
Abstract
Background
Although both rheumatoid factor (RF) and anticyclic citrullinated peptide antibodies (anti-CCP) are useful for diagnosing rheumatoid arthritis (RA), the impact of these autoantibodies on the efficacy of tumor necrosis factor (TNF) inhibitors has been controversial. The aim of this post hoc analysis of a randomized double-blind study (the RISING study) was to investigate the influences of RF and anti-CCP on the clinical response to infliximab in patients with RA.
Methods
Methotrexate-refractory patients with RA received 3 mg/kg of infliximab from weeks 0 to 6 and then 3, 6, or 10 mg/kg every 8 weeks from weeks 14 to 46. In this post hoc analysis, patients were stratified into three classes on the basis of baseline RF/anti-CCP titers: “low/low-C” (RF < 55 IU/ml, anti-CCP < 42 U/ml), “high/high-C” (RF ≥ 160 IU/ml, anti-CCP ≥ 100 U/ml), and “middle-C” (neither low/low-C nor high/high-C). Baseline plasma TNF level, serum infliximab level, and disease activity were compared between the three classes.
Results
Baseline RF and anti-CCP titers showed significant correlations with baseline TNF and infliximab levels in weeks 2–14. Comparison of the three classes showed that baseline TNF level was lowest in the low/low-C group and highest in the high/high-C group (median 0.73 versus 1.15 pg/ml), that infliximab levels at week 14 were highest in the low/low-C group and lowest in the high/high-C group (median 1.0 versus 0.1 μg/ml), and that Disease Activity Score in 28 joints based on C-reactive protein at week 14 was lowest in the low/low-C group and highest in the high/high-C group (median 3.17 versus 3.82). A similar correlation was observed at week 54 in the 3 mg/kg dosing group, but not in the 6 or 10 mg/kg group. Significant decreases in both RF and anti-CCP were observed during infliximab treatment.
Conclusions
RF/anti-CCP titers correlated with TNF level. This might explain the association of RF/anti-CCP with infliximab level and clinical response in patients with RA. Baseline RF/anti-CCP titers may serve as indices that aid infliximab treatment.
Trial registration
ClinicalTrials.gov, NCT00691028. Retrospectively registered on 3 June 2008.
Similar content being viewed by others


Background
Both rheumatoid factor (RF) and anticyclic citrullinated peptide antibodies (anti-CCP) are useful for diagnosing rheumatoid arthritis (RA) [1, 2], and they have been shown to be associated with the progression of joint destruction in patients with RA [3, 4]. However, the influence of these autoantibodies on the clinical status and disease activity of patients with RA has yet to be fully clarified.
RF and anti-CCP have recently been shown to influence the efficacy of some non-tumor necrosis factor (non-TNF) biological disease-modifying antirheumatic drugs (DMARDs) [5,6,7,8,9]. However, the influence of these autoantibodies on the efficacy of TNF inhibitors, the first biological DMARDs approved for RA, has been controversial [10,11,12,13,14,15,16].
The RISING study was a randomized, double-blind trial that demonstrated the usefulness of dose escalation of infliximab (IFX) in RA [17]. In a post hoc analysis of this study, we previously reported that the baseline plasma TNF level greatly influenced serum IFX levels and predicted clinical response at 1 year [18].
RF/anti-CCP double-positive but not single-positive patients with RA were reported to show significantly higher circulating TNF levels than double-negative patients [19]. We therefore hypothesized that “both RF-high and anti-CCP-high” would correlate with a higher TNF level, which would result in a lower IFX level and clinical response. In the present analysis using data from the RISING study, we explored the association between baseline RF and anti-CCP titers with efficacy of IFX therapy in patients with active RA despite methotrexate (MTX) treatment.
Methods
Study protocol
The protocol of the RISING study has been published elsewhere [17, 18]. Patients with active RA (diagnosed according to 1987 American College of Rheumatology criteria [20]) despite MTX treatment were treated with a standard dose (3 mg/kg) of an IFX originator (Remicade; Mitsubishi Tanabe Pharma Corporation, Osaka, Japan) at weeks 0, 2, and 6 (W0, W2, and W6, respectively), after which they were randomized to three dosing groups and treated with 3, 6, or 10 mg/kg of IFX every 8 weeks from W14 to W46. Active RA was defined by the presence of at least six swollen joints, at least six tender joints, and an erythrocyte sedimentation rate ≥ 28 mm/h or a serum C-reactive protein (CRP) level ≥ 2.0 mg/dl.
Disease activity and laboratory testing
Disease activity was evaluated by the Disease Activity Score in 28 joints based on C-reactive protein (DAS28-CRP). Because there is controversy about the cutoff level of DAS28-CRP, which might underestimate disease activity when using cutoff values validated for DAS28 based on erythrocyte sedimentation rate [21], we used the cutoff levels that were previously estimated in Japanese patients with RA as follows: clinical remission (REM) < 2.3, low disease activity without clinical remission (LDA), ≥ 2.3 but < 2.7, moderate disease activity (MDA) ≥ 2.7 but ≤ 4.1, and high disease activity (HDA) > 4.1 [22].
RF titers were measured by a latex agglutination test using the Auto LIA-RF kit (Nissui Pharmaceutical Co., Tokyo, Japan) with a detectable limit of ≥ 3 IU/ml (normal range ≤ 15 IU/ml). Anti-CCP titers were measured by performing an enzyme-linked immunosorbent assay (ELISA) using the DIASTAT anti-CCP kit (Euro Diagnostica, Malmö, Sweden) with a detectable range of ≥ 0.6 to < 100 U/ml (normal range ≤ 5.0 U/ml). Disease activity, RF, and anti-CCP at W54 were evaluated using the last observation carried forward approach.
Baseline plasma TNF levels (just before the first IFX infusion) were measured by ELISA using the QuantiGlo ELISA Kit (QTA00B; R&D Systems Inc., Minneapolis, MN, USA) as described previously [18]. Baseline plasma interleukin (IL)-6 and serum matrix metalloproteinase (MMP)-3 levels were measured by ELISA [18]. All laboratory tests were performed at LSI Medience Corporation (Tokyo, Japan).
Serum IFX levels and anti-infliximab antibody (ATI) positivity were measured by ELISA [17] at Mitsubishi Tanabe Pharma Corporation using the same ELISA system (Janssen Biotech, Inc.; Horsham, PA, USA) as that used in previous phases II and III studies for RA [23,24,25]. IFX levels were evaluated at W2, W6, W10, W14, and W54, with the lower detection level of < 0.1 μg/ml. ATI positivity was evaluated at W54 in study completers or at 12 weeks after the last infusion in noncompleters. Patients with detectable serum IFX levels were considered to be ATI-negative and were not evaluated for ATI positivity (i.e., serum IFX levels were < 0.1 μg/ml in all ATI-positive patients), as described previously [17, 23,24,25].
Stratification of patients using baseline RF and anti-CCP titers
Baseline RF and anti-CCP cutoff values for patient stratification were defined as follows: RF-low < 55 IU/ml and RF-high ≥ 160 IU/ml (both are tertile values at baseline in this study) and anti-CCP-low < 42 U/ml and anti-CCP-high ≥ 100 U/ml. The lower cutoff for anti-CCP of 42 U/ml was the first tertile for baseline anti-CCP titer, whereas the upper cutoff of 100 U/ml corresponded to the upper detection limit for anti-CCP (Additional file 1).
Patients with RA were then stratified into the following three classes on the basis of the above-mentioned cutoff values: low/low class (both RF-low and anti-CCP-low, low/low-C), high/high class (both RF-high and anti-CCP-high, high/high-C), and middle class (patients who did not meet the criteria for either class, middle-C) (Additional file 2). The following data were compared between the three classes: baseline plasma TNF level, serum IFX levels at W2, W6, W10, W14, and W54, and disease activities at W0, W2, W6, W10, W14, and W54.
Statistical analysis
Spearman’s rank correlation test was used to evaluate the correlation of baseline RF titer and baseline anti-CCP titer with patient characteristics, serum IFX levels, and disease activity. The Kruskal-Wallis test or chi-square test was used to compare patients’ characteristics, IFX levels, and disease activity among the three dosing groups (3, 6, and 10 mg/kg) or among three classes stratified on the basis of RF/anti-CCP at baseline (low/low-C, middle-C, and high/high-C). In addition, RF titers, anti-CCP titers, and the rate of three classes at W30 and W54 were compared with those at baseline (W0) using the Wilcoxon signed-rank test in each dosing group. All statistical analyses were performed using SAS version 9.4 software (SAS Institute Japan Ltd., Tokyo, Japan). p < 0.05 (two-tailed) was considered to indicate statistical significance.
Results
Patient baseline characteristics and clinical response at week 54
Table 1 shows patient baseline characteristics and clinical response at W54 for each IFX dosing group. Median (IQR), first tertile, and second tertile of baseline RF titers were 92 (37–237), 55, and 160 IU/ml, respectively (Additional file 1). The proportion of patients who were RF-negative (≤15 IU/ml) was 13% (41 of 307). Although no significant difference was observed in patient baseline characteristics among three dosing groups, the RF-negative rate tended to be high in the 3 mg/kg group.
The median (IQR) and first tertile of baseline anti-CCP titers were ≥ 100 (28, ≥ 100) and 42 U/ml, respectively. The proportion of patients with a baseline anti-CCP titer above the upper detection limit (≥ 100 U/ml) was 58% (177 of 307), and the proportion of patients who were anti-CCP-negative (≤ 5.0 U/ml) was 8% (25 of 307). The proportion of patients who were seronegative for both RF and anti-CCP was 6% (19 of 307). Comorbidity was observed in 78% of patients; the major comorbidities were hypertension (21%), pollinosis (17%), osteoporosis (13%), and anemia (12%).
Table 1 also shows the clinical responses of the 3, 6, and 10 mg/kg dosing groups at W54. Significant differences in DAS28-CRP and disease activity criteria at W54 were observed among the three dosing groups. In contrast, both RF and anti-CCP titers significantly decreased after IFX treatment in each dosing group; however, no significant difference was observed among the three dosing groups (Additional file 3).
Correlations of baseline RF and anti-CCP titers with patient baseline characteristics
Table 2 shows the correlations of baseline RF and anti-CCP titers with patient baseline characteristics. The baseline RF titer showed significant correlations with sex, age, duration of disease, total modified Sharp score, MMP-3, and anti-CCP, as well as TNF level, although the correlation coefficient for each was low. In contrast, the baseline anti-CCP titer showed significant correlations with comorbidity and RF as well as TNF level. Accordingly, TNF level was the only baseline characteristic that correlated with both RF and anti-CCP.
Correlations of baseline RF and anti-CCP titers with serum IFX levels
We previously reported a significant negative correlation between the TNF level and IFX level [18]. In the present analysis, we explored the association of baseline RF and anti-CCP titers with IFX levels in W2 to W14 in patients receiving 3 mg/kg of IFX (Table 3). Similarly to our previous findings regarding TNF and IFX levels, significant negative correlations were noted between IFX levels and both baseline RF and anti-CCP titers at all time points (W2 to W14). Among the other patient baseline characteristics analyzed, only sex was significantly correlated with IFX levels at all time points.
Correlation of patient baseline characteristics with the three classes stratified by baseline RF and anti-CCP titers
We initially hypothesized that TNF level should be low in patients who are negative for RF and anti-CCP at baseline, which would lead to high IFX levels. However, the relatively small patient group of 41 RF-negative patients and 25 anti-CCP-negative patients in the RISING study prevented analysis of differences in IFX level and disease activity at W54 between the three IFX dosing groups. To resolve this issue, we stratified the patients in the RISING study into three classes using cutoff values for both RF and anti-CCP as described in the Methods section above as low/low-C (RF-low/anti-CCP-low), high/high-C (RF-high/anti-CCP-high), and middle-C (those who did not meet the criteria for either class) (Additional file 2).
Table 4 shows patient baseline characteristics in the three stratified classes. A significant difference was observed in baseline TNF levels among three classes, with the TNF level being lowest in low/low-C (median 0.73 pg/ml), middle in middle-C (median 0.91 pg/ml), and highest in high/high-C (median 1.15 pg/ml). The proportions of patients with a high baseline TNF level ≥ 1.65 pg/ml [18] in low/low-C, middle-C, and high/high-C were 8%, 8%, and 30%, respectively. Regarding disease activity and Health Assessment Questionnaire at baseline, significant differences were observed among the three classes; however, the values were lower in middle-C.
Correlation of serum IFX levels and disease activity until week 14 in the three stratified classes
Table 5 shows the IFX levels in W2 to W14 and disease activity in W0 to W14 in the three classes. Significant differences in IFX levels were observed in W2 to W14, with observed levels highest in low/low-C and lowest in high/high-C. Even in high/high-C, median IFX levels in W2 to W10 (2 or 4 weeks after the previous infusion) were above the threshold level for clinical response (≥ 1.0 μg/ml), the value for which has been reported in previous clinical studies using the same ELISA system [17, 24, 25]. However, in high/high-C, the median IFX level at W14 was 0.4 μg/ml, and the proportion of patients with IFX levels ≥ 1.0 μg/ml was only 30%. The corresponding proportion in middle-C was between that in low/low-C and that in high/high-C for each time point.
With regard to disease activity, an opposite trend was observed: The median DAS28-CRP was lowest in low/low-C and highest in high/high-C, although the difference (marginally significant) was observed only at W14 (8 weeks after the previous infusion).
Correlation of serum IFX levels and disease activity at week 54 with the three stratified classes in each IFX dosing group
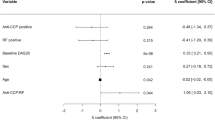
Figure 1a and b shows the IFX levels and DAS28-CRP at W54 in the three stratified classes in each IFX dosing group (3, 6, or 10 mg/kg group). In the 3 mg/kg dosing group, a significant difference in IFX levels at W54 was observed among the three stratified classes. The proportion of patients with IFX level ≥ 1.0 μg/ml at W54 was 52% in low/low-C but only 12% in high/high-C with a median IFX level of 0.1 μg/ml (close to the lower detection limit).

a, b Serum infliximab level and disease activity at week 54 in three stratified classes. Differences among three classes stratified on the basis of rheumatoid factor and anti-cyclic citrullinated peptide antibodies at week 0 in serum infliximab (IFX) level at week 54 (a) and with disease activity at week 54 b were evaluated by Kruskal-Wallis test. Disease activity was evaluated using Disease Activity Score in 28 joints based on C-reactive protein with the following REM cutoff levels: < 2.3, LDA ≥ 2.3 but < 2.7, MDA ≥ 2.7 but ≤ 4.1, and HDA > 4.1 [22]. HDA High disease activity, LDA Low disease activity without clinical remission, MDA Moderate disease activity, REM Clinical remission
A significant difference was also observed in disease activity at W54 in patients receiving 3 mg/kg of IFX. The proportions of patients with REM and HDA were 48% and 9% in low/low-C and 24% and 38% in high/high-C, respectively. In patients receiving IFX at 6 or 10 mg/kg, the IFX level at W54 was lowest in high/high-C, but not to a significant degree. The median IFX level in high/high-C at W54 was 3.0 or 3.8 μg/ml in patients receiving 6 or 10 mg/kg of IFX, respectively, either of which was ≥ 1.0 μg/ml. With regard to disease activity at W54 in patients receiving IFX at 6 or 10 mg/kg, no significant difference was observed among the three classes. In addition, the proportion of patients with RF-high/anti-CCP-high decreased, and the proportion of those with RF-low/anti-CCP-low increased during IFX treatment in each dosing group, despite no differences among the three dosing groups (Additional file 3).
ATI positivity
As described in the Methods section above, patients with detectable serum IFX levels (≥ 0.1 μg/ml) were defined as ATI-negative and were not evaluated for ATI positivity. ATI positivity was evaluated in 98 patients. ATI positivity rates in low/low-C, middle-C, and high/high-C were 13% (3 of 23, ATI was analyzed in 5), 34% (16 of 47, ATI was analyzed in 26), and 28% (8 of 29, ATI was analyzed in 14), respectively, in the 3 mg/kg dosing group (n = 99); 15% (3 of 20, ATI was analyzed in 6), 24% (15 of 62, ATI was analyzed in 21), and 27% (6 of 22, ATI was analyzed in 7), respectively, in the 6 mg/kg group (n = 104); and 10% (1 of 10, ATI was analyzed in 1), 14% (10 of 74, ATI was analyzed in 14), and 10% (2 of 20, ATI was analyzed in 4), respectively, in the 10 mg/kg group (n = 104). ATI positivity rates in low/low-C tended to be lower than in the other classes, but no significant difference was observed among the three dosing groups.
Discussion
Despite its efficacy in treating RA [26,27,28,29], IFX treatment is very costly. Therefore, predicting the clinical efficacy of IFX therapy is extremely important with regard to medical economics. Although prediction of the clinical efficacy of IFX therapy has been investigated in many studies, results have been controversial [10, 11, 30]. Although researchers in some studies reported that early response predicted long-term responses [31, 32], identifying predictive factors “at baseline” would be even more worthwhile in establishing IFX treatment strategies.
Our previous findings derived from a post hoc analysis of the RISING study demonstrated that patients with a high baseline TNF level had low IFX levels during IFX therapy and that this was associated with a poor clinical response 1 year later, particularly in patients on 3 mg/kg therapy [18]. However, TNF levels are generally quite low, and measurement results can differ markedly depending on the assay system used [18, 33,34,35]. In addition, measurement of TNF levels is not routine in clinical practice. Thus, other factors that can easily be measured in the clinical setting and can predict the efficacy of IFX therapy are desired.
In this post hoc analysis of the RISING study, we found a positive correlation of baseline TNF level, and a negative correlation of IFX levels, in W2 to W14 with baseline RF and anti-CCP titers. We then stratified patients using baseline RF and anti-CCP titers into low/low-C, middle-C, and high/high-C to evaluate the correlation with TNF levels as well as IFX levels and clinical responses. We found that RF-high/anti-CCP-high patients (high/high-C) had higher baseline TNF and lower IFX levels than other classes (Tables 4 and 5).
In RF-high/anti-CCP-high patients, humoral immunity may be enhanced, leading to an increasing risk of ATI expression, which correlates with lower IFX levels [36, 37]. Indeed, ATI positivity was higher in high/high-C than in low/low-C in the 3 and 6 mg/kg dosing groups, despite the absence of a significant difference. Therefore, the low IFX level in high/high-C might be due to the induction of ATI production in this patient class. Meanwhile, we observed a negative correlation between baseline RF/anti-CCP and IFX level even at the early induction phase (W2, after the first infusion), in which most patients were thought not to produce ATI (Table 5). We therefore considered that the correlation of baseline RF/anti-CCP with IFX level is likely due to the high baseline TNF level and that high ATI positivity in high/high-C may be the consequence of a low IFX level. However, we did not evaluate ATI positivity in patients with a detectable serum IFX level, and we did not exclude the effect of ATI production on the low IFX level.
Upon evaluating the correlation between DAS28-CRP until W14 and the three stratified classes, a significant correlation was observed in only at W14 (8 weeks after the previous infusion) (Table 5). Although IFX levels at W2 to W10 were lower in high/high-C than in the other classes, ≥ 60% of patients in high/high-C had a serum level > 1.0 μg/ml, which was reported as the threshold value for clinical response in several clinical studies using the same ELISA system [17, 24, 25]. In contrast, the median serum IFX level at W14 was 0.4 μg/ml, and approximately one-third of patients showed a level that was below the lower limit of detection (< 0.1 μg/ml). Given these findings, we believe that the difference (marginally significant) in disease activity observed only at W14 was likely due to the markedly low IFX levels at W14 in high/high-C.
Similarly to these findings at W14, significant differences in IFX levels and disease activity were also observed at W54 in patients who continued to receive IFX at 3 mg/kg (Fig. 1a and b): high IFX levels and LDA in low/low-C, low IFX levels and HDA in high/high-C, and intermediate values in middle-C. Given these findings, baseline RF and anti-CCP titers were clearly associated with treatment response at W54 in patients receiving 3 mg/kg IFX.
In contrast, in patients receiving IFX at 6 or 10 mg/kg, IFX level at W54 tended to be lowest in high/high-C. However, no significant difference was observed in either IFX level or disease activity. In high/high-C, the median IFX levels at W54 in the 6 and 10 mg/kg dosing groups were 3.0 and 3.8 μg/ml, respectively, and the proportions of patients with a level above the threshold for clinical response (≥ 1.0 μg/ml) at W54 were 60% and 80%, respectively. Given these findings, the lack of difference in disease activity at W54 in the 6 and 10 mg/kg dosing groups was likely due to the sufficiently high IFX levels observed even in high/high-C.
Upon comparing disease activity criteria between the three IFX dosing groups (3, 6, and 10 mg/kg), in each of the three classes, no significant difference was observed in low/low-C (p = 0.845 by Kruskal-Wallis test), whereas some degree of difference was observed in high/high-C (p = 0.183) and middle-C (p = 0.026). These findings suggest that dose escalation of IFX might not be clinically meaningful in low/low-C, most of whom maintained the threshold for clinical response. Dose escalation would therefore be more effective in middle-C and high/high-C.
In addition to baseline RF and anti-CCP titers, sex was found to be significantly correlated with IFX levels in W2 to W14; indeed, IFX levels tended to be higher in female than in male patients. However, baseline RF titers were significantly lower in female patients, and baseline TNF levels tended to be lower in female than in male patients (median 0.90 versus 1.03 pg/ml). In addition, the female-to-male ratio in high/high-C was lower than in low/low-C (data not shown). Differences in baseline RF and TNF levels and in female-to-male ratio among the classes might have contributed to the apparent correlations between sex and IFX levels.
Although details regarding the mechanism underlying the correlation between RF/anti-CCP and TNF levels are unknown, a previous in vitro study showed that anti-CCP induced the production of inflammatory cytokines in the synovial membrane and that this was amplified by RF [38]. This finding suggests that the induction of TNF production in the synovial membrane may elevate circulating TNF levels in patients with high RF/anti-CCP titers. In this study, RF and anti-CCP titers at W54 were significantly decreased in all three IFX dosing groups compared with those at W0 (Additional file 3), suggesting that a “vicious cycle” might exist in patients with RA whereby RF/anti-CCP promotes TNF production, which in turn contributes to further induction of RF/anti-CCP through an as yet unknown mechanism.
In the BeSt Study, patients who sustained drug-free remission were reported to have significantly lower baseline RF and anti-CCP titers than those who did not [39]. In patients in whom RF and anti-CCP titers returned to the normal range with IFX therapy, the aforementioned “vicious cycle” might have been stopped. This stop might enable tapering of IFX in these patients with RA (i.e., dose reduction or withdrawal). However, further study is needed to prove this hypothesis.
Some IFX biosimilars, which are available for rheumatological as well as dermatological and gastroenterological conditions in some countries, have been reported to show the same efficacy, safety, and pharmacokinetics as the IFX originator Remicade [40]. Therefore, our results might theoretically be applicable to these IFX biosimilars. However, we used only the IFX originator in this study, and further study is needed to confirm the adaptation.
Several limitations of this study warrant mention. The first and most critical limitation is that the upper detection limit for anti-CCP was 100 U/ml, and baseline anti-CCP titers were ≥ 100 U/ml in 58% of patients in this study. Because of this low upper limit, we could not stratify three classes using a “true second tertile” of anti-CCP (58% were stratified as anti-CCP-high), and analyses in patients with an extremely high anti-CCP titer were difficult. Second, we could not delineate each influence of RF or anti-CCP on TNF level, IFX levels, or disease activity, because RF and anti-CCP were significantly correlated (rho = 0.373, p < 0.0001) and resulted in the small numbers of patients with RF-high/anti-CCP-low or RF-low/anti-CCP-high. Third, TNF level could not be explained solely using RF and anti-CCP titers. Despite the significant correlation of RF/anti-CCP titers with TNF level, the correlation coefficients were low. In addition, TNF level was also significantly correlated with other baseline characteristics, such as DAS28-CRP, age, and IL-6 level. Accordingly, we cannot rule out the possibility that other factors besides RF/anti-CCP titers influenced the TNF level. Fourth, IFX levels may not actually be linked to baseline RF/anti-CCP titers, but may be linked to RF/anti-CCP titers at the point of measurement. Although both RF and anti-CCP titers were significantly reduced in all three dosing groups after IFX treatment (Additional file 3), both autoantibody levels at baseline and W54 were closely correlated in this study (rho = 0.819 for RF, rho = 0.871 for anti-CCP). In addition, IFX levels at W54 tended to be more strongly correlated with RF and anti-CCP titers at W54 than at W0 (data not shown). Under these conditions, some inaccuracy may exist when predicting clinical response on the basis of baseline RF/anti-CCP titers in certain patient populations, such as those showing extreme or no change of RF/anti-CCP titers regardless of their clinical response during IFX therapy. Allowing for these limitations, these findings will provide useful indices for IFX treatment strategy. However, given that the RISING study did not measure circulating autoantibodies other than RF and anti-CCP, future studies may be required to clarify the influence of other autoantibodies on IFX levels and clinical responses in patients with RA.
Conclusions
The findings of our present post hoc analysis of the RISING study demonstrated that baseline RF and anti-CCP titers are associated with both TNF level at baseline and IFX levels during subsequent IFX therapy, as well as that clinical responses are predictable to some degree before the start of IFX therapy. These findings will provide useful indices in implementing a strategy for long-term use of IFX in accordance with treat-to-target strategy [41, 42].
Abbreviations
- ATI:
-
Anti-infliximab antibody
- BMI:
-
Body mass index
- CCP:
-
Cyclic citrullinated peptide
- CRP:
-
C-reactive protein
- DAS28-CRP:
-
Disease Activity Score in 28 joints based on C-reactive protein
- DMARD:
-
Disease-modifying antirheumatic drug
- ELISA:
-
Enzyme-linked immunosorbent assay
- HAQ:
-
Health Assessment Questionnaire
- HDA:
-
High disease activity
- IFX:
-
Infliximab
- IL:
-
Interleukin
- LDA:
-
Low disease activity without clinical remission
- MDA:
-
Moderate disease activity
- MMP:
-
Matrix metalloproteinase
- MTX:
-
Methotrexate
- NSAID:
-
Nonsteroidal anti-inflammatory drug
- RA:
-
Rheumatoid arthritis
- REM:
-
Clinical remission
- RF:
-
Rheumatoid factor
- TNF:
-
Tumor necrosis factor
References
Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham III CO, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62:2569–81.
Neogi T, Aletaha D, Silman AJ, Naden RL, Felson DT, Aggarwal R, et al. The 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for rheumatoid arthritis: phase 2 methodological report. Arthritis Rheum. 2010;62:2582–91.
Lindqvist E, Eberhardt K, Bendtzen K, Heinegård D, Saxne T. Prognostic laboratory markers of joint damage in rheumatoid arthritis. Ann Rheum Dis. 2005;64:196–201.
Machold KP, Stamm TA, Nell VPK, Pflugbeil S, Aletaha D, Steiner G, et al. Very recent onset rheumatoid arthritis: clinical and serological patient characteristics associated with radiographic progression over the first years of disease. Rheumatology. 2007;46:342–9.
Maneiro RJ, Salgado E, Carmona L, Gomez-Reino JJ. Rheumatoid factor as predictor of response to abatacept, rituximab and tocilizumab in rheumatoid arthritis: systematic review and meta-analysis. Semin Arthritis Rheum. 2013;43:9–17.
Nüßlein HG, Alten R, Galeazzi M, Lorenz HM, Nurmohamed MT, Bensen WG, et al. Prognostic factors for abatacept retention in patients who received at least one prior biologic agent: an interim analysis from the observational, prospective ACTION study. BMC Musculoskelet Disord. 2015;16:176.
Gottenberg JE, Ravaud P, Cantagrel A, Combe B, Flipo RM, Schaeverbeke T, et al. Positivity for anti-cyclic citrullinated peptide is associated with a better response to abatacept: data from the ‘Orencia and Rheumatoid Arthritis’ registry. Ann Rheum Dis. 2012;71:1815–9.
Isaacs JD, Cohen SB, Emery P, Tak PP, Wang J, Lei G, et al. Effect of baseline rheumatoid factor and anticitrullinated peptide antibody serotype on rituximab clinical response: a meta-analysis. Ann Rheum Dis. 2013;72:329–36.
Kawashiri SY, Kawakami A, Iwamoto N, Fujikawa K, Aramaki T, Tamai M, et al. In rheumatoid arthritis patients treated with tocilizumab, the rate of clinical disease activity index (CDAI) remission at 24 weeks is superior in those with higher titers of IgM-rheumatoid factor at baseline. Mod Rheumatol. 2011;21:370–4.
Gibbons LJ, Hyrich KL. Biologic therapy for rheumatoid arthritis: clinical efficacy and predictors of response. BioDrugs. 2009;23:111–24.
Emery P, Dörner T. Optimising treatment in rheumatoid arthritis: a review of potential biological markers of response. Ann Rheum Dis. 2011;70:2063–70.
Lv Q, Yin Y, Li X, Shan G, Wu X, Liang D, et al. The status of rheumatoid factor and anti-cyclic citrullinated peptide antibody are not associated with the effect of anti-TNFα agent treatment in patients with rheumatoid arthritis: a meta-analysis. PLoS One. 2014;9:e89442.
Potter C, Hyrich KL, Tracey A, Lunt M, Plant D, Symmons DPM, et al. Association of rheumatoid factor and anti-cyclic citrullinated peptide positivity, but not carriage of shared epitope or PTPN22 susceptibility variants, with anti-tumour necrosis factor response in rheumatoid arthritis. Ann Rheum Dis. 2009;68:69–74.
Rycke LD, Verhelst X, Kruithof E, Van den Bosch F, Hoffman IEA, Veys EM, et al. Rheumatoid factor, but not anti-cyclic citrullinated peptide antibodies, is modulated by infliximab treatment in rheumatoid arthritis. Ann Rheum Dis. 2005;64:299–302.
Klaasen R, Cantaert T, Wijbrandts CA, Teitsma C, Gerlag DM, Out TA, et al. The value of rheumatoid factor and anti-citrullinated protein antibodies as predictors of response to infliximab in rheumatoid arthritis: an exploratory study. Rheumatology. 2011;50:1487–93.
Canhão H, Rodrigues AM, Mourão AF, Martins F, Santos MJ, Canas-Silva J, et al. Comparative effectiveness and predictors of response to tumour necrosis factor inhibitor therapies in rheumatoid arthritis. Rheumatology. 2012;51:2020–6.
Takeuchi T, Miyasaka N, Inoue K, Abe T, Koike T. Impact of trough serum level on radiographic and clinical response to infliximab plus methotrexate in patients with rheumatoid arthritis: results from the RISING study. Mod Rheumatol. 2009;19:478–87.
Takeuchi T, Miyasaka N, Tatsuki Y, Yano T, Yoshinari T, Abe T, et al. Baseline tumour necrosis factor alpha levels predict the necessity for dose escalation of infliximab therapy in patients with rheumatoid arthritis. Ann Rheum Dis. 2011;70:1208–15.
Sokolove J, Johnson DS, Lahey LJ, Wagner CA, Cheng D, Thiele GM, et al. Rheumatoid factor as a potentiator of anti-citrullinated protein antibody-mediated inflammation in rheumatoid arthritis. Arthritis Rheumatol. 2014;66:813–21.
Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315–24.
Fleischmann R, van der Heijde D, Koenig AS, Pedersen R, Szumski A, Marshall L, et al. How much does Disease Activity Score in 28 joints ESR and CRP calculations underestimate disease activity compared with the Simplified Disease Activity Index? Ann Rheum Dis. 2015;74:1132–7.
Inoue E, Yamanaka H, Hara M, Tomatsu T, Kamatani N. Comparison of Disease Activity Score (DAS)28- erythrocyte sedimentation rate and DAS28-C-reactive protein threshold values. Ann Rheum Dis. 2007;66:407–9.
Maini RN, Breedveld FC, Kalden JR, Smolen JS, Davis D, Macfarlane JD, et al. Therapeutic efficacy of multiple intravenous infusions of anti-tumor necrosis factor alpha monoclonal antibody combined with low-dose weekly methotrexate in rheumatoid arthritis. Arthritis Rheum. 1998;41:1552–63.
St Clair EW, Wagner CL, Fasanmade AA, Wang B, Schaible T, Kavanaugh A, et al. The relationship of serum infliximab concentrations to clinical improvement in rheumatoid arthritis: results from ATTRACT, a multicenter, randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2002;46:1451–9.
Rahman MU, Strusberg I, Geusens P, Berman A, Yocum D, Baker D, et al. Double-blinded infliximab dose escalation in patients with rheumatoid arthritis. Ann Rheum Dis. 2007;66:1233–8.
Lipsky PE, van der Heijde DMFM, St Clair EW, Furst DE, Breedveld FC, Kalden JR, et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. N Engl J Med. 2000;343:1594–602.
St Clair EW, van der Heijde DMFM, Smolen JS, Maini RN, Bathon JM, Emery P, et al. Combination of infliximab and methotrexate therapy for early rheumatoid arthritis: a randomized, controlled trial. Arthritis Rheum. 2004;50:3432–43.
Westhovens R, Yocum D, Han J, Berman A, Strusberg I, Geusens P, et al. The safety of infliximab, combined with background treatments, among patients with rheumatoid arthritis and various comorbidities: a large, randomized, placebo-controlled trial. Arthritis Rheum. 2006;54:1075–86.
Nam JL, Winthrop KL, van Vollenhoven RF, Pavelka K, Valesini G, Hensor EMA, et al. Current evidence for the management of rheumatoid arthritis with biological disease-modifying antirheumatic drugs: a systematic literature review informing the EULAR recommendations for the management of RA. Ann Rheum Dis. 2010;69:976–86.
Marotte H, Miossec P. Biomarkers for prediction of TNFα blockers response in rheumatoid arthritis. Joint Bone Spine. 2010;77:297–305.
Buch MH, Seto Y, Bingham SJ, Bejarano V, Bryer D, White J, et al. C-reactive protein as a predictor of infliximab treatment outcome in patients with rheumatoid arthritis: defining subtypes of nonresponse and subsequent response to etanercept. Arthritis Rheum. 2005;52:42–8.
Takeuchi T, Miyasaka N, Inui T, Yano T, Yoshinari T, Abe T, et al. Prediction of clinical response after 1 year of infliximab therapy in rheumatoid arthritis based on disease activity at 3 months: posthoc analysis of the RISING study. J Rheumatol. 2015;42:599–607. A published erratum appears in J Rheumatol. 2015;42:905.
Petrovic-Rackov L, Pejnovic N. Clinical significance of IL-18, IL-15, IL-12 and TNF-alpha measurement in rheumatoid arthritis. Clin Rheumatol. 2006;25:448–52.
Klimiuk PA, Sierakowski S, Latosiewicz R, Cylwik B, Skowronski J, Chwiecko J. Serum cytokines in different histological variants of rheumatoid arthritis. J Rheumatol. 2001;28:1211–7.
Keyszer G, Lambiri I, Nagel R, Keysser C, Keysser M, Gromnica-Ihle E, et al. Circulating levels of matrix metalloproteinases MMP-3 and MMP-1, tissue inhibitor of metalloproteinases 1 (TIMP-1), and MMP-1/TIMP-1 complex in rheumatic disease: correlation with clinical activity of rheumatoid arthritis versus other surrogate markers. J Rheumatol. 1999;26:251–8.
van Schouwenburg PA, Rispens T, Wolbink GJ. Immunogenicity of anti-TNF biologic therapies for rheumatoid arthritis. Nat Rev Rheumatol. 2013;9:164–72.
Garcês S, Demengeot J, Benito-Garcia E. The immunogenicity of anti-TNF therapy in immune-mediated inflammatory diseases: a systematic review of the literature with a meta-analysis. Ann Rheum Dis. 2013;72:1947–55.
Laurent L, Anquetil F, Clavel C, Ndongo-Thiam N, Offer G, Miossec P, et al. IgM rheumatoid factor amplifies the inflammatory response of macrophages induced by the rheumatoid arthritis-specific immune complexes containing anticitrullinated protein antibodies. Ann Rheum Dis. 2015;74:1425–31.
Klarenbeek NB, van der Kooij SM, Güler-Yüksel M, van Groenendael JHLM, Han KH, Kerstens PJSM, et al. Discontinuing treatment in patients with rheumatoid arthritis in sustained clinical remission: exploratory analyses from the BeSt study. Ann Rheum Dis. 2011;70:315–9.
Dörner T, Kay J. Biosimilars in rheumatology: current perspectives and lessons learnt. Nat Rev Rheumatol. 2015;11:713–24.
Smolen JS, Breedveld FC, Burmester GR, Bykerk V, Dougados M, Emery P, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis. 2016;75:3–15.
Singh JA, Saag KG, Bridges Jr SL, Akl EA, Bannuru RR, Sullivan MC, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68:1–26.
Acknowledgements
The authors thank all the investigators who participated in the RISING study.
Funding
Mitsubishi Tanabe Pharma Corporation sponsored this clinical trial and was responsible for the collection and analysis of data.
Availability of data and materials
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
TT participated in the development of the study design, participated in the study as an investigator, analyzed and interpreted data, and wrote the manuscript with input from all the other coauthors. NM participated in the development of the study design, participated in the study as an investigator, interpreted data, and revised the manuscript. TI analyzed and interpreted the data, including the statistical analysis, and provided assistance with preparing the manuscript. TYano analyzed and interpreted the data, including the statistical analysis, and provided assistance with preparing the manuscript. TYoshinari participated in the development of the study design, analyzed and interpreted the data, and helped to revise the manuscript. TA participated in the development of the study design, participated in the study as an investigator, interpreted data, and revised the manuscript. TK participated in the development of the study design, participated in the study as an investigator, interpreted data, and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
The RISING study protocol was approved by each institution’s ethics committee between August and November 2005, and the study conducted in accordance with the Declaration of Helsinki and good clinical practice. Written informed consent was obtained from all patients. The institutional ethics committees granting approval (approval dates) were as follows: Asahi University Murakami Memorial Hospital (September 14, 2005); Asahikawa Medical University Hospital (September 26, 2005); Chiba University Hospital (September 20, 2005); Dohgo Spa Hospital (September 5, 2005); Dokkyo Medical University Hospital (September 26, 2005); Fujita Health University Hospital (September 28, 2005); Fukui General Hospital (August 26, 2005); Fukushima Daiichi Hospital (September 22, 2005); Hamamatsu University School of Medicine, University Hospital (October 6, 2005); Higashi Hiroshima Memorial Hospital (August 23, 2005); Hiroshima City Hospital (September 13, 2005); Hokkaido University Hospital (October 18, 2005); Japanese Red Cross Kitami Hospital (October 24, 2005); Japanese Red Cross Saitama Hospital (September 6, 2005); Jichi Medical University Hospital (September 16, 2005); Kagawa University Hospital (September 28, 2005); Kanazawa University Hospital (October 19, 2005); Kasumigaseki Urban Clinic (October 20, 2005); Keio University Hospital (October 20, 2005); Kitakyushu Municipal Medical Center (September 29, 2005); Kitasato University Hospital (September 21, 2005); Kobe University Hospital (November 16, 2005); Kondo Clinic of Rheumatology and Orthopedic Surgery (September 27, 2005); Kumamoto Orthopedic Hospital (September 21, 2005); Kyoto University Hospital (October 19, 2005); Kyushu University Hospital (October 27, 2005); Marunouchi Hospital (October 26, 2005); Matsubara Mayflower Hospital (September 14, 2005); Matsuyama Red Cross Hospital (September 14, 2005); Nagasaki University Hospital (September 20, 2005); National Hospital Organization Chiba East Hospital (September 13, 2005); National Hospital Organization Kyushu Medical Center (September 28, 2005); National Hospital Organization Mie Chuo Medical Center (September 1, 2005); National Hospital Organization Morioka National Hospital (October 4, 2005); National Hospital Organization Nagoya Medical Center (September 7, 2005); National Hospital Organization Osaka Minami Medical Center (September 30, 2005); National Hospital Organization Sagamihara National Hospital (September 21, 2005); Nihon University Itabashi Hospital (October 25, 2005); Niigata University Medical and Dental Hospital (October 4, 2005); Nippon Medical School Hospital (September 22, 2005); Ohta Nishinouchi Hospital (September 13, 2005); Oita University Hospital (September 13, 2005); Osaka City University Hospital (September 28, 2005); Osaka Red Cross Hospital (September 16, 2005); Osaka Rosai Hospital (September 15, 2005); Osaka University Hospital (October 18, 2005); Saiseikai Takaoka Hospital (October 17, 2005); Saitama Medical Center, Saitama Medical University (September 15, 2005); Saitama Medical University Hospital (September 27, 2005); Sapporo Medical University Hospital (November 10, 2005); Sapporo Social Insurance General Hospital (September 12, 2005); Sasebo Chuo Hospital (October 17, 2005); Seirei Hamamatsu General Hospital (September 12, 2005); Shimane University Hospital (September 20, 2005); Showa University Hospital (October 17, 2005); Taga General Hospital (September 22, 2005); University of Tokyo Hospital (September 22, 2005); Toho University Medical Center Ohashi Hospital (September 28, 2005); Toho University Omori Medical Center (October 25, 2005); Tokushima University Hospital (September 15, 2005); Tokyo Medical and Dental University Hospital of Medicine (September 26, 2005); Tokyo Metropolitan Ohtsuka Hospital (November 15, 2005); Tokyo Women’s Medical University Hospital (September 9, 2005); Tokyo Women’s Medical University Medical Center East (September 9, 2005); Tomishiro Central Hospital (August 15, 2005); Tsukuba University Hospital (September 13, 2005); University Hospital, University of Occupational and Environmental Health, Japan (September 13, 2005); Utazu Hama Clinic (October 7, 2005); Yamaguchi University Hospital (August 31, 2005); Yamanashi Prefectural Central Hospital (September 20, 2005); and Yamauchi Hospital (September 9, 2005).
Consent for publication
Not applicable.
Competing interests
TT has received grant support, consultant’s fees, and/or lecture fees from AbbVie GK, Asahi Kasei Medical, Asahi Kasei Pharma, Astellas Pharma, AstraZeneca K.K., AYUMI Pharmaceutical, Bristol-Myers K.K., Celltrion, Chugai Pharmaceutical, Daiichi Sankyo, Eisai, Eli Lilly Japan, Janssen Pharmaceutical K.K., Merck Serono, Mitsubishi Tanabe Pharma, Nippon Kayaku, Nippon Shinyaku, Novartis Pharma K.K., Pfizer Japan, Taisho Toyama Pharmaceutical, Takeda Pharmaceutical, and Teijin Pharma. TI, TYano, and TYoshinari are employees of Mitsubishi Tanabe Pharma. TK has received consultant’s fees and/or lecture fees from AbbVie GK, Astellas Pharma, Bristol-Myers K.K., Chugai Pharmaceutical, Daiichi Sankyo, Eisai, Eli Lilly Japan, Mitsubishi Tanabe Pharma, Pfizer Japan, Santen Pharmaceutical, Taisho Toyama Pharmaceutical, Teijin Pharma, and UCB Japan. NM and TA declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Distribution of RF and anti-CCP titers at week 0 in all patients (n = 307). (PDF 39 kb)
Additional file 2:
Stratification of patients based on RF and anti-CCP titers at week 0. (PDF 419 kb)
Additional file 3:
RF and anti-CCP titers at weeks 0, 30, and 54. (PDF 479 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Takeuchi, T., Miyasaka, N., Inui, T. et al. High titers of both rheumatoid factor and anti-CCP antibodies at baseline in patients with rheumatoid arthritis are associated with increased circulating baseline TNF level, low drug levels, and reduced clinical responses: a post hoc analysis of the RISING study. Arthritis Res Ther 19, 194 (2017). https://doi.org/10.1186/s13075-017-1401-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-017-1401-2