
Abstract
Background
Production of AmpC and extended spectrum beta-lactamases among urinary isolates has created a serious problem to the successful management of the urinary tract infection. The main purpose of this study was to determine the rates of the extended spectrum beta-lactamase (ESBL) production and AmpC beta-lactamase (ABL) production among urinary isolates.
Results
Among total 564 urinary isolates, 514 (91.1%) were gram negative bacilli and 50 (8.9%) were gram positive cocci. E. coli (76.1%) was the most common bacteria isolated. Staphylococcus aureus (6.7%) was the predominant gram positive bacteria isolated. 35 (6.8%) of the 514 gram negative bacilli were ESBL producers. Similarly, 14 (2.7%) of the gram negative bacilli were ABL producers. Only one isolate was ESBL and ABL co-producer. Highest rate of susceptibility of gram negative bacteria was seen toward amikacin (97.3%) followed by imipenem (94.4%). Similarly, highest rate of susceptibility among gram positive cocci was seen toward vancomycin (100%) followed by amikacin (93.5%).
Conclusions
Low rates of AmpC and extended spectrum beta-lactamases production in comparison to other previous studies were reported. On the basis of the antimicrobial susceptibility patterns of the bacteria we reported in our study, amikacin, imipenem and nitrofurantoin can be used for the preliminary treatment of urinary tract infections caused by gram negative bacteria and vancomycin and amikacin for treatment of urinary tract infections caused by gram positive bacteria.
Similar content being viewed by others

Background
Urinary tract infection is among the commonly encountered bacterial infections in human [1]. Antibiotics are important therapeutic means for the treatment of bacterial infections. However, the development of drug resistance among the bacteria has created a serious problem to the successful treatment of the bacterial infections. Production of AmpC and extended spectrum beta-lactamases are the important mechanisms of drug resistance mainly among gram negative bacteria. All ESBL producing organisms should be considered resistant to all penicillins (except temocillin), cephalosporins (except cefoxitin and cefotetan) and aztreonam [2, 3]. So, there are limited treatment options for infections caused by extended spectrum beta-lactamase (ESBL) producing organisms and their involvement in severe infections may result into treatment failure if the antibiotics are chosen just on the basis of regular antimicrobial susceptibility testing without determination of ESBL production [3]. ESBL producing bacteria may show in vitro susceptibility to some extended spectrum cephalosporins but the use of such antibiotics for treatment of the infections by ESBL producing strains may result into treatment failure [3]. Similarly, AmpC β-lactamases producing organisms are resistant to narrow, broad-, and expanded-spectrum cephalosporins and cephamycins and can not be inhibited by clavulanate, sulbactam, and tazobactam [4]. They show non-beta-lactam coresistance and have a few treatment options [5]. Further, they have high potential to transfer the drug resistance features to other bacteria horizontally [5]. In Nepal, limited information is present in AmpC beta-lactamase (ABL) producing bacteria in comparison to extended-spectrum β-lactamase-producing organisms [5]. Different studies in Nepal have reported the different rates of ESBL and ABL production among gram negative bacteria [1, 5]. So in this study we determined the prevalence of the ESBL and ABL producing organisms in causing urinary tract infection.
Methods
Study design and setting
A descriptive cross-sectional hospital based study was conducted using all 564 urinary isolates isolated from April 2014 to October 2014 at Microbiology Laboratory of Alka Hospital, Lalitpur, Nepal. The isolates were already collected and stored.
Identification of the organisms
The organisms were identified using colony morphology, Gram’s stain and biochemical tests [6, 7]. The common biochemical tests used were oxidase test, catalase test, sulphur indole motility test, urease test, citrate utilization test, tripal sugar iron agar test, methyl red and Voger-Proskauer test, coagulase test, bile esculin agar test etc.
Antimicrobial susceptibility testing
The antimicrobial susceptibility testing was performed using Kirby-Bauer disc diffusion technique following clinical and laboratory standards institute guidelines [8].
Detection of ESBL and ABL production
Detection of ESBL production was done by combined disc method using ceftazidime and ceftazidime/clavulanic acid discs [8] and detection of ABL production was done by using cefoxitin and cefoxitin/boronic acid discs [9].
Results
Among total 564 bacteria, 514 (91.1%) were gram negative bacilli and 50 (8.9%) were gram positive cocci. E. coli (76.1%) was the most common bacteria followed by Staphylococcus aureus (6.7%), Klebsiella pneumoniae (4.6%), Proteus mirabilis (2.3%), Citrobacter freundii (2.3%), Providencia spp. (1.6%), Enterococcus faecalis (1.6%), Morganella morganii (1.4%), Acinetobacter spp. (1.1%), Proteus vulgaris (0.9%), coagulase negative Staphylococcus spp. (0.6%), Klebsiella oxytoca (0.4%) and Pseudomonas aeruginosa (0.2%).
Production of ESBL and ABL by gram negative urinary isolates
35 (6.8%) of the 514 gram negative bacilli were ESBL producers. Among ESBL producing gram negative bacilli, 33 were E. coli and 2 were K. pneumoniae. Similarly, 14 (2.7%) of the gram negative bacilli were ABL producers. Among which, 10 were E. coli and 1 each K. pneumoniae, C. freundii, K. oxytoca and M. morganii. Only one isolate was ESBL and ABL co-producer.
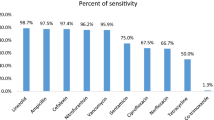
Antibiotic susceptibility patterns of gram negative bacilli
Highest rate of susceptibility was seen toward amikacin (97.3%) followed by imipenem (94.4%) (Table 1).
Antibiotic susceptibility patterns of gram positive cocci
Highest rate of susceptibility was seen toward vancomycin (100%) followed by amikacin (93.5%) (Table 2).
Discussion
As in our study, Bhatt et al. [10] also found the gram negative bacilli to be higher in number among urinary isolates (92.3%) followed by gram positive cocci (7.7%) with E. coli being most common organism. In our study, 6.8% and 2.7% of all gram negative bacilli isolated were found to be ESBL and ABL producers, while one isolate was ESBL and ABL co-producer. However, Chander and Shrestha reported higher rate of ESBL production among uropathogens in Nepal [11]. Similarly, Ansari et al. [12] found the rates of ABL production (9%) and ESBL/ABL co-production (4%) to be higher. The prevalence of drug resistance among clinical isolates due to different mechanisms varies from place to place and is changing with time. The main reason for this may be difference in the antibiotic usage in different area during different period of time. The co-expressions of different variants of ESBL and AmpC genes may be responsible for AmpC/ESBL co-production [13] but sometime this co-production may give false negative tests in the detection of ESBL [13]. In this study, highest rate of susceptibility among gram negative isolate was seen toward amikacin followed by imipenem and nitrofurantoin. Similarly, Noor et al. reported highest rate of susceptibility toward imipenem followed by amikacin among uropathogens [14]. Neupane et al. also found the highest rate of susceptibility toward amikacin (87.5%) followed by nitrofurantoin (72.6%) [15]. High rate of susceptibility to nitrofurantoin was also noted by Bhatt et al. (82.2%) [10]. Though the bacteria show high susceptibility to these drugs, amikacin belonging to aminoglycosides which have nephrotoxic effect and imipenem being an intravenous antibiotic, they are not recommended as the first line therapy in the treatment of urinary tract infection. Further, nitrofurantoin is recommended only for the treatment of uncomplicated urinary tract infection because it does not give good tissue concentration [16].
Among gram positive cocci, highest rate of susceptibility was seen toward vancomycin (100%) followed by amikacin (93.5%). No vancomycin resistant S. aureus isolates have been reported from Nepal [17].
Limitations of the study
Due to lack of resources and limited time available we could not use molecular techniques and large numbers of samples in our study.
Conclusion
Low rates of AmpC and extended spectrum beta-lactamases production in comparison to other previous studies were reported. On the basis of the antimicrobial susceptibility patterns of the bacteria we reported in our study, amikacin, imipenem and nitrofurantoin can be used for the preliminary treatment of urinary tract infections caused by gram negative bacteria and vancomycin and amikacin for the treatment of urinary tract infections caused by gram positive bacteria.
Abbreviations
- ABL:
-
AmpC beta-lactamase
- ESBL:
-
extended spectrum beta-lactamase
References
Bhandari R, Pant ND, Poudel A, Sharma M. Assessment of the effectiveness of three different cephalosporin/clavulanate combinations for the phenotypic confirmation of extended-spectrum beta-lactamase producing bacteria isolated from urine samples at National Public Health Laboratory, Kathmandu, Nepal. BMC Res Notes. 2016;9:390.
Pitout JD, Nordmann P, Laupland KB, Poirel L. Emergence of Enterobacteriaceae producing extended-spectrum beta-lactamases (ESBLs) in the community. J Antimicrob Chemother. 2005;56(1):52–9.
Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005;18(4):657–86.
Thomson KS. Extended-spectrum-beta-lactamase, AmpC, and Carbapenemase issues. J Clin Microbiol. 2010;48(4):1019–25.
Baral P, Neupane S, Shrestha B, Ghimire KR, Marasini BP, Lekhak B. Clinical and microbiological observational study on AmpC β-lactamase-producing Enterobacteriaceae in a hospital of Nepal. Braz J Infect Dis. 2013;17(2):256–9.
Cheesbrough M. District laboratory practice in tropical countries, part II. 2nd ed. New York: Cambridge University Press; 2006.
Holt JG, Krieg NR, Sneath PHA, Staley JT, Williams ST. Bergey’s manual of determinative bacteriology. Baltimore: Williamsons and Wilkins; 1994.
Clinical and Laboratory Standards Institute. CLSI document M100-S24. Performance standards for antimicrobial susceptibility testing. 24th ed. Wayne: CLSI; 2014.
Tan TY, Ng LSY, He J, Koh TH, Hsu LY. Evaluation of screening methods to detect plasmid-mediated AmpC in Escherichia coli, Klebsiella pneumoniae and Proteus mirabilis. Antimicrob Agents Chemother. 2009;53(1):146–9.
Bhatt CP, Shrestha B, Khadka S, Swar S, Shah B, Pun K. Etiology of urinary tract infection and drug resistance cases of uropathogens. J Kathmandu Med Coll. 2012;1(2):114–20.
Chander A, Shrestha CD. Prevalence of extended spectrum beta lactamase producing Escherichia coli and Klebsiella pneumoniae urinary isolates in a tertiary care Hospital in Kathmandu, Nepal. BMC Res Notes. 2013;6:487.
Ansari S, Nepal HP, Gautam R, Shrestha S, Neopane P, Gurung G, et al. Community acquired multi-drug resistant clinical isolates of Escherichia coli in a tertiary care center of Nepal. Antimicrob Resistance Infect Control. 2015;4:15.
Hussain M, Hasan F, Shah AA, Hameed A, Jung M, Rayamajhi N, et al. Prevalence of class A and AmpC β-lactamases in clinical Escherichia coli isolates from Pakistan Institute of Medical Science, Islamabad, Pakistan. Jpn J Infect Dis. 2011;64:249–52.
Noor AF, Shams F, Munshi SK, Hassan M, Noor R. Prevalence and antibiogram profile of uropathogens isolated from hospital and community patients with urinary tract infections in Dhaka city. J Bangladesh Acad Sci. 2013;37(1):57–63.
Neupane S, Pant ND, Khatiwada S, Chaudhary R, Banjara MR. Correlation between biofilm formation and resistance toward different commonly used antibiotics along with extended spectrum beta lactamase production in uropathogenic Escherichia coli isolated from the patients suspected of urinary tract infections visiting Shree Birendra Hospital, Chhauni, Kathmandu, Nepal. Antimicrob Resist Infect Control. 2016;5:5.
Honderlick P, Cahen P, Gravisse J, Vignon D. Uncomplicated urinary tract infections, what about fosfomycin and nitrofurantoin in 2006? Pathol Biol. 2006;54:462–6.
Kshetry AO, Pant ND, Bhandari R, Khatri S, Shrestha KL, Upadhaya SK, et al. Minimum inhibitory concentration of vancomycin to methicillin resistant Staphylococcus aureus isolated from different clinical samples at a tertiary care hospital in Nepal. Antimicrob Resist Infect Control. 2016;5:27.
Authors’ contributions
NDP conceived and designed the study, carried out the research works, analyzed data, and prepared the manuscript. SR and RB designed the study, carried out the research works, and analyzed the data. AG, RP and MA helped in analysis of data and in research works. JA and VKS monitored the study. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to thank Tri-Chandra Multiple Campus, Kathmandu, Nepal and Alka Hospital, Lalitpur, Nepal for providing opportunity to conduct this study. The authors are also grateful to all the patients and technical staffs for their help during the study.
Competing interests
The authors declare that there is no conflict of interest regarding the publication of this paper.
Availability of data and materials
The data related to this study can be made available by the authors of this article if requested.
Ethical approval and consent
To conduct this study the permission was taken from Alka Hospital, Lalitpur, Nepal.
Consent for publication
Not applicable.
Funding
To conduct this study no fund was obtained from any sources.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Rai, S., Pant, N.D., Bhandari, R. et al. AmpC and extended spectrum beta-lactamases production among urinary isolates from a tertiary care hospital in Lalitpur, Nepal. BMC Res Notes 10, 467 (2017). https://doi.org/10.1186/s13104-017-2784-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-017-2784-5