signaling. Stem Cell Res Ther. 2017;8(1):34.
Guo Y, Su L, Li Y, Guo N, Xie L, Zhang D, et al. The synergistic therapeutic effect of hepatocyte growth factor and granulocyte colony-stimulating factor on pulmonary hypertension in rats. Heart Vessel. 2014;29(4):520–31.
Huang WC, Ke MW, Cheng CC, Chiou SH, Wann SR, Shu CW, et al. Therapeutic benefits of induced pluripotent stem cells in monocrotaline-induced pulmonary arterial hypertension. PLoS One. 2016;11(2):e0142476.
Jiang L, Song XH, Liu P, Zeng CL, Huang ZS, Zhu LJ, et al. Platelet-mediated mesenchymal stem cells homing to the lung reduces monocrotaline-induced rat pulmonary hypertension. Cell Transplant. 2012;21(7):1463–75.
Kang H, Kim KH, Lim J, Kim YS, Heo J, Choi J, et al. The therapeutic effects of human mesenchymal stem cells primed with sphingosine-1 phosphate on pulmonary artery hypertension. Stem Cells Dev. 2015;24(14):1658–71.
Kim KC, Lee HR, Kim SJ, Cho MS, Hong YM. Changes of gene expression after bone marrow cell transfusion in rats with monocrotaline-induced pulmonary hypertension. J Korean Med Sci. 2012;27(6):605–13.
Kim KC, Lee JC, Lee H, Cho MS, Choi SJ, Hong YM. Changes in Caspase-3, B cell leukemia/lymphoma-2, interleukin-6, tumor necrosis factor-α and vascular endothelial growth factor gene expression after human umbilical cord blood derived mesenchymal stem cells transfusion in pulmonary hypertension rat models. Korean Circulation J. 2016;46(1):79–92.
Lee H, Kim KC, Choi SJ, Hong YM. Optimal dose and timing of umbilical stem cells treatment in pulmonary arterial hypertensive rats. Yonsei Med J. 2017;58(3):570–80.
Lee H, Lee JC. The effect of umbilical cord blood derived mesenchymal stem cells in monocrotaline-induced pulmonary artery hypertension rats. J Korean Med Sci. 2015;30(5):576–85.
Liang M, Li H, Zheng S, Ning J, Xu C, Wang H, et al. Comparison of early and delayed transplantation of adipose tissue-derived mesenchymal stem cells on pulmonary arterial function in monocrotaline-induced pulmonary arterial hypertensive rats. Eur Heart J Suppl. 2015;17:F4–F12.
Lim J, Kim Y, Heo J, Kim KH, Lee S, Lee SW, et al. Priming with ceramide-1 phosphate promotes the therapeutic effect of mesenchymal stem/stromal cells on pulmonary artery hypertension. Biochem Biophys Res Commun. 2016;473(1):35–41.
Liu J, Han Z, Han Z, He Z. Mesenchymal stem cells suppress CaN/NFAT expression in the pulmonary arteries of rats with pulmonary hypertension. Exp Ther Med. 2015;10(5):1657–64.
Liu K, Liu R, Cao G, Sun H, Wang X, Wu S. Adipose-derived stromal cell autologous transplantation ameliorates pulmonary arterial hypertension induced by shunt flow in rat models. Stem Cells Dev. 2011;20(6):1001–10.
Luan Y, Zhang X, Kong F, Cheng GH, Qi TG, Zhang ZH. Mesenchymal stem cell prevention of vascular remodeling in high flow-induced pulmonary hypertension through a paracrine mechanism. Int Immunopharmacol. 2012;14(4):432–7.
Luan Y, Zhang X, Qi TG, Cheng GH, Sun C, Kong F. Long-term research of stem cells in monocrotaline-induced pulmonary arterial hypertension. Clin Exp Med. 2014;14(4):439–46.
Luo L, Lin T, Zheng S, Xie Z, Chen M, Lian G, et al. Adipose-derived stem cells attenuate pulmonary arterial hypertension and ameliorate pulmonary arterial remodeling in monocrotaline-induced pulmonary hypertensive rats. Clin Exp Hypertens. 2015;37(3):241–8.
Raoul W, Wagner-Ballon O, Saber G, Hulin A, Marcos E, Giraudier S, et al. Effects of bone marrow-derived cells on monocrotaline- and hypoxia-induced pulmonary hypertension in mice. Respir Res. 2007;8:8.
Rathinasabapathy A, Bruce E, Espejo A, Horowitz A, Sudhan DR, Nair A, et al. Therapeutic potential of adipose stem cell-derived conditioned medium against pulmonary hypertension and lung fibrosis. Br J Pharmacol. 2016;173(19):2859–79.
Somanna NK, Wörner PM, Murthy SN, Pankey EA, Schächtele DJ, Hilaire RCS, et al. Intratracheal administration of cyclooxygenase-1-transduced adipose tissue-derived stem cells ameliorates monocrotaline-induced pulmonary hypertension in rats. Am J Physiol Heart Circ Physiol. 2014;307(8):H1187–H95.
Umar S, de Visser YP, Steendijk P, Schutte CI, Laghmani el H, Wagenaar GT, et al. Allogenic stem cell therapy improves right ventricular function by improving lung pathology in rats with pulmonary hypertension. Am J Physiol Heart Circ Physiol. 2009;297(5):H1606–16.
Zhang Y, Liao S, Yang M, Liang X, Poon MW, Wong CY, et al. Improved cell survival and paracrine capacity of human embryonic stem cell-derived mesenchymal stem cells promote therapeutic potential for pulmonary arterial hypertension. Cell Transplant. 2012;21(10):2225–39.
Zhang ZH, Lu Y, Luan Y, Zhao JJ. Effect of bone marrow mesenchymal stem cells on experimental pulmonary arterial hypertension. Exp Ther Med. 2012;4(5):839–43.
Lau J, Ioannidis JP, Terrin N, Schmid CH, Olkin I. The case of the misleading funnel plot. BMJ (Clinical research ed). 2006;333(7568):597–600.
Leibacher J, Henschler R. Biodistribution, migration and homing of systemically applied mesenchymal stem/stromal cells. Stem Cell Res Ther. 2016;7:7.
Zhu JH, Wang XX, Zhang FR, Shang YP, Tao QM, Zhu JH, et al. Safety and efficacy of autologous endothelial progenitor cells transplantation in children with idiopathic pulmonary arterial hypertension: open-label pilot study. Pediatr Transplant. 2008;12(6):650–5.
Zhao R, Su Z, Wu J, Ji HL. Serious adverse events of cell therapy for respiratory diseases: a systematic review and meta-analysis. Oncotarget. 2017;8(18):30511–23.
Yagi H, Kitagawa Y. The role of mesenchymal stem cells in cancer development. Front Genet. 2013;4:261.
Ridge SM, Sullivan FJ, Glynn SA. Mesenchymal stem cells: key players in cancer progression. Mol Cancer. 2017;16(1):31.
Deng J, Zhang Y. Cell transplantation for spinal cord injury: tumorigenicity of induced pluripotent stem cell-derived neural stem/progenitor cells. Stem Cells Int. 2018;2018:5653787.
Spees JL, Lee RH, Gregory CA. Mechanisms of mesenchymal stem/stromal cell function. Stem Cell Res Ther. 2016;7(1):125.
Qiu Y, Li M-Y, Feng T, Feng R, Mao R, Chen B-L, et al. Systematic review with meta-analysis: the efficacy and safety of stem cell therapy for Crohn’s disease. Stem Cell Res Ther. 2017;8(1):136.
Yubo M, Yanyan L, Li L, Tao S, Bo L, Lin C. Clinical efficacy and safety of mesenchymal stem cell transplantation for osteoarthritis treatment: a meta-analysis. PLoS One. 2017;12(4):e0175449.
Acknowledgements
We thank the Chinese Evidence Based Medicine Center at West China Hospital of Sichuan University for providing the Stata 14.0 statistical software.
Funding
This study was supported by the Natural Science Foundation of Henan Province (Grant No. 182300410369), Science and Technology Innovation Talents in Universities of Henan Province (Grant No. 16IRTSTHN021), Scientific and Technological Innovation leaders in Central Plains (Grant No. 194200510017), Provincial Ministry Co-construction Project from Medical Scientific and Technological Research Program of Henan Province (Grant No. SBGJ2018020), the "51282" Project Leaders of Scientific and Technological Innovative Talents from Health and Family Planning Commission in Henan Province (2016-32).
Availability of data and materials
All supporting data are included in the article and its additional files.
Author information
Authors and Affiliations
Contributions
All the authors contributed extensively to the work presented in this article. TWS, XFD, and HYL conceived the study. HYL and BY performed the literature search and analysed the data. LFL and TW contributed to key data interpretation. XFD and HYL contributed to the study protocol and wrote the article. QCK and LXW resolved any differences through discussions. TWS revised the article. The corresponding author had full access to all of the data and has final responsibility for the article submitted for publication. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors consent to publication of the present manuscript.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Figure S1. Meta-analysis of overall pooled WMDs with 95% CIs across studies for secondary outcomes in PAH. Forest plot showing that SC therapy significantly reduced the RV/LV+S in animals with PAH from a random-effects model. Abbreviations: PAH, pulmonary arterial hypertension; RV/LV+S, the weight ratio of the right ventricle to the left ventricle plus septum; WMD, weighted mean difference. (TIF 1900 kb)
Additional file 2:
Figure S2. Meta-analysis of overall pooled WMDs with 95% CIs across studies for secondary outcomes in PAH. Forest plot showing that SC therapy significantly reduced the RV/BW in animals with PAH from a random-effects model. Abbreviations: PAH, pulmonary arterial hypertension; RV/BW, right ventricle to body weight ratio; WMD, weighted mean difference. (TIF 987 kb)
Additional file 3:
Figure S3. Meta-analysis of overall pooled WMDs with 95% CIs across studies for secondary outcomes in PAH. Forest plot showing that SC therapy significantly reduced the WA in animals with PAH from a random-effects model. Abbreviations: PAH, pulmonary arterial hypertension; WA, pulmonary arteriole area index; WMD, weighted mean difference. (TIF 358 kb)
Additional file 4:
Figure S4. Meta-analysis of overall pooled WMDs with 95% CIs across studies for secondary outcomes in PAH. Forest plot showing that SC therapy significantly reduced the WT in animals with PAH from a random-effects model. Abbreviations: PAH, pulmonary arterial hypertension; WT, wall thickness; WMD, weighted mean difference. (TIF 1560 kb)
Additional file 5:
Figure S5. Funnel plot indicates significant publication bias regarding mPAP in animal studies of PAH. (TIF 347 kb)
Additional file 6:
Figure S6. Funnel plot indicates no significant publication bias regarding mPAP in animal studies of PAH. (TIF 356 kb)
Additional file 7:
Figure S7. Funnel plots demonstrating no significant publication bias among the included studies for mRVP in PAH. (TIF 347 kb)
Additional file 8:
Figure S8. Funnel plots demonstrating no significant publication bias among the included studies for RV/LV+S in PAH. (TIF 357 kb)
Additional file 9:
Figure S9. Funnel plots demonstrating no significant publication bias among the included studies for RV/BW in PAH. (TIF 340 kb)
Additional file 10:
Figure S10. Funnel plots demonstrating no significant publication bias among the included studies for WT in PAH. (TIF 360 kb)
Additional file 11:
Table S1. The PRISMA 2009 checklist. (DOCX 26.7 kb)
Additional file 12:
Table S2. The detailed search strategy. (DOCX 17.6 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Ding, XF., Liang, HY., Yuan, B. et al. Efficacy of stem cell therapy for pulmonary arterial hypertension: a systematic review and meta-analysis of preclinical studies. Stem Cell Res Ther 10, 55 (2019). https://doi.org/10.1186/s13287-019-1162-8
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13287-019-1162-8