
Abstract
During chronic liver injury, hepatic stellate cells (HSC) are activated and proliferate, which causes excessive extracellular matrix (ECM) deposition, leading to scar formation and fibrosis. Medicinal plants are gaining popularity as antifibrotic agents, and are often safe, cost-effective, and versatile. This review aims to describe the protective role and mechanisms of medicinal plants in the inhibition of HSC activation and ECM deposition during the pathogenesis of liver fibrosis. A systematic literature review on the anti-fibrotic mechanisms of hepatoprotective plants was performed in PubMed, which yielded articles about twelve relevant plants. Many of these plants act via disruption of the transforming growth factor beta 1 signaling pathway, possibly through reduction in oxidative stress. This reduction could explain the inhibition of HSC activation and reduction in ECM deposition. Medicinal plants could be a source of anti-liver fibrosis compounds.
Similar content being viewed by others


Introduction
Liver fibrosis is caused by inappropriate tissue repair via connective tissue deposition, which results from chronic liver injuries, including those from alcohol, chronic viral hepatitis, autoimmune diseases, parasites, metabolic diseases, and toxins or other drugs [1]. When fibrosis is not controlled, it can progress into cirrhosis. Cirrhosis was previously considered to be irreversible, but some studies suggest that fibrosis and cirrhosis could be reversible [2].
Liver fibrosis is a public health problem that results in significant morbidity and mortality [3]. Hundreds of thousands of people worldwide suffer from cirrhosis, partially because of the obesity pandemic combined with the high incidence of alcohol abuse and viral hepatitis [4]. Chronic viral hepatitis (B and C), alcoholic liver disease, and nonalcoholic fatty liver disease are the three most common causes of liver cirrhosis [5]. The prevalence of chronic liver diseases is predicted to increase, partially owing to the rising prevalence of obesity and metabolic syndrome, especially in developed countries [6].
The pathogenesis of liver fibrosis is complex and varies among different kinds of hepatic injuries. Usually after acute liver damage, parenchymal cells are regenerated to replace the necrotic and apoptotic cells. This regenerative process is associated with an inflammatory response and a limited deposition of extracellular matrix (ECM). When the liver is subjected to chronic injury, the regenerative response fails and hepatocytes are replaced with abundant ECM, which is mainly composed of collagen types I, III, and IV; fibronectin; elastin; laminin; and proteoglycans [7]. Hepatic stellate cells (HSC) are the main source of ECM [8].
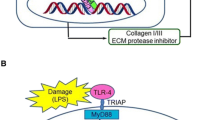
There is no standard treatment for liver fibrosis [7], but a reduction in liver injury events, such as cessation of alcohol intake or successful viral hepatitis treatment can control fibrosis. Nevertheless, these actions are often insufficient to avoid eventual progression to cirrhosis in the vast majority of patients [9]. Although important advances have been made in understanding the pathogenesis of hepatic fibrosis over the past 20 years, efficient antifibrotic drugs have yet to be developed. There are two ways by which medicinal plants and their bioactive compounds and extracts could reduce liver fibrosis: via inhibition of HSC activation and via reduction of ECM deposition (Figure 1). Liver fibrosis treatment should take into account the versatility of its pathogenesis and should act upon all pathways involved, beginning with HSC activation and ECM deposition.

Antifibrotic medicinal plants targeting HSC activation and ECM deposition. HSC: hepatic stellate cells, ECM: extracellular matrix, 1: C. longsa, S. marianum, G. biloba, S. miltiorrhiza, G. glabra, S. baicalensis, B. falcatum, Phyllanthus species, B. aristata, Ginseng species, A. paniculata, and Coffea species. 2: C. longa, S. marianum, G. biloba, S. miltiorrhiza, G. glabra, S. baicalensis, B. falcatum, Phyllanthus species, B. aristata, Ginseng species, and Coffea species.
Medicinal plants are often safe, cost-effective, and versatile, and are therefore popular potential antifibrotic agents. This review aims to describe the role of some hepatoprotective plants in the inhibition of HSC activation and ECM deposition in the pathogenesis of liver fibrosis. These plants include: Curcuma longa, Silybum marianum, Ginkgo biloba, Salvia miltiorrhiza, Glycyrrhiza glabra, Scutellaria baicalensis, Bupleurum falcatum, Phyllanthus species, Berberis aristata, Ginseng species, Andrographis paniculata, and Coffea species.
Literature inclusion criteria
The 12 plant species were selected because of their known hepatoprotective activities. A three-step progressive searching method was applied using PubMed. In each of the steps, only pertinent articles were selected. First, a global search on the liver activity of each plant species was undertaken using the keywords “liver” and “plant species name”. The antifibrotic activities were classified under two different pathways: inhibition of HSC activation and suppression of ECM deposition. Bioactive compounds and extracts from every reviewed species were selected. Second, a more advanced search was performed using the terms “liver fibrosis” and “plant species name or bioactive extract name or bioactive compound name”. Finally, a search on the antifibrotic mechanisms of each species was performed using the terms “hepatic stellate cells activation”, “extracellular matrix”, “collagen”, and “plant species name or bioactive extract name or bioactive compound name”.
Inhibition of hepatic stellate cell activation
Role of hepatic stellate cell activation in the pathogenesis of liver fibrosis
HSC activation, which includes initiation and perpetuation, is an early event in liver fibrogenesis. The activation of HSCs converts normal, quiescent vitamin A-rich cells into myofibroblast-like cells characterized by proliferation, chemotaxis, fibrogenesis, contractility, matrix degradation, retinoid loss, and white blood cell chemoattractant/cytokine release [10]-[14].
HSCs are initiated when gene expression and phenotype changes render the quiescent cells responsive to other cytokines and stimuli [10],[12]. Several paracrine stimuli from damaged hepatocytes and other neighboring cell types, such as Kupffer cells, platelets, sinusoidal endothelium, and immune cells initiate the activation of HSCs [15]. Transforming growth factor beta 1 (TGF-β1), platelet-derived growth factor (PDGF), and epidermal growth factor (EGF) mediate platelet stimuli [15],[16]. By producing fibronectin and activating latent TGF-β1, injured endothelial cells provoke HSC activation. Kupffer cells are important sources of paracrine stimuli for HSCs because they express TGF-β1, transforming growth factor alpha (TGF-α), reactive oxygen species, and lipid peroxides. These Kupffer cell paracrines lead to matrix synthesis, cell proliferation, and the release of retinoids [15] and matrix metalloproteinase (MMP)-9 [17] for collagen synthesis through the activation of latent TGF-β1 [18]. Kupffer cells also inhibit fibrogenesis via the production of anti-inflammatory interleukin-10 and nitric oxide (NO), which decrease collagen synthesis, increase collagenase production, and reduce cell proliferation and contractility [15]. All these stimuli trigger important changes in the composition of ECM, especially an increase in type I and III fibril-forming collagens and fibronectin [10]. This compositional transformation of the matrix induces new fibrogenic stimuli, which further exacerbate fibrosis [12].
During HSC activation, regulatory pathways like epigenetic regulation of nuclear factor kappa B (NF-κB) and reduction in peroxisome proliferator-activated receptor gamma (PPARγ) expression modulate the expression of many genes, such as type I collagen (α1 and α2 chains), smooth muscle α-actin, TGF-β1, TGF-β receptors (TβRI and II), MMP-2, and tissue inhibitor of metalloproteinases (TIMP)-1 and −2 [10],[12].
Perpetuation of HSC activation results in maintenance of the activated phenotype and therefore the generation of fibrosis [15]. Scars are formed through changes in HSC behavior, like proliferation, fibrogenesis, contractility, chemotaxis, retinoid loss, white blood cell chemoattractant/cytokine release, and matrix degradation [12].
Cell proliferation further promotes liver fibrosis by increasing the number of collagen-producing cells. Several mitogens have been identified to be responsible in liver fibrosis, namely PDGF; vascular endothelial growth factor (VEGF); thrombin and its receptor, EGF; TGF-α; keratinocyte growth factor; insulin-like growth factor; protease-activated receptor agonists; basic fibroblast growth factor; monocyte chemotactic factor; interleukin-6; connective tissue growth factor (CTGF); endothelin-1; and angiotensin-II [11],[12],[19].
HSCs migrate towards injured areas in the liver, which increases the fibrogenic response at a specific site via mediation of several chemoattractants, including PDGF, monocyte chemoattractant protein-1 (MCP-1), and chemokine receptor CXCR3 [10],[12].
Fibrogenesis is defined as increased fibrotic matrix production, especially that of collagen type I [12]. TGF-β1, produced by HSCs and other neighboring cell types like Kupffer cells, sinusoidal endothelial cells, bile duct epithelial cells, and hepatocytes [11], is a potent fibrogenic signal [20] as it increases the production of collagen I and other matrix constituents like fibronectin and proteoglycans [12],[21]. These effects are induced by the interaction between TGF-β1 and the membrane receptor complex formed by TβRI and TβRII, leading to the phosphorylation of intracellular mediators, namely Smad proteins. Smad proteins are divided into three groups: receptor-activated Smad (R-Smad), common-Smad (Co-Smad) and inhibitory-Smad (I-Smad). Phosphoylated R-Smad (Smad1, Smad2, Smad3, Smad5 and Smad8) dissociate from anchoring proteins and associate with Co-Smad (Smad4). R-Smad-Co-Smad complexes are transported into the nucleus where they act as transcription factors. This cascade is inhibited by I-Smad (Smad6 and Smad7) [20]. CTGF (through TGF-β-dependent and -independent pathways), endothelin-1, leptin, and angiotensin II have also been reported as fibrogenic factors for HSCs [11],[22].
Stellate cell contractility is associated with portal hypertension and may lead to the collapse and shrunken state of cirrhotic livers [23]. The increased expression of contractile proteins, smooth muscle α-actin, and smooth muscle myosins via calcium-dependent and calcium-independent pathways mediate the contractility of HSCs [11]. Endothelin-1, NO, angiotensinogen II, eicosanoids, atrial natriuretic peptide, somatostatin, and carbon monoxide are some of the signals that contribute to the contractile phenotype of HSCs [12]. Because HSCs are so important to fibrogenesis, the inhibition of HSC activation is a possible therapeutic approach to reversing liver fibrosis [1],[4]. For instance, PPARγ ligands [24], interferon gamma (IFNγ) [25], and antioxidants [26] reduce liver fibrosis by inhibiting TGF-β1 expression and therefore HSC activation.
Hepatic stellate cell activation as a target of antifibrotic medicinal plants
All the reviewed medicinal plants were shown to suppress HSC activation. Since the activation of HSCs occurs via a complex network of signaling pathways, different targets have been investigated to explain the antifibrotic activity (Table 1).
Activation of TGF-β1/Smad signaling is one of the most important profibrogenic pathways [20]. The disruption of this pathway is a common feature of all of the reviewed antifibrotic plants. Down-regulation of the expression of TGF-β1 and its receptors, TβRI and II, and modulation of its mediators Smad 2, 3, and 7 has been observed via curcumin [28],[30],[32],[34],[37],[38] and compounds from S. miltiorrhiza[49],[66],[70],[75]-[78],[83],[88]-[91],[98], G. glabra[102],[103] and Coffea species [120]-[128]. Several mechanisms have been identified for the inhibition of TGF-β1 signaling via curcumin, like PPARγ activation and antioxidation. Curcumin inhibits NF-κB [27], leptin [39], advanced glycation end-product (AGE) [33], low-density lipoprotein (LDL) [40],[41], and insulin [42] mediated HSC activation by stimulating PPARγ activity and inducing de novo synthesis of glutathione [27],[33],[39] − [42]. Inhibition of NF-κB and stimulation of PPARγ activities are also observed in G. biloba extract [56],[57], 18α glycyrrhizin [101], glycyrrhetinic acid [104], and baicalin [107]. Salianic acid B and salvianolic acid B inhibited p38 mitogen-activated protein kinases [88],[90],[94],[99],[100] and extracellular signal-regulated kinases (ERK) signaling [46],[90],[92],[94],[96],[98],[100] by blocking phosphorylation of mitogen-activated protein kinase kinase 3/6, inhibiting expression of myocyte enhancer factor-2 [94], and suppressing phosphorylation of mitogen-activated protein kinase kinase [96],[100], in activated HSCs. Further, salvianolic acid B reduced hepatic fibrosis by disrupting angiotensin II signaling via down-regulation of angiotensin II receptor type 1, ERK, and c-Jun phosphorylation [98]. Andrographolide from A. paniculata decreased the hepatic level of cannabinoid receptor 1 via inactivation of c-Jun N-terminal kinases and the ERK phosphorylation cascade [119].
HSC proliferation is mediated by different proteins, including PDGF, CTGF, VEGF, and TGF-α through various signal molecules, such as ERK and focal adhesion kinase (FAK) [12]. Some plant extracts target these growth factors and their respective signaling pathways to reduce the proliferative response of HSCs. CTGF is inhibited by curcumin [34],[36], silymarin [54], G. biloba extract [59], Salvia extract [49],[76], and caffeine [120],[128]-[130]via inhibition of TGF-β signaling. Moreover, curcumin was shown to reduce the promoter activity of CTGF and suppress its gene expression by reducing NF-κB activity [36]. NF-κB was inhibited by suppression of ERK activity and suppression of Toll like receptor-4 gene expression via PPARγ activation [36].
PDGF and its receptor PDGF-βR were found to be down-regulated by curcumin [35],[37], salvianolic acid A [63] and B [92], coffee [123], and ginsenoside Rg1 [116]. Ginsenoside Rg1 down-regulated the expression of PDGF-βR by reducing NF-κB activity [116]. Different bioactive compounds from S. miltiorrhiza reduced HSC proliferation. The monomer IH764-3 inhibited HSC proliferation by down-regulating FAK and ERK expression [64],[65],[80], while salvianolic acid B attenuated PDGF-induced c-Jun N-terminal kinases, p38, and protein kinase C delta phosphorylations [95].
VEGF and its receptors were suppressed by curcumin [45] and coffee [122], which could also explain their amelioration of angiogenesis in the fibrotic liver. Additionally, curcumin reduced TGF-α levels [43].
Cyclins, and cyclin inhibitors, are essential proteins for the control of the cell cycle, and potential therapeutic targets for inhibiting HSC proliferation. The cyclin D1 gene was down-regulated by curcumin through PPARγ activation [30]. Inhibition of HSC proliferation by salvianolic acid A was mediated by the induction of cell cycle inhibitory proteins p21 and p27, down-regulation of cyclins D1 and E, and suppression of protein kinase B phosphorylation [63].
Medicinal plants also regulate the contraction of HSCs. For example, salvianolic acid B lowered portal pressure and attenuated the contraction of HSC by inhibiting the Ras homolog family member A signaling pathway [97] and decreasing the HSC free calcium ion concentration [93].
Reduction in extracellular matrix deposition
Role of extracellular matrix deposition in the pathogenesis of liver fibrosis
Liver fibrosis is a dynamic process in which the equilibrium between ECM synthesis and degradation is impaired [11]. HSCs, neutrophils, and macrophages are the main cellular contributors to ECM degradation [1], while HSCs, portal myofibroblasts, bone-marrow-derived cells, and the epithelial–mesenchymal transition are responsible for ECM synthesis [14]. All these cells involve several molecular effectors such as matrix proteins, MMPs and TIMPs.
During fibrogenesis, several ECM proteins, especially collagens type I, III, and IV; proteoglycans; laminin; and fibronectin are over-expressed by activated HSCs and other cells, which results in pathological scar formation [131]. Accumulation of ECM not only depends on up-regulation of ECM production, but also on MMP–TIMP expression [132],[133]. In the early phases of liver injury, HSCs transiently express MMP-3 and MMP-13, which is a matrix-degrading phenotype. In the later stages of liver injury, the inhibition of fibrillar liver collagen degradation prevails over ECM synthesis, as evidenced by increased TIMP-1 expression, which leads to a decrease in collagen degradation by MMP-1 and MMP-13 [133]. TIMP-1 was found to protect HSCs from apoptosis [134]. Regulation of the plasminogen activation system, including enhanced production of the urokinase-plasminogen activator (uPA) and uPA receptor and modulation of plasminogen activator inhibitor type 1 (PAI-1), is another method by which HSCs regulate the ECM [135]-[137]. Macrophages also take part in matrix breakdown [9],[138], since macrophages produce MMPs, like MMP-13 [139],[140] and MMP-9 [141],[142] through the mitogen-activated protein kinase and NF-κB pathways [143].
The dynamic process of matrix degradation and synthesis could be a therapeutic target to reversing liver fibrosis and restoring normal liver architecture [4],[11],[144]. Indeed, MMP-8 cloned into an adenoviral vector reversed fibrosis in cirrhotic animal livers [145]. In vivo reduction of liver fibrosis has also been observed with similar therapeutic approaches involving MMP-1 [146], TIMP-1 scavengers [147], and uPA [148].
Extracellular matrix deposition as a target of antifibrotic medicinal plants
All of the reviewed medicinal plants, except A. paniculata, were shown to reduce ECM deposition. Plant compound targets include multiple components of the ECM, such as collagen species, laminin, and fibronectin, as well as MMPs, TIMPs, and the plasminogen activation system (Table 2).
Curcumin, silymarin, silybin, silibinin, G. biloba extracts like GbE761, salvianolic acids A and B, salianic acid B, S. miltiorrhiza extracts, magnesium lithospermate B, tanshinone IIA, monomer IH764-3, glycyrrhizin, glycyrrhetinic acid, glycyrrhizic acid, baicalin, saikosaponin A and D, P. amarus extracts, berberine, P. notoginseng saponins, ginsenoside Rb1, red ginseng extract, conventional and decaffeinated coffee, 1,7-dimethylxanthine, caffeine, and chlorogenic acid, reduced hepatic collagen content by down-regulating hepatic expression of type I and III collagen and/or decreasing the serum levels of type III procollagen and type IV collagen. Fibronectin expression was reduced by curcumin [37]. Serum levels of laminin and hyaluronic acid were lowered by curcumin, G. biloba extracts like GbE761, salvianolic acid B, SMND-309, baicalin, saikosaponin D, and P. notoginseng saponins. Expression of MMPs, like MMP-1, −2, −7, −9, and −13, were enhanced by curcumin [30],[43],[154],[157], G. biloba extract [166], S. miltiorrhiza[66],[77], salianic acid B [90], monomer IH764-3 [178], glycyrrhizin [181], baicalin [105], berberine [114], and P. notoginseng saponins [185], which stimulate the degradation of collagen deposits. However, MMPs have been observed to be downregulated after treatment with curcumin [158], silymarin [50],[51], S. miltiorrhiza[172], salvianolic acid B [175], ethanol extract of P. niruri[111], ginsenoside Rb1 [117], conventional and decaffeinated coffee, and caffeine [125],[126],[128]. Tissue remodeling induced by MMPs progresses liver fibrosis, so reducing MMP expression could be an antifibrotic strategy. Moreover, curcumin, silymarin, G. biloba extract, S. miltiorrhiza, monomer IH764-3, baicalin, P. amarus extract, P. notoginseng saponins, and ginsenoside Rb1 inhibited the expression of TIMP-1 and −2. Salvianic acid A (danshensu) and red ginseng extract down-regulated the expression of PAI-1 [173],[184], while salvianic acid A up-regulated uPA expression [173].
Since ECM proteins, MMPs, and TIMPS are over-expressed when HSCs are activated, the inhibition of HSC activation and proliferation is the main method by which plants can suppress ECM deposition. The antifibrotic mechanism is mainly the result of down-regulating the TGF-β1/Smad signaling pathway.
Highlights
Inhibition of HSC activation and subsequent ECM deposition via medicinal plants is the result of TGF-β1/Smad signaling disruption. The down-regulation of TβRI and II and modulation of Smads suggests a common mechanism upstream to the pathway affected by the plants. Since oxidative stress is involved in the activation of HSCs, antioxidative properties could be the common mechanism by which the plants inhibit HSC activation and ECM deposition.
The antifibrotic properties of medicinal plants have mainly been observed in liver fibrosis models in vitro and in vivo. Clinical studies are sparse and mainly recruited chronic hepatitis B and C patients to assess the hepatoprotective effects of medicinal plants. Silymarin, glycyrrhizin, and S. miltiorrhiza have been somewhat successfully tested. Glycyrrhizin treatment induced a decrease in alanine transaminase and maintenance and improvement of necroinflammation in chronic hepatitis C nonresponders, and those patients unlikely to respond to interferon therapy when they receive at least three injections weekly over the course of 4, 22, or 52 weeks [190]-[193]. Since glycyrrhizin had no effect on hepatitis C RNA [190], investigation of the hepatoprotective mechanisms, such as inhibition of HSC activation and ECM deposition, is necessary.
Salvia injection and salvianolic acid B, have been tested in patients infected with hepatitis B. Salvianolic acid B, administrated over 6 months, reversed liver fibrosis and inflammation more effectively than IFNγ in patients with hepatitis B, as suggested by significant improvement in serum hyaluronic acid, laminin, type IV collagen, and procollagen III peptide as compared with the IFNγ group [194]. The same results, as well as decreased levels of alanine transaminase and aspartate transaminase were observed in fibrotic and cirrhotic patients infected with hepatitis B virus who were treated with Salvia injections over 45 [195] or 60 days [196]. However, another study on chronic hepatitis B patients treated with S. miltiorrhiza injection showed improvements only in symptoms, physical signs, and liver functions, not antifibrotic effects. Therefore, additional clinical studies are required to understand the effect of S. miltiorrhiza injection on liver fibrosis [197].
Clinical studies on silymarin administration for the treatment of hepatitis C were inconclusive. Silymarin has antiviral activity and has been associated with reduced progression from fibrosis to cirrhosis in advanced hepatitis C patients [198]. However, it has low oral bioavailability at 0.73% in rat plasma [199]-[201] and has not always been associated with hepatic improvement. For example, it was not effective in patients with chronic viral hepatitis C infection that who also unsuccessfully treated with interferon-based therapy [202].
Besides HSC activation and ECM deposition, other events like oxidative stress, inflammation, and immune responses are involved in the fibrogenic response [10],[11],[13],[14]. These pathways are potential targets that could help reduce hepatic fibrosis. Nevertheless, several medicinal plants have been shown to inhibit HSC activation and ECM deposition during liver fibrosis.
Abbreviations
- AGE:
-
Advanced glycation end-product
- Co-Smad:
-
Common-Smad
- CTGF:
-
Connective tissue growth factor
- ECM:
-
Extracellular matrix
- EGF:
-
Epidermal growth factor
- ERK:
-
Extracellular signal-regulated kinases
- FAK:
-
Focal adhesion kinase
- HSC:
-
Hepatic stellate cells
- IFNγ:
-
Interferon gamma
- I-Smad:
-
Inhibitory-Smad
- LDL:
-
Low-density lipoprotein
- MCP-1:
-
Monocyte chemoattractant protein-1
- MMP:
-
Matrix metalloproteinase
- NF-κB:
-
Nuclear factor kappa B
- NO:
-
Nitric oxide
- PAI-1:
-
Plasminogen activator inhibitor type 1
- PDGF:
-
Platelet-derived growth factor
- PDGF-βR:
-
Platelet-derived growth factor beta
- PPARγ:
-
Peroxisome proliferator-activated receptor gamma
- R-Smad:
-
Receptor-activated Smad
- TGF-α:
-
Transforming growth factor alpha
- TGF-β1:
-
Transforming growth factor beta 1
- TβRII:
-
Transforming growth factor beta 1 receptor II
- TβRI:
-
Transforming growth factor beta 1 receptor I
- TIMP:
-
Tissue inhibitor of metalloproteinases
- uPA:
-
urokinase-plasminogen activator
- VEGF:
-
Vascular endothelial growth factor
References
Mormone E, George J, Nieto N: Molecular pathogenesis of hepatic fibrosis and current therapeutic approaches. Chem Biol Interact. 2011, 193: 225-231.
Ellis EL, Mann DA: Clinical evidence for the regression of liver fibrosis. J Hepatol. 2012, 56: 1171-1180.
Sánchez-Valle V, Chávez-Tapia NC, Uribe M, Méndez-Sánchez N: Role of oxidative stress and molecular changes in liver fibrosis: a review. Curr Med Chem. 2012, 19: 4850-4860.
Friedman SL: Liver fibrosis – from bench to bedside. J Hepatol. 2003, 38: S38-S53.
Poynard T, Mathurin P, Lai CL, Guyader D, Poupon R, Tainturier MH, Myers RP, Muntenau M, Ratziu V, Vogel A, Capron F, Chedid A, Bedossa P, PANFIBROSIS Group: A comparison of fibrosis progression in chronic liver diseases. J Hepatol. 2003, 38: 257-265.
Lim YS, Kim WR: The global impact of hepatic fibrosis and end-stage liver disease. Clin Liver Dis. 2008, 12: 733-746.
Bataller R, Brenner DA: Liver fibrosis. J Clin Invest. 2005, 115: 209-218.
Reeves HL, Friedman SL: Activation of hepatic stellate cells—a key issue in liver fibrosis. Front Biosci. 2002, 7: d808-d826.
Henderson NC, Iredale JP: Liver fibrosis: cellular mechanisms of progression and resolution. Clin Sci (Lond). 2007, 112: 265-280.
Friedman SL: Mechanisms of hepatic fibrogenesis. Gastroenterology. 2008, 134: 1655-1669.
Rockey DC: Translating and understanding of the pathogenesis of hepatic fibrosis to novel therapies. Clin Gastroenterol Hepatol. 2013, 11: 224-231.
Friedman SL: Hepatic stellate cells: Protean, multifunctional and enigmatic cells of the liver. Physiol Rev. 2008, 88: 125-172.
Lee UE, Friedman SL: Mechanisms of hepatic fibrogenesis. Best Pract Res Clin Gastroenterol. 2011, 25: 195-206.
Jiao J, Friedman SL, Aloman C: Hepatic fibrosis. Curr Opin Gastroenterol. 2009, 25: 223-229.
Friedman SL: Hepatic fibrosis – role of hepatic stellate cell activation. Med Gen Med. 2002, 4: 27-
Bachem MG, Melchior R, Gressner AM: The role of thrombocytes in liver fibrogenesis: effects of platelet lysate and thrombocyte-derived growth factors on the mitogenic activity and glycosaminoglycan synthesis of cultures rat liver fat storing cells. J Clin Chem Clin Biochem. 1989, 27: 555-565.
Winwood PJ, Schuppan D, Iredale JP, Kawser CA, Docherty AJ, Arthur MJ: Kupffer cell-derived 95-kd type IV collagenase/gelatinase B: characterization and expression in cultured cells. Hepatology. 1995, 22: 304-315.
Yu Q, Stamenkovic I: Cell surface-localized matrix metalloproteinase-9 proteolytically activates TGF-beta and promotes tumor invasion and angiogenesis. Genes Dev. 2000, 14: 163-176.
Pinzani M, Marra F: Cytokine receptors and signaling in hepatic stellate cells. Semin Liver Dis. 2001, 21: 397-416.
Mauviel A: Transforming growth factor-β: a key mediator of fibrosis. Meth Mol Med. 2005, 117: 69-80.
George J, Roulot D, Koteliansky VE, Bissell DM: In vivo inhibition of rat stellate cell activation by soluble transforming growth factor beta type II receptor: a potential new therapy for hepatic fibrosis. Proc Natl Aca Sci USA. 1999, 96: 12719-12724.
Grotendorst GR: Connective tissue growth factor: a mediator of TGF-beta action on fibroblasts. Cytokine Growth Factor Rev. 1997, 8: 171-179.
Rockey DC: Vascular mediators in the injured liver. Hepatology. 2003, 37: 4-12.
Attia YM, Elalkamy EF, Hammam OA, Mahmoud SS, El-Khatib AS: Telmisartan, an AT1 receptor blocker and a PPAR gamma activator, alleviates liver fibrosis induced experimentally by Schistosoma mansoni infection. Parasit Vectors. 2013, 6: 199-
Baroni GS, D’Ambrosio L, Curto P, Casini A, Mancini R, Jezequel AM, Benedetti A: Interferon gamma decreases hepatic stellate cell activation and extracellular matrix deposition in rat liver fibrosis. Hepatology. 1996, 23: 1189-1199.
Calleja MA, Vieites JM, Montero-Meterdez T, Torres MI, Faus MJ, Gil A, Suárez A: The antioxidant effect of β-caryophyllene protects rat liver from carbon tetrachloride-induced fibrosis by inhibiting hepatic stellate cell activation. Br J Nutr. 2013, 109: 394-401.
Xu J, Fu Y, Chen A: Activation of peroxisome proliferator-activated receptor-gamma contributes to the inhibitory effects of curcumin on rat hepatic stellate cell growth. Am J Physiol Gastrointest Liver Physiol. 2003, 285: G20-G30.
Zheng S, Chen A: Activation of PPARgamma is required for curcumin to induce apoptosis and to inhibit the expression of extracellular matrix genes in hepatic stellate cells in vitro. Biochem J. 2004, 384: 149-157.
He YJ, Shu JC, Lü X, Fang L, Sheng Y: Prophylactic effect of curcumin on hepatic fibrosis and its relationship with activated hepatic stellate cells. Zhonghua Gan Zang Bing Za Zhi. 2006, 14: 337-340.
Cheng Y, Ping J, Xu LM: Effects of curcumin on peroxisome proliferator-activated receptor gamma expression and nuclear translocation/redistribution in culture-activated rat hepatic stellate cells. Chin Med J. 2007, 120: 794-801.
Shu JC, He YJ, Lv X, Ye GR, Wang LX: Curcumin prevents liver fibrosis by inducing apoptosis and suppressing activation of hepatic stellate cells. J Nat Med. 2009, 63: 415-420.
Wu SJ, Tam KW, Tsai YH, Chang CC, Chao JC: Curcumin and saikosaponin a inhibit chemical-induced liver inflammation and fibrosis in rats. Am J Chin Med. 2010, 38: 99-111.
Lin J, Tang Y, Kang Q, Feng Y, Chen A: Curcumin inhibits gene expression of receptor for advanced glycation end-products (RAGE) in hepatic stellate cells in vitro by elevating PPARγ activity and attenuating oxidative stress. Br J Pharmacol. 2012, 166: 2212-2227.
Yao QY, Xu BL, Wang JY, Liu HC, Zhang SC, Tu CT: Inhibition by curcumin of multiples sites of the transforming growth factor-beta1 signalling pathway ameliorates the progression of liver fibrosis induced by carbon tetrachloride in rats. BMC Complement Altern Med. 2012, 12: 156-
Park SD, Jung JH, Lee HW, Kwon YM, Chung KH, Kim MG, Kim CH: Zedoariae rhizoma and curcumin inhibits platelet-derived growth factor-induced proliferation of human hepatic myofibroblasts. Int Immunopharmacol. 2005, 5: 555-569.
Chen A, Zheng S: Curcumin inhibits connective tissue growth factor gene expression in activated hepatic stellate cells in vitro by blocking NF-κB and ERK signalling. Br J Pharmacol. 2008, 153: 557-567.
Fu Y, Zheng S, Lin J, Ryerse J, Chen A: Curcumin protects the rat liver from CCl4-caused injury and fibrogenesis by attenuating oxidative stress and suppressing inflammation. Mol Pharmacol. 2008, 73: 399-409.
Reyes-Gordillo K, Segovia J, Shibayama M, Tsutsumi V, Vergara T, Moreno MG, Muriel P: Curcumin prevents and reverses cirrhosis induced by bile duct obstruction or CCl4 in rats: role of TGF-beta modulation and oxidative stress. Fundam Clin Pharmacol. 2008, 22: 417-427.
Tang Y, Zheng S, Chen A: Curcumin eliminates leptin’s effects on hepatic stellate cell activation via interrupting leptin signalin. Endocrinology. 2009, 150: 3011-3020.
Kang Q, Chen A: Curcumin suppresses expression of low-density lipoprotein (LDL) receptor, leading to the inhibition of LDL-induced activation of hepatic stellate cells. Br J Pharmacol. 2009, 157: 1354-1367.
Kang Q, Chen A: Curcumin eliminates oxidized LDL roles in activating hepatic stellate ells by suppressing gene expression of lectin-like oxidized LDL receptor-1. Lab Invest. 2009, 89: 1275-1290.
Lin J, Zheng S, Chen A: Curcumin attenuates the effects of insulin on stimulating hepatic stellate cell activation by interrupting insulin signaling and attenuating oxidative stress. Lab Invest. 2009, 89: 1397-1409.
Morsy MA, Abdalla AM, Mahmoud AM, Abdelwahab SA, Mahmoud ME: Protective effects of curcumin, α-lipoic acid, and N-acetylcysteine against carbon tetrachloride-induced liver fibrosis in rats. J Physiol Biochem. 2012, 68: 29-35.
Tu CT, Yao QY, Xu BL, Wang JY, Zhou CH, Zhang SC: Protective effects of curcumin against hepatic fibrosis induced by carbon tetrachloride: modulation of high-mobility group box 1, Toll-like receptor 4 and 2 expression. Food Chem Toxicol. 2012, 50: 3343-3351.
Yao Q, Lin Y, Li X, Shen X, Wang J, Tu C: Curcumin ameliorates intrahepatic angiogenesis and capillarization of the sinusoids in carbon tetrachloride-induced rat liver fibrosis. Toxicol Lett. 2013, 222: 72-82.
Cheng Y, Ping J, Liu C, Tan YZ, Chen GF: Study on effects of extracts from Salvia Miltiorrhiza and Curcuma Longa in inhibiting phosphorylated extracellular signal regulated kinase expression in rat’s hepatic stellate cells. Chin J Integr Med. 2006, 12: 207-211.
Jia JD, Bauer M, Cho JJ, Ruehl M, Milani S, Boigk G, Riecken EO, Schuppan D: Antifibrotic effect of silymarin in rat secondary biliary fibrosis is mediated by downregulation of procollagen alpha1(I) and TIMP-1. J Hepatol. 2001, 35: 392-398.
Jeong DH, Lee GP, Jeong WI, Do SH, Yang HJ, Yuan DW, Park HY, Kim KJ, Jeong KS: Alterations of mast cells and TGF-beta1 on the silymarin treatment for CCl(4)-induced hepatic fibrosis. World J Gastroenterol. 2005, 11: 1141-1148.
Hsu YC, Lin YL, Chiu YT, Shiao MS, Lee CY, Huang YT: Antifibrotic effects of Salvia miltiorrhiza on dimethylnitrosamine-intoxicated rats. J Biomed Sci. 2005, 12: 185-195.
Chen IS, Chen YC, Chou CH, Chuang RF, Sheen LY, Chiu CH: Hepatoprotection of silymarin against thioacetamide-induced chronic liver fibrosis. J Sci Food Agric. 2012, 92: 1441-1447.
El-Lakkany NM, Hammam OA, El-Maadawy WH, Badawy AA, Ain-Shoka AA, Ebeid FA: Anti-inflammatory/anti-fibrotic effects of the hepatoprotective silymarin and the schistosomicide praziquantel against Schistosoma mansoni-induced liver fibrosis. Parasit Vectors. 2012, 5: 9-
Li CC, Hsiang CY, Wu SL, Ho TY: Identification of novel mechanisms of silymarin on the carbon tetrachloride-induced liver fibrosis in mice by nuclear factor-κB bioluminescent imaging-guided transcriptomic analysis. Food Chem Toxicol. 2012, 50: 1568-1575.
Kim M, Yang SG, Kim JM, Lee JW, Kim YS, Lee JI: Silymarin suppresses hepatic stellate cell activation in a dietary rat model of non-alcoholic steatohepatitis: analysis of isolated hepatic stellate cells. Int J Mol Med. 2012, 30: 473-479.
Tzeng JI, Chen MF, Chung HH, Cheng JT: Silymarin decreases connective tissue growth factor to improve liver fibrosis in rats treated with carbon tetrachloride. Phytother Res. 2013, 27: 1023-1028.
Ding J, Yu J, Wang C, Hu W, Li D, Luo Y, Luo H, Yu H: Ginkgo biloba extract alleviates liver fibrosis induced by CCl in rats. Liver Int. 2005, 25: 1224-1232.
Liu SQ, Yu JP, He L, Yu HG, Luo HS: Effects of nuclear factor kappaB and transforming growth factor beta1 in the anti-liver fibrosis process using Ginkgo biloba extract. Zhonghua Gan Zang Bing Za Zhi. 2005, 13: 903-907.
Liu SQ, Yu JP, Chen HL, Luo HS, Chen SM, Yu HG: Therapeutic effects and molecular mechanisms of Ginkgo biloba extract on liver fibrosis in rats. Am J Chin Med. 2006, 34: 99-114.
He SX, Luo JY, Wang YP, Wang YL, Fu H, Xu JL, Zhao G, Liu EQ: Effects of extract from Ginkgo biloba on carbon tetrachloride-induced liver injury in rats. World J Gastroenterol. 2006, 12: 3924-3928.
Zhang C, Zhu Y, Wan J, Xu H, Shi H, Lu X: Effects of Ginkgo biloba extract on cell proliferation, cytokines and extracellular matrix of hepatic stellate cells. Liver Int. 2006, 26: 1283-1290.
Zhang CF, Zhang CQ, Zhu YH, Wang J, Xu HW, Ren WH: Ginkgo biloba extract EGb 761 alleviates hepatic fibrosis and sinusoidal microcirculation disturbance in patients with chronic hepatitis B. Gastroen Res. 2008, 1: 20-28.
Zhang XL, Liu L, Jiang HQ: Salvia miltiorrhiza monomer IH764-3 induces hepatic stellate cell apoptosis via caspase-3 activation. World J Gastroenterol. 2002, 8: 515-519.
Chor SY, Hui AY, To KF, Chan KK, Go YY, Chan HL, Leung WK, Sung JJ: Anti-proliferative and pro-apoptotic effects of herbal medicine on hepatic stellate cell. J Ethnopharmacol. 2005, 100: 180-186.
Lin YL, Lee TF, Huang YJ, Huang YT: Antiproliferative effect of salvianolic acid A on rat hepatic stellate cells. J Pharm Pharmacol. 2006, 58: 933-939.
Fang SM, Li CS, An JY, Dun ZN, Yao DM, Liu L, Zhang XL: The role of extracellular signal-regulated kinase in induction of apoptosis with salvia miltiorrhiza monomer IH764-3 in hepatic stellate cells. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2011, 27: 402-406.
Liu L, Wei J, Huo X, Fang S, Yao D, Gao J, Jiang H, Zhang X: The Salvia miltiorrhiza monomer IH764-3 induces apoptosis of hepatic stellate cells in vivo in a bile duct ligation-induced model of liver fibrosis. Mol Med Rep. 2012, 6: 1231-1238.
Wasser S, Ho JM, Ang HK, Tan CE: Salvia miltiorrhiza reduces experimentally-induced hepatic fibrosis in rats. J Hepatol. 1998, 29: 760-771.
Shang Q, Zhang D, Guan W: The inhibitory effect in vitro of salvia miltiorrhiza and tetramethyl pyrazine on the growth of fibroblasts. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 1998, 12: 321-324.
Shang Q, Zhang D, Guan W: The influence of salvia miltiorrhiza and tetramethyl pyrazine on DNA content of cicatricial fibroblasts and its cellular cycle. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 1998, 12: 325-328.
Nan JX, Park EJ, Kang HC, Park PH, Kim JY, Sohn DH: Anti-fibrotic effects of a hot-water extract from Salvia miltiorrhiza roots on liver fibrosis induced by biliary obstruction in rats. J Pharm Pharmacol. 2001, 53: 197-204.
Wang YM, Wei FK, Liu M: Effect of Salvia miltiorrhiza on autocrining growth factor by fibroblasts cultured in vitro. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2002, 16: 408-410.
Lay IS, Chiu JH, Shiao MS, Lui WY, Wu CW: Crude extract of Salvia miltiorrhiza and salvianolic acid B enhance in vitro angiogenesis in murine SVR endothelial cell line. Planta Med. 2003, 69: 26-32.
Wang JM, Yao XX, Li XT, Yang SL, Su Z: Effects of Radix Salviae Miltiorrhizae on Ca2+ in hepatic stellate cells. Sichuan Da Xue Xue Bao Yi Xue Ban. 2005, 36: 221-224.
Yao XX, Lv T: Effects of pharmacological serum from normal and liver fibrotic rats on HSCs. World J Gastroenterol. 2005, 11: 2444-2449.
Lv T, Yao XX: Comparison of protocatechuic aldchyde in Radix Salvia miltiorrhiza and corresponding pharmacological sera from normal and fibrotic rats by high performance liquid chromatography. World J Gastroenterol. 2006, 12: 2195-2200.
Paik YH, Yoon YJ, Lee HC, Jung MK, Kang SH, Chung SI, Kim JK, Cho JY, Lee KS, Han KH: Antifibrotic effects of magnesium lithospermate B on hepatic stellate cells and thioacetamide-induced cirrhotic rats. Exp Mol Med. 2011, 43: 341-349.
Sferra R, Vetuschi A, Catitti V, Ammanniti S, Pompili S, Melideo D, Frieri G, Gaudio E, Latella G: Boswellia serrata and Salvia miltiorrhiza extracts reduce DMN-induced hepatic fibrosis in mice by TGF-beta1 downregulation. Eur Rev Med Pharmacol Sci. 2012, 16: 1484-1498.
Zhang Y, Zhang Y, Xie Y, Gao Y, Ma J, Yuan J, Li J, Wang J, Li L, Zhang J, Chu L: Multitargeted inhibition of hepatic fibrosis in chronic iron-overloaded mice by Salvia miltiorrhiza. J Ethnopharmacol. 2013, 148: 671-681.
Sun RF, Liu LX, Zhang HY: Effect of tanshinone II on hepatic fibrosis in mice. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2009, 29: 1012-1017.
Liu J: The effect of IH764-3 on proliferation and function of fibroblasts. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 1993, 15: 201-205.
Liu L, Jiang HQ, Zhang XL: The effect and mechanism of Salvia miltiorrhiza monomer IH764-3 on proliferation and collagen synthesis of hepatic stellate cells stimulated by H2O2. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2003, 19: 78-81.
Liu J, Hua G, Liu W, Cui Y, Huang H, Zhao S, Chu Y, Yang C, Chen W: The effect of IH764-3 on fibroblast proliferation and function. Chin Med Sci J. 1992, 7: 142-147.
Liu CH, Liu P, Hu YY, Xu LM, Tan YZ, Wang ZN, Liu C: Effects of salvianolic acid-A on rat hepatic stellate cell proliferation and collagen production in culture. Acta Pharmacol Sin. 2000, 21: 721-726.
Liu C, Liu P, Hu Y, Zhu D: Effects of salvianolic acid-B on TGF-beta 1 stimulated hepatic stellate cell activation and its intracellular signaling. Zhonghua Yi Xue Za Zhi. 2002, 82: 1267-1272.
Lin YL, Wu CH, Luo MH, Huang YJ, Wang CN, Shiao MS, Huang YT: In vitro protective effects of salvianolic acid B on primary hepatocytes and hepatic stellate cells. J Ethnopharmacol. 2006, 105: 215-222.
Wang R, Yu XY, Guo ZY, Wang YJ, Wu Y, Yuan YF: Inhibitory effects of salvianolic acid B on CCl(4)-induced hepatic fibrosis through regulating NF-κB/IκBα signaling. J Ethnopharmacol. 2012, 144: 592-598.
Hu Y, Wang R, Zhang X, Liu C, Liu C, Liu P, Zhu D: Effects of carbon tetrachloride-injured hepatocytes on hepatic stellate cell activation and salvianolic acid A preventive action in vitro. Zhonghua Gan Zang Bing Za Zhi. 2000, 8: 299-301.
Liu CH, Hu YY, Wang XL, Liu P, Xu LM: Effects of salvianolic acid-A on NIH/3 T3 fibroblast proliferation, collagen synthesis and gene expression. World J Gastroenterol. 2000, 6: 361-364.
Liu P, Liu CH, Wang HN, Hu YY, Liu CC: Effect of salvianolic acid B on collagen production and mitogen-activated protein kinase activity in rat hepatic stellate cells. Acta Pharmacol Sin. 2002, 23: 733-738.
Zhao JF, Liu CH, Hu YY, Xu LM, Liu P, Liu C: Effect of salvianolic acid B on Smad3 expression in hepatic stellate cells. Hepatobiliary Pancreat Dis Int. 2004, 3: 102-105.
Xue DY, Hong JH, Xu LM: Salianic-acid B inhibits MAPK signaling in activated rat hepatic stellate cells. Zhonghua Gan Zang Bing Za Zhi. 2004, 12: 471-474.
Wang XN, Hu YY, Liu CH, Liu P, Zhu DY: Effects of salvianolic acid B on expressions of TGF-beta1 and its receptors in liver of rats with dimethylnitrosamine-induced hepatic fibrosis. Zhong Xi Yi Jie He Xue Bao. 2005, 3: 286-289.
Xue DY, Hong JH, Xu LM: Effects of salvianolic acid B on signal transduction induced by transforming growth factor-beta1 and platelet-derived growth factor- BB in hepatic stellate cells of rats. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2006, 26: 439-442.
Zhang J, Zhang WW, Xu LM: Effect and mechanism of salvianolic-acid B on inhibiting endothelin-1-induced contraction of human hepatic stellate cells. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2009, 29: 60-64.
Lv Z, Song Y, Xue D, Zhang W, Cheng Y, Xu L: Effect of salvianolic-acid B on inhibiting MAPK signaling induced by transforming growth factor-β1 in activated rat hepatic stellate cells. J Ethnopharmacol. 2010, 132: 384-392.
Tsai MK, Lin YL, Huang YT: Differential inhibitory effects of salvianolic acids on activation of rat hepatic stellate cells by platelet-derived growth factor. Planta Med. 2011, 77: 1495-1503.
Song YF, Lü ZG, Xu LM: Salvianolic acid B inhibits ERK signal transduction pathway activated by transforming growth factor-β1 in rat hepatic stellate cells. Zhong Xi Yi Jie He Xue Bao. 2012, 10: 454-461.
Xu H, Zhou Y, Lu C, Ping J, Xu LM: Salvianolic acid B lowers portal pressure in cirrhotic rats and attenuates contraction of rat hepatic stellate cells by inhibiting RhoA signaling pathway. Lab Invest. 2012, 92: 1738-1748.
Li S, Wang L, Yan X, Wang Q, Tao Y, Li J, Peng Y, Liu P, Liu C: Salvianolic acid B attenuates rat hepatic fibrosis via downregulating angiotensin II signaling. Evid Based Complement Alternat Med. 2012, 2012: 160726-
Song YF, Lv ZG, Xu LM: Effects of salvianolic-acid B on the p38MAPK signaling pathway and its transcriptional factor induced by transforming growth factor b1 in activated rat hepatic stellate cells. Zhonghua Gan Zang Bing Za Zhi. 2012, 20: 902-907.
Lv Z, Xu L: Salvianolic Acid B inhibits ERK and p38 MAPK signaling in TGF-β1-stimulated human hepatic stellate lell line (LX-2) via distinct pathways. Evid Based Complement Altern Med. 2012, 2012: 960128-
Qu Y, Chen WH, Zong L, Xu MY, Lu LG: 18α-Glycyrrhizin induces apoptosis and suppresses activation of rat hepatic stellate cells. Med Sci Monit. 2012, 18: BR24-BR32.
Dong L, Sun JY, Fang GT, Jiang LD, Wang JY: Effects of glycyrrhizin on TGFbeta1 stimulated hepatic stellate cell signaling transduction. Zhonghua Gan Zang Bing Za Zhi. 2005, 13: 828-831.
Moro T, Shimoyama Y, Kushida M, Hong YY, Nakao S, Higashiyama R, Sugioka Y, Inoue H, Okazaki I, Inagaki Y: Glycyrrhizin and its metabolite inhibit Smad3-mediated type I collagen gene transcription and suppress experimental murine liver fibrosis. Life Sci. 2008, 83: 531-539.
Wang JY, Zhang QS, Guo JS, Hu MY: Effects of glycyrrhetinic acid on collagen metabolism of hepatic stellate cells at different stages of liver fibrosis in rats. World J Gastroenterol. 2001, 7: 115-119.
Li X, Peng XD, Zhang WL, Dai LL: Inhibiting effects of denshensu, baicalin, astragalus and Panax notoginseng saponins on hepatic fibrosis and their possible mechanisms. Zhonghua Gan Zang Bing Za Zhi. 2008, 16: 193-197.
Peng XD, Dai LL, Huang CQ, He CM, Chen LJ: Correlation between anti-fibrotic effect of baicalin and serum cytokines in rat hepatic fibrosis. World J Gastroenterol. 2009, 15: 4720-4725.
Qiao H, Han H, Hong D, Ren Z, Chen Y, Zhou C: Protective effects of baicalin on carbon tetrachloride induced liver injury by activating PPARγ and inhibiting TGFβ1. Pharm Biol. 2011, 49: 38-45.
Fan J, Li X, Li P, Li N, Wang T, Shen H, Siow Y, Choy P, Gong Y: Saikosaponin-d attenuates the development of liver fibrosis by preventing hepatocyte injury. Biochem Cell Biol. 2007, 85: 189-195.
Wang X, Wang Q, Burczynski FJ, Kong W, Gong Y: Saikosaponin A of Bupleurum chinense (Chaihu) elevates bone morphogenetic protein 4 (BMP-4) during hepatic stellate cell activation. Phytomedicine. 2013, 20: 1330-1335.
Suresh V, Asha VV: Preventive effect of ethanol extract of Phyllanthus rheedii Wight. on D-galactosamine induced hepatic damage in Wistar rats. J Ethnopharmacol. 2008, 116: 447-453.
Amin ZA, Alshawsh MA, Kassim M, Ali HM, Abdulla MA: Gene expression profiling reveals underlying molecular mechanism of hepatoprotective effect of Phyllanthus niruri on thioacetamide-induced hepatotoxicity in Sprague Dawley rats. BMC Complement Altern Med. 2013, 13: 160-
Zhang BJ, Xu D, Guo Y, Ping J, Chen LB, Wang H: Protection by and anti-oxidant mechanism of berberine against rat liver fibrosis induced by multiple hepatotoxic factors. Clin Exp Pharmacol Physiol. 2008, 35: 303-309.
Sun X, Zhang X, Hu H, Lu Y, Chen J, Yasuda K, Wang H: Berberine inhibits hepatic stellate cell proliferation and prevents experimental liver fibrosis. Biol Pharm Bull. 2009, 32: 1533-1537.
Domitrović R, Jakovac H, Marchesi VV, Blažeković B: Resolution of liver fibrosis by isoquinoline alkaloid berberine in CCl4-intoxicated mice is mediated by suppression of oxidative stress and upregulation of MMP-2 expression. J Med Food. 2013, 16: 518-528.
Wu YL, Wan Y, Jin XJ, OuYang BQ, Bai T, Zhao YQ, Nan JX: 25-OCH3-PPD induces the apoptosis of activated t-HSC/Cl-6 cells via c-FLIP-mediated NF-κB activation. Chem Biol Interact. 2011, 194: 106-112.
Geng J, Peng W, Huang Y, Fan H, Li S: Ginsenoside-Rg1 from Panax notoginseng prevents hepatic fibrosis induced by thioacetamide in rats. Eur J Pharmacol. 2010, 634: 162-169.
Lo YT, Tsai YH, Wu SJ, Chen JR, Chao JC: Ginsenoside Rb1 inhibits cell activation and liver fibrosis in rat hepatic stellate cells. J Med Food. 2011, 14: 1135-1143.
Peng XD, Dai LL, Huang CQ, He CM, Yang B, Chen LJ: Relationship between anti-fibrotic effect of Panax notoginseng saponins and serum cytokines in rat hepatic fibrosis. Biochem Biophys Res Commun. 2009, 388: 31-34.
Lee TY, Lee KC, Chang HH: Modulation of the cannabinoid receptors by andrographolide attenuates hepatic apoptosis following bile duct ligation in rats with fibrosis. Apoptosis. 2010, 15: 904-914.
Gressner OA, Lahme B, Rehbein K, Siluschek M, Weiskirchen R, Gressner AM: Pharmacological application of caffeine inhibits TGF-beta-stimulated connective tissue growth factor expression in hepatocytes via PPARgamma and SMAD2/3-dependent pathways. J Hepatol. 2008, 49: 758-767.
Gressner OA: About coffee, cappuccino and connective tissue growth factor-Or how to protect your liver?. Environ Toxicol Pharmacol. 2009, 28: 1-10.
Shi H, Dong L, Zhang Y, Bai Y, Zhao J, Zhang L: Protective effect of a coffee preparation (Nescafe pure) against carbon tetrachloride-induced liver fibrosis in rats. Clin Nutr. 2010, 29: 399-405.
Shin JW, Wang JH, Kang JK, Son CG: Experimental evidence for the protective effects of coffee against liver fibrosis in SD rats. J Sci Food Agric. 2010, 90: 450-455.
Klemmer I, Yagi S, Gressner OA: Oral application of 1,7-dimethylxanthine (paraxanthine) attenuates the formation of experimental cholestatic liver fibrosis. Hepatol Res. 2011, 41: 1094-1109.
Furtado KS, Prado MG, Aguiar E, Silva MA, Dias MC, Rivelli DP, Rodrigues MA, Barbisan LF: Coffee and caffeine protect against liver injury induced by thioacetamide in male Wistar rats. Basic Clin Pharmacol Toxicol. 2012, 111: 339-347.
Arauz J, Moreno MG, Cortés-Reynosa P, Salazar EP, Muriel P: Coffee attenuates fibrosis by decreasing the expression of TGF-β and CTGF in a murine model of liver damage. J Appl Toxicol. 2013, 33: 970-979.
Shim SG, Jun DW, Kim EK, Saeed WK, Lee KN, Lee HL, Lee OY, Choi HS, Yoon BC: Caffeine attenuates liver fibrosis via defective adhesion of hepatic stellate cells in cirrhotic model. J Gastroenterol Hepatol. 2013, 28: 1877-1884.
Arauz J, Zarco N, Segovia J, Shibayama M, Tsutsumi V, Muriel P: Caffeine prevents experimental liver fibrosis by blocking the expression of TGF-β. Eur J Gastroenterol Hepatol. 2013, 26: 164-173.
Gressner OA, Siluschek M, Lahme B, Gressner AM: Intraperitoneal application of caffeine prevents D-galactosamine-induced hepatic expression of connective tissue growth factor (CTGF/CCN2) in the rat. J Hepatol. 2009, 50: 1053-1055.
Gressner OA, Lahme B, Siluschek M, Gressner AM: Identification of paraxanthine as the most potent caffeine-derived inhibitor of connective tissue growth factor expression in liver parenchymal cells. Liver Int. 2009, 29: 886-897.
Rockey DC: Current and future anti-fibrotic therapies for chronic liver disease. Clin Liver Dis. 2008, 12: 939-962.
Knittel T, Mehde M, Grundmann A, Saile B, Scharf JG, Ramadori G: Expression of matrix metalloproteinases and their inhibitor during hepatic tissue repair in rat. Histochem Cell Biol. 2000, 113: 443-453.
Benyon RC, Arthur MJ: Extracellular matrix degradation and the role of hepatic stellate cells. Semin Liver Dis. 2001, 21: 373-384.
Murphy FR, Issa R, Zhou X, Ratnarajah S, Nagase H, Arthur MJ, Benyon C, Iredale JP: Inhibition of apoptosis of activated hepatic stellate cells by tissue inhibitor of metalloproteinase-1 is mediated via effects on matrix metalloproteinase inhibition: implications for reversibility of liver fibrosis. J Biol Chem. 2002, 277: 11069-11076.
Knittel T, Fellmer P, Ramadori G: Gene expression and regulation of plasminogen activator inhibitor type I in hepatic stellate cells of rat liver. Gastroenterology. 1996, 111: 745-754.
Zhang LP, Takahara T, Yata Y, Furui K, Jin B, Kawada N, Watanabe A: Increased expression of plasminogen activator and plasminogen activator inhibitor during liver fibrogenesis of rats: role of stellate cells. J Hepatol. 1999, 31: 703-711.
Fibbi G, Pucci M, Grappone C, Pellegrini G, Salzano R, Casini A, Milani S, Del Rosso M: Functions of the fibrinolytic system in human Ito cells and its control by basic fibroblast and platelet-derived growth factor. Hepatology. 1999, 29: 868-878.
Wynn TA, Barron L: Macrophages: master regulators of inflammation and fibrosis. Semin Liver Dis. 2010, 30: 245-257.
Hironaka K, Sakaida I, Matsumura Y, Kaino S, Miyamoto K, Okita K: Enhanced interstitial collagenase (Matrix metalloproteinase-13) production of Kupffer cell by gadolimium chloride prevents pig serum-induced rat liver fibrosis. Biochem Biophys Res Commun. 2000, 267: 290-295.
Fallowfield JA, Mizuno M, Kendall TJ, Constandinou CM, Benyon RC, Duffield JS, Iredale JP: Scar-associated macrophages are a major source of hepatic matrix metalloproteinase-13 and facilitate the resolution of murine hepatic fibrosis. J Immunol. 2007, 178: 5288-5295.
Friedman SL: Mac the knife? Macrophages: the double-edged sword of hepatic fibrosis. J Clin Invest. 2005, 115: 29-32.
Knittel T, Mehde M, Kobold D, Saile B, Dinter C, Ramadori G: Expression patterns of matrix metalloproteinases and their inhibitors in parenchymal and non-parenchymal cells of rat liver: regulation by TNF-α and TGF-β1. J Hepatol. 1999, 30: 48-60.
Huang WC, Sala-Newby GB, Susana A, Johnson JL, Newby AC: Classical macrophage activation up-regulates several matrix metalloproteinase’s through mitogen activated protein kinases and nuclear factor–κB. PLoS One. 2012, 7: e42507-
Fallowfield JA: Therapeutic targets in liver fibrosis. Am J Physiol Gastrointest Liver Physiol. 2011, 300: G709-G715.
Siller-López F, Sandoval A, Salgado S, Salazar A, Bueno M, Garcia J, Vera J, Gálvez J, Hernández I, Ramos M, Aguilar-Cordova E, Armendariz-Borunda J: Treatment with human metalloproteinase-8 gene delivery ameliorates experimental rat liver cirrhosis. Gastroenterology. 2004, 126: 1122-1133.
Iimuro Y, Nishio T, Morimoto T, Nitta Tm Stefanovic B, Choi SK, Brenner DA, Yamaoka Y: Delivery of matrix metalloproteinase-1 attenuates established liver fibrosis in the rat. Gastroenterology. 2003, 124: 445-458.
Roderfeld M, Weiskirchen R, Wagner S, Berres ML, Henkel C, Grötzinger J, Gressner AM, Matern S, Roeb E: Inhibition of hepatic fibrogenesis by matrix metalloproteinase-9 mutants in mice. FASEB J. 2006, 20: 444-454.
Bueno M, Salgado S, Beas-Zárate C, Armendariz-Borunda J: Urokinase-type plasminogen activator gene therapy in liver cirrhosis is mediated by collagens gene expression down-regulation and up-regulation of MMPs, HGF and VEGF. J Gene Med. 2006, 8: 1291-1299.
Lin YL, Lin CY, Chi CW, Huang YT: Study on antifibrotic effects of curcumin in rat hepatic stellate cells. Phytother Res. 2009, 23: 927-932.
Kang HC, Nan JX, Park PH, Kin JY, Lee SH, Woo SW, Zhao YZ, Park EJ, Sohn DH: Curcumin inhibits collagen synthesis and hepatic stellate cell activation in-vivo and in-vitro. J Pharm Pharmacol. 2002, 54: 119-126.
Yang W, Chen H, Jiang Y: Inhibitive effect of curcumin and amiloride on the fibrosis of rat hepatic stellate cells induced by oxidative stress. Zhong Yao Cai. 2003, 26: 795-798.
Zheng S, Chen A: Curcumin suppresses the expression of extracellular matrix genes in activated hepatic stellate cells by inhibiting gene expression of connective tissue growth factor. Am J Physiol Gastrointest Liver Physiol. 2006, 290: G883-G893.
Bruck R, Ashkenazi M, Weiss S, Goldiner I, Shapiro H, Aeed H, Genina O, Helpern Z, Pines M: Prevention of liver cirrhosis in rats by curcumin. Liver Int. 2007, 27: 373-383.
Cheng Y, Ping J, Liu C: Effect of curcumin on activity of matrix metalloproteinase 2, 9 and nuclear expression of RelA in rat hepatic stellate cells by activating peroxisome proliferator-activated receptor gamma signal. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2007, 27: 439-443.
Shu JC, Ye GR, Lü X, Fang L, Wu HE, Chen XJ: Therapeutic effects of curcumin treatment on hepatic fibrosis. Zhonghua Gan Zang Bing Za Zhi. 2007, 15: 753-757.
Vizzutti F, Provenzano A, Galastri S, Milani S, Delogu W, Novo E, Caligiuri A, Zamara E, Arena U, Laffi G, Parola M, Pinzani M, Marra F: Curcumin limits the fibrogenic evolution of experimental steatohepatitis. Lab Invest. 2010, 90: 104-115.
Pinlaor S, Prakobwong S, Hiraku Y, Pinlaor P, Laothong U, Yongvanit P: Reduction of periductal fibrosis in liver fluke-infected hamsters after long-term curcumin treatment. Eur J Pharmacol. 2010, 638: 134-141.
Hassan ZK, Al-Olayan EM: Curcumin reorganizes miRNA expression in a mouse model of liver fibrosis. Asian Pac J Canc Prev. 2012, 13: 5405-5408.
Zhang Z, Guo Y, Zhang S, Zhang Y, Wang Y, Ni W, Kong D, Chen W, Zheng S: Curcumin modulates cannabinoid receptors in liver fibrosis in vivo and inhibits extracellular matrix expression in hepatic stellate cells by suppressing cannabinoid receptor type-1 in vitro. Eur J Pharmacol. 2013, 721: 133-140.
Boigk G, Stroedter L, Herbst H, Waldschmidt J, Riecken EO, Schuppan D: Silymarin retards collagen accumulation in early and advanced biliary fibrosis secondary to complete bile duct obliteration in rats. Hepatology. 1997, 26: 643-649.
Lieber CS, Leo MA, Cao Q, Ren C, DeCarli LM: Silymarin retards the progression of alcohol-induced hepatic fibrosis in baboons. J Clin Gastroenterol. 2003, 37: 336-339.
Trappoliere M, Caligiuri A, Schmid M, Bertolani C, Failli P, Vizzutti F, Novo E, di Manzano C, Marra F, Loguercio C, Pinzani M: Silybin, a component of sylimarin, exerts anti-inflammatory and anti-fibrogenic effects on human hepatic stellate cells. J Hepatol. 2009, 50: 1102-1111.
Shaker ME, Zalata KR, Mehal WZ, Shiha GE, Ibrahim TM: Comparison of imatinib, nilotinib and silymarin in the treatment of carbon tetrachloride-induced hepatic oxidative stress, injury and fibrosis. Toxicol Appl Pharmacol. 2011, 252: 165-175.
Ezhilarasan D, Karthikeyan S, Vivekanandan P: Ameliorative effect of silibinin against N-nitrosodimethylamine-induced hepatic fibrosis in rats. Environ Toxicol Pharmacol. 2012, 34: 1004-1013.
Lin YL, Hsu YC, Chiu YT, Huang YT: Antifibrotic effects of a herbal combination regimen on hepatic fibrotic rats. Phytother Res. 2008, 22: 69-76.
Luo YJ, Yu JP, Shi ZH, Wang L: Ginkgo biloba extract reverses CCl4-induced liver fibrosis in rats. World J Gastroenterol. 2004, 10: 1037-1042.
Li W, Dai QT, Liu ZE: Preliminary study on early fibrosis of chronic hepatitis B treated with Ginkgo biloba Composita. Zhongguo Zhong Xi Yi Jie He Za Zhi. 1995, 15: 593-595.
Sener G, Kabasakal L, Yüksel M, Gedik N, Alican Y: Hepatic fibrosis in biliary-obstructed rats is prevented by Ginkgo biloba treatment. World J Gastroenterol. 2005, 11: 5444-5449.
Huang SZ, Luo YJ, Wang L, Cai KY: Effect of ginkgo biloba extract on livers in aged rats. World J Gastroenterol. 2005, 11: 132-135.
Hu YY, Liu P, Liu C, Xu LM, Liu CH, Zhu DY, Huang MF: Actions of salvianolic acid A on CCl4-poisoned liver injury and fibrosis in rats. Zhongguo Yao Li Xue Bao. 1997, 18: 478-480.
Lee TY, Wang GJ, Chiu JH, Lin HC: Long-term administration of Salvia miltiorrhiza ameliorates carbon tetrachloride-induced hepatic fibrosis in rats. J Pharm Pharmacol. 2003, 55: 1561-1568.
Oh SH, Cho KH, Yang BS, Roh YK: Natural compounds from Danshen suppress the activity of hepatic stellate cells. Arch Pharm Res. 2006, 29: 762-767.
Zhang L, Wu T, Chen JM, Yang LL, Song HY, Ji G: Danshensu inhibits acetaldehyde-induced proliferation and activation of hepatic stellate cell-T6. Zhong Xi Yi Jie He Xue Bao. 2012, 10: 1155-1161.
Tsai MK, Lin YL, Huang YT: Effects of salvianolic acids on oxidative stress and hepatic fibrosis in rats. Toxicol Appl Pharmacol. 2010, 242: 155-164.
Wang L, Tao Y, Li S, Chen G, Liu C: Effects of salvianolic acid B on lipid peroxidation and metalloproteinase-2 activity in fibrotic liver in rat. Zhongguo Zhong Yao Za Zhi. 2010, 35: 71-75.
Hou J, Tian J, Jiang W, Gao Y, Fu F: Therapeutic effects of SMND-309, a new metabolite of salvianolic acid B, on experimental liver fibrosis. Eur J Pharmacol. 2011, 650: 390-395.
Tao YY, Wang QL, Shen L, Fu WW, Liu CH: Salvianolic acid B inhibits hepatic stellate cell activation through transforming growth factor beta-1 signal transduction pathway in vivo and in vitro. Exp Biol Med (Maywood). 2013, 238: 1284-1296.
Liu L, Jiang HQ, Zhang XL, Zhao DQ: Effect of Salvia miltiorrhiza monomer IH764-3 on MMP-13 and TIMP-1 by downregulating the expression of focal adhesion kinase in hepatic stellate cell stimulated by H2O2. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2007, 23: 482-486.
Yang C: Effect of IH764-3 on prolyl hydroxylation in collagen biosynthesis. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 1993, 15: 364-368.
Guo XL, Liang B, Wang XW, Fan FG, Kin J, Lan R, Yang JH, Wang XC, Jin L, Cao Q: Glycyrrhizic acid attenuates CCl4-induced hepatocyte apoptosis in rats via a p53-mediated pathway. World J Gastroenterol. 2013, 19: 3781-3791.
Abe K, Ikeda T, Wake K, Sato T, Sato T, Inoue H: Glycyrrhizin prevents of lipopolysaccharide/D-galactosamine-induced liver injury through down-regulation of matrix metalloproteinase-9 in mice. J Pharm Pharmacol. 2008, 60: 91-97.
He Y, Hu ZF, Li P, Xiao C, Chen YW, Li KM, Guo JZ, Pan L, Xiong JP: Experimental study of saikosaponin-D (SSd) on lipid peroxidation of hepatic fibrosis on rat. Zhongguo Zhong Yao Za Zhi. 2008, 33: 915-919.
Surya Narayanan B, Latha P, Rukkumani R: Protective effects of Phyllanthus amarus on fibrotic markers during alcohol and polyunsaturated fatty acid-induced toxicity. Toxicol Mech Methods. 2011, 21: 48-52.
Ki SH, Yang JH, Ku SK, Kim SC, Kim YW, Cho IJ: Red ginseng extract protects against carbon tetrachloride-induced liver fibrosis. J Ginseng Res. 2013, 37: 45-53.
Jiang H, Xia LZ, Li Y, Li X, Wu J: Effect of Panax notoginseng saponins on expressions of MMP-13 and TIMP-1 in rats with hepatic fibrosis. Zhongguo Zhong Yao Za Zhi. 2013, 38: 1206-1210.
Vitaglione P, Morisco F, Mazzone G, Amoruso DC, Ribecco MT, Romano A, Fogliano V, Caporaso N, D’Argenio G: Coffee reduces liver damage in a rat model of steatohepatitis: the underlying mechanisms and the role of polyphenols and melanoidins. Hepatology. 2010, 52: 1652-1661.
Moreno MG, Chávez E, Aldaba-Muruato LR, Segovia J, Vergara P, Tsutsumi V, Shibayama M, Rivera-Espinoza Y, Muriel P: Coffee prevents CCl(4)-induced liver cirrhosis in the rat. Hepatol Int. 2011, 5: 857-863.
Shi H, Dong L, Bai Y, Zhao J, Zhang Y, Zhang L: Chlorogenic acid against carbon tetrachloride-induced liver fibrosis in rats. Eur J Pharmacol. 2009, 623: 119-124.
Shi H, Dong L, Jiang J, Zhao J, Zhao G, Dang X, Lu X, Jia M: Chlorogenic acid reduces liver inflammation and fibrosis through inhibition of toll-like receptor 4 signaling pathway. Toxicology. 2013, 303: 107-114.
van Rossum TG, Vulto AG, Hop WC, Brouwer JT, Niesters HG, Schalm SW: Intravenous glycyrrhizin for the treatment of chronic hepatitis C: a double-blind, randomized, placebo-controlled phaseI/II trial. J Gastroenterol Hepatol. 1999, 14: 1093-1099.
van Rossum TG, Vulto AG, Hop WC, Schalm SW: Glycyrrhizin-induced reduction of ALT in European patients with chronic hepatitis C. Am J Gastroenterol. 2001, 96: 2432-2437.
Orlent H, Hansen BE, Willems M, Brouwer JT, Huber R, Kullak-Ublick GA, Gerken G, Zeuzem S, Nevens F, Tielemans WC, Zondervan PE, Lagging M, Westin H, Schalm SW: Biochemical and histological effects of 26 weeks of glycyrrhizin treatment in chronic hepatitis C: a randomized phase II trial. J Hepatol. 2006, 45: 539-546.
Manns MP, Wedemeyer H, Singer A, Khomutjanskaja N, Dienes HP, Roskams T, Goldin R, Hehnke U, Inoue H, European SNMC, Study Group: Glycyrrhizin in patients who failed previous interferon alpha-based therapies: biochemical and histological effects after 52 weeks. J Viral Hepat. 2012, 19: 537-546.
Liu P, Hu YY, Liu C, Zhu DY, Xue HM, Xu ZQ, Xu LM, Liu CH, Gu HT, Zhang ZQ: Clinical observation of salvianolic acid B in treatment of liver fibrosis in chronic hepatitis B. World J Gastroenterol. 2002, 8: 679-685.
She SF, Huang XZ, Tong GD: Clinical study on treatment of liver fibrosis by different dosages of Salvia injection. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2004, 24: 17-20.
Ye F, Liu Y, Qiu G, Zhao Y, Liu M: Clinical study in treatment of cirrosis by different stages of salvia injection. Zhong Yao Cai. 2005, 28: 850-854.
Jin CX, Yang J, Sun HF: Comparative study of the clinical effects of salvia miltiorrhiza injection and shengmai injection on chronic hepatitis B. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2006, 26: 936-938.
Freedman ND, Curto TM, Morishima C, Seeff LB, Goodman ZD, Wright EC, Sinha R, Everhart JE, HALT-C Trial Group: Silymarin use and liver disease progression in the Hepatitis C Antiviral Long-Term Treatment against Cirrhosis. Aliment Pharmacol Ther. 2011, 33: 127-137.
Wu JW, Lin LC, Hung SC, Chi CW, Tsai TH: Analysis of silibinin in rat plasma and bile for hepatobiliary excretion nd oral bioavilbility application. J Pharm Biomed Anal. 2007, 45: 635-641.
Hawke RL, Schrieber SJ, Soule TA, Wen Z, Smith PC, Reddy KR, Wahed AS, Belle SH, Afdhal NH, Navarro VJ, Berman J, Liu QY, Doo E, Fried MW, SyNCH Trial group: Silymarin ascending multiple oral dosing phase I study in noncirrhotic patients with chronic hepatitis C. J Clin Pharmacol. 2010, 50: 434-449.
Schrieber SJ, Hawke RL, Wen Z, Smith PC, Reddy KR, Wahed AS, Belle SH, Afdhal NH, Navarro VJ, Meyers CM, Doo E, Fried MW: Differences in the disposition of silymarin between patients with nonalcoholic fatty liver disease and chronic hepatitis C. Drug Metab Dispos. 2011, 39: 2182-2190.
Fried MW, Navrro VJ, Afdhal N, Belle SH, Wahed AS, Hawke RL, Doo E, Meyers CM, Reddy KR, Silymarin in NASH and C Hepatitis (SyNCH) Study Group: Effect of silymarin (milk thistle) on liver disease in patients with chronic hepatitis C unseccessfully treated with interferin therapy: a randomized controlled trial. JAMA. 2012, 308: 274-282.
Acknowledgements
Supported by: CONACYT for the PhD student grant. This work was partially funded by endowments from Instituto Tecnológico de Estudios Superiores de Monterrey (cat-134) and the Zambrano–Hellion Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
FD and DEC conceived and designed the study. FD and DEC analyzed the data. FD, DEC, JEM, MTG, and CR wrote the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

{kind=link}
Cite this article
Duval, F., Moreno-Cuevas, J.E., González-Garza, M.T. et al. Protective mechanisms of medicinal plants targeting hepatic stellate cell activation and extracellular matrix deposition in liver fibrosis. Chin Med 9, 27 (2014). https://doi.org/10.1186/s13020-014-0027-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13020-014-0027-4