
Abstract
Background
An improved prehospital diagnostic accuracy of cardiogenic pulmonary oedema could potentially improve initial treatment, triage, and outcome. A pilot study was conducted to assess the feasibility, time-use, and diagnostic accuracy of prehospital lung ultrasound (PLUS) for the diagnosis of cardiogenic pulmonary oedema.
Methods
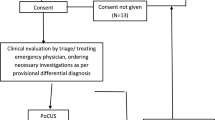
A prospective observational study was conducted in a prehospital setting. Patients were included if the physician based prehospital mobile emergency care unit was activated and one or more of the following two were present: respiratory rate >30/min., oxygen saturation <90 %. Exclusion criteria were: age <18 years, permanent mental disability or PLUS causing a delay in life-saving treatment or transportation. Following clinical assessment PLUS was performed and presence or absence of interstitial syndrome was registered. Audit by three physicians using predefined diagnostic criteria for cardiogenic pulmonary oedema was used as gold standard.
Results
A total of 40 patients were included in the study. Feasibility of PLUS was 100 % and median time used was 3 min. The gold standard diagnosed 18 (45.0 %) patients with cardiogenic pulmonary oedema. The diagnostic accuracy of PLUS for the diagnosis of cardiogenic pulmonary oedema was: sensitivity 94.4 % (95 % confidence interval (CI) 72.7–99.9 %), specificity 77.3 % (95 % CI 54.6–92.2 %), positive predictive value 77.3 % (95 % CI 54.6–92.2 %), negative predictive value 94.4 % (95 % CI 72.7–99.9 %).
Discussion
The sensitivity of PLUS is high, making it a potential tool for ruling-out cardiogenic pulmonary. The observed specificity was lower than what has been described in previous studies.
Conclusions
Performed, as part of a physician based prehospital emergency service, PLUS seems fast and highly feasible in patients with respiratory failure. Due to its diagnostic accuracy, PLUS may have potential as a prehospital tool, especially to rule out cardiogenic pulmonary oedema.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Lung ultrasound (LUS) has over the last 20 years undergone a rapid development. From the viewpoint that the lung was an organ that ultrasound could not be used to investigate, several studies have shown that LUS can be used for a variety of the most common diagnosis seen in emergency medicine and traumatology [1, 2]. The prehospital physician faces the difficult task of differentiating between pulmonary and cardiac causes of acute respiratory failure using only history and physical examination [3]. One way to distinguish between cardiac and pulmonary causes of dyspnoea is to diagnose the presence of pulmonary oedema. Cardiogenic pulmonary oedema can with LUS be visualized as a characteristic pattern, the interstitial syndrome (IS) [1, 4, 5]. Other conditions such as non-cardiogenic pulmonary oedema, interstitial lung disease, acute respiratory distress syndrome, interstitial pneumonia can however also present itself as IS [1]. In emergency settings cardiogenic pulmonary oedema is however the most common cause of non-traumatic respiratory failure, the finding of IS has thus pragmatically been interpreted as being consistent with cardiogenic pulmonary oedema [4, 6]. This pragmatic assumption has been validated in an emergency department setting [5, 7]. Using this assumption LUS has been shown to have a high diagnostic accuracy for the diagnosis of cardiogenic pulmonary oedema which surpasses history taking, clinical examination, blood samples and chest x-ray [5]. Prehospital LUS (PLUS) to diagnose and exclude pulmonary oedema is partly described in a single case report and partly in a single prospective observational study [8, 9]. Additionally PLUS has been assessed as a possible monitoring tool for prehospital treatment of cardiogenic pulmonary oedema [10]. The results suggest that PLUS have a high diagnostic accuracy for the diagnosis of cardiac pulmonary oedema. Based on the above, some of the potential benefits of PLUS for assessing patients with acute respiratory failure are an increased prehospital diagnostic accuracy of cardiogenic pulmonary oedema, improved prehospital treatment of these patients, and earlier and more accurate notification of the receiving facility. A prospective pilot study was conducted with the primary aim to assess the feasibility of prehospital LUS in patients with signs of respiratory failure. Secondary aims were to assess time-use, and diagnostic accuracy for cardiogenic pulmonary oedema.
Methods
Setting and study population
The study was conducted as a prospective cross-sectional study of patients with respiratory failure in which Mobile Emergency Care Unit (MECU) in Odense, Denmark, was activated. The MECU in Odense consists of a rapid-response car operating all year round, 24/7. The car is manned with a specially trained emergency medicine technician and a physician with specialist training in anaesthesiology. Twelve physicians are employed at the MECU. The MECU operates as part of a two-tiered system, in which it supplements ambulances manned with either two emergency medicine technicians or an emergency medicine technician and a paramedic. The MECU covers an area of approximately 2500 square km and serves a population of 250,000 to 490,000 depending on time of the day. In average the MECU is dispatched to 4900 calls per year, corresponding to 13.5 calls per day. Patients with respiratory symptoms admitted to hospital by the MECU are either transported to the department of general emergency medicine or the department of cardiology, both located at Odense University Hospital, Denmark.
Inclusion and exclusion criteria
Patients were included if they fulfilled one or more of the following two signs of respiratory failure: (1) respiratory rate >30 breaths per minute or (2) peripheral oxygen saturation without supplementary oxygen treatment <90 %. Patients were excluded if they were below 18 years of age, if the treating physician deemed that PLUS would delay life-saving treatment or transportation, or if informed consent could not be obtained due to permanent mental disability.
Initial prehospital presumptive diagnosis and treatment
The result of the initial prehospital assessment including presumptive diagnosis and treatment initiated were prehospitally registered, encrypted and stored using an iPad. The data from the iPad were continuously transferred to a separate study database.
Prehospital lung ultrasound examination
PLUS was performed using a SonoSite Edge (Bothell, Washington, USA) ultrasound machine, with a microconvex transducer (C11X)(8-5 mHz). As soon as the patient had been included in the project, PLUS was performed. The prehospital physician was allowed to decide whether PLUS was made on-scene or en-route to the hospital. The PLUS examination was performed using a standardized protocol. Several different LUS protocols involving a wide range of scanning zones have been described [1]. In the present study a protocol based on a mixture of a protocol described by Volpicelli et al. for use in an emergency department setting and a protocol described by Lichtenstein et al. for use in an intensive care unit setting were used [6, 11]. The transducer was placed in two scanning zones (anterior and lateral) on each side of the patient’s chest. In each scanning zone it was then noted whether three or more B-lines were present or not. Based on the PLUS findings it was then determined whether the patient was positive or negative of having interstitial syndrome. IS was defined as the presence of three or more B-lines in a longitudinal plane between two ribs in two or more of scanning fields, bilaterally. This definition was based on the international consensus definition of IS, with the modification that the total number of scanning zones were limited to two per side, rather than four [1]. It was chosen to reduce the number of scanning zones in order to decrease time used for the examination. The results of the PLUS examination, time used, and whether the findings had altered treatment or the presumptive diagnosis were prehospitally registered using the same iPad and system as described above. Time used for PLUS was defined from the physician beginning to use the ultrasound machine (incl. preparing the machine for use) to the transducer leaving the skin of the patient after completing the examination. The department receiving the patient was informed that the patient had been included in the study but the result of the PLUS examination was blinded. Prior to the initiation of the project, a short training of all the physicians working at the physician based prehospital emergency service was performed. The training consisted of a theoretical lecture (45 min) as well as practical demonstration involving hands-on training of each physician (45 min). The physicians manning the MECU were all specialists in anaesthesiology and thus had basic competencies in ultrasound for invasive procedures such as nerve blocks and vascular access. A few of the physicians had competencies in transthoracic and transeosophageal echocardiography. Only one of the physicians were experienced in the use of lung ultrasound prior to the study.
Echocardiography
All included patients were as a part of the study referred for echocardiography performed by a cardiologist. This was done in order to systematically identify the enrolled patients’ cardiac status and to be able to identify any patients with heart failure who had not been diagnosed as IS positive.
Blinded audit
The presence or absence of cardiogenic pulmonary oedema was established using blinded audit. Two physicians (AH (cardiologist), SP (emergency medicine physician)) independently of each other audited the patient’s hospital stay. The two auditors used the following predefined criteria to determine whether cardiac pulmonary oedema was present or absent upon patient admission to the hospital. At least two of the following three criteria had to be met: (1) clinical signs of pulmonary oedema (e.g. increased ventilation rate, hypoxemia, bilateral crackles identified by auscultation), (2) imaging study with signs of pulmonary oedema (chest X-ray, computed tomography of the chest, LUS performed in the hospital) or (3) the patient was diagnosed with a diseases which can be complicated by pulmonary oedema (systolic heart failure as part of the acute coronary syndrome, systolic heart failure, non-systolic heart failure, hypertensive crisis, arrhythmia, heart valve disease). In case of disagreement on the presence/non-presence of cardiac pulmonary oedema between the two initial auditors, an additional audit was performed by a third auditor (LV (cardiologist)) thus making the final decision. All auditors were blinded towards the results of the PLUS examination. The predefined diagnostic criteria and audit method were based on two previously conducted studies of patients with respiratory symptoms admitted to an emergency department [7, 12].
Statistical analysis
Descriptive statistics of demographic characteristics, medical history, and initial vital signs were performed using numbers, percentages, median and interquartile-range (IQR). Descriptive statistics of the PLUS examination and its possible clinical impact were performed including site at which PLUS was performed, time used for PLUS, proportion of patients in which PLUS had altered treatment, or the prehospital presumptive diagnosis. The PLUS feasibility was calculated as the proportion of included patients in which PLUS could be performed according to the predefined ultrasound protocol. Agreement between the two initial auditors was calculated as a proportion and using the Cohen k test. The diagnostic accuracy of the initial prehospital presumptive diagnosis and PLUS for the diagnosis of cardiogenic pulmonary oedema were calculated. These calculations were expressed as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (PLR), negative likelihood ratio (NLR), and their 95 % confidence intervals (CI). Blinded audit diagnosis was used as reference test for all calculations. Data analysis was conducted using Stata Release version 11.0 (StataCorp LP).
Results
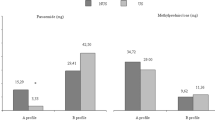
Between September 2013 and October 2014 a total of 45 patients were included in the study. Five patients included were excluded upon arrival at the ED were information from previous admissions revealed a diagnosis consistent with permanent mental disability. Forty patients remained for study analysis. Baseline characteristics of the included patients are provided in Table 1. Feasibility of PLUS was 100 % and median time used for the examination was 3 min (IQR 2–4 min). In all but one patient (97.5 %), the PLUS examination was performed on-scene prior to transportation of the patient [13]. The 40 PLUS examinations were performed by seven different physicians manning the MECU. In 27.5 % (95 % CI 13.0–42.0 %) of the patients PLUS findings led to a change in the prehospital presumptive diagnosis and in 22.5 % (95 % CI 9.0–36.0 %) it also led to a change in the initial prehospital treatment. Typical PLUS findings are shown in Fig. 1. The median transport time to the hospital was 10 min (IQR 5–15 min, range 4–20 min). Twenty-six (65.0 %) of the patients were admitted to the department of general emergency medicine, 13 (32.5 %) to the department of cardiology, and one (2.5 %) patient to the department of oncology. During the hospital stay, six (15.0 %) patients received non-invasive ventilation at the department of respiratory medicine and 3 (7.5 %) patients were transferred to the intensive care unit. The inhospital and 30-day mortality was 7.5 % (95 % CI 0–16.0 %) and 15 % (95 % CI 3.4–26.6 %) respectively. The most common abnormal echocardiography findings were: 14 (35 %) patients with systolic heart failure, eight (20 %) patients with mitral valve insufficiency and seven (17.5 %) patients with aortic valve stenosis. Other findings were a dilated right ventricle in five (12.5 %) patients and non-systolic heart failure in two (5 %) patients. The blinded audit diagnosed 18 (45.0 %) patients with cardiogenic pulmonary oedema. The overall agreement between the two initial auditors for the diagnosis of cardiogenic pulmonary oedema was 87.5 % (k 0.746). When stratified according to a audit diagnosis of presence or absence of cardiogenic pulmonary oedema, significantly more patients received treatment with nitroglycerin and diuretics in the cardiogenic pulmonary oedema group, whereas significantly more patients received bronchodilators and systemic steroids in the group in which cardiogenic pulmonary oedema was absent (Table 2). The contingency tables and diagnostic accuracy of the prehospital clinical assessment and PLUS for the diagnosis of cardiogenic pulmonary oedema are provided in Tables 3 and 4. No adverse events related to the PLUS examination were observed.

PLUS findings. a Image from a PLUS examination performed in a patient in which cardiogenic pulmonary oedema was absent. The pleuraline (PL) appears as a hyperechoic (white), horizontal line. No B-lines are present. b Image from a PLUS examination performed in a patient with cardiogenic pulmonary oedema. Multiple B-lines (arrows) are seen as hyperechoic (white), vertical, reverberation artefacts. The B-lines originate from the pleuraline (PL) and extends to the bottom of the field of view without fading
Discussion
In a population of patients with respiratory failure, PLUS was fast, highly feasible, and had an acceptable diagnostic accuracy for the diagnosis of cardiogenic pulmonary oedema. Especially the sensitivity of PLUS is high, making it an excellent tool for ruling-out cardiogenic pulmonary oedema, in the case of a PLUS examination with no signs of IS. The specificity was however somewhat lower and not better than the specificity of the clinical assessment. A single prehospital study and several studies conducted in an in-hospital setting have found LUS to have both a high sensitivity and specificity for the diagnosis of cardiogenic pulmonary oedema [5, 8, 11]. One possible explanation for the lower specificity found in this study might be the relatively high proportion of patients with other conditions which may also cause IS, as reflected by the proportion of patients in which the initial chest x-ray performed in the ED was described with pulmonary fibrosis or possible interstitial lung disease (Appendix, Table 6). Another possible reason for the lower specificity might be the limited level of training in PLUS prior to the study. Studies assessing the learning curve for focused LUS have however found LUS to have a step learning curve for the diagnosis of IS with a high diagnostic accuracy despite limited training [14, 15]. A third possible explanation may be the gold standard missing patients with cardiogenic pulmonary oedema since chest x-ray often was the only imaging modality used for pulmonary assessment in the patients. Several studies have found focused LUS to have a higher diagnostic accuracy than conventional chest x-ray for the diagnosis of cardiogenic pulmonary oedema [1, 5]. Additionally, in the time gap between PLUS and initial imaging at the hospital, the patient in most cases would have received treatment and thereby reduce the severity of the cardiogenic pulmonary oedema and thus the changes which could be visualized by chest x-ray in the ED. The transportation times were however relatively short and the diagnostic criteria used for the gold standard did not solely rely on imaging findings. Based on the k value, the agreement between the two auditors was substantial according to Fleiss’ guidelines [16]. The PLUS diagnostic criteria were based on the international definition of IS, using a definition in which multiple B-lines had to be present in all four scanning zones or in both of the two anterior zones might have improved the PLUS specificity [1]. As indicated in other studies, such a definition would however also have lead to a decreased sensitivity and thereby also affect PLUS’ utility as an efficient rule-out tool [17]. The PLUS protocol assessing two zones on each hemithorax was chosen in order to reduce the time used for the ultrasound examination. The median time use of 3 min corresponds to what has been reported using a three zone approach in an intensive care setting and the eight zone approach in an ED setting [6, 11]. The two zone approach did thus not seem to reduce ultrasound examination time when compared to a three or eight zone approach. This may however be due to fact that relatively experienced or specially trained physicians performed the LUS examinations in the other studies [6, 11]. A direct comparison of the time used for the different approaches performed by the same physicians is thus needed to assess whether there is a clinical significant time difference or not. When compared to the diagnostic accuracy of the prehospital clinical assessment, the clinical impact of using PLUS as a standard diagnostic test in patients with respiratory failure would be a fast and efficient means of ruling-out cardiogenic pulmonary oedema. This would have clinical important applications regarding several aspects. The use of inhaled bronchodilators in patients with cardiogenic pulmonary oedema is associated with a worse outcome [18]. In areas with long transportation times to the nearest hospital, PLUS could potentially be used to monitor treatment response during the transportation [10]. Prehospital ultrasound of trauma patient seems to have a potential effect on prehospital triage and selection of receiving facility [19]. PLUS could possible in the same manner be used to guide whether the patient should be transferred to a cardiology department or a general emergency department. PLUS may thus potentially improve be prehospital treatment, monitoring and transportation in patients with acute respiratory failure. Depending on how the prehospital and in-hospital systems are organised, PLUS can be used to guide which patients who do not have cardiogenic pulmonary oedema and can thus safely be transported to a general emergency department and to identify patients with a high risk of cardiogenic pulmonary oedema needing initial assessment by a cardiologist.
Limitations
Being a single-MECU study, the results cannot necessarily be applied to other MECUs or other prehospital settings. Being a pilot study with a relatively small sample size, the results has to be interpreted with caution, as also reflected by the relatively wide 95 % CI’s of the results. The study results are however still useful for generating hypotheses for future studies. The physicians performing the examinations only had limited PLUS training, this would however reflect a “real-life-setting” in which the MECU physician does not necessarily have extensive skills and experience in focused ultrasound. In some of the few published LUS learning studies, using LUS to assess whether interstitial syndrome is present or absent, a high diagnostic accuracy could be achieved even after short training as used in the present study [14, 15, 20]. Even though patients were included prospectively, the study results may have been affected by selection bias. No registration was performed of the patients not included in the study; hence no data are available for the screening process for patient participation in the study. Since patients had to be able to give informed consent in order to participate in the study, patients with very severe respiratory failure who could not give consent was not included. Seen from a study design perspective, ideally all patients with signs of respiratory failure should have been included no matter whether consent could be given or not. Such a design was however not possible in order to obtain approval from the Committee on Biomedical Research Ethics. To what extent patients were not included due to inclusion criteria not being met, due to the treating physician deemed that PLUS would delay life-saving treatment or transportation, or due to patient not being able to give informed consent is not known. Even though all the physicians received the same training prior to the study, differences in ultrasound competencies prior to the study might also have introduced selection bias if more experienced sonographers were more likely to include patients. Based on the average number of MECU activations per year and the relatively common occurrence of patients with respiratory failure one would expect that inclusion of 40 patients to the study could have been completed faster than it did. There is thus a high risk of selection bias being introduced in the patient recruitment process. To what extent this has affected study results are unknown due to the lack of available data.
Conclusion
Performed as a part of a physician based MECU, PLUS seems fast and highly feasible in patients with respiratory failure. Due to its diagnostic accuracy, PLUS may have potential as a prehospital tool, especially to rule out cardiogenic pulmonary oedema. Due to the relatively small sample size, the results has to be interpreted with caution, the results are however still useful for generating hypotheses for future studies.
References
Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, Melniker L, Gargani L, Noble VE, Via G, Dean A, Tsung JW, Soldati G, Copetti R, Bouhemad B, Reissig A, Agricola E, Rouby JJ, Arbelot C, Liteplo A, Sargsyan A, Silva F, Hoppmann R, Breitkreutz R, Seibel A, Neri L, Storti E, Petrovic T, International Liaison Committee on Lung Ultrasound for International Consensus Conference on Lung U. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38:577–91.
Kristensen MS, Teoh WH, Graumann O, Laursen CB. Ultrasonography for clinical decision-making and intervention in airway management: from the mouth to the lungs and pleurae. Insights Imaging. 2014;5:253–79.
Badgett RG, Lucey CR, Mulrow CD. Can the clinical examination diagnose left-sided heart failure in adults? JAMA. 1997;277:1712–9.
Lichtenstein D, Meziere G. A lung ultrasound sign allowing bedside distinction between pulmonary edema and COPD: the comet-tail artifact. Intensive Care Med. 1998;24:1331–4.
Pivetta E, Goffi A, Lupia E, Tizzani M, Porrino G, Ferreri E, Volpicelli G, Balzaretti P, Banderali A, Iacobucci A, Locatelli S, Casoli G, Stone MB, Maule MM, Baldi I, Merletti F, Cibinel G. Lung ultrasound-implemented diagnosis of acute decompensated heart failure in the Emergency Department - a SIMEU multicenter study. Chest. 2015;148(1):202–10.
Lichtenstein DA, Meziere GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest. 2008;134:117–25.
Laursen CB, Sloth E, Lassen AT, Christensen R, Lambrechtsen J, Madsen PH, Henriksen DP, Davidsen JR, Rasmussen F. Point-of-care ultrasonography in patients admitted with respiratory symptoms: a single-blind, randomised controlled trial. Lancet Respir Med. 2014;2:638–46.
Prosen G, Klemen P, Strnad M, Grmec S. Combination of lung ultrasound (a comet-tail sign) and N-terminal pro-brain natriuretic peptide in differentiating acute heart failure from chronic obstructive pulmonary disease and asthma as cause of acute dyspnea in prehospital emergency setting. Crit Care. 2011;15:R114.
Zechner PM, Aichinger G, Rigaud M, Wildner G, Prause G. Prehospital lung ultrasound in the distinction between pulmonary edema and exacerbation of chronic obstructive pulmonary disease. Am J Emerg Med. 2010;28:389 e381–382.
Strnad M, Prosen G, Borovnik LV. Bedside lung ultrasound for monitoring the effectiveness of prehospital treatment with continuous positive airway pressure in acute decompensated heart failure. Eur J Emerg Med. 2016;23:50–5.
Volpicelli G, Mussa A, Garofalo G, Cardinale L, Casoli G, Perotto F, Fava C, Frascisco M. Bedside lung ultrasound in the assessment of alveolar-interstitial syndrome. Am J Emerg Med. 2006;24:689–96.
Laursen CB, Sloth E, Lambrechtsen J, Lassen AT, Madsen PH, Henriksen DP, Davidsen JR, Rasmussen F. Focused sonography of the heart, lungs, and deep veins identifies missed life-threatening conditions in admitted patients with acute respiratory symptoms. Chest. 2013;144:1868–75.
Frasure SE, Matilsky DK, Siadecki SD, Platz E, Saul T, Lewiss RE. Impact of patient positioning on lung ultrasound findings in acute heart failure. Eur Heart J Acute Cardiovasc Care. 2015;4:326–32.
Noble VE, Lamhaut L, Capp R, Bosson N, Liteplo A, Marx JS, Carli P. Evaluation of a thoracic ultrasound training module for the detection of pneumothorax and pulmonary edema by prehospital physician care providers. BMC Med Educ. 2009;9:3.
Martindale JL, Noble VE, Liteplo A. Diagnosing pulmonary edema: lung ultrasound versus chest radiography. Eur J Emerg Med. 2013;20:356–60.
Fleiss JL. Statistical methods for rates and proportions. 2nd ed. New York: Wiley; 1981.
Volpicelli G, Cardinale L, Mussa A, Valeria C. Diagnosis of cardiogenic pulmonary edema by sonography limited to the anterior lung. Chest. 2009;135:883. author reply 883-884.
Singer AJ, Emerman C, Char DM, Heywood JT, Kirk JD, Hollander JE, Summers R, Lee CC, Wynne J, Kellerman L, Peacock WF. Bronchodilator therapy in acute decompensated heart failure patients without a history of chronic obstructive pulmonary disease. Ann Emerg Med. 2008;51:25–34.
O’Dochartaigh D, Douma M. Prehospital ultrasound of the abdomen and thorax changes trauma patient management: a systematic review. Injury. 2015;46:2093–102.
Bedetti G, Gargani L, Corbisiero A, Frassi F, Poggianti E, Mottola G. Evaluation of ultrasound lung comets by hand-held echocardiography. Cardiovasc Ultrasound. 2006;4:34.
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, Lijmer JG, Moher D, Rennie D, de Vet HC. Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. Standards for reporting of diagnostic accuracy. Clin Chem. 2003;49:1–6.
Authors’ contributions
CBL: Has contributed to conception and design, acquisition of data, analysis and interpretation of data. Has drafted the submitted article. Has approved the final version to be published. AH: Has contributed to conception and design, acquisition of data, analysis and interpretation of data. Has drafted the submitted article. Has approved the final version to be published. SP: Has contributed to conception and design, acquisition of data, analysis and interpretation of data. Has drafted the submitted article. Has approved the final version to be published. SM: Has contributed to conception and design, acquisition of data, analysis and interpretation of data. Has drafted the submitted article. Has approved the final version to be published. LV: Has contributed to conception and design, acquisition of data, analysis and interpretation of data. Has drafted the submitted article. Has approved the final version to be published. HB: Has contributed to conception and design, acquisition of data, analysis and interpretation of data. Has drafted the submitted article. Has approved the final version to be published.
Competing interests
CBL: Has received payment as author of e-learn material for courses in ultrasound organized by USabcd A/S. AH: None. SP: None. SM: None. LV: Study investigator for Novartis and Sanofi, and study advisory board member for Novartis and Boehringer Ingelheim. HB: None.
Ethics approval and consent to participate
The study was conducted according to the Helsinki Declaration and approved by the Committee on Biomedical Research Ethics for The Region of Southern Denmark (ID S-20130029) and the hospital’s local branch of the Danish Data Protection Agency. Study was conducted according to Standards for Reporting Diagnostic accuracy studies (STARD)(STARD checklist, see appendix, Table 6) [21].
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Laursen, C.B., Hänselmann, A., Posth, S. et al. Prehospital lung ultrasound for the diagnosis of cardiogenic pulmonary oedema: a pilot study. Scand J Trauma Resusc Emerg Med 24, 96 (2016). https://doi.org/10.1186/s13049-016-0288-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13049-016-0288-2