
Abstract
Background
Dosing in obese critically ill patients is challenging due to pathophysiological changes derived from obesity and/or critical illness, and it remains fully unexplored. This study estimated the micafungin probability of reaching adequate 24-h area under the curve (AUC0–24h)/minimum inhibitory concentration (MIC) values against Candida spp. for an obese/nonobese, critically ill/noncritically ill, large population.
Methods
Blood samples for pharmacokinetic analyses were collected from 10 critically ill nonobese patients, 10 noncritically ill obese patients, and 11 critically ill morbidly obese patients under empirical/directed micafungin treatment. Patients received once daily 100–150 mg micafungin at the discretion of the treating physician following the prescribing information and hospital guidelines. Total micafungin concentrations were determined by high-performance liquid chromatography (HPLC). Monte-Carlo simulations were performed and the probability of target attainment (PTA) was calculated using the AUC0–24/MIC cut-offs 285 (C. parapsilosis), 3000 (all Candida spp.), and 5000 (nonparapsilosis Candida spp.). Intravenous once-daily 100-mg, 150-mg, and 200-mg doses were simulated at different body weights (45, 80, 115, 150, and 185 kg) and age (30, 50, 70 and 90 years old). PTAs ≥ 90% were considered optimal. Fractional target attainment (FTA) was calculated using published MIC distributions. A dosing regimen was considered successful if the FTA was ≥ 90%.
Results
Overall, 100 mg of micafungin was once-daily administered for nonobese and obese patients with body mass index (BMI) ≤ 45 kg/m2 and 150 mg for morbidly obese patients with BMI > 45 kg/m2 (except two noncritically ill obese patients with BMI ~ 35 kg/m2 receiving 150 mg, and one critically ill patient with BMI > 45 kg/m2 receiving 100 mg). Micafungin concentrations in plasma were best described using a two-compartment model. Weight and age (but not severity score) were significant covariates and improved the model. FTAs > 90% were obtained against C. albicans with the 200 mg/24 h dose for all body weights (up to 185 kg), and with the 150 mg/24 h for body weights < 115 kg, and against C. glabrata with the 200 mg/24 h dose for body weights < 115 kg.
Conclusion
The lack of adequacy for the 100 mg/24 h dose suggested the need to increase the dose to 150 mg/24 h for C. albicans infections. Further pharmacokinetic/pharmacodynamic studies should address optimization of micafungin dosing for nonalbicans Candida infections.
Similar content being viewed by others

Background
Obesity, which is increasing at an alarming rate in developed countries, is a significant risk factor for nosocomial infections, especially following surgery due to the immune dysfunction associated with obesity [1]. In addition, pathophysiological changes in obese patients (e.g., reduced regional blood flow, altered cardiac output, increased fat and lean mass, etc.) might modify the pharmacokinetic/pharmacodynamic (PK/PD) profile of antimicrobials [2, 3]. On the other hand, critically ill patients also present pathophysiological changes (hepatic and/or renal dysfunction, hypoalbuminemia or increased capillary permeability, use of organ support modalities) that can alter antimicrobial clearance and volume of distribution [4]. Thus, dosing in obese critically ill patients is a challenging scenario for intensivists that has not been fully explored [5].
Micafungin is an echinocandin, a lipopeptide that exhibits concentration-dependent fungicidal activity against most species of Candida [6], and is licensed as a first-line treatment for invasive candidiasis [7]. The recently published study EUROBACT was conducted in 162 intensive care units (ICUs) in 24 countries. It showed that, among patients with candidemia, Candida albicans was the most frequent fungi isolated (57.1%), followed by Candida glabrata (15.3%), Candida parapsilosis (10.2%), and Candida tropicalis (6.1%) [8].
Altered serum concentrations of micafungin associated with morbid obesity in critically ill patients might impact the achievement of therapeutic drug exposures as defined by the area under the serum concentration curve over a 24-h period (AUC0–24h)/minimum inhibitory concentration (MIC), the pharmacodynamic index linked to clinical efficacy for micafungin [9, 10]. A previous study conducted by our group showed cumulative fraction responses > 90% for micafungin at the standard dose (100 mg) against C. albicans and C. glabrata in a special population of critically ill patients on continuous venovenous hemofiltration [11].
The aim of this study was to estimate the micafungin probability of achieving adequate AUC0–24h/MIC values against Candida spp. for a large population using Monte-Carlo simulations [10] and data from obese, critically ill, and morbidly obese critically ill patients treated with micafungin.
Methods
A pharmacokinetic study was carried out in patients under micafungin empirical or directed treatment for invasive candidiasis. The population consisted of 11 morbidly obese critically ill adult patients (from the Hospital Universitario La Paz, Madrid, Spain), 10 nonobese critically ill patients, and 10 obese noncritically ill patients (from the Hospital del Mar, Barcelona, Spain). Patients admitted to ICUs were those considered to be critically ill. The study protocol was approved by the Ethics Committee of the Hospital La Paz (Madrid, Spain) and the Hospital del Mar (Barcelona, Spain). Written informed consent was obtained from patients (or relatives if the patient was unable to provide due to their critical situation) before blood sampling.
Demographic and clinical data prior to initiation of antifungal treatment were collected. Severity (Simplified Acute Physiology Score (SAPS) II) [12], Sequential Organ Failure Assessment (SOFA) score [13], and risk for invasive candidiasis (Candida score) [14] (except for patients with microbiologically documented infections) were calculated. Patients received dosage regimens of once-daily 100 mg or 150 mg micafungin (Astellas Pharma S.A., Spain) diluted in 100 ml isotonic saline solution that was intravenously infused over 60 min at the discretion of the treating physician (following the prescribing information and hospital treatment guidelines). On day 3, blood samples were collected at baseline (predose) and after 1, 3, 5, 8, 18, and 24 h. Additional blood samples at day 0 and day 7 were collected when feasible.
Sample handling and storage
Blood samples were immediately placed on ice and centrifuged at 3000 rpm for 10 min. Following on, they were stored at −80 °C. The samples were transported by a commercial courier company to the Burns Trauma and Critical Care Research Centre, The University of Queensland, Australia, for further analysis.
Drug assay
Total micafungin concentrations in plasma were measured by a validated ultra-high-performance liquid chromatography (UHPLC)-tandem mass spectrometry (MS/MS) method, from 0.2 to 30 μg/ml, on a Shimadzu Nexera 2 UHPLC system coupled to a Shimadzu 8030+ triple quadruple mass spectrometer (Shimadzu, Kyoto, Japan) [15]. Clinical samples were assayed alongside plasma calibrators and quality controls and met batch acceptance criteria [16].
Generation of large population data
Population pharmacokinetic modeling
To describe total micafungin concentrations, one- and two-compartment models were developed with the nonparametric adaptive grid algorithm within the freely available Pmetrics software package for R (Los Angeles, CA, USA) [17, 18]. Elimination from the central compartment, and intercompartmental distribution into the peripheral compartment (two-compartment model), were modeled as first-order processes. The discrimination between different models resulted from the comparison of the −2 log-likelihood (−2LL). A p value of < 0.05 was considered statistically significant.
Population pharmacokinetics covariate screening
Age, gender, body weight, body mass index (BMI), Acute Physiology and Chronic Health Evaluation (APACHE) II, serum creatinine concentration, measured creatinine clearance, Cockroft-Gault estimated creatinine clearance, and serum albumin concentration were evaluated as covariates. Covariate selection was performed using a stepwise linear regression from R on all covariates and Bayesian posterior parameters. Potential covariates were separately entered into the model and statistically tested by use of the –2LL values. If inclusion of the covariate resulted in a statistically significant improvement in the LL values (p < 0.05) and in an improvement of the goodness-of-fit plots, then the covariate was retained in the final model.
Model diagnostics
Goodness-of-fit was assessed by linear regression, with an observed-predicted plot, coefficients of determination, and LL values. Predictive performance evaluation was based on mean error of prediction (bias) and mean bias-adjusted squared error of prediction (imprecision) of the population and individual prediction models. The internal validity of the population pharmacokinetic model was assessed by the bootstrap resampling method (n = 1000) and normalized prediction distribution errors (NPDE) [19]. Using a visual predictive check method, parameters obtained from the bootstrap method were plotted with the observed concentrations. NPDE plots were checked for normal distribution characteristics and trends in data errors [19].
Probability of target attainment (PTA)
Monte-Carlo simulations (n = 1000) were employed using Pmetrics software to determine the PTA of achieving the PK/PD target of AUC0–24/MIC (285 for C. parapsilosis, 3000 for all Candida spp., and 5000 for nonparapsilosis Candida spp.) [11] for varying MICs (0.008 to 1 μg/ml). Intravenous once-daily doses of 100 mg, 150 mg, and 200 mg were simulated at different body weight (45, 80, 115, 150, and 185 kg) and age (30, 50, 70, and 90 years old). PTAs ≥ 90% were considered optimal.
Fractional target attainment (FTA) calculation
Published MIC distribution data of C. parapsilosis, nonparapsilosis Candida spp., and all Candida spp. from the SENTRY study [20] were used to determine the FTA, which identifies the potential success of the treatment by comparing the pharmacodynamic exposure (i.e, PTA) against an MIC distribution. Specifically, PTA values determined at each MIC were multiplied by the fraction of isolates found at that MIC, and the sum of the products equaled the FTA. A value of FTA ≥ 90% against a population of organisms was considered optimal.
Statistical analysis
Correlations were assessed by means of scatter graphs and the Pearson correlation coefficient (r).
Results
Table 1 shows the demographic data, baseline analytical parameters, and clinical scores for the patients distributed by obese/nonobese and critically/noncritically ill categorization. Overall, the standard 100-mg dose of micafungin was once-daily administered for nonobese and obese patients with BMI ≤ 45 kg/m2. The 150-mg dose was administered for morbidly obese patients with BMI > 45 kg/m2, with the exception of two noncritically ill obese patients with BMI of around 35 kg/m2 who received the 150-mg dose, and one critically ill patient with BMI > 45 kg/m2 who received the 100-mg dose.
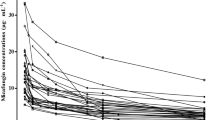
Figure 1 shows the mean observed concentration-time profile of micafungin concentrations for the study population.

Micafungin concentrations. Mean observed micafungin concentration-time profiles (error bars represent standard deviation)
Pharmacokinetic model
A two-compartment linear model (including zero order input of drug into the central compartment) best described the time course of 242 total plasma concentrations of micafungin. The goodness-of-fit of the model was improved (p < 0.05) by the inclusion of the covariate body weight (normalized to 70 kg) and age (normalized to 60 years old to an exponential value of 0.75) for micafungin clearance. Use of this exponent on age improved the model better than either covariate added as a linear function alone and reflected the likely nonlinear effect of the increasing body weight and age on micafungin clearance. Addition of body weight or age alone did not statistically improve the model when compared with the structural model (− 2LL value, 595.2 vs 596.4 for weight inclusion, p = 0.0586; 587.5 vs 596.4 for age inclusion, p = 0.597). When both the covariates body weight and age were included, the log likelihood value decreased significantly (−2LL, 415.6; p = 0.0238) and the goodness-of-fit of the model also showed an improvement. The final covariate model was as follows:
Where TVCL is the typical value of micafungin clearance, Wt is the total body weight (kg) and Age is the patient’s age (years).
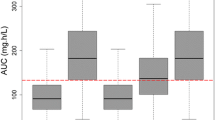
The mean ± standard deviation (SD) population pharmacokinetic parameter estimates for the final covariate model are shown in Table 2. The diagnostic plots confirmed the appropriateness of the model as shown in Fig. 2. The final covariate model was then used for Monte-Carlo dosing simulations.

Diagnostic plots for the final population pharmacokinetic covariate model. a Observed micafungin concentrations versus population predicted concentrations. b Observed micafungin concentrations versus individual predicted concentrations. c Visual predictive check (circles represent observed data). Concentrations are expressed as μg/ml
Dosing simulations
PTAs for AUC0–24/MIC of 285, 3000, or 5000 for different micafungin doses (100 mg, 150 mg, 200 mg) and body weights (from 45 kg to 185 kg) for patients with a medium age of 70 years old (no significant changes were observed in simulations with different patient ages) are described in Table 3. The Monte-Carlo simulations showed that increases in the micafungin dose resulted in increased PTAs. For nonparapsilosis Candida (AUC/MIC > 5000) this target attainment was only obtained with > 90% probability with doses of 150 mg and 200 mg against isolates with MICs up to 0.008 μg/ml, regardless of the patient’s weight.
FTAs for the simulated PTAs against MIC distributions for C. albicans, C. glabrata, C. parapsilosis, and C. tropicalis are shown in Table 4. FTAs > 90% were obtained against C. albicans with the 200 mg/24 h dose for all body weights, and with the 150 mg/24 h dose for body weights of 45 kg, 80 kg, and 115 kg, and against C. glabrata for body weights of 45 kg, 80 kg, and 115 kg with the 200 mg/24 h dose. No FTAs > 90% were obtained with the 100 mg/24 h dose regardless of the species or the patient’s weight.
Discussion
The present Monte-Carlo simulation using data from obese, critically ill, and morbidly obese critically ill patients treated with micafungin estimated the micafungin probability of achieving adequate AUC0–24h/MIC values against Candida spp. for a large population. Our results showed the lack of adequate micafungin exposure (in terms of FTAs) with the 100 mg/24 h dose regardless of the Candida species or the patient’s weight. Against C. albicans, micafungin exposure was adequate with the 150 mg/24 h dose for patients weighing up to 115 kg and with the 200 mg/24 h dose for those surpassing such a weight.
As in previous studies, plasma concentrations of micafungin were best described using a two-compartment model and, as mentioned, weight was a significant covariate [21]. Unlike the introduction of the severity score as a covariate, introducing the patient’s age improved the model. The influence of severity scores on micafungin exposure in severely ill patients is controversial among studies in the literature; while one study considered SOFA as a relevant covariate [22], another study did not find a correlation of APACHE II or SOFA with exposure, suggesting the possibility of being ruled out as a cause of low drug exposure [23]. The reason for this could be the high interindividual variability found in studies investigating micafungin exposure in critically ill patients [23,24,25] in contrast to data from healthy volunteers or patients under continuous venovenous hemofiltration [11, 24], which represent more uniform populations.
On the contrary, weight has been described as markedly influencing micafungin clearance [21] both in patients weighing > 66.3 kg [26] and in healthy volunteers in a study including subjects with BMI < 25, 25–40, and > 40 kg/m2 [27, 28]. In the present simulation, the inclusion of weight as a covariate improved the model. According to the results of our model, for MIC values > 0.008 μg/ml, the 100 mg/24 h dose failed to achieve the optimal ratio threshold of AUC0–24h/MIC of 3000. This cut-off was associated with therapeutic outcome in animal models for disseminated candidiasis by C. albicans [29], and it was extrapolated to humans [9] using data from clinical trials of invasive candidiasis/candidemia [30]. The increase in micafungin exposure provided by the doses of 150 or 200 mg/24 h markedly improved the coverage encompassing MICs of 0.016 μg/ml for body weights up to 80 kg (with the 150 mg/24 h dose) or for all body weights (200 mg/24 h dose). When considering recent MIC distributions for C. albicans, the most frequent isolated species, our results indicate that, to obtain adequate coverage (FTA ≥ 90%), the micafungin dose should be increased to 150 mg/24 h for nonobese patients (≤ 115 kg) and to 200 mg/24-h for those with body weight > 115 kg. This finding is consistent with previous reports showing the need for an increase in doses of antifungals in obese patients [5, 15, 31, 32] due to inadequate exposure with standards doses, as described with micafungin [26, 33]. In this sense, there is a report suggesting inadequate exposure with micafungin 100 mg/24 h in an obese critically ill patient weighing 230 kg [34]. Exposure may be crucial in morbidly obese critically ill patients when compared with the ICU population or obesity alone [32]. A timely and sufficiently high exposure to the appropriate antifungal agent is essential for the eradication of the pathogen. This acquires importance since, worldwide, mean weight, both in men and women, has been increasing over the last decades. In the USA, during 2013 and 2014, the overall age-adjusted prevalence of obesity was 37.7% [35].
Increasing the dose to 200 mg/24 h would overcome the problem caused by being overweight for C. albicans; however, such an increase would not solve the problem for other Candida species, requiring higher exposures. Since a previous study indicated that the maximum tolerated dose of micafungin in patients undergoing hematopoietic stem cell transplantation was at least up to 8 mg/kg/24 h [36], strategies including individualized dosing have been advocated as a great opportunity to further improve the efficacy of micafungin [27], an antifungal with reported 70–80% efficacy in the treatment of candidemia with the current dosing of 100 mg/24 h [27, 30, 37, 38].
The results of this study are of high importance due to the very limited information available on the pharmacokinetics and efficacy of echinocandins in obese critically ill patients, especially in those with morbid obesity. Most studies have been performed with caspofungin. In agreement with our results, pharmacokinetic studies with caspofungin showed lower exposure in overweight and obese patients, whether critically ill [39] or not [40], and also showed the benefits of increasing the dose in morbidly obese patients [41]. Similarly, the limited data in the literature regarding the influence of obesity on the pharmacokinetics of anidulafungin confirm the lower anidulafungin exposure in patients with morbid obesity compared with nonobese patients [32] and the need for increasing the dose in a critically ill morbid obese patient [42].
The present study is the first population assessment of micafungin in critically ill nonobese, noncritically ill obese, and critically ill morbidly obese patients. Several limitations and challenges must be kept in mind in this respect. Despite the relatively large sample size in this study, the distribution of patients resulted in a low number of individuals in some of the groups. In addition, the present study is a pharmacodynamic modeling not designed to examine the effect of micafungin exposure on patient outcome; clinical trials should address this issue from a clinical perspective.
Conclusion
The results of this study indicate that micafungin exposure was adequate with the 150 mg/24 h dose for patients weighing up to 115 kg and with the 200 mg/24 h dose for those surpassing such weight to cover C. albicans. The 200 mg/24 h dose covered C. glabrata for patients weighing up to 115 kg. Since other species of Candida were not successfully covered, further PK/PD studies should address this point to optimize dosing for nonalbicans Candida infections.
Abbreviations
- APACHE:
-
Acute Physiology and Chronic Health Evaluation
- AUC:
-
Area under the curve
- BMI:
-
Body mass index
- FTA:
-
Fractional target attainment
- ICU:
-
Intensive care unit
- LL:
-
Log-likelihood
- MIC:
-
Minimum inhibitory concentration
- MS/MS:
-
Tandem mass spectrometry
- NPDE:
-
Normalized prediction distribution errors
- PK/PD:
-
Pharmacokinetic/pharmacodynamic
- PTA:
-
Probability of target attainment
- SAPS:
-
Simplified Acute Physiology Score
- SD:
-
Standard deviation
- SOFA:
-
Sequential Organ Failure Assessment
- UHPLC:
-
Ultra-high-performance liquid chromatography
References
Milner JJ, Beck MA. The impact of obesity on the immune response to infection. Proc Nutr Soc. 2012;71:298–306.
Knibbe CA, Brill MJ, van Rongen A, Diepstraten J, van der Graaf PH, Danhof M. Drug disposition in obesity: toward evidence-based dosing. Annu Rev Pharmacol Toxicol. 2015;55:149–67.
Jain R, Chung SM, Jain L, Khurana M, Lau SW, Lee JE, et al. Implications of obesity for drug therapy: limitations and challenges. Clin Pharmacol Ther. 2011;90:77–89.
Roberts JA, Lipman J. Pharmacokinetic issues for antibiotics in the critically ill patient. Crit Care Med. 2009;37:840–51.
Alobaid AS, Hites M, Lipman J, Taccone FS, Roberts JA. Effect of obesity on the pharmacokinetics of antimicrobials in critically ill patients: a structured review. Int J Antimicrob Agents. 2016;47:259–68.
Chandrasekar PH, Sobel JD. Micafungin: a new echinocandin. Clin Infect Dis. 2006;42:1171–8.
Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Executive summary: clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62:409–17.
Paiva JA, Pereira JM, Tabah A, Mikstacki A, de Carvalho FB, Koulenti D, et al. Characteristics and risk factors for 28-day mortality of hospital acquired fungemias in ICUs: data from the EUROBACT study. Crit Care. 2016;20:53.
Andes D, Ambrose PG, Hammel JP, Van Wart SA, Iyer V, Reynolds DK, et al. Use of pharmacokinetic-pharmacodynamic analyses to optimize therapy with the systemic antifungal micafungin for invasive candidiasis or candidemia. Antimicrob Agents Chemother. 2011;55:2113–21.
Turnidge J, Paterson DL. Setting and revising antibacterial susceptibility breakpoints. Clin Microbiol Rev. 2007;20:391–408.
Maseda E, Grau S, Villagran MJ, Hernandez-Gancedo C, Lopez-Tofiño A, Roberts JA, et al. Micafungin pharmacokinetic/pharmacodynamic adequacy for the treatment of invasive candidiasis in critically ill patients on continuous venovenous haemofiltration. J Antimicrob Chemother. 2014;69:1624–32.
Le Gall JR, Lemeshow S, Saulnier F. A new simplified acute physiologic score (SAPS-II) based on a European/North-American multicenter study. JAMA. 1993;270:2957–63.
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996;22:707–10.
León C, Ruiz-Santana S, Saavedra P, Almirante B, Nolla-Salas J, Alvarez-Lerma F, et al. A bedside scoring system (“Candida score”) for early antifungal treatment in nonneutropenic critically ill patients with Candida colonization. Crit Care Med. 2006;34:730–7.
Alobaid AS, Wallis SC, Jarrett P, Starr T, Stuart J, Lassig-Smith M, et al. Population pharmacokinetics of piperacillin in nonobese, obese, and morbidly obese critically ill patients. Antimicrob Agents Chemother. 2017;61:e01276–316.
Food and Drug Administration. Guidance for industry: bioanalytical method validation. Rockville: U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Center for Veterinary Medicine (CVM); 2001.
Tatarinova T, Neely M, Bartroff J, van Guilder M, Yamada W, Bayard D, et al. Two general methods for population pharmacokinetic modelling: non-parametric adaptive grid and non-parametric Bayesian. J Pharmacokinet Pharmacodyn. 2013;40:189–99.
Neely MN, van Guilder MG, Yamada WM, Schumitzky A, Jelliffe RW. Accurate detection of outliers and subpopulations with Pmetrics, a nonparametric and parametric pharmacometric modeling and simulation package for R. Ther Drug Monit. 2012;34:467–76.
Mentré F, Escolano S. Prediction discrepancies for the evaluation of nonlinear mixed-effects models. J Pharmacokinet Pharmacodyn. 2006;33:345–67.
Pfaller MA, Messer SA, Woosley LN, Jones RN, Castanheira M. Echinocandin and triazole antifungal susceptibility profiles for clinical opportunistic yeast and mold isolates collected from 2010 to 2011: application of new CLSI clinical breakpoints and epidemiological cutoff values for characterization of geographic and temporal trends of antifungal resistance. J Clin Microbiol. 2013;51:2571–81.
Wasmann RE, Muilwijk EW, Burger DM, Verweij PE, Knibbe CA, Brüggemann RJ. Clinical pharmacokinetics and pharmacodynamics of micafungin. Clin Pharmacokinet. 2017; https://doi.org/10.1007/s40262-017-0578-5. [Epub ahead of print].
Jullien V, Azoulay E, Schwebel C, Le Saux T, Charles PE, Cornet M, et al. Population pharmacokinetics of micafungin in ICU patients with sepsis and mechanical ventilation. J Antimicrob Chemother. 2017;72:181–9.
Lempers VJ, Schouten JA, Hunfeld NG, Colbers A, van Leeuwen HJ, Burger DM, et al. Altered micafungin pharmacokinetics in intensive care unit patients. Antimicrob Agents Chemother. 2015;59:4403–9.
Martial LC, Ter Heine R, Schouten JA, Hunfeld NG, van Leeuwen HJ, Verweij PE, et al. Population pharmacokinetic model and pharmacokinetic target attainment of micafungin in intensive care unit patients. Clin Pharmacokinet. 2017; https://doi.org/10.1007/s40262-017-0509-5. [Epub ahead of print].
Chang CC, Slavin MA, Chen SC. New developments and directions in the clinical application of the echinocandins. Arch Toxicol. 2017;91:1613–21.
Gumbo T, Hiemenz J, Ma L, Keirns JJ, Buell DN, Drusano GL. Population pharmacokinetics of micafungin in adult patients. Diagn Microbiol Infect Dis. 2008;60:329–31.
Hall RG, Swancutt MA, Gumbo T. Fractal geometry and the pharmacometrics of micafungin in overweight, obese, and extremely obese people. Antimicrob Agents Chemother. 2011;55:5107–12.
Pasipanodya JP, Hall RG 2nd, Gumbo T. In silico-derived bedside formula for individualized micafungin dosing for obese patients in the age of deterministic chaos. Clin Pharmacol Ther. 2015;97:292–7.
Andes D, Diekema DJ, Pfaller MA, Bohrmuller J, Marchillo K, Lepak A. In vivo comparison of the pharmacodynamic targets for echinocandin drugs against Candida species. Antimicrob Agents Chemother. 2010;54:2497–506.
Kuse ER, Chetchotisakd P, da Cunha CA, Ruhnke M, Barrios C, Raghunadharao D, et al. Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet. 2007;369:1519–27.
Alobaid AS, Wallis SC, Jarrett P, Starr T, Stuart J, Lassig-Smith M, et al. Effect of obesity on the population pharmacokinetics of fluconazole in critically ill patients. Antimicrob Agents Chemother. 2016;60:6550–7.
Lempers VJ, van Rongen A, van Dongen EP, van Ramshorst B, Burger DM, Aarnoutse RE, et al. Does weight impact anidulafungin pharmacokinetics? Clin Pharmacokinet. 2016;55:1289–94.
Yang Q, Wang T, Xie J, Wang Y, Zheng X, Chen L, et al. Pharmacokinetic/pharmacodynamic adequacy of echinocandins against Candida spp. in intensive care unit patients and general patient populations. Int J Antimicrob Agents. 2016;47:397–402.
Zomp A, Bookstaver PB, Ahmed Y, Turner JE, King C. Micafungin therapy in a critically ill, morbidly obese patient. J Antimicrob Chemother. 2011;66:2678–80.
Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in obesity among adults in the United States, 2005 to 2014. JAMA. 2016;315:2284–91.
Sirohi B, Powles RL, Chopra R, Russell N, Byrne JL, Prentice HG, et al. A study to determine the safety profile and maximum tolerated dose of micafungin (FK463) in patients undergoing haematopoietic stem cell transplantation. Bone Marrow Transplant. 2006;38:47–51.
Pappas PG, Rotstein CM, Betts RF, Nucci M, Talwar D, De Waele JJ, et al. Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis. 2007;45:883–93.
Goto N, Hara T, Tsurumi H, Ogawa K, Kitagawa J, Kanemura N, et al. Efficacy and safety of micafungin for treating febrile neutropenia in hematological malignancies. Am J Hematol. 2010;85:872–6.
Nguyen TH, Hoppe-Tichy T, Geiss HK, Rastall AC, Swoboda S, Schmidt J, et al. Factors influencing caspofungin plasma concentrations in patients of a surgical intensive care unit. J Antimicrob Chemother. 2007;60:100–6.
Hall RG, Swancutt MA, Meek C, Leff R, Gumbo T. Weight drives caspofungin pharmacokinetic variability in overweight and obese people: fractal power signatures beyond two-thirds or three-fourths. Antimicrob Agents Chemother. 2013;57:2259–64.
Ferriols-Lisart R, Aguilar G, Pérez-Pitarch A, Puig J, Ezquer-Garín C, Alós M. Plasma concentrations of caspofungin in a critically ill patient with morbid obesity. Crit Care. 2017;21:200.
Liu P, Ruhnke M, Meersseman W, Paiva JA, Kantecki M, Damle B. Pharmacokinetics of anidulafungin in critically ill patients with candidemia/ invasive candidiasis. Antimicrob Agents Chemother. 2013;57:1672–6.
Acknowledgements
The authors thank A. López-Tofiño and C. Hernández Gancedo (Department of Anesthesia and Surgical Intensive Care, Hospital Universitario La Paz, Madrid, Spain) for their support during the study, and L. Aguilar (PRISM-AG) for his critical review of the manuscript.
Funding
This work was supported in part by an unrestricted grant from Astellas Pharma S.A. (Madrid, Spain). The funder had no role in the study design, data collection and interpretation, or the decision to submit the work for publication. JAR is funded by a Career Development Fellowship from the National Health and Medical Research Council of Australia (APP1048652).
Availability of data and materials
Data from patients are recorded in their corresponding medical records at participating hospitals. The anonymous datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request and with permission of the corresponding hospital.
Author information
Authors and Affiliations
Contributions
EM, SG, and JAR designed the study. EM, M-PC-M, AS-d-l-R, AM-F, CAG-B, and FG collected data. SG, SL, and JAR analyzed blood samples and analyzed data. EM, SG, JAR, and M-JG analyzed results and prepared the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Hospital La Paz (Madrid, Spain) and Hospital del Mar (Barcelona, Spain). Written informed consent was obtained from patients (or relatives if the patient was unable to provide due to their critical situation) before blood sampling.
Competing interests
EM has received consultancy fees and payment for lectures from Astellas Pharma S.A. (Madrid, Spain), Pfizer, Novartis, Angellini, and Merck Sharp and Dohme. SG has received grants for research from Astellas Pharma S.A. (Madrid, Spain), Pfizer, Roche Pharma, and Angelini Pharma, and funds for speaking at symposia organized by Pfizer, Astellas Pharma S.A., and Merck Sharp and Dohme. SL has received travel grants from Astellas Pharma for medical conference attendance. CAG-B has received travel grants from Astellas Pharma for Sepsis Valladolid 2014 Congress attendance. The remaining authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Maseda, E., Grau, S., Luque, S. et al. Population pharmacokinetics/pharmacodynamics of micafungin against Candida species in obese, critically ill, and morbidly obese critically ill patients. Crit Care 22, 94 (2018). https://doi.org/10.1186/s13054-018-2019-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-018-2019-8