
Abstract
Background
The extended-spectrum β-lactamase (ESBL) producing bacteria are present as the serious public health problems due to their resistance to large number of antibiotics. The main aims of this study were to determine the prevalence and antibiotic resistance patterns of bacteria producing extended-spectrum β-lactamases (ESBLs) and to find the suitable cephalosporin/clavulanate combination for phenotypic confirmation of ESBL production.
Methods
During the study period from April 2013 to November 2013, a total of 1003 urine samples from the patients visiting National Public Health Laboratory, Kathmandu, Nepal were collected and processed. The isolates were identified with the help of colony characteristics, gram stain and conventional biochemical tests. Antimicrobial susceptibility testing was performed by Kirby Bauer disc diffusion method. ESBL production screening was done by using ceftriaxone, while ESBL production confirmation was done by using three different 3rd generation cephalosporin/clavulanate combinations.
Results
Of the 138 isolates, Escherichia coli was the most predominant with 88 (63.8 %) isolates. Among the antibiotics tested for gram negative bacteria, highest susceptibility was seen toward imipenem followed by amikacin. Of the total isolates, 68 (49.3 %) were suspected as ESBL producers. Of these, 44 (64.7 %) were phenotypically confirmed to be ESBL producers. The majority of ESBL producers were E. coli with 34 (72.3 %) isolates. Of the three different 3rd generation cephalosporin/clavulanate combinations used, ceftazidime/clavulanate combination was found to be most effective for phenotypic confirmation of ESBL producers and was statistically highly significant (P < 0.01).
Conclusion
Based on the findings of our study, we recommend to use ceftazidime/clavulanate combination for phenotypic confirmation of ESBL producers. Routine ESBL testing for uropathogens along with conventional antibiogram would be useful for proper early management of all the cases of urinary tract infections.
Similar content being viewed by others


Background
Urinary tract infection (UTI) is one of the most common bacterial infections in humans both in the community and hospital setting, and are associated with significant morbidity and mortality as well as high economic burden on society [1]. The disease may be asymptomatic, but if symptoms develop they include cloudy or bloody urine, low-grade fever, back discomfort, fatigue, nausea and vomiting [2]. Most common causative agents of UTI are bacteria of enteric origin and among them Escherichia coli is the most frequent uropathogen [3]. Antibiotic resistance in bacteria is increasing worldwide in both out patients and hospitalized patients. It varies according to geographic location and the haphazard use of antibiotics is playing a significant role in the emergence of the drug resistant bacteria [4, 5]. The β-lactamases are the major defense of gram negative bacteria against β-lactam antibiotics. Extended-spectrum β-lactamase (ESBL) producing organisms have been increasingly detected worldwide with their varying prevalence in different settings and the extent of the problem is under-recognized due to unawareness and poor laboratory detection and reporting at many centers [6]. Considering, the rapid rise in ESBL producing organisms and the lack of accurate figures about the prevalence and the resistance patterns of clinically relevant bacteria producing ESBL in Nepalese population, we conducted this study. Further this study will be helpful for the laboratory personnel to choose most effective cephalosporin/clavulanate combination for phenotypic confirmation of ESBL production.
We processed urine samples of patients suspected of UTI to determine prevalence and the antibiotic susceptibility patterns of clinically relevant bacteria producing extended spectrum β-lactamases and to find the suitable cephalosporin/clavulanate combination for phenotypic confirmation of ESBL producing bacteria.
Methods
The study was conducted at National Public Health Laboratory, Teku, Kathmandu, Nepal from April 2013 to November 2013. During this period, a total of 1003 urine samples from patients suspected of UTI were collected and processed by using standard laboratory methods.
Sample collection and transportation
The patients were given a clean, wide mouth, dry and sterile leak proof container and requested for 5–10 ml mid-stream urine sample. Before providing the container, each patient was instructed properly for the collection of sample. The container was then labelled properly and immediately delivered to the laboratory with the request form for further processing. The quality of the sample was evaluated before processing in terms of proper labelling, visible signs of contamination, improper screwing of cap etc. The improper sample was rejected and the patient was requested to submit next sample.
Culture of specimen
Culture of each urine sample was done on Cystine Lactose Electrolyte Deficient agar plate. An inoculating loop of standard dimension was used to take up fixed and a known volume (0.001 ml) of mixed uncentrifuged urine for inoculation. After inoculation the plates were incubated aerobically at 37 °C for 24 h and were observed for significant growth (105 cfu/ml).
Identification of the isolates
Isolated bacteria were identified by using standard microbiological tools and techniques as described in the Bergey’s manual of systematic bacteriology which involve morphological appearance of the colonies, staining reaction and biochemical properties. Each of the organism was isolated in pure form before performing biochemical tests. The biochemical tests used for the identification included catalase test, oxidase test, sulfide indole and motility test, methyl red test, Voges Proskauer test, citrate utilization test, oxidation fermentation test and triple sugar iron test.
Antibiotic susceptibility testing
The antimicrobial susceptibility testing was done by modified Kirby-Bauer disk diffusion method as recommended by Clinical and Laboratory Standards Institute (CLSI) using Mueller–Hinton agar [7].
Screening and confirmation of ESBL producing isolates
Bacterial isolates were first tested with ceftriaxone (30 µg) as per the CLSI screening criteria. The isolates were suspected to be ESBL producers, if zone of inhibition was ≤25 mm. The suspected ESBL producing isolates were tested for confirmation for ESBL production by combined disc method, using cefpodoxime (10 µg) and cefpodoxime (10 µg) + clavulanate (1 µg), cefotaxime (30 µg) and cefotaxime (30 µg) + clavulanate (10 µg) and ceftazidime (30 µg) and ceftazidime (30 µg) + clavulanate (10 µg). An increase in zone diameter of ≥5 mm in the presence of clavulanate from any or all of the set was confirmed as ESBL production. The antibiotic discs used in the study were supplied by Hi-media laboratories pvt. ltd., India. As controls, E. coli ATCC 25922 (ESBL negative) and Klebsiella pneumoniae ATCC 700603 (ESBL positive) were used.
Data analysis
SPSS version 19.0 was used for statistical analysis. Chi-square test was applied and P < 0.01 was considered statistically significant.
Results
A total of 1003 urine samples were processed for culture, of which 611 (60.9 %) were from male patients and 392 (39.1 %) were from female patients. Of the 611 samples from male, 63 (10.3 %) showed significant growth. Similarly, of the 392 samples from female, 75 (19.1 %) showed significant growth.
Distribution of urinary isolates
Total of 138 bacteria belonging to 13 different species were isolated (Table 1). Among the isolates gram negative bacteria were found predominant constituting 134 (97.10 %) out of 138. Of all the isolates, E. coli was the most frequently isolated species (63.8 %) followed by Pseudomonas aeruginosa (8.7 %). The least common isolates were Edwardsiella spp., Providencia spp., and Serratia spp. Similarly gram positive bacteria constitute 2.9 % of the total isolates and Staphylococcus aureus was the only gram positive bacterium isolated.
Among the 138 growth positive samples, 63 (45.7 %) were from males and 75 (54.3 %) were from females. Among the different isolates, E. coli was the most predominant bacteria both in male 38 (43.2 %) and female 50 (56.8 %).
Antibiotic susceptibility patterns of gram negative isolates
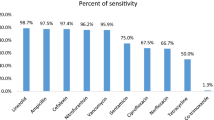
Out of 13 antibiotics tested for gram negative isolates, 7 different antibiotics (belonging to 5 different classes) were used as first line drugs and other six antibiotics were used as second line drugs. Among the first line drugs used, highest rate of susceptibility was shown to nitrofurantoin (61.9 %) and which is statistically significant (P < 0.01). Among the second line drugs used, highest rate of susceptibility was shown toward imipenem (96.4 %) followed by amikacin (91.1 %) and piperacillin/tazobactam (69.6 %). Ampicillin was found as the drug to which most strains were resistant with only 24.6 % of isolates being susceptible (Table 2).
ESBL production among various isolates
Of the 68 suspected ESBL positive isolates, 44 (64.7 %) were ESBL positive whereas 24 (35.3 %) were ESBL negative on confirmation (Table 3). Among the 44 ESBL positive isolates, the majority consist of E. coli (77.27 %). Of the total primary screened E. coli 72.3 % were ESBL positive.
Confirmation of ESBL production using 3 different cephalosporins and respective clavulanic acid combination disks
Among the 68 suspected ESBL positive isolates that were subjected to ESBL confirmation test using three different combination disks, the ceftazidime/ceftazidime+ clavulanate detected 44 ESBL positive isolates whereas cefpodoxime/cefpodoxime+ clavulanate and cefotaxime/cefotaxime+ clavulanate detected 38 and 36 ESBL positive isolates respectively (Table 4). Ceftazidime/clavulanate was found relatively suitable in detection of ESBL positive isolates and was statistically significant (P < 0.01).
Discussion
Similar to our study the studies carried out by Tankhiwale et al., Begum et al. and Baral et al. showed a low percentage of growth positivity [8–10]. The reason behind the low growth rate observed in this study might be due to the prior use of antibiotics, infection due to slow growing organisms or due to those organisms that were not able to grow on the routine media we used. Our findings were in accordance with the findings of Awasthi et al. [11] who found 95.92 % of the urinary isolates to be gram negative bacteria and 4.08 % of the isolates to be gram positive bacteria. Higher prevalence of E. coli seen in our study also resembled the results of the studies done by other researchers [10, 12–14].
Our finding regarding the susceptibility of the gram negative bacteria toward nitrofurantoin resembled the findings reported by Tankhiwale et al. and Baral et al. [8, 10]. Nitrofurantoin should be considered as drug of choice for acute, uncomplicated UTI due to its specificity toward urinary tract and low level of in vitro resistance shown by the bacteria [15]. Nitrofurantoin is not generally prescribed in UTI caused by Proteus spp. as this urease producing organism render urine alkaline and thus decreasing the potency of the drug in vivo [16]. Among the antibiotics evaluated secondarily, highest numbers of the gram negative isolates were found to be susceptible to imipenem followed by amikacin. Higher resistance to penicillins seen in our study might be due to the production of penicillin destroying enzymes (β-lactamases) by the bacteria.
In our study, the rate of ESBL production among the uropathogens was similar to the rates of ESBL production reported by other studies [2, 10]. In our study three different cephalosporins combination with clavulanic acid were used for confirmation of ESBL production and maximum ESBL production was detected by CAZ/CAZ+CV combination which correlated with another study [17].
Limitation of the study
Since this study was conducted in the low income country, where the availability of the advanced laboratory is not easy, we could not use molecular techniques to confirm our findings.
Conclusion
Among the three different combination disks, CAZ/CAZ+CV was found to be the best combination in confirmation of ESBL production. Routine ESBL production testing for uropathogens along with conventional antibiogram would be useful for early proper management of all cases of UTIs.
Abbreviations
- UTI:
-
urinary tract infection
- ESBL:
-
extended spectrum β-lactamase
References
Wagenlehner FME, Naber KG. Treatment of bacterial urinary tract infections: present and future. Eur Urol. 2006;49:235–44.
Neupane S, Pant ND, Khatiwada S, Chaudhary R, Banjara MR. Correlation between biofilm formation and resistance toward different commonly used antibiotics along with extended spectrum beta lactamase production in uropathogenic Escherichia coli isolated from the patients suspected of urinary tract infections visiting Shree Birendra Hospital, Chhauni, Kathmandu Nepal. Antimicrob Resist Infect Control. 2016;15(5):5.
Chang SL, Shortliffe LD. Pediatric urinary tract infections. Pediatr Clin N Am. 2006;53:379–400.
Taneja N, Rao P, Arora J, Dogra A. Occurrences of ESBL & AmpC β-lactamases and susceptibility to newer antimicrobial agents in complicated UTI. Indian J Med Res. 2008;127:85–8.
Levi SB. Antibiotic resistance: consequences of inaction. Clin Infect Dis. 2001;2001(33):124–9.
Ashrafian F, Askari E, Kalamatizade E, Ghabouli Shahroodi MJ, Naderi-Nasab M. The frequency of extended spectrum beta lactamase in Escherichia coli and Klebsiella pneumonia. J med bacteriol. 2012;1:12–9.
CLSI. Performance standards for antimicrobial susceptibility testing; Twenty-First Informational Supplement. CLSI document M100-S21. Wayne PA: Clinical and Laboratory Standards Institute. 2011.
Tankhiwale SS, Jalgaonkar SV, Ahamad S, Hassani U. Evaluation of extended spectrum beta lactamase in urinary isolates. Indian J Med Res. 2004;120:553–6.
Begum S, Salam MA, Begum FAN, Hassan P, Haq JA. Detection of extended spectrum β-lactamase in Pseudomonas spp. isolated from two tertiary care hospitals in Bangladesh. BMC Res Notes. 2013;6:7.
Baral P, Neupane S, Marasini BP, Ghimire KR, Lekhak B, Shrestha B. High prevalence of multidrug resistance in bacterial uropathogens from Kathmandu Nepal. BMC Res Notes. 2012;5:38.
Awasthi TR, Pant ND, Dahal PR. Prevalence of multidrug resistant bacteria in causing community acquired urinary tract infection among the patients attending outpatient Department of Seti Zonal Hospital, Dhangadi, Nepal. Nepal J Biotechnol. 2015;3(1):55–9.
Jadhav S, Gandham N, Paul A, Mishra RN, Mani KR. Charactarization of multidrug resistant uropathogens E. coli (UPEC) with special reference to B2-025B-ST131-CTX-M-15 in India. J Pharm Biochem Sci. 2012;23:1–4.
Farrel DJ, Morrisey I, Rubies D, Robbins M, Felmingham D. A UK multicenter study of the antimicrobial susceptibility of bacterial pathogens causing UTI. J Infect. 2003;46:94–100.
Kahlmeter G. The ECO-SENS project: a prospective, multinational, multicenter epidemiological survey of the prevalence and antimicrobial susceptibility of urinary tract pathogens-interim report. J Antimicrob Chemother. 2000;46:15–22.
Obi CL, Tarupiwa A, Simango C. Scope of urinary pathogens isolated in the public Health Bacteriology Laboratory, Harare: antibiotic susceptibility patterns of isolates and incidence of haemolytic bacteria. Cent Afr J Med. 1996;42:244–9.
Collee JG, Frasier AG, Marmion BP, Simmons A. In: Collee JG, Frasier AG, Marmion BP, Simmons A, editors. Mackie and McCartney practical medical microbiology. 14th ed. New York: Churchill Livingstone; 1999. p. 361–7.
Svard L. Evaluation of phenotypic and genotypic extended-spectrum beta-lactamase detection methods. A project work submitted to school of biological science. Dublin: Dublin Institute of Technology; 2007. p. 48–53.
Authors’ contributions
NDP and RB contributed in conception and designing of the study, collection and processing of the samples, statistical analysis of data and preparation of manuscript. AP and MS were involved in monitoring of the study. All authors read and approved the final manuscript.
Acknowledgements
The authors thank the management of Nepal Public Health Laboratory (NPHL) for providing opportunity to conduct this study. Our thanks also go to the staff of NPHL who assisted us technically in carrying out the laboratory work. No sources provided any fund.
Competing interests
The authors declare that they have no competing interests.
Availability of supporting data
The supporting data can be made available by the authors of this article to all the interested researchers upon request.
Ethical consideration
Before commencing of the study the research protocol was approved and the need for consent was waived by Goldengate International College, Kathmandu, Nepal.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Bhandari, R., Pant, N.D., Poudel, A. et al. Assessment of the effectiveness of three different cephalosporin/clavulanate combinations for the phenotypic confirmation of extended-spectrum beta-lactamase producing bacteria isolated from urine samples at National Public Health Laboratory, Kathmandu, Nepal. BMC Res Notes 9, 390 (2016). https://doi.org/10.1186/s13104-016-2192-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-016-2192-2