
Abstract
Subjective cognitive decline (SCD) is regarded as the first clinical manifestation in the Alzheimer’s disease (AD) continuum. Investigating populations with SCD is important for understanding the early pathological mechanisms of AD and identifying SCD-related biomarkers, which are critical for the early detection of AD. With the advent of advanced neuroimaging techniques, such as positron emission tomography (PET) and magnetic resonance imaging (MRI), accumulating evidence has revealed structural and functional brain alterations related to the symptoms of SCD. In this review, we summarize the main imaging features and key findings regarding SCD related to AD, from local and regional data to connectivity-based imaging measures, with the aim of delineating a multimodal imaging signature of SCD due to AD. Additionally, the interaction of SCD with other risk factors for dementia due to AD, such as age and the Apolipoprotein E (ApoE) ɛ4 status, has also been described. Finally, the possible explanations for the inconsistent and heterogeneous neuroimaging findings observed in individuals with SCD are discussed, along with future directions. Overall, the literature reveals a preferential vulnerability of AD signature regions in SCD in the context of AD, supporting the notion that individuals with SCD share a similar pattern of brain alterations with patients with mild cognitive impairment (MCI) and dementia due to AD. We conclude that these neuroimaging techniques, particularly multimodal neuroimaging techniques, have great potential for identifying the underlying pathological alterations associated with SCD. More longitudinal studies with larger sample sizes combined with more advanced imaging modeling approaches such as artificial intelligence are still warranted to establish their clinical utility.
Similar content being viewed by others

Highlights
-
The main imaging features and neuroimaging advances in individuals with SCD related to AD are summarized.
-
The symptoms of SCD are associated with specific and distinctive underlying pathological events.
-
A preferential vulnerability of AD-signature regions in individuals with SCD are described.
-
The risk factors for dementia due to AD may interact with SCD and aggregate brain alterations.
Background
Alzheimer’s disease (AD) is one of the most common causes of dementia, with a dramatically increasing incidence in recent years that is expected to reach 115 million in 2050 [World Alzheimer Report 2018, www.alz.co.uk]. Currently available treatments are moderately beneficial at best for the symptomatic stages of AD [1]. Patients with preclinical AD are defined as cognitively unimpaired individuals with abnormal AD biomarkers [2]. At this very early stage, individuals still have sufficiently intact cognitive function that can be harnessed and directed toward either compensation or restitution of function [3]. More importantly, evolving biomarker studies enable to identify individuals with preclinical AD, which provides the best opportunity for therapeutic success and prevents cognitive decline before the onset of clinical symptoms.
Subjective cognitive decline (SCD), the first clinical manifestation in the AD continuum, is self-experienced decline in cognitive function without evidence of objective cognitive impairment [3,4,5]. SCD is postulated to manifest at a relatively late phase of preclinical AD and is associated with increased risks of AD biomarker abnormalities and future cognitive decline and dementia [2, 4, 6], making it a high-risk condition for the development of dementia due to AD. However, knowledge about the relationship between SCD and AD neuroimaging biomarkers is still controversial. Thus, investigating populations with SCD is important for understanding the early pathological mechanisms of preclinical AD and identifying SCD-related biomarkers, which are crucial for the early detection of AD with relatively inexpensive and easy measures.
Although SCD is a heterogeneous concept that can be induced by many conditions other than AD [4], including normal aging, psychiatric conditions (e.g., depression), other neurological and medical disorders (e.g., frontal temporal dementia and dementia with Lewy bodies), substance abuse and certain medications, we specifically focus on SCD due to AD, and these other conditions have been excluded from all studies included in this review. With the advent of neuroimaging techniques, such as positron emission tomography (PET) and magnetic resonance imaging (MRI) [7], structural and functional brain alterations have been detected in vivo during the asymptomatic stage of AD [8, 9]. An increasing number of neuroimaging studies have indicated that the symptoms of SCD are associated with specific and distinctive underlying pathological events, such as the abnormal deposition of ß-amyloid and tau proteins, gray matter atrophy, disruptions in the white matter (WM) and deficits in brain function [3, 10, 11]. The utility of neuroimaging techniques makes it possible to understand the neuropathological mechanisms underlying SCD related to AD and to provide potential pathological and imaging biomarkers for the early detection and even prediction of AD.
The purpose of this review is to provide a state-of-the-art and comprehensive summary of the literature regarding advances in neuroimaging findings in individuals with SCD within the context of AD by including studies using different imaging modalities. The limitations of current studies and future directions are also discussed.
Methods
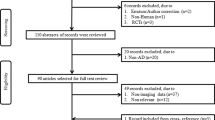
We searched the PubMed and Science Direct databases for articles describing the neuroimaging changes in individuals with SCD related to AD published from January 1994 to September 2019. The search terms used were “((subjective cognitive decline[Title/Abstract]) OR (subjective memory decline[Title/Abstract]) OR (subjective cognitive complaint[Title/Abstract]) OR (subjective cognitive complaints[Title/Abstract]) OR (subjective memory impairment[Title/Abstract]) OR (subjective memory impairments[Title/Abstract]) OR (subjective memory complaint[Title/Abstract]) OR (subjective memory complaints[Title/Abstract]) OR (cognitive complaints[Title/Abstract]) OR (subjective cognitive impairment[Title/Abstract]) OR (subjective cognitive impairments[Title/Abstract])) AND (Alzheimer’s disease) AND (neuroimaging OR PET OR MRI OR EEG OR MEG OR NIRs OR ASL OR DKI OR DSI OR DTI OR fMRI OR sMRI OR QSM)”. The studies were included based on the following inclusion criteria: (1) studies that described neuroimaging changes in individuals with SCD related to AD, (2) participants with SCD exhibited normal performance on standard neuropsychological tests and were free of other medical or psychiatric causes, and (3) original research published in English with the full-text available, regardless of the research settings. The following types of studies were excluded: (1) case reports, conference abstracts, reviews and study design or protocols, (2) studies with an interventional/experimental study design, and (3) studies not related to our topics: i.e., studies that did not use neuroimaging markers and studies focused on SCD that was caused by other conditions (e.g., cerebrovascular disease, epilepsy, Parkinson’s disease, dementia with Lewy bodies, etc.), studies focused on MCI or dementia populations, studies focused on other risk factors for impaired cognitive function (e.g., sleep changes, depression, nutritional status, etc.) and studies focused on other topics not related to our aim. After detailed evaluations, 114 studies were included and reviewed. A detailed description of the article selection process is presented in the flowchart (Fig. 1). We discussed and summarized the neuroimaging changes related to SCD in the background of AD in detail according to the different neuroimaging modalities, including neuroimaging performed at the molecular, structural, and functional levels.

Flowchart of the literature screening process and results. Abbreviations: SCD=subjective cognitive decline; CVD=cerebrovascular disease; PD=Parkinson’s disease; DLB=dementia with Lewy body; MCI=mild cognitive impairment; AD=Alzheimer’s disease
Standard terminology and diagnostic criteria
The concept of SCD was first introduced in the early 1980s by Reisberg and colleagues to define an early stage of AD and was initially assessed using the Global Deterioration Scale [12]. In recent years, SCD has received various labels, including subjective cognitive complaints, subjective memory complaints, subjective cognitive impairment, subjective memory impairment, subjective memory decline and others [4]. Although the impairment has attracted increasing attention since 2005, SCD research has been hampered by the lack of a common nomenclature, and uniform criteria for defining SCD are not available. Some studies identified SCD with a single question such as “Do you feel you can remember things as well as you used to?”, while other groups assessed SCD with structured questionnaires such as the Mood and Feelings Questionnaire (MFQ) and/or the self-evaluated Everyday Cognition Scale (E-Cog). In 2014, a consensus terminology and a conceptual framework for research on SCD related to AD was proposed by the Subjective Cognitive Decline Initiative (SCD-I) [4]. This framework unified the multiple descriptors into a single term, SCD, and presented a set of features of SCD due to AD, named “SCD-plus”, to facilitate the comparison of study findings, data pooling, meta-analyses, and collaborative multicenter research. These features include onset within 5 years, age at onset ≥ 60 years, concerns regarding feelings of worse performance than other individuals of the same age, confirmation of cognitive decline by an informant, possession of the Apolipoprotein E (ApoE) ɛ4 genotype and the presence of biomarker evidence for AD. Recently, two additional SCD plus features were proposed, including consistent SCD over time and seeking medical help because of SCD [5]. The framework also supports some flexibility in the classification of SCD, but researchers are responsible for explicitly clarifying how they operationalize SCD and why they chose a particular approach. All these efforts help further advance the investigation of SCD related to AD.
Only a few longitudinal studies of people with carefully phenotyped SCD have investigated the rate of progression of SCD to dementia due to AD [13, 14]. With clinical advances, the increasing number of memory clinics will facilitate the enrollment of subjects with SCD and increase awareness about SCD and the concept of cognitive protection.
Positron emission tomography
β-amyloid deposition
The advent of PET amyloid tracers allows the quantification of amyloid deposition in vivo [15,16,17]. 11C-Pittsburgh Compound B (PiB) was the first amyloid PET ligand with high affinity for amyloid [18]. Additionally, the development of 18F-labeled ligands (18F-florbetapir, 18F-florbetaben and 18F-flutemetamol) has facilitated their widespread use due to longer half-lives (~110 min) [19,20,21]. A meta-analysis reported a prevalence of amyloid pathology among individuals with SCD of 12%-43% [22]. According to Perrotin et al. and Snitz et al., subjects with SCD showed a significant increase in amyloid positivity compared with healthy controls (HCs) [23, 24]. Furthermore, several studies using the amyloid load as a continuous variable verified the relationship between the amyloid burden and the severity of SCD [25,26,27,28,29]. However, some other studies did not report this relationship [30,31,32,33]. Therefore, the correlations between the existence and severity of SCD with amyloid pathology remain inconsistent, potentially due to the different research settings and methods for the operationalization of SCD used among studies.
In clinical patients with dementia due to AD, amyloid deposition exhibits a diffuse pattern that initiates from the prefrontal and posterior parietal regions with the highest vulnerability [34, 35]. Interestingly, a similar pattern of the spatial distribution of amyloid deposition was also observed in individuals with SCD, which was mainly distributed in the temporal [24], medial prefrontal, anterior and posterior cingulate cortices and the precuneus [25]. Therefore, consistent with the “amyloid cascade” hypothesis [36], the increase in amyloid levels in AD-specific regions might be associated with SCD, potentially more than 10 years prior to the ensuing cognitive impairment.
Furthermore, several studies have focused on the clinical features of SCD, such as specific involved cognitive domains, related concerns, and the confirmation of informants, and explored their relationships with the amyloid burden to increase the predictive power of SCD to the underlying amyloid pathology. For example, Amariglio et al. (2012) revealed a significant correlation between scores of the memory and executive subscales of SCD with the amyloid burden [29]. As shown in another study, self-reported confusion, but not the total SCD score, predicted global and regional amyloid deposition in SCD [32]. Moreover, SCD-related worry was also found to be associated with the cortical amyloid load [33]. Therefore, the additional features of SCD may enhance its association with AD pathology.
Recently, several studies have consistently suggested that higher amyloid aggregation at baseline indicated a faster rate of decline in various cognition domains [37, 38] and a more rapid increase in SCD severity over time [39] in individuals with SCD. In addition, subjects in the amyloid-positive group with a greater number of subjective memory complaints displayed a greater rate of progression to mild cognitive decline (MCI) [40] and dementia due to AD [41]. These investigations provided evidence that SCD with a high amyloid load may indicate a faster longitudinal cognitive decline and worse clinical progression.
Notably, amyloid deposition in subjects with SCD is also affected by other risk factors for dementia due to AD, such as the ApoE ɛ4 genotype and age. Individuals with SCD may present higher allelic frequencies of ApoE ɛ4, and cerebral amyloid levels might be partially predicted by the ApoE ɛ4 level [42]. In another study of individuals with SCD from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) database, ApoE ɛ4 carriers with SCD showed higher levels of amyloid accumulation than noncarriers. However, no hypometabolism or atrophy was detected [43]. Aging is also associated with increased cerebral amyloid deposition in cognitively normal elderly people. A meta-analysis [22] reported an association between the occurrence of cerebral amyloid pathology in cognitively normal individuals and age, increasing from 10% to 44% in individuals between 50 and 90 years of age. Zwan et al. (2016) assessed multiple risk factors for high amyloid levels, including SCD, the ApoE genotype, age, and episodic memory [44], to further elucidate the relationship. However, the effects of the interactions among SCD, the ApoE genotype, age and other potential contributing factors on preclinical AD are complicated and are not completely understood to date. Therefore, additional investigations are needed to clarify the relationship among different risk factors for dementia due to AD.
Tau burden
Pathological tau deposition represents another key biomarker of AD [45, 46]. The development of selective tau tracers, such as the most extensively used tracer 18F-Flortaucipir [47], allows researchers to investigate regional distribution of tau pathology in the living human brain [46, 48, 49]. In the preclinical stage, the relationship between the symptoms of SCD and tau burden has been reported by Swinford and colleagues [50]. They scanned SCD subjects using 18F-flortaucipir PET and determined that the self-reported memory concern was associated with frontal tau levels, whereas the informant-reported concern was related to parietal tau levels. However, until now, the tau PET studies in individuals with SCD are currently limited. More evidence is needed to further elucidate the association between tau and amyloid pathology and their contribution to SCD and clinical progression.
Cerebral glucose metabolism
18F-Fluorodeoxyglucose (FDG)-PET has been used to quantify abnormal cerebral glucose metabolism [40, 51, 52]. Hypometabolism in individuals with MCI and dementia due to AD have been consistently confirmed, primarily in the posterior parietal and temporal regions [53, 54]. The hypometabolic profile in AD-related regions has been characterized in subjects with SCD and involves the parietotemporal cortex, precuneus, precentral and parahippocampal gyri [55,56,57]. However, Scheef et al. (2012) observed increased metabolism in the right medial temporal lobe in the SCD group compared with HCs, which may suggest compensatory neuronal activity. Additionally, metabolic deficits associated with SCD have been observed in high-risk genetic carriers of ApoE ɛ4 [55].
Moreover, some studies have explored the relationship between regional glucose metabolism and cognitive performance in subjects with SCD. For example, the metabolism in both the left hippocampus and the right amygdala was positively correlated with verbal logical memory immediate recall [58]. FDG-PET not only enables the prediction of cognitive function but also may serve as a prognostic marker for tracking longitudinal cognitive changes. Scheef and colleagues identified an association between hypometabolism in the right precuneus at baseline and the degree of longitudinal memory decline [59]. Based on these findings, hypometabolism may be a potential functional biomarker for the early detection of AD (Table 1).
Structural MRI and diffusion MRI
Gray matter
Both cortical and subcortical atrophy develop as AD progresses, making its volumetry one of the most well-established imaging biomarkers of AD [62]. As preferential target locations of neurofibrillary tangles [45], the entorhinal cortex and hippocampus display marked atrophy in patients with dementia due to AD [63,64,65,66].
However, during the SCD stage, neuroimaging findings regarding gray matter changes remain mixed. Some studies have observed a decreased hippocampal volume in individuals with SCD both at baseline [59, 67,68,69,70,71,72,73,74] and during a significant longitudinal decline, with an annual decrease of 1.9% [75, 76], whereas other studies have not reported significant changes [77,78,79,80,81,82,83]. The heterogeneity of SCD may be one of the causes of the inconsistent results, as evidence has suggested that patients with clinically defined SCD who present with smaller brain volumes have a higher risk of developing dementia than community-recruited subjects with SCD [23]. When combined with genetic risk factors, SCD subjects who are ApoE ɛ4 carriers showed more severe atrophy in the left hippocampus [84] and an additive reduction in the right cortical surface area [85] than noncarriers; this outcome is consistent with the results from longitudinal studies [86]. Furthermore, some studies have investigated the volumetric differences in subcortical regions, including the cholinergic basal forebrain nuclei and the hippocampal subfield, between individuals with SCD and HCs. The findings have converged to suggest that SCD is associated with a significant reduction in the volume of the cholinergic basal forebrain and the CA1 region of the hippocampus compared with HCs [87,88,89,90]. In addition to a reduced subcortical volume, a thinner cortex, particularly in the temporal-parietal lobe, was associated with a more rapid memory deterioration and an increased risk of disease progression in subjects with SCD compared with HCs [91,92,93,94].
Interestingly, Peter et al. [95] used a multivariate pattern analysis (MVPA) to summarize the structural imaging profile of a subject into a single meaningful value via a multivariate classification framework. The researchers trained a classifier to separate individuals with dementia due to AD from HCs and found that the gray matter atrophy pattern of a subject with SCD was similar to the brain of a patient with dementia due to AD but was significantly different from an HC. The voxels with greatest contributions to the classification were mainly distributed in hippocampal and parahippocampal areas. The findings of the study by Peter and colleagues suggested that the multivariate analysis may represent a powerful method for detecting subtle and distributed changes in the early stages of AD.
Using brain network modeling methods, a gray matter network can be constructed by calculating the structural covariance between pairs of regions. According to previous studies, gray matter networks of patients with dementia due to AD tend to be more randomly organized with lower clustering coefficients and altered small-world properties [96,97,98], suggesting that AD may be a disconnection syndrome. Recently, Verfaillie et al. [99] and Tijms et al. [100] have reported altered patterns of gray matter networks in individuals with SCD that are similar to patients with dementia due to AD. Both groups of researchers showed that the gray matter network of individuals with SCD was more randomly organized than HCs, and the disrupted network properties were associated with a steeper decline in global cognition and a higher risk of disease progression. Moreover, Ten Kate et al. [101] observed an association between a higher level of global amyloid deposition and lower clustering and fewer small-world properties of gray matter structural networks in subjects with SCD. Overall, although some negative results have been reported, individuals with SCD related to AD have been repeatedly shown to present a reduced gray matter volume and cortical thickness and a disrupted gray matter network.
White matter
Diffusion tensor imaging (DTI) has been increasingly applied to investigate microstructural alterations in the WM of patients with a neurodegenerative disease [102], which might reflect the pathological alterations of WM degeneration, such as axon loss, damage or demyelination. For patients with MCI and dementia due to AD, widespread disruptions with decreased fractional anisotropy (FA) and increased mean diffusivity (MD), particularly in the cingulum bundles and corpus callosum, and significant topological alterations of the brain structural connectome have been consistently reported [103,104,105,106,107,108].
In individuals with SCD, significantly decreased FA and increased MD have been observed in the cerebrum, mainly in the hippocampal body, entorhinal cortex and parahippocampal gyrus, uncinated fasciculi, longitudinal fasciculi and corpus callosum [77, 78, 109,110,111,112,113], whereas Kiuchi et al. and Viviano et al. reported no statistically significant differences in diffusion metrics [114, 115]. Various reasons for the discrepancy are plausible, including different operational definitions of SCD and differences in other factors (e.g., medication noncompliance, blood pressure, and scanner differences). Interestingly, by performing a whole-brain voxelwise analysis, Selnes et al. [116] found increased radial diffusivity (RD) and MD in widespread WM tracts but no changes in FA in subjects with SCD. This finding may indicate that FA is less sensitive than diffusivity metrics in revealing early pathological processes. In addition, genetic risk factors may aggravate degeneration in individuals with SCD. For instance, compared with noncarriers, ApoE ɛ4 carriers in SCD populations showed lower FA in the splenium of the corpus callosum and the anterior corona radiata [117]. Another investigation categorized individuals with SCD into a high-risk group and a low-risk group based on age, ApoE genotype, K-MMSE recall score and the Seoul Verbal Learning Test. The high-risk group showed more severe microstructural disruptions with reduced FA in the tracts connecting the hippocampus, parahippocampal gyrus, supramarginal gyrus and parts of the frontotemporal lobes [118].
In contrast to the quantification of local diffusion metrics, other scholars have investigated the topological organization of structural networks underlying SCD with a graph theory analysis. As shown in the study by Shu and colleagues, the SCD connectome exhibited lower global and local efficiency and reduced rich-club and local connections, which were correlated with impaired memory performance in subjects with SCD [119]. According to Yan et al., only a limited number of peripheral regions and the connectivity among nonhub regions were disrupted in patients with SCD, whereas rich-club integration remained stable in the early stage of SCD but subsequently progressed to exhibit disruptions associated with MCI and dementia due to AD [120]. Overall, topological measures of the brain structural connectome are sensitive metric of the early stage of AD, which establishes them as potential imaging markers of SCD.
The relationship between gray matter and WM alterations in subjects with SCD remains largely unknown. Research combining MRI volumetric and DTI measures suggested that individuals with SCD showed a lower entorhinal cortical volume, lower FA and higher MD in the hippocampal body and entorhinal WM [78]. According to another study [118], individuals with SCD with a high risk of progression had more severe WM disruption than the low-risk SCD group but no evident gray matter atrophy. Thus, relatively high-risk SCD may predict an underlying microstructural disruption in the WM that precedes gray matter atrophy during AD progression. However, during the SCD stage, the order of gray matter or WM alterations and the relationship between them require further investigation and elucidation to help us obtain a better understanding of the pathological mechanisms underlying AD development. The combination of multiple MRI modalities provides the opportunity to characterize biomarker features at different disease stages and precisely track the progression of neurodegenerative alterations (Table 2).
Functional MRI
Resting-state fMRI
Resting-state fMRI (rs-fMRI) is a noninvasive technique that detects alterations of spontaneous brain activity and interregional functional connectivity (FC) by measuring intrinsic blood oxygen level-dependent (BOLD) low-frequency signal fluctuation. Based on accumulating evidence, the FC of the default mode network (DMN) is selectively disrupted in patients with MCI and dementia due to AD [52, 129, 130]. The DMN can be detected in a resting state and plays an important role in episodic memory processing, self-reference, social cognition and overall brain function [131,132,133]. The DMN consists of a set of highly interconnected brain regions, including the posterior cingulate cortex, medial prefrontal cortex, lateral temporoparietal cortices and the hippocampus [134]. Importantly, these regions are among the earliest locations to show gray matter atrophy, hypometabolism and amyloid deposition during the initiation of AD pathology.
For subjects with SCD, our group reported a higher amplitude of low-frequency fluctuations (ALFF) of spontaneous brain activity in the left inferior parietal lobule and right middle occipital gyrus and a lower ALFF in the precuneus and cerebellum than in HCs [122, 135]. The alterations in ALFF were correlated with the verbal episodic memory scores of subjects with SCD [122]. The increased ALFF in SCD subjects may reflect a compensatory mechanism for functional deficits in the preclinical stage of AD. Yang et al. observed a higher accuracy of discriminating individuals with SCD from HCs when ALFF and fractional ALFF features were combined than when only single features were used [135].
Other studies have focused on the alterations in intrinsic functional networks. Subjects with SCD exhibited higher FC in the retrosplenial cortex and precuneus and lower FC in the frontal-parietal cortex and putative posterior memory system [115, 136, 137]. As an important potential biomarker, the DMN has also received increasing attention in individuals with SCD. However, the results remain heterogeneous. In terms of connectivity between the DMN and other regions, Verfaillie et al. [128] found increased connectivity between the posterior DMN and the medial temporal memory system in subjects with SCD; in contrast, decreased connectivity between the DMN and hippocampus was observed in individuals with SCD in another study [138]. Regarding the connectivity within the DMN, one study reported reduced DMN connectivity in individuals with SCD relative to HCs [139], conflicting with the findings of another study [73]. In addition, Yasuno and colleagues reported reduced FC in cortical midline structures where some of the DMN regions are located in individuals with SCD [113]. Furthermore, some studies also explored the interactions of SCD with other risk factors for dementia due to AD and their effects on FC. Cavedo et al. [60] found sex-specific alterations in the resting state (FC) of the DMN. The study conducted by Chiesa et al. revealed that ApoE ɛ4 carriers presented a slower longitudinal increase in FC in the frontal lobes than noncarriers [140]. Overall, these findings indicate an important role for the functional network, particularly the DMN, in SCD, suggesting that the DMN may represent a specific target for the early intervention and treatment of AD, although these results are heterogeneous and more studies based on rs-fMRI are needed to explore the role of the DMN in SCD.
Task-based fMRI
Task-based fMRI has been widely used to explore changes in functional activity during different cognitive tasks by examining the changes in BOLD signals. Medial temporal lobe hypoactivation, parietal hyperactivation, and frontal hyperactivation during memory tasks have been reported in patients with MCI and dementia due to AD [141,142,143,144]. Task-based fMRI studies of subjects with SCD remain scarce, and the current findings are controversial.
In one study, subjects with SCD showed increased activation in the middle frontal gyrus, the precuneus and the cingulate gyrus relative to HCs during working memory tasks [145]. However, a different effect was observed in another study [146], which showed that SCD was associated with reduced activation in the right hippocampus and increased activation in the right dorsolateral prefrontal cortex during an episodic memory recall task. In addition, Rodda et al. reported increased activation in the prefrontal cortex, left medial temporal lobe, bilateral thalamus, posterior cingulate and caudate of individuals with SCD during the encoding of novel words and a divided attention task [147, 148]. Notably, these regions displaying greater activation during different tasks were proposed to be mainly involved in the DMN, which may reflect the deployment of some compensatory processes. However, researchers have not yet clearly determined whether these differences are specific to successful memory encoding or related to general cognitive processes. Hayes and colleagues applied a subsequent memory paradigm to examine potential differences in the subsequent memory effect between cognitively intact older adults with and without SCD [149]. The researchers found that SCD was associated with more limited subsequent memory effects on the occipital lobe, superior parietal lobe, and posterior cingulate cortex and more disrupted subsequent memory effects on areas of the DMN. Interestingly, Hu and colleagues identified an association between increased delay discount in individuals with SCD and changes in the brain network related to episodic memory [150]. Hence, the altered functional activation patterns observed during memory tasks may indicate brain functional reorganization due to SCD. However, some advanced modeling approaches, such as dynamic causal modeling, should be productively applied to investigate early functional alterations in individuals with SCD.
Arterial spin labeling
Arterial spin labeling (ASL) MRI is a noninvasive technique for quantifying cerebral perfusion that has been implicated as a useful biomarker of the early stages of AD [151]. Patients with MCI exhibit hypoperfusion in the temporal parietal cortex [152,153,154,155], and patients with dementia due to AD present with decreased cerebral blood flow (CBF) in a wide range of brain areas [152, 156,157,158,159] compared with cognitively normal adults. In addition, some studies even reported that cognitively normal adults with the ApoE ɛ4 allele [154, 160, 161] and a maternal family history of AD [152] had an altered CBF (including a greater decrease in CBF over time, reduced CBF and increased resting-state CBF) compared with controls.
However, fewer ASL-MRI studies of individuals with SCD are available. To the best of our knowledge, only two studies have explored the differences in CBF between individuals with SCD and HCs. According to Hays et al., patients with SCD exhibited lower CBF in the medial orbitofrontal cortex and higher CBF in the right putamen than HCs [162], while de Eulate et al. did not observe any differences in total blood flow between individuals with SCD and HCs [163].
The results for the relationship between cognition and CBF are also inconsistent. Hays et al. observed negative association between verbal memory and CBF within the posterior cingulate cortex, middle temporal gyrus, hippocampus, fusiform gyrus and inferior frontal gyrus in patients with SCD [162], while Leeuwis et al. did not observed correlation between CBF and cognition in patients with SCD [164].
These controversial results may be due to the use of different cohorts and image processing methodologies. Hays et al. used voxelwise statistics among community-dwelling older volunteers, and the other two studies focused on defined ROI regions in the Amsterdam Dementia Cohort. In summary, ASL-MRI has vast potential as a biomarker of SCD, but additional studies using this modality are needed (Table 3).
EEG/MEG
Electroencephalography (EEG) and magnetoencephalography (MEG) are noninvasive techniques that record the electrical activity and magnetic fields generated by neuronal activity in the brain, respectively. During the last few decades, many studies have investigated the alterations in EEG and/or MEG signals in patients with MCI and dementia due to AD and have reported slowing brain rhythms and abnormal FC in the patients [166,167,168,169].
While the advanced stages of AD may be associated with functional disconnection [170], earlier stages may be apparent in terms of spectral measures and cortical rhythms detected using EEG [171,172,173]. Indeed, spectral data have shown a higher alpha power in patients with SCD that was most strongly correlated with a decline in verbal memory performance and the working memory reaction time [171]. In addition, Gouw et al. [173] reported association between abnormal delta, theta and alpha power and alpha peak frequency with clinical progression. In addition, amplitude abnormalities in delta, theta, and alpha rhythms have been recorded for individuals with SCD compared with HCs, suggesting that individuals with SCD present an abnormal pattern of dominant cortical alpha rhythms [172]. Furthermore, when separating individuals with SCD into decliners and nondecliners based on whether cognition decreased longitudinally, decliners showed increases in theta power, slowing of the mean frequency and changes in covariance among regions, particularly in the right hemisphere [174].
Using MEG, researchers have observed a significant alteration in spontaneous alpha activity in elderly participants with SCD, and this alteration was related to a decrease in cognitive performance [175]. An increase in brain activation in subjects with SCD and MCI during a memory task has also been reported [176]. Then, based on connectivity-based analyses, researchers revealed that participants with MCI and SCD exhibited a very similar pattern of alterations combining hypersynchronization over anterior brain regions (affecting the connection between the cingulate gyrus, frontal regions and anterior temporal areas) and hyposynchronization affecting more posterior areas (including parietal and medial temporal structures and occipital regions) [168]. Furthermore, subjects with SCD showed decreased clustering and transitivity in theta and beta bands, but increased modularity and transitivity in the alpha band, based on a graph theory analysis [177].
Overall, the aforementioned evidence supports the hypothesis that EEG/MEG measures play important roles in detecting early functional brain alterations in individuals with SCD and may serve as early imaging biomarkers of AD initiation (Table 4).
Multimodal neuroimaging studies
Multimodal neuroimaging techniques combing PET and MRI have been used with increasing frequency to improve our understanding of the pathological interactions underlying SCD due to AD [179]. Abnormal amyloid pathology is earliest pathological change and triggers downstream neurodegeneration events [2]. A between-group analysis performed by Chetelat et al. indicated that, in participants with SCD, individuals with a higher level of amyloid deposition showed significant gray matter atrophy compared with individuals with a low level of amyloid deposition [180]. Further correlation analyses between imaging modalities also supported the relationship between amyloid pathology and reduced integrity of brain structures in both the gray matter and WM ranging from voxel level to brain connectome properties in subjects with SCD [101, 181, 182]. Ferreira et al. tested a disease severity index generated from a multivariate analysis involving amyloid PET and structural MRI data, and this index may potentially identify individuals with SCD with the AD-like pattern, as an appropriate risk population [183]. More comprehensively, Wirth et al. incorporated amyloid PET, FDG-PET and structural MRI data to determine the pathological pattern in the AD continuum. The results revealed three distinct imaging biomarker patterns, which were detected in individuals with different stages of AD [184].
Regarding the relationship between amyloid and functional alterations, several studies have presented diverse results. Chiesa et al. described an association between a greater amyloid load and reduced posterior basal forebrain resting-state functional connectivity (RSFC) in the hippocampus and thalamus [185]. Li et al. showed a positive association between a higher degree centrality [186] of the bilateral hippocampus and left fusiform gyrus with total tau and phosphorylated tau levels, rather than cerebral amyloid deposition [187]. Additional studies have reported significantly decreased WM connections and FC loss in individuals with SCD [113]. Thus, the relationship between AD pathology and brain function during the SCD stage lacks accurate evidence, which may be due to the different methodologies used to acquire parameters, preprocess data and quantify the results.
Multimodal studies involving EEG have indicated that the slowing property detected with EEG was related to white matter lesions (WMLs) and medial temporal atrophy (MTA), but not to the amyloid load [178, 188]. Gaubert et al. divided patients with SCD into four subgroups according to their amyloid status (based on 18F-florbetapir PET) and neurodegeneration status (based on FDG-PET). The results demonstrated that in neurodegeneration-positive subjects, amyloid burden was related to delta power following a U-shaped curve and related to other EEG metrics, such as gamma power, spectral entropy, and complexity, following an inverted U-shaped curve [189].
Tau protein deposition is regarded as another critical pathological biomarker of AD. However, the complicated relationships between amyloid, tau, neurodegenerations and cognitive decline are not clearly understood. Studies using amyloid PET and tau PET have coincidentally suggested that both tau protein and amyloid pathology contributed to the manifestation of SCD [190, 191]. Specifically, amyloid and tau pathologies may give rise to different subjective cognitive domains [191].
In longitudinal studies using FDG-PET and MRI modalities, the longitudinal reduction in cognitive performance was associated with brain hypometabolism in the precuneus at baseline, but not with gray matter atrophy [59]. Specifically, patients with SCD from the clinic displayed greater gray matter atrophy progression over time compared with patients with SCD from the community, indicating that clinical SCD may represent a greater risk of dementia due to AD [192]. Overall, the multimodal neuroimaging technique offers a great advantage in exploring the relationship between different AD biomarkers, and more multimodal neuroimaging studies of SCD are required (Table 5).
Shortcomings and emerging trends
Factors contributing to heterogeneous neuroimaging findings in SCD
The inconsistent and heterogeneous neuroimaging findings in SCD may result from several factors: (a) The use of different diagnostic criteria and assessment strategies for SCD may be a factor contributing to the heterogenous findings. Although unified research criteria for SCD have been proposed by SCD-I, it has not been universally used. The evaluation and classification measurements of SCD vary among investigations, including both qualitative methods (SCD/no SCD based on binary questions) and quantitative measures (e.g., E-Cog, MFQ, and Memory Assessment Clinics Questionnaire (MAC-Q)) (b) Variations in the demographics of the cohorts, both within and across studies, may be another influencing factor. Converging evidence has suggested that demographic characteristics such as age, sex, education level and the presence of the ApoE ɛ4 allele are important factors influencing cognition. However, the distributions of these demographics are highly variable. (c) Methodological differences in the acquisition of parameters and the quantification methods (e.g., voxel-based analysis, region-of-interest analysis, connectivity or connectome-based approaches) may also be factors producing some inconsistencies in the results, indicating that the interpretations and comparisons of these findings should be viewed with caution. However, despite the existence of these influencing factors, most studies included in the current review still described some common neuroimaging alterations in individuals with SCD.
Longitudinal imaging studies
Longitudinal research in this field is still limited. Most of the studies investigating the neuroimaging changes in individuals with SCD often employ a cross-sectional design in which neuroimaging measures are compared between individuals with SCD and HCs. However, this commonly used design does not account for the differences in individual trajectories of brain changes. Longitudinal studies including follow-up scans enable the assessment of individual trajectories of brain changes and the identification of AD pathology in subjects with SCD. Additionally, longitudinal studies facilitate the investigation and validation of causality between pathological markers and emerging neurodegeneration and cognitive decline. Importantly, longitudinal designs allow researchers to explore biomarkers for the early prediction of disease conversion by investigating the subsets of patients with SCD who ultimately progress to dementia due to AD.
It is encouraging to learn that multiple international neuroimaging projects investigating dementia due to AD or preclinical AD are collecting data via longitudinal designs. Specifically, the ADNI database, an integral part of a multisite longitudinal study, is collecting multimodal imaging data (including MRI, DTI, fMRI and PET) and has started adding an SCD group from ADNI-2 [194]. MEMENTO is a clinic-based study that recruited 2323 patients with cognitive impairments and subjects with SCD at baseline who will be followed over a 5-year period [195]. In addition, the FACEHBI [196], INSIGHT-preAD [197], DELCODE [198] and SILCODE (trial registration: NCT03370744) [199] are ongoing longitudinal observational studies of individuals with SCD that will facilitate research exploring the developmental trajectory of different pathological biomarkers in AD. Importantly, opening and sharing these neuroimaging datasets of patients with SCD has been encouraged to accelerate the development of research in this field.
Multimodal imaging studies
Different neuroimaging techniques have captured different aspects of the brain abnormalities involved in SCD to help reveal its multimodal signature. However, no single-modality imaging method is currently able to accurately characterize the pathological mechanisms underlying the full spectrum of SCD. Thus, the increasingly utility of multimodal neuroimaging technology provides an opportunity to determine the complicated relationships between amyloid, tau and downstream neurodegenerative pathologies occurring in the AD process. For SCD populations, several studies combining multimodal neuroimaging techniques such as PET and MRI have recently been conducted. However, the complicated relationships between distinct pathological biomarkers, such as amyloid, tau, and macroscale structural and functional brain alterations during the SCD stage, from local to connectivity level changes, still remain largely unexplored. More multimodal imaging studies are urgently needed to understand the interactions between different pathological changes in the early stage of AD.
Additionally, newly developed molecular tracers, imaging sequences and ultrahigh field MRI techniques, such as the use of 7-T scanners, will be helpful to detect more subtle alterations in the early stage of the disease and should be applied to further investigate SCD populations.
Individual prediction with artificial intelligence
Artificial intelligence, such as machine learning and deep learning, offers a systematic approach to developing sophisticated, automatic, and objective classification frameworks for analyzing high-dimensional data. Additionally, artificial intelligence techniques are able to learn complex and subtle patterns of change across various imaging modalities [200]. Over the last decade, classification methods based on imaging have been increasingly integrated to identify the imaging signature of AD [201,202,203], offering promising tools for individualized diagnoses and prognostic predictions. However, until recently, neuroimaging-based studies for classifying SCD have been scarce [111, 126, 135, 204,205,206]. The early identification of SCD and the prediction of disease progression at the individual level is important for timely interventions. Furthermore, machine learning not only detects subtle and distributed changes but also enables the extraction of biomarkers from high-dimensional neuroimaging data. Recently, the neuroimaging-based “brain age” has been proposed as an important biomarker of an individual’s brain health [207]. Additionally, the SPARE-AD index was proposed based on a support vector machine (SVM) classifier between HCs and age-matched patients with dementia due to AD and was used to quantify the spatial pattern of abnormality [201]. Peter and colleagues used similar methods and showed that the extracted index was higher in individuals with SCD than in HCs [95]. The biomarker obtained based on machine learning might be more sensitive at detecting the early stage of AD because it captures a multivariable pattern. Overall, artificial intelligence combined with neuroimaging big data has the potential to enable individualized diagnoses of SCD due to AD and to extract sensitive imaging biomarkers from important features selected from high-dimensional neuroimaging data.
Conclusions
In this review, we have provided a comprehensive summary of the molecular, structural and functional brain alterations of individuals with SCD related to AD investigated at different scales, ranging from regional to large-scale network-based imaging measures.
We collected consistent results from the articles included in this review and summarized the shared neuroimaging changes observed in individuals with SCD in the context of AD, as shown in Fig. 2. Regarding the pathological alterations at the molecular level, PET studies have observed early amyloid deposition, an increased tau burden and hypometabolism in individuals with SCD. MRI techniques enable assessments of alterations in macroscopic brain structures, such as decreased hippocampal volume and thinner entorhinal cortex; as well as microstructural deficits in WM tracts, such as decreased FA in the hippocampus and parahippocampal gyrus and abnormal functional activity. These assessments also illustrate the abnormal FC of the DMN and topological alterations in the whole-brain connectome. Based on these findings, we identify a preferential vulnerability of highly selected brain regions that are mainly affected in individuals with MCI or dementia due to AD, including the hippocampus, medial temporal lobe, precuneus and temporoparietal regions, indicating that individuals with SCD share a similar pattern of pathological alterations with individuals with MCI and dementia due to AD. As different neuroimaging techniques can reflect different aspects of brain abnormalities, we also suggest that the combination of multiple imaging modalities may provide a more comprehensive understanding of the pathological process than a single modality. However, a small number of conflicting findings of neuroimaging changes in individuals with SCD due to AD exist, including reports of no relationship between SCD and amyloid pathology, the preservation of gray matter structure (e.g., the hippocampal volume) and WM integrity, and even hypermetabolism of cerebral glucose in SCD subjects. In particular for studies of brain function, although most studies have reported abnormal FC of the DMN in individuals with SCD, the directions of these results (i.e., increased FC or reduced FC) are still relatively inconsistent. These inconsistent results may be due to the differences in the methods used to classify and assess SCD, the demographics of the cohorts, and the acquisition of parameters and quantification methods.

Multimodal imaging signature of SCD. The consistent results were collected from the articles included in this review to provide a comprehensive summary of common neuroimaging changes in SCD. a SCD individuals exhibit a pattern of amyloid accumulation within the medial prefrontal, cingulum and precuneus cortex, which are early sites of vulnerability in MCI and dementia due to AD. b The medial temporal lobe is frequently characterized by hypometabolism, whereas other studies have reported a strong association between SCD and hypometabolism within the precuneus. c Individuals with SCD showed decreased hippocampal volume and thinner entorhinal cortex than healthy controls. d The abnormal FC between the posterior DMN and other regions are frequently reported in resting-state fMRI studies. e DTI studies have reported decreased FA in hippocampal and parahippocampal white matter in SCD individuals. Abbreviations: SCD = Subjective cognitive decline; MCI = Mild cognitive impairment; AD = Alzheimer’s disease; DTI = Diffusion tensor imaging; DMN = Default mode network; fMRI = Functional MRI; FC=Functional connectivity
In conclusion, the pathological alterations underlying the manifestation of SCD are parallel to those underlying MCI and dementia due to AD based on the results obtained using neuroimaging techniques, supporting the notion that SCD represents an early precursor of dementia due to AD. While cognitive function is preserved, early detection of SCD is imperative to ensure that patients will benefit from early intervention and obtain the appropriate treatment in a timely manner. In the future, with additional validation studies of larger samples and longitudinal studies, the combination of multimodal neuroimaging techniques may help identify SCD individuals presenting with early AD pathologies who may be eligible for clinical trials for the early detection and secondary intervention of AD.
Availability of data and materials
Not applicable.
Abbreviations
- SCD:
-
Subjective cognitive decline
- AD:
-
Alzheimer’s disease
- PET:
-
Positron emission tomography
- MRI:
-
Magnetic resonance imaging
- ApoE :
-
Apolipoprotein E
- MFQ:
-
Mood and Feelings Questionnaire
- E-Cog:
-
Everyday Cognition Scale
- SCD-I:
-
Subjective Cognitive Decline Initiative
- PiB:
-
Pittsburgh Compound B
- HCs:
-
Healthy controls
- FDG:
-
18F-Fluorodeoxyglucose
- MVPA:
-
Multivariate pattern analysis
- DTI:
-
Diffusion tensor imaging
- WM:
-
White matter
- FA:
-
Fractional anisotropy
- MD:
-
Mean diffusivity
- RD:
-
Radial diffusivity
- fMRI:
-
Functional MRI
- BOLD:
-
Blood oxygen level-dependent
- rs-fMRI:
-
Resting-state fMRI
- DMN:
-
Default mode network
- ALFF:
-
Amplitude of low-frequency fluctuations
- FC:
-
Functional connectivity
- ASL:
-
Arterial spin labeling
- CBF:
-
Cerebral blood flow
- EEG:
-
Electroencephalography
- MEG:
-
Magnetoencephalography
- RSFC:
-
Resting-state functional connectivity
- WMLs:
-
White matter lesions
- MTA:
-
Medial temporal atrophy
- SVM:
-
Support vector machine
- MAC-Q:
-
Memory assessment clinics questionnaire
- CSF:
-
Cerebrospinal fluid
- MCI:
-
Mild cognitive impairment
- ADNI:
-
Alzheimer’s Disease Neuroimaging Initiative
References
Ong SS, Doraiswamy PM, Lad EM. Controversies and Future Directions of Ocular Biomarkers in Alzheimer Disease. JAMA Neurol. 2018;75:650–1.
Jack CR, Bennett DA, Blennow K, Carrillo MC, Dunn B, Haeberlein SB, Holtzman DM, Jagust W, Jessen F, Karlawish J, et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer's disease. Alzheimers Dement. 2018;14:535–62.
Rabin LA, Smart CM, Amariglio RE. Subjective Cognitive Decline in Preclinical Alzheimer's Disease. Annu Rev Clin Psychol. 2017;13:369–96.
Jessen F, Amariglio RE, van Boxtel M, Breteler M, Ceccaldi M, Chetelat G, Dubois B, Dufouil C, Ellis KA, van der Flier WM, et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014;10:844–52.
Jessen F, Amariglio RE, Buckley RF, van der Flier WM, Han Y, Molinuevo JL, Rabin L, Rentz DM, Rodriguez-Gomez O, Saykin AJ, et al. The characterisation of subjective cognitive decline. Lancet Neurol. 2020;19:271–8.
Slot RER, Sikkes SAM, Berkhof J, Brodaty H, Buckley R, Cavedo E, Dardiotis E, Guillo-Benarous F, Hampel H, Kochan NA, et al. Subjective cognitive decline and rates of incident Alzheimer's disease and non-Alzheimer’s disease dementia. Alzheimers Dement. 2019;15:465–76.
Teichmann M, Epelbaum S, Samri D, Levy Nogueira M, Michon A, Hampel H, Lamari F, Dubois B. Free and Cued Selective Reminding Test - accuracy for the differential diagnosis of Alzheimer's and neurodegenerative diseases: A large-scale biomarker-characterized monocenter cohort study (ClinAD). Alzheimers Dement. 2017;13:913–23.
Habib M, Mak E, Gabel S, Su L, Williams G, Waldman A, Wells K, Ritchie K, Ritchie C, O'Brien JT. Functional neuroimaging findings in healthy middle-aged adults at risk of Alzheimer's disease. Ageing Res Rev. 2017;36:88–104.
Mak E, Gabel S, Mirette H, Su L, Williams GB, Waldman A, Wells K, Ritchie K, Ritchie C, O'Brien J. Structural neuroimaging in preclinical dementia: From microstructural deficits and grey matter atrophy to macroscale connectomic changes. Ageing Res Rev. 2017;35:250–64.
Sun Y, Yang FC, Lin CP, Han Y. Biochemical and neuroimaging studies in subjective cognitive decline: progress and perspectives. CNS Neurosci Ther. 2015;21:768–75.
Lista S, Molinuevo JL, Cavedo E, Rami L, Amouyel P, Teipel SJ, Garaci F, Toschi N, Habert MO, Blennow K, et al. Evolving Evidence for the Value of Neuroimaging Methods and Biological Markers in Subjects Categorized with Subjective Cognitive Decline. J Alzheimers Dis. 2015;48(Suppl 1):S171–91.
Reisberg B, Ferris SH, de Leon MJ, Crook T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am J Psychiatry. 1982;139:1136–9.
Bessi V, Mazzeo S, Padiglioni S, Piccini C, Nacmias B, Sorbi S, Bracco L. From Subjective Cognitive Decline to Alzheimer's Disease: The Predictive Role of Neuropsychological Assessment, Personality Traits, and Cognitive Reserve. A 7-Year Follow-Up Study. J Alzheimers Dis. 2018;63:1523–35.
Mazzeo S, Bessi V, Padiglioni S, Bagnoli S, Bracco L, Sorbi S, Nacmias B. KIBRA T allele influences memory performance and progression of cognitive decline: a 7-year follow-up study in subjective cognitive decline and mild cognitive impairment. Neurol Sci. 2019;40:1559–66.
Ikonomovic MD, Klunk WE, Abrahamson EE, Mathis CA, Price JC, Tsopelas ND, Lopresti BJ, Ziolko S, Bi W, Paljug WR, et al. Post-mortem correlates of in vivo PiB-PET amyloid imaging in a typical case of Alzheimer's disease. Brain. 2008;131:1630–45.
Klunk WE, Engler H, Nordberg A, Bacskai BJ, Wang Y, Price JC, Bergstrom M, Hyman BT, Langstrom B, Mathis CA. Imaging the pathology of Alzheimer's disease: amyloid-imaging with positron emission tomography. Neuroimaging Clin N Am. 2003;13:781–9 ix.
Herholz K, Ebmeier K. Clinical amyloid imaging in Alzheimer's disease. Lancet Neurol. 2011;10:667–70.
Klunk WE, Engler H, Nordberg A, Wang Y, Blomqvist G, Holt DP, Bergström M, Savitcheva I, Huang GF, Estrada S, et al. Imaging brain amyloid in Alzheimer's disease with Pittsburgh Compound-B. Ann Neurol. 2004;55:306–19.
Barthel H, Sabri O. Clinical use and utility of amyloid imaging. J Nucl Med. 2017;58:1711–7.
Anand K, Sabbagh M. Amyloid Imaging: Poised for Integration into Medical Practice. Neurotherapeutics. 2017;14:54–61.
Suppiah S, Didier MA, Vinjamuri S. The Who, When, Why, and How of PET amyloid imaging in management of alzheimer’s disease-review of literature and interesting images. Diagnostics (Basel). 2019;9:65.
Jansen WJ, Ossenkoppele R, Knol DL, Tijms BM, Scheltens P, Verhey FR, Visser PJ, Aalten P, Aarsland D, Alcolea D, et al. Prevalence of cerebral amyloid pathology in persons without dementia: a meta-analysis. Jama. 2015;313:1924–38.
Perrotin A, La Joie R, de La Sayette V, Barre L, Mezenge F, Mutlu J, Guilloteau D, Egret S, Eustache F, Chetelat G. Subjective cognitive decline in cognitively normal elders from the community or from a memory clinic: Differential affective and imaging correlates. Alzheimers Dement. 2017;13:550–60.
Snitz BE, Lopez OL, McDade E, Becker JT, Cohen AD, Price JC, Mathis CA, Klunk WE. Amyloid-beta Imaging in Older Adults Presenting to a Memory Clinic with Subjective Cognitive Decline: A Pilot Study. J Alzheimers Dis. 2015;48(Suppl 1):S151–9.
Perrotin A, Mormino EC, Madison CM, Hayenga AO, Jagust WJ. Subjective cognition and amyloid deposition imaging: a Pittsburgh Compound B positron emission tomography study in normal elderly individuals. Arch Neurol. 2012;69:223–9.
Snitz BE, Weissfeld LA, Cohen AD, Lopez OL, Nebes RD, Aizenstein HJ, McDade E, Price JC, Mathis CA, Klunk WE. Subjective Cognitive Complaints, Personality and Brain Amyloid-beta in Cognitively Normal Older Adults. Am J Geriatr Psychiatry. 2015;23:985–93.
Chen X, Farrell ME, Moore W, Park DC. Actual memory as a mediator of the amyloid-subjective cognitive decline relationship. Alzheimers Dement. 2019;11:151–60.
Rowe CC, Ellis KA, Rimajova M, Bourgeat P, Pike KE, Jones G, Fripp J, Tochon-Danguy H, Morandeau L, O'Keefe G, et al. Amyloid imaging results from the Australian Imaging, Biomarkers and Lifestyle (AIBL) study of aging. Neurobiol Aging. 2010;31:1275–83.
Amariglio RE, Becker JA, Carmasin J, Wadsworth LP, Lorius N, Sullivan C, Maye JE, Gidicsin C, Pepin LC, Sperling RA, et al. Subjective cognitive complaints and amyloid burden in cognitively normal older individuals. Neuropsychologia. 2012;50:2880–6.
Rodda J, Okello A, Edison P, Dannhauser T, Brooks DJ, Walker Z. 11C-PIB PET in subjective cognitive impairment. Eur Psychiatry. 2010;25:123–5.
Cacciamani F, Tandetnik C, Gagliardi G, Bertin H, Habert MO, Hampel H, Boukadida L, Revillon M, Epelbaum S, Dubois B. Low Cognitive Awareness, but Not Complaint, is a Good Marker of Preclinical Alzheimer's Disease. J Alzheimers Dis. 2017;59:753–62.
McCluskey GE, Yates P, Villemagne VL, Rowe C, Szoeke CEI. Self-reported confusion is related to global and regional beta-amyloid: data from the Women's healthy ageing project. Brain Imaging Behav. 2018;12:78–86.
Verfaillie SCJ, Timmers T, Slot RER, van der Weijden CWJ, Wesselman LMP, Prins ND, Sikkes SAM, Yaqub M, Dols A, Lammertsma AA, et al. Amyloid-beta Load Is Related to Worries, but Not to Severity of Cognitive Complaints in Individuals With Subjective Cognitive Decline: The SCIENCe Project. Front Aging Neurosci. 2019;11:7.
Thal DR, Rüb U, Orantes M, Braak H. Phases of Aβ-deposition in the human brain and its relevance for the development of AD. Neurology. 2002;58:1791–800.
Grothe MJ, Barthel H, Sepulcre J, Dyrba M, Sabri O, Teipel SJ. In vivo staging of regional amyloid deposition. Neurology. 2017;89:2031–8.
Hardy JA, Higgins GA. Alzheimer’s Disease: The amyloid cascade hypothesis. Science. 1992;256:184–5.
Hollands S, Lim YY, Buckley R, Pietrzak RH, Snyder PJ, Ames D, Ellis KA, Harrington K, Lautenschlager N, Martins RN, et al. Amyloid-beta related memory decline is not associated with subjective or informant rated cognitive impairment in healthy adults. J Alzheimers Dis. 2015;43:677–86.
Timmers T, Ossenkoppele R, Verfaillie SCJ, van der Weijden CWJ, Slot RER, Wesselman LMP, Windhorst AD, Wolters EE, Yaqub M, Prins ND, et al. Amyloid PET and cognitive decline in cognitively normal individuals: the SCIENCe project. Neurobiol Aging. 2019;79:50–8.
Amariglio RE, Buckley RF, Mormino EC, Marshall GA, Johnson KA, Rentz DM, Sperling RA. Amyloid-associated increases in longitudinal report of subjective cognitive complaints. Alzheimers Dement. 2018;4:444–9.
Watson KT, Wroolie TE, Tong G, Foland-Ross LC, Frangou S, Singh M, McIntyre RS, Roat-Shumway S, Myoraku A, Reiss AL, Rasgon NL. Neural correlates of liraglutide effects in persons at risk for Alzheimer’s disease. Behav Brain Res. 2019;356:271–8.
Buckley RF, Maruff P, Ames D, Bourgeat P, Martins RN, Masters CL, Rainey-Smith S, Lautenschlager N, Rowe CC, Savage G, et al. Subjective memory decline predicts greater rates of clinical progression in preclinical Alzheimer's disease. Alzheimers Dement. 2016;12:796–804.
Moreno-Grau S, Rodriguez-Gomez O, Sanabria A, Perez-Cordon A, Sanchez-Ruiz D, Abdelnour C, Valero S, Hernandez I, Rosende-Roca M, Mauleon A, et al. Exploring APOE genotype effects on Alzheimer's disease risk and amyloid beta burden in individuals with subjective cognitive decline: The FundacioACE Healthy Brain Initiative (FACEHBI) study baseline results. Alzheimers Dement. 2018;14:634–43.
Risacher SL, Kim S, Nho K, Foroud T, Shen L, Petersen RC, Jack CR Jr, Beckett LA, Aisen PS, Koeppe RA, et al. APOE effect on Alzheimer's disease biomarkers in older adults with significant memory concern. Alzheimers Dement. 2015;11:1417–29.
Zwan MD, Villemagne VL, Dore V, Buckley R, Bourgeat P, Veljanoski R, Salvado O, Williams R, Margison L, Rembach A, et al. Subjective Memory Complaints in APOEvarepsilon4 Carriers are Associated with High Amyloid-beta Burden. J Alzheimers Dis. 2016;49:1115–22.
Braak H, Braak E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 1991;82:239–59.
Villemagne VL, Fodero-Tavoletti MT, Masters CL, Rowe CC. Tau imaging: early progress and future directions. Lancet Neurol. 2015;14:114–24.
Marquié M, Normandin MD, Vanderburg CR, Costantino IM, Bien EA, Rycyna LG, Klunk WE, Mathis CA, Ikonomovic MD, Debnath ML, et al. Validating novel tau positron emission tomography tracer [F-18]-AV-1451 (T807) on postmortem brain tissue. Ann Neurol. 2015;78:787–800.
Saint-Aubert L, Lemoine L, Chiotis K, Leuzy A, Rodriguez-Vieitez E, Nordberg A. Tau PET imaging: present and future directions. Mol Neurodegener. 2017;12:19.
Márquez F, Yassa MA. Neuroimaging Biomarkers for Alzheimer’s Disease. Mol Neurodegener. 2019;14:21.
Swinford CG, Risacher SL, Charil A, Schwarz AJ, Saykin AJ. Memory concerns in the early Alzheimer's disease prodrome: Regional association with tau deposition. Alzheimers Dement. 2018;10:322–31.
Kato T, Inui Y, Nakamura A, Ito K. Brain fluorodeoxyglucose (FDG) PET in dementia. Ageing Res Rev. 2016;30:73–84.
Bai F, Watson DR, Shi Y, Wang Y, Yue C, YuhuanTeng WD, Yuan Y, Zhang Z. Specifically progressive deficits of brain functional marker in amnestic type mild cognitive impairment. PLoS One. 2011;6:e24271.
De Santi S, de Leon MJ, Rusinek H, Convit A, Tarshish CY, Roche A, Tsui WH, Kandil E, Boppana M, Daisley K, et al. Hippocampal formation glucose metabolism and volume losses in MCI and AD. Neurobiol Aging. 2001;22:529–39.
Minoshima S, Frey KA, Koeppe RA, Foster NL. Kuhl DE. A diagnostic approach in Alzheimer's disease using three-dimensional stereotactic surface projections of fluorine-18-FDG PET. J Nucl Med. 1995;36:1238–48.
Mosconi L, De Santi S, Brys M, Tsui WH, Pirraglia E, Glodzik-Sobanska L, Rich KE, Switalski R, Mehta PD, Pratico D, et al. Hypometabolism and altered cerebrospinal fluid markers in normal apolipoprotein E E4 carriers with subjective memory complaints. Biol Psychiatry. 2008;63:609–18.
Song IU, Choi EK, Oh JK, Chung YA, Chung SW. Alteration patterns of brain glucose metabolism: comparisons of healthy controls, subjective memory impairment and mild cognitive impairment. Acta Radiol. 2016;57:90–7.
Vannini P, Hanseeuw B, Munro CE, Amariglio RE, Marshall GA, Rentz DM, Pascual-Leone A, Johnson KA, Sperling RA. Hippocampal hypometabolism in older adults with memory complaints and increased amyloid burden. Neurology. 2017;88:1759–67.
Gardener SL, Sohrabi HR, Shen KK, Rainey-Smith SR, Weinborn M, Bates KA, Shah T, Foster JK, Lenzo N, Salvado O, et al. Cerebral Glucose Metabolism is Associated with Verbal but not Visual Memory Performance in Community-Dwelling Older Adults. J Alzheimers Dis. 2016;52:661–72.
Scheef L, Spottke A, Daerr M, Joe A, Striepens N, Kolsch H, Popp J, Daamen M, Gorris D, Heneka MT, et al. Glucose metabolism, gray matter structure, and memory decline in subjective memory impairment. Neurology. 2012;79:1332–9.
Cavedo E, Chiesa PA, Houot M, Ferretti MT, Grothe MJ, Teipel SJ, Lista S, Habert MO, Potier MC, Dubois B, Hampel H. Sex differences in functional and molecular neuroimaging biomarkers of Alzheimer's disease in cognitively normal older adults with subjective memory complaints. Alzheimers Dement. 2018;14:1204–15.
Matias-Guiu JA, Cabrera-Martin MN, Valles-Salgado M, Perez-Perez A, Rognoni T, Moreno-Ramos T, Carreras JL, Matias-Guiu J. Neural Basis of Cognitive Assessment in Alzheimer Disease, Amnestic Mild Cognitive Impairment, and Subjective Memory Complaints. Am J Geriatr Psychiatry. 2017;25:730–40.
Bayram E, Caldwell JZK, Banks SJ. Current understanding of magnetic resonance imaging biomarkers and memory in Alzheimer's disease. Alzheimers Dement. 2018;4:395–413.
Jack CR Jr, Petersen RC, Xu YC, Waring SC, O'Brien PC, Tangalos EG, Smith GE, Ivnik RJ, Kokmen E. Medial temporal atrophy on MRI in normal aging and very mild Alzheimer’s disease. Neurology. 1997;49:786–94.
Krasuski JS, Alexander GE, Horwitz B, Daly EM, Murphy DG, Rapoport SI, Schapiro MB. Volumes of medial temporal lobe structures in patients with Alzheimer's disease and mild cognitive impairment (and in healthy controls). Biol Psychiatry. 1998;43:60–8.
Pennanen C, Kivipelto M, Tuomainen S, Hartikainen P, Hänninen T, Laakso MP, Hallikainen M, Vanhanen M, Nissinen A, Helkala E-L, et al. Hippocampus and entorhinal cortex in mild cognitive impairment and early AD. Neurobiol Aging. 2004;25:303–10.
Teipel SJ, Pruessner JC, Faltraco F, Born C, Rocha-Unold M, Evans A, Moller HJ, Hampel H. Comprehensive dissection of the medial temporal lobe in AD: measurement of hippocampus, amygdala, entorhinal, perirhinal and parahippocampal cortices using MRI. J Neurol. 2006;253:794–800.
Flier W, Buchem M, Weverling-Rijnsburger AE, Mutsaers E, Bollen EEM, Admiraal-Behloul F, Westendorp RJ, Middelkoop HM. Memory complaints in patients with normal cognition are associated with smaller hippocampal volumes. J Neurol. 2004;251:671–5.
Kim MJ, Seo SW, Kim GH, Kim ST, Lee JM, Qiu A, Na DL. Less depressive symptoms are associated with smaller hippocampus in subjective memory impairment. Arch Gerontol Geriatr. 2013;57:110–5.
Rogne S, Vangberg T, Eldevik P, Wikran G, Mathiesen EB, Schirmer H. Magnetic Resonance Volumetry: Prediction of Subjective Memory Complaints and Mild Cognitive Impairment, and Associations with Genetic and Cardiovascular Risk Factors. Dement Geriatr Cogn Dis Extra. 2016;6:529–40.
Striepens N, Scheef L, Wind A, Popp J, Spottke A, Cooper-Mahkorn D, Suliman H, Wagner M, Schild HH, Jessen F. Volume loss of the medial temporal lobe structures in subjective memory impairment. Dement Geriatr Cogn Disord. 2010;29:75–81.
Yue L, Wang T, Wang J, Li G, Wang J, Li X, Li W, Hu M, Xiao S. Asymmetry of Hippocampus and Amygdala Defect in Subjective Cognitive Decline Among the Community Dwelling Chinese. Front Psychiatry. 2018;9:226.
Sanchez-Benavides G, Grau-Rivera O, Suarez-Calvet M, Minguillon C, Cacciaglia R, Gramunt N, Falcon C, Gispert JD, Molinuevo JL. Brain and cognitive correlates of subjective cognitive decline-plus features in a population-based cohort. Alzheimers Res Ther. 2018;10:123.
Hafkemeijer A, Altmann-Schneider I, Oleksik AM, van de Wiel L, Middelkoop HA, van Buchem MA, van der Grond J, Rombouts SA. Increased functional connectivity and brain atrophy in elderly with subjective memory complaints. Brain Connect. 2013;3:353–62.
van Rooden S, van den Berg-Huysmans AA, Croll PH, Labadie G, Hayes JM, Viviano R, van der Grond J, Rombouts S, Damoiseaux JS. Subjective Cognitive Decline Is Associated with Greater White Matter Hyperintensity Volume. J Alzheimers Dis. 2018;66:1283–94.
Nunes T, Fragata I, Ribeiro F, Palma T, Maroco J, Cannas J, Secca M, Menezes C, Carmo I, Cunha G, et al. The outcome of elderly patients with cognitive complaints but normal neuropsychological tests. J Alzheimers Dis. 2010;19:137–45.
Cherbuin N, Sargent-Cox K, Easteal S, Sachdev P, Anstey KJ, Hippocampal Atrophy I. Associated with Subjective Memory Decline: The PATH Through Life Study. The Am J Geriatr Psychiatry. 2015;23:446–55.
Fan LY, Lai YM, Chen TF, Hsu YC, Chen PY, Huang KZ, Cheng TW, Tseng WI, Hua MS, Chen YF, Chiu MJ. Diminution of context association memory structure in subjects with subjective cognitive decline. Hum Brain Mapp. 2018;39:2549–62.
Ryu SY, Lim EY, Na S, Shim YS, Cho JH, Yoon B, Hong YJ, Yang DW. Hippocampal and entorhinal structures in subjective memory impairment: a combined MRI volumetric and DTI study. Int Psychogeriatr. 2017;29:785–92.
Saykin AJ, Wishart HA, Rabin LA, Santulli RB, Flashman LA, West JD, McHugh TL, Mamourian AC. Older adults with cognitive complaints show brain atrophy similar to that of amnestic MCI. Neurology. 2006;67:834–42.
Shen L, Saykin AJ, Kim S, Firpi HA, West JD, Risacher SL, McDonald BC, McHugh TL, Wishart HA, Flashman LA. Comparison of manual and automated determination of hippocampal volumes in MCI and early AD. Brain Imaging Behav. 2010;4:86–95.
Jessen F, Feyen L, Freymann K, Tepest R, Maier W, Heun R, Schild H-H, Scheef L. Volume reduction of the entorhinal cortex in subjective memory impairment. Neurobiol Aging. 2006;27:1751–6.
Platero C, Lopez ME, Carmen Tobar MD, Yus M, Maestu F. Discriminating Alzheimer's disease progression using a new hippocampal marker from T1-weighted MRI: The local surface roughness. Hum Brain Mapp. 2019;40:1666–76.
Tepest R, Wang L, Csernansky JG, Neubert P, Heun R, Scheef L, Jessen F. Hippocampal surface analysis in subjective memory impairment, mild cognitive impairment and Alzheimer's dementia. Dement Geriatr Cogn Disord. 2008;26:323–9.
Striepens N, Scheef L, Wind A, Meiberth D, Popp J, Spottke A, Kolsch H, Wagner M, Jessen F. Interaction effects of subjective memory impairment and ApoE4 genotype on episodic memory and hippocampal volume. Psychol Med. 2011;41:1997–2006.
Sun Y, Wang X, Wang Y, Dong H, Lu J, Scheininger T, Ewers M, Jessen F, Zuo XN, Han Y. Anxiety correlates with cortical surface area in subjective cognitive decline: APOE epsilon4 carriers versus APOE epsilon4 non-carriers. Alzheimers Res Ther. 2019;11:50.
Stewart R, Godin O, Crivello F, Maillard P, Mazoyer B, Tzourio C, Dufouil C. Longitudinal neuroimaging correlates of subjective memory impairment: 4-year prospective community study. Br J Psychiatry. 2011;198:199–205.
Cantero JL, Iglesias JE, Van Leemput K, Atienza M. Regional Hippocampal Atrophy and Higher Levels of Plasma Amyloid-Beta Are Associated With Subjective Memory Complaints in Nondemented Elderly Subjects. J Gerontol A Biol Sci Med Sci. 2016;71:1210–5.
Perrotin A, de Flores R, Lamberton F, Poisnel G, La Joie R, de la Sayette V, Mezenge F, Tomadesso C, Landeau B, Desgranges B, Chetelat G. Hippocampal Subfield Volumetry and 3D Surface Mapping in Subjective Cognitive Decline. J Alzheimers Dis. 2015;48(Suppl 1):S141–50.
Zhao W, Wang X, Yin C, He M, Li S, Han Y. Trajectories of the Hippocampal Subfields Atrophy in the Alzheimer's Disease: A Structural Imaging Study. Frontiers Neuroinform. 2019;13:13.
Scheef L, Grothe MJ, Koppara A, Daamen M, Boecker H, Biersack H, Schild HH, Wagner M, Teipel S, Jessen F. Subregional volume reduction of the cholinergic forebrain in subjective cognitive decline (SCD). NeuroImage. 2019;21:101612.
Meiberth D, Scheef L, Wolfsgruber S, Boecker H, Block W, Traber F, Erk S, Heneka MT, Jacobi H, Spottke A, et al. Cortical thinning in individuals with subjective memory impairment. J Alzheimers Dis. 2015;45:139–46.
Schultz SA, Oh JM, Koscik RL, Dowling NM, Gallagher CL, Carlsson CM, Bendlin BB, LaRue A, Hermann BP, Rowley HA, et al. Subjective memory complaints, cortical thinning, and cognitive dysfunction in middle-aged adults at risk for AD. Alzheimers Dement (Amst). 2015;1:33–40.
Verfaillie SCJ, Tijms B, Versteeg A, Benedictus MR, Bouwman FH, Scheltens P, Barkhof F, Vrenken H, van der Flier WM. Thinner temporal and parietal cortex is related to incident clinical progression to dementia in patients with subjective cognitive decline. Alzheimers Dement. 2016;5:43–52.
Verfaillie SCJ, Slot RE, Tijms BM, Bouwman F, Benedictus MR, Overbeek JM, Koene T, Vrenken H, Scheltens P, Barkhof F, van der Flier WM. Thinner cortex in patients with subjective cognitive decline is associated with steeper decline of memory. Neurobiol Aging. 2018;61:238–44.
Peter J, Scheef L, Abdulkadir A, Boecker H, Heneka M, Wagner M, Koppara A, Kloppel S, Jessen F. Gray matter atrophy pattern in elderly with subjective memory impairment. Alzheimers Dement. 2014;10:99–108.
Friedman EJ, Young K, Tremper G, Liang J, Landsberg AS, Schuff N. Alzheimer's Disease Neuroimaging I: Directed network motifs in Alzheimer's disease and mild cognitive impairment. PLoS One. 2015;10:e0124453.
Li Y, Wang Y, Wu G, Shi F, Zhou L, Lin W, Shen D. Alzheimer's Disease Neuroimaging I: Discriminant analysis of longitudinal cortical thickness changes in Alzheimer's disease using dynamic and network features. Neurobiol Aging. 2012;33:427 e415–30.
Pereira JB, Mijalkov M, Kakaei E, Mecocci P, Vellas B, Tsolaki M, Kloszewska I, Soininen H, Spenger C, Lovestone S, et al. Disrupted network topology in patients with stable and progressive mild cognitive impairment and alzheimer's disease. Cereb Cortex. 2016;26:3476–93.
Verfaillie SCJ, Slot RER, Dicks E, Prins ND, Overbeek JM, Teunissen CE, Scheltens P, Barkhof F, van der Flier WM, Tijms BM. A more randomly organized grey matter network is associated with deteriorating language and global cognition in individuals with subjective cognitive decline. Hum Brain Mapp. 2018;39:3143–51.
Tijms BM, Ten Kate M, Gouw AA, Borta A, Verfaillie S, Teunissen CE, Scheltens P, Barkhof F, van der Flier WM. Gray matter networks and clinical progression in subjects with predementia Alzheimer's disease. Neurobiol Aging. 2018;61:75–81.
Ten Kate M, Visser PJ, Bakardjian H, Barkhof F, Sikkes SAM, van der Flier WM, Scheltens P, Hampel H, Habert MO, Dubois B, Tijms BM. Gray Matter Network Disruptions and Regional Amyloid Beta in Cognitively Normal Adults. Front Aging Neurosci. 2018;10:67.
Le Bihan D. Looking into the functional architecture of the brain with diffusion MRI. Nat Rev Neurosci. 2003;4:469–80.
Bai F, Shu N, Yuan Y, Shi Y, Yu H, Wu D, Wang J, Xia M, He Y, Zhang Z. Topologically convergent and divergent structural connectivity patterns between patients with remitted geriatric depression and amnestic mild cognitive impairment. J Neurosci. 2012;32:4307–18.
Daianu M, Jahanshad N, Nir TM, Jack CR Jr, Weiner MW, Bernstein MA, Thompson PM. Alzheimer's Disease Neuroimaging I: Rich club analysis in the Alzheimer's disease connectome reveals a relatively undisturbed structural core network. Hum Brain Mapp. 2015;36:3087–103.
Lo CY, Wang PN, Chou KH, Wang J, He Y, Lin CP. Diffusion tensor tractography reveals abnormal topological organization in structural cortical networks in Alzheimer's disease. J Neurosci. 2010;30:16876–85.
Wang XN, Zeng Y, Chen GQ, Zhang YH, Li XY, Hao XY, Yu Y, Zhang M, Sheng C, Li YX, Sun Y. Abnormal organization of white matter networks in patients with subjective cognitive decline and mild cognitive impairment. Oncotarget. 2016;7:48953–62.
Zhang Y, Schuff N, Du AT, Rosen HJ, Kramer JH, Gorno-Tempini ML, Miller BL, Weiner MW. White matter damage in frontotemporal dementia and Alzheimer's disease measured by diffusion MRI. Brain. 2009;132:2579–92.
Ito K, Sasaki M, Takahashi J, Uwano I, Yamashita F, Higuchi S, Goodwin J, Harada T, Kudo K, Terayama Y. Detection of early changes in the parahippocampal and posterior cingulum bundles during mild cognitive impairment by using high-resolution multi-parametric diffusion tensor imaging. Psychiatry Res. 2015;231:346–52.
Li XY, Tang ZC, Sun Y, Tian J, Liu ZY, Han Y. White matter degeneration in subjective cognitive decline: a diffusion tensor imaging study. Oncotarget. 2016;7:54405–14.
Wang Y, West JD, Flashman LA, Wishart HA, Santulli RB, Rabin LA, Pare N, Arfanakis K, Saykin AJ. Selective changes in white matter integrity in MCI and older adults with cognitive complaints. Biochim Biophys Acta. 1822;2012:423–30.
Brueggen K, Dyrba M, Cardenas-Blanco A, Schneider A, Fliessbach K, Buerger K, Janowitz D, Peters O, Menne F, Priller J, et al. Structural integrity in subjective cognitive decline, mild cognitive impairment and Alzheimer's disease based on multicenter diffusion tensor imaging. J Neurol. 2019;266:2465–74.
Ohlhauser L, Parker AF, Smart CM, Gawryluk JR. White matter and its relationship with cognition in subjective cognitive decline. Alzheimers Dement. 2019;11:28–35.
Yasuno F, Kazui H, Yamamoto A, Morita N, Kajimoto K, Ihara M, Taguchi A, Matsuoka K, Kosaka J, Tanaka T, et al. Resting-state synchrony between the retrosplenial cortex and anterior medial cortical structures relates to memory complaints in subjective cognitive impairment. Neurobiol Aging. 2015;36:2145–52.
Kiuchi K, Kitamura S, Taoka T, Yasuno F, Tanimura M, Matsuoka K, Ikawa D, Toritsuka M, Hashimoto K, Makinodan M, et al. Gray and white matter changes in subjective cognitive impairment, amnestic mild cognitive impairment and Alzheimer's disease: a voxel-based analysis study. PLoS One. 2014;9:e104007.
Viviano RP, Hayes JM, Pruitt PJ, Fernandez ZJ, van Rooden S, van der Grond J, Rombouts SARB, Damoiseaux JS. Aberrant memory system connectivity and working memory performance in subjective cognitive decline. NeuroImage. 2019;185:556–64.
Selnes P, Fjell AM, Gjerstad L, Bjørnerud A, Wallin A, Due-Tønnessen P, Grambaite R, Stenset V, Fladby T. White matter imaging changes in subjective and mild cognitive impairment. Alzheimers Dement. 2012;8:S112–21.
Lee YM, Ha JK, Park JM, Lee BD, Moon E, Chung YI, Kim JH, Kim HJ, Mun CW, Kim TH, Kim YH. Impact of Apolipoprotein E4 Polymorphism on the Gray Matter Volume and the White Matter Integrity in Subjective Memory Impairment without White Matter Hyperintensities: Voxel-Based Morphometry and Tract-Based Spatial Statistics Study under 3-Tesla MRI. J Neuroimaging. 2016;26:144–9.
Hong YJ, Kim CM, Jang EH, Hwang J, Roh JH, Lee JH. White Matter Changes May Precede Gray Matter Loss in Elderly with Subjective Memory Impairment. Dement Geriatr Cogn Disord. 2016;42:227–35.
Shu N, Wang X, Bi Q, Zhao T, Han Y. Disrupted Topologic Efficiency of White Matter Structural Connectome in Individuals with Subjective Cognitive Decline. Radiology. 2018;286:229–38.
Yan T, Wang W, Yang L, Chen K, Chen R, Han Y. Rich club disturbances of the human connectome from subjective cognitive decline to Alzheimer's disease. Theranostics. 2018;8:3237–55.
Jung NY, Seo SW, Yoo H, Yang JJ, Park S, Kim YJ, Lee J, Lee JS, Jang YK, Lee JM, et al. Classifying anatomical subtypes of subjective memory impairment. Neurobiol Aging. 2016;48:53–60.
Sun Y, Dai Z, Li Y, Sheng C, Li H, Wang X, Chen X, He Y, Han Y. Subjective Cognitive Decline: Mapping Functional and Structural Brain Changes-A Combined Resting-State Functional and Structural MR Imaging Study. Radiology. 2016;281:185–92.
Lauriola M, Esposito R, Delli Pizzi S, de Zambotti M, Londrillo F, Kramer JH, Rabinovici GD, Tartaro A. Sleep changes without medial temporal lobe or brain cortical changes in community-dwelling individuals with subjective cognitive decline. Alzheimers Dement. 2017;13:783–91.
Norton DJ, Amariglio R, Protas H, Chen K, Aguirre-Acevedo DC, Pulsifer B, Castrillon G, Tirado V, Munoz C, Tariot P, et al. Subjective memory complaints in preclinical autosomal dominant Alzheimer disease. Neurology. 2017;89:1464–70.
Risacher SL, Tallman EF, West JD, Yoder KK, Hutchins GD, Fletcher JW, Gao S, Kareken DA, Farlow MR, Apostolova LG, Saykin AJ. Olfactory identification in subjective cognitive decline and mild cognitive impairment: Association with tau but not amyloid positron emission tomography. Alzheimers Dement. 2017;9:57–66.
Zhao W, Luo Y, Zhao L, Mok V, Su L, Yin C, Sun Y, Lu J, Shi L, Han Y. Automated Brain MRI Volumetry Differentiates Early Stages of Alzheimer's Disease From Normal Aging. J Geriatr Psychiatry Neurol. 2019;32:354–64.
Niemantsverdriet E, Ribbens A, Bastin C, Benoit F, Bergmans B, Bier JC, Bladt R, Claes L, De Deyn PP, Deryck O, et al. A Retrospective Belgian Multi-Center MRI Biomarker Study in Alzheimer's Disease (REMEMBER). J Alzheimers Dis. 2018;63:1509–22.
Verfaillie SCJ, Pichet Binette A, Vachon-Presseau E, Tabrizi S, Savard M, Bellec P, Ossenkoppele R, Scheltens P, van der Flier WM, Breitner JCS, Villeneuve S. Subjective Cognitive Decline Is Associated With Altered Default Mode Network Connectivity in Individuals With a Family History of Alzheimer's Disease. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018;3:463–72.
Beauchet O, Launay CP, Chabot J, Levinoff EJ, Allali G. Subjective Memory Impairment and Gait Variability in Cognitively Healthy Individuals: Results from a Cross-Sectional Pilot Study. J Alzheimers Dis. 2017;55:965–71.
Li Y, Wang X, Li Y, Sun Y, Sheng C, Li H, Li X, Yu Y, Chen G, Hu X, et al. Abnormal Resting-State Functional Connectivity Strength in Mild Cognitive Impairment and Its Conversion to Alzheimer’s Disease. Neural Plasticity. 2016;2016:1–12.
Buckner RL. Molecular, structural, and functional characterization of alzheimer's disease: evidence for a relationship between default activity, amyloid, and memory. J Neurosci. 2005;25:7709–17.
Greicius MD, Srivastava G, Reiss AL, Menon V. Default-mode network activity distinguishes Alzheimer’s disease from healthy aging: Evidence from functional MRI. PNAS. 2004;101:4637–42.
Greicius MD, Krasnow B, Reiss AL, Menon V. Functional connectivity in the resting brain: A network analysis of the default mode hypothesis. PNAS. 2003;100:253–8.
Raichle ME, MacLeod AM, Snyder AZ, Powers WJ, Gusnard DA, Shulman GL. A default mode of brain function. PNAS. 2001;98:676–82.
Yang L, Yan Y, Wang Y, Hu X, Lu J, Chan P, Yan T, Han Y. Gradual Disturbances of the Amplitude of Low-Frequency Fluctuations (ALFF) and Fractional ALFF in Alzheimer Spectrum. Front Neurosci. 2018;12:975.
Dillen KNH, Jacobs HIL, Kukolja J, von Reutern B, Richter N, Onurûr A, Dronse J, Langen K-J, Fink GR. Aberrant functional connectivity differentiates retrosplenial cortex from posterior cingulate cortex in prodromal Alzheimer's disease. Neurobiol Aging. 2016;44:114–26.
Dong C, Liu T, Wen W, Kochan NA, Jiang J, Li Q, Liu H, Niu H, Zhang W, Wang Y, et al. Altered functional connectivity strength in informant-reported subjective cognitive decline: A resting-state functional magnetic resonance imaging study. Alzheimers Dement. 2018;10:688–97.
Dillen KNH, Jacobs HIL, Kukolja J, Richter N, von Reutern B, Onur OA, Langen KJ, Fink GR. Functional Disintegration of the Default Mode Network in Prodromal Alzheimer's Disease. J Alzheimers Dis. 2017;59:169–87.
Wang Y, Risacher SL, West JD, McDonald BC, Magee TR, Farlow MR, Gao S, O'Neill DP, Saykin AJ. Altered default mode network connectivity in older adults with cognitive complaints and amnestic mild cognitive impairment. J Alzheimers Dis. 2013;35:751–60.
Chiesa PA, Cavedo E, Vergallo A, Lista S, Potier MC, Habert MO, Dubois B, Thiebaut de Schotten M, Hampel H. Differential default mode network trajectories in asymptomatic individuals at risk for Alzheimer's disease. Alzheimers Dement. 2019;15:940–50.
Kato T, Knopman D, Liu H. Dissociation of regional activation in mild AD during visual encoding: a functional MRI study. Neurology. 2001;57:812–6.
Petrella JR, Wang L, Krishnan S, Slavin MJ, Prince SE, Tran TT, Doraiswamy PM. Cortical deactivation in mild cognitive impairment: high-field-strength functional MR imaging. Radiology. 2007;245:224–35.
Rombouts SA, Barkhof F, Veltman DJ, Machielsen WC, Witter MP, Bierlaagh MA, Lazeron RH, Valk J, Scheltens P. Functional MR imaging in Alzheimer's disease during memory encoding. AJNR Am J Neuroradiol. 2000;21:1869–75.
Sperling RA, Bates JF, Chua EF, Cocchiarella AJ, Rentz DM, Rosen BR, Schacter DL, Albert MS. fMRI studies of associative encoding in young and elderly controls and mild Alzheimer's disease. J Neurol Neurosurg Psychiatry. 2003;74:44–50.
Dumas JA, Kutz AM, McDonald BC, Naylor MR, Pfaff AC, Saykin AJ, Newhouse PA. Increased working memory-related brain activity in middle-aged women with cognitive complaints. Neurobiol Aging. 2013;34:1145–7.
Erk S, Spottke A, Meisen A, Wagner M, Walter H, Jessen F. Evidence of neuronal compensation during episodic memory in subjective memory impairment. Arch Gen Psychiatry. 2011;68:845–52.
Rodda JE, Dannhauser TM, Cutinha DJ, Shergill SS, Walker Z. Subjective cognitive impairment: increased prefrontal cortex activation compared to controls during an encoding task. Int J Geriatr Psychiatry. 2009;24:865–74.
Rodda J, Dannhauser T, Cutinha DJ, Shergill SS, Walker Z. Subjective cognitive impairment: Functional MRI during a divided attention task. Eur Psychiatry. 2011;26:457–62.
Hayes JM, Tang L, Viviano RP, van Rooden S, Ofen N, Damoiseaux JS. Subjective memory complaints are associated with brain activation supporting successful memory encoding. Neurobiol Aging. 2017;60:71–80.
Hu X, Uhle F, Fliessbach K, Wagner M, Han Y, Weber B, Jessen F. Reduced future-oriented decision making in individuals with subjective cognitive decline: A functional MRI study. Alzheimers Dement. 2017;6:222–31.
Hays CC, Zlatar ZZ, Wierenga CE. The Utility of Cerebral Blood Flow as a Biomarker of Preclinical Alzheimer's Disease. Cell Mol Neurobiol. 2016;36:167–79.
Okonkwo OC, Xu G, Oh JM, Dowling NM, Carlsson CM, Gallagher CL, Birdsill AC, Palotti M, Wharton W, Hermann BP, et al. Cerebral blood flow is diminished in asymptomatic middle-aged adults with maternal history of Alzheimer's disease. Cereb Cortex. 2014;24:978–88.
Alexopoulos P, Sorg C, Forschler A, Grimmer T, Skokou M, Wohlschlager A, Perneczky R, Zimmer C, Kurz A, Preibisch C. Perfusion abnormalities in mild cognitive impairment and mild dementia in Alzheimer's disease measured by pulsed arterial spin labeling MRI. Eur Arch Psychiatry Clin Neurosci. 2012;262:69–77.
Bangen KJ, Restom K, Liu TT, Wierenga CE, Jak AJ, Salmon DP, Bondi MW. Assessment of Alzheimer's disease risk with functional magnetic resonance imaging: an arterial spin labeling study. J Alzheimers Dis. 2012;31(Suppl 3):S59–74.
Binnewijzend MA, Kuijer JP, Benedictus MR, van der Flier WM, Wink AM, Wattjes MP, van Berckel BN, Scheltens P, Barkhof F. Cerebral blood flow measured with 3D pseudocontinuous arterial spin-labeling MR imaging in Alzheimer disease and mild cognitive impairment: a marker for disease severity. Radiology. 2013;267:221–30.
Yoshiura T, Hiwatashi A, Yamashita K, Ohyagi Y, Monji A, Takayama Y, Nagao E, Kamano H, Noguchi T, Honda H. Simultaneous measurement of arterial transit time, arterial blood volume, and cerebral blood flow using arterial spin-labeling in patients with Alzheimer disease. AJNR Am J Neuroradiol. 2009;30:1388–93.
Alsop DC, Detre JA, Grossman M. Assessment of cerebral blood flow in Alzheimer's disease by spin-labeled magnetic resonance imaging. Ann Neurol. 2000;47:93–100.
Mak HK, Chan Q, Zhang Z, Petersen ET, Qiu D, Zhang L, Yau KK, Chu LW, Golay X. Quantitative assessment of cerebral hemodynamic parameters by QUASAR arterial spin labeling in Alzheimer's disease and cognitively normal Elderly adults at 3-tesla. J Alzheimers Dis. 2012;31:33–44.
Asllani I, Habeck C, Scarmeas N, Borogovac A, Brown TR, Stern Y. Multivariate and univariate analysis of continuous arterial spin labeling perfusion MRI in Alzheimer's disease. J Cereb Blood Flow Metab. 2008;28:725–36.
Thambisetty M, Beason-Held L, An Y, Kraut MA, Resnick SM. APOE epsilon4 genotype and longitudinal changes in cerebral blood flow in normal aging. Arch Neurol. 2010;67:93–8.
Wierenga CE, Clark LR, Dev SI, Shin DD, Jurick SM, Rissman RA, Liu TT, Bondi MW. Interaction of age and APOE genotype on cerebral blood flow at rest. J Alzheimers Dis. 2013;34:921–35.
Hays CC, Zlatar ZZ, Campbell L, Meloy MJ, Wierenga CE. Subjective Cognitive Decline Modifies the Relationship Between Cerebral Blood Flow and Memory Function in Cognitively Normal Older Adults. J Int Neuropsychol Soc. 2018;24:213–23.
de Eulate RG, Goni I, Galiano A, Vidorreta M, Recio M, Riverol M, Zubieta JL, Fernandez-Seara MA. Reduced Cerebral Blood Flow in Mild Cognitive Impairment Assessed Using Phase-Contrast MRI. J Alzheimers Dis. 2017;58:585–95.
Leeuwis AE, Benedictus MR, Kuijer JPA, Binnewijzend MAA, Hooghiemstra AM, Verfaillie SCJ, Koene T, Scheltens P, Barkhof F, Prins ND, van der Flier WM. Lower cerebral blood flow is associated with impairment in multiple cognitive domains in Alzheimer's disease. Alzheimers Dement. 2017;13:531–40.
Yang L, Yan Y, Li Y, Hu X, Lu J, Chan P, Yan T, Han Y. Frequency-dependent changes in fractional amplitude of low-frequency oscillations in Alzheimer's disease: a resting-state fMRI study. Brain Imaging Behav. 2019.
Fernandez A, Hornero R, Mayo A, Poza J, Gil-Gregorio P, Ortiz T. MEG spectral profile in Alzheimer’s disease and mild cognitive impairment. Clin Neurophysiol. 2006;117:306–14.
Garces P, Vicente R, Wibral M, Pineda-Pardo JA, Lopez ME, Aurtenetxe S, Marcos A, de Andres ME, Yus M, Sancho M, et al. Brain-wide slowing of spontaneous alpha rhythms in mild cognitive impairment. Front Aging Neurosci. 2013;5:100.
Lopez-Sanz D, Bruna R, Garces P, Martin-Buro MC, Walter S, Delgado ML, Montenegro M, Lopez Higes R, Marcos A, Maestu F. Functional Connectivity Disruption in Subjective Cognitive Decline and Mild Cognitive Impairment: A Common Pattern of Alterations. Front Aging Neurosci. 2017;9:109.
Neto E, Allen EA, Aurlien H, Nordby H, Eichele T. EEG Spectral Features Discriminate between Alzheimer's and Vascular Dementia. Front Neurol. 2015;6:25.
Stam C, Jones B, Nolte G, Breakspear M, Scheltens P. Small-World Networks and Functional Connectivity in Alzheimer's Disease. Cereb Cortex. 2006;17:92–9.
Alexander DM, Arns MW, Paul RH, Rowe DL, Cooper N, Esser AH, Fallahpour K, Stephan BC, Heesen E, Breteler R, et al. EEG markers for cognitive decline in elderly subjects with subjective memory complaints. J Integr Neurosci. 2006;5:49–74.
Babiloni C, Visser PJ, Frisoni G, De Deyn PP, Bresciani L, Jelic V, Nagels G, Rodriguez G, Rossini PM, Vecchio F, et al. Cortical sources of resting EEG rhythms in mild cognitive impairment and subjective memory complaint. Neurobiol Aging. 2010;31:1787–98.
Gouw AA, Alsema AM, Tijms BM, Borta A, Scheltens P, Stam CJ, van der Flier WM. EEG spectral analysis as a putative early prognostic biomarker in nondemented, amyloid positive subjects. Neurobiol Aging. 2017;57:133–42.
Prichep LS, John ER, Ferris SH, Rausch L, Fang Z, Cancro R, Torossian C, Reisberg B. Prediction of longitudinal cognitive decline in normal elderly with subjective complaints using electrophysiological imaging. Neurobiol Aging. 2006;27:471–81.
Lopez-Sanz D, Bruna R, Garces P, Camara C, Serrano N, Rodriguez-Rojo IC, Delgado ML, Montenegro M, Lopez-Higes R, Yus M, Maestu F. Alpha band disruption in the AD-continuum starts in the Subjective Cognitive Decline stage: a MEG study. Sci Rep. 2016;6:37685.
Maestu F, Baykova E, Ruiz JM, Montejo P, Montenegro M, Llanero M, Solesio E, Gil P, Yubero R, Paul N, et al. Increased biomagnetic activity in healthy elderly with subjective memory complaints. Clin Neurophysiol. 2011;122:499–505.
Lopez-Sanz D, Garces P, Alvarez B, Delgado-Losada ML, Lopez-Higes R, Maestu F. Network Disruption in the Preclinical Stages of Alzheimer's Disease: From Subjective Cognitive Decline to Mild Cognitive Impairment. Int J Neural Syst. 2017;27:1750041.
Teipel S, Bakardjian H, Gonzalez-Escamilla G, Cavedo E, Weschke S, Dyrba M, Grothe MJ, Potier MC, Habert MO, Dubois B, Hampel H. No association of cortical amyloid load and EEG connectivity in older people with subjective memory complaints. Neuroimage Clin. 2018;17:435–43.
Chetelat G. Multimodal Neuroimaging in Alzheimer's Disease: Early Diagnosis, Physiopathological Mechanisms, and Impact of Lifestyle. J Alzheimers Dis. 2018;64:S199–s211.
Chetelat G, Villemagne VL, Pike KE, Baron JC, Bourgeat P, Jones G, Faux NG, Ellis KA, Salvado O, Szoeke C, et al. Larger temporal volume in elderly with high versus low beta-amyloid deposition. Brain. 2010;133:3349–58.
Chetelat G, Villemagne VL, Bourgeat P, Pike KE, Jones G, Ames D, Ellis KA, Szoeke C, Martins RN, O'Keefe GJ, et al. Relationship between atrophy and beta-amyloid deposition in Alzheimer disease. Ann Neurol. 2010;67:317–24.
Teipel SJ, Cavedo E, Weschke S, Grothe MJ, Rojkova K, Fontaine G, Dauphinot L, Gonzalez-Escamilla G, Potier M-C, Bertin H, et al. Cortical amyloid accumulation is associated with alterations of structural integrity in older people with subjective memory complaints. Neurobiol Aging. 2017;57:143–52.
Ferreira D, Falahati F, Linden C, Buckley RF, Ellis KA, Savage G, Villemagne VL, Rowe CC, Ames D, Simmons A, Westman E. A ‘Disease Severity Index’ to identify individuals with Subjective Memory Decline who will progress to mild cognitive impairment or dementia. Sci Rep. 2017;7:44368.
Wirth M, Bejanin A, La Joie R, Arenaza-Urquijo EM, Gonneaud J, Landeau B, Perrotin A, Mezenge F, de La Sayette V, Desgranges B, Chetelat G. Regional patterns of gray matter volume, hypometabolism, and beta-amyloid in groups at risk of Alzheimer's disease. Neurobiol Aging. 2018;63:140–51.
Chiesa PA, Cavedo E, Grothe MJ, Houot M, Teipel SJ, Potier MC, Habert MO, Lista S, Dubois B, Hampel H. Relationship between Basal Forebrain Resting-State Functional Connectivity and Brain Amyloid-beta Deposition in Cognitively Intact Older Adults with Subjective Memory Complaints. Radiology. 2019;290:167–76.
Dubois B, Hampel H, Feldman HH, Scheltens P, Aisen P, Andrieu S, Bakardjian H, Benali H, Bertram L, Blennow K, et al. Preclinical Alzheimer's disease: Definition, natural history, and diagnostic criteria. Alzheimers Dement. 2016;12:292–323.
Li K, Luo X, Zeng Q, Jiaerken Y, Xu X, Huang P, Shen Z, Xu J, Wang C, Zhou J, Zhang MM. Aberrant functional connectivity network in subjective memory complaint individuals relates to pathological biomarkers. Transl Neurodegen. 2018;7.
Kramberger MG, Giske K, Cavallin L, Kåreholt I, Andersson T, Winblad B, Jelic V. Subclinical white matter lesions and medial temporal lobe atrophy are associated with EEG slowing in a memory clinic cohort. Clin Neurophysiol. 2017;128:1575–82.
Gaubert S, Raimondo F, Houot M, Corsi MC, Naccache L, Diego Sitt J, Hermann B, Oudiette D, Gagliardi G, Habert MO, et al. EEG evidence of compensatory mechanisms in preclinical Alzheimer's disease. Brain. 2019;142:2096–112.
Buckley RF, Hanseeuw B, Schultz AP, Vannini P, Aghjayan SL, Properzi MJ, Jackson JD, Mormino EC, Rentz DM, Sperling RA, et al. Region-Specific Association of Subjective Cognitive Decline With Tauopathy Independent of Global beta-Amyloid Burden. JAMA Neurol. 2017;74:1455–63.
Shokouhi S, Conley AC, Baker SL, Albert K, Kang H, Gwirtsman HE, Newhouse PA. The relationship between domain-specific subjective cognitive decline and Alzheimer's pathology in normal elderly adults. Neurobiol Aging. 2019;81:22–9.
Kuhn E, Moulinet I, Perrotin A, La Joie R, Landeau B, Tomadesso C, Bejanin A, Sherif S, De La Sayette V, Desgranges B, et al. Cross-sectional and longitudinal characterization of SCD patients recruited from the community versus from a memory clinic: subjective cognitive decline, psychoaffective factors, cognitive performances, and atrophy progression over time. Alzheimers Res Ther. 2019;11:61.
Eliassen CF, Reinvang I, Selnes P, Grambaite R, Fladby T, Hessen E. Biomarkers in subtypes of mild cognitive impairment and subjective cognitive decline. Brain Behav. 2017;7:e00776.
Beckett LA, Donohue MC, Wang C, Aisen P, Harvey DJ, Saito N. The Alzheimer's Disease Neuroimaging Initiative phase 2: Increasing the length, breadth, and depth of our understanding. Alzheimers Dement. 2015;11:823–31.
Dufouil C, Dubois B, Vellas B, Pasquier F, Blanc F, Hugon J, Hanon O, Dartigues JF, Harston S, Gabelle A, et al. Cognitive and imaging markers in non-demented subjects attending a memory clinic: study design and baseline findings of the MEMENTO cohort. Alzheimers Res Ther. 2017;9:67.
Rodriguez-Gomez O, Sanabria A, Perez-Cordon A, Sanchez-Ruiz D, Abdelnour C, Valero S, Hernandez I, Rosende-Roca M, Mauleon A, Vargas L, et al. FACEHBI: A Prospective Study of Risk Factors, Biomarkers and Cognition in a Cohort of Individuals with Subjective Cognitive Decline. Study Rationale and Research Protocols. J Prev Alzheimers Dis. 2017;4:100–8.
Dubois B, Epelbaum S, Nyasse F, Bakardjian H, Gagliardi G, Uspenskaya O, Houot M, Lista S, Cacciamani F, Potier MC, et al. Cognitive and neuroimaging features and brain beta-amyloidosis in individuals at risk of Alzheimer’s disease (INSIGHT-preAD): a longitudinal observational study. Lancet Neurol. 2018;17:335–46.
Jessen F, Spottke A, Boecker H, Brosseron F, Buerger K, Catak C, Fliessbach K, Franke C, Fuentes M, Heneka MT, et al. Design and first baseline data of the DZNE multicenter observational study on predementia Alzheimer's disease (DELCODE). Alzheimers Res Ther. 2018;10:15.
Li X, Wang X, Su L, Hu X, Han Y. Sino Longitudinal Study on Cognitive Decline (SILCODE): protocol for a Chinese longitudinal observational study to develop risk prediction models of conversion to mild cognitive impairment in individuals with subjective cognitive decline. BMJ Open. 2019;9:e028188.
Sajda P. Machine learning for detection and diagnosis of disease. Annu Rev Biomed Eng. 2006;8:537–65.
Da X, Toledo JB, Zee J, Wolk DA, Xie SX, Ou Y, Shacklett A, Parmpi P, Shaw L, Trojanowski JQ, et al. Integration and relative value of biomarkers for prediction of MCI to AD progression: spatial patterns of brain atrophy, cognitive scores, APOE genotype and CSF biomarkers. NeuroImage Clin. 2014;4:164–73.
Davatzikos C, Xu F, An Y, Fan Y, Resnick SM. Longitudinal progression of Alzheimer’s-like patterns of atrophy in normal older adults: the SPARE-AD index. Brain. 2009;132:2026–35.
Toledo JB, Da X, Bhatt P, Wolk DA, Arnold SE, Shaw LM, Trojanowski JQ, Davatzikos C. Relationship between plasma analytes and SPARE-AD defined brain atrophy patterns in ADNI. PLoS One. 2013;8:e55531.
Chincarini A, Bosco P, Gemme G, Esposito M, Rei L, Squarcia S, Bellotti R, Minthon L, Frisoni G, Scheltens P, et al. Automatic temporal lobe atrophy assessment in prodromal AD: Data from the DESCRIPA study. Alzheimers Dement. 2014;10:456–67.
Yan T, Wang Y, Weng Z, Du W, Liu T, Chen D, Li X, Wu J, Han Y. Early-Stage Identification and Pathological Development of Alzheimer's Disease Using Multimodal MRI. J Alzheimers Dis. 2019;68:1013–27.
Lopez-Sanz D, Bruna R, Delgado-Losada ML, Lopez-Higes R, Marcos-Dolado A, Maestu F, Walter S. Electrophysiological brain signatures for the classification of subjective cognitive decline: towards an individual detection in the preclinical stages of dementia. Alzheimers Res Ther. 2019;11:49.
Cole JH, Franke K. Predicting Age Using Neuroimaging: Innovative Brain Ageing Biomarkers. Trends Neurosci. 2017;40:681–90.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Key Research and Development Program of China (2016YFC1306300, 2018YFC1312001), National Natural Science Foundation of China (61633018, 81671761, 81871425), Beijing Municipal Commission of Health and Family Planning (PXM2020_026283_000002), Beijing Nature Science Foundation (7161009) and Fundamental Research Funds for the Central University (2017XTCX04).
Author information
Authors and Affiliations
Contributions
YH, NS, and YS conceived and designed the manuscript. XW and WH contributed equally to search literature, tabulate the results and write the manuscript. LS and YX revised and provided critical input to the manuscript. YS, NS, and YH revised and finalized the review. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, X., Huang, W., Su, L. et al. Neuroimaging advances regarding subjective cognitive decline in preclinical Alzheimer’s disease. Mol Neurodegeneration 15, 55 (2020). https://doi.org/10.1186/s13024-020-00395-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13024-020-00395-3