
Abstract
Background
Understanding injury patterns specific for paediatric casualties of armed conflict is essential to facilitate preparations by organizations that provide medical care in conflict areas. The aim of this retrospective cohort study is to identify injury patterns and treatment requirements that are specific for paediatric patients in conflict zones.
Methods
Characteristics of children (age < 15 years) treated in medical facilities supported by the International Committee of the Red Cross (ICRC) between 1988 and 2014 in Kabul, Kao-i-Dang, Lokichogio, Kandahar, Peshawar, Quetta and Goma were analysed; patient characteristics were compared between treatment facilities and with those of adult patients (age ≥ 15 years).
Results
Of the patients listed in the database, 15% (5843/38,088) were aged < 15 years. The median age was 10 years (IQR 6–12); 75% (4406/5843) were male. Eighty-six percent (5012/5,843) of the admitted children underwent surgery, with a median of 2 surgeries per patient (IQR 1–3). When compared with adult patients, children were more frequently seen with fragment injuries, burns and mine injuries; they had injuries to multiple body regions more often and had higher in-hospital mortality rates.
Conclusions
Children more often sustained injuries to multiple body regions and had higher in-hospital mortality than adults. These findings could have implications for how the ICRC and other organizations prepare personnel and structure logistics to meet the treatment needs of paediatric victims of armed conflicts.
Similar content being viewed by others


Introduction
The impact of war on children’s lives is extensive [1,2,3,4]. In conflict, the paediatric workload in military hospitals is 6% of all patients[5,6,7,8,9,10], and an even greater portion of paediatric patients (18%) is treated in humanitarian hospitals [11, 12]. Additionally, the percentage of paediatric patients is markedly higher among the surgical patient population in military hospitals (16%) [13, 14] as well as in humanitarian efforts (30%) [15,16,17,18,19], which again emphasizes that war-wounded children demand extensive care and resources [5, 8,9,10, 13, 20,21,22,23,24]. Additionally, younger age (≤ 8 years) has been independently associated with mortality in trauma patients admitted to combat support hospitals in Iraq and Afghanistan [9, 10, 22].
Given this context, it is of value to note that pre-deployment military medical training did not seem to fully meet the educational needs of their deployed personnel in the treatment of paediatric patients [25,26,27]. Our research group recently performed a survey among the medical personnel of the International Committee of the Red Cross (ICRC), a neutral and impartial humanitarian organization that provides assistance to victims of war. This survey revealed a need for additional training on the treatment of paediatric patients [28]. Furthermore, no referral centre for paediatric patients was available on most deployments, which demonstrates that these patients are largely dependent on ICRC’s medical facilities in conflict areas [28].
Consequently, the paediatric population in an armed conflict is at risk for many different reasons. It is therefore imperative to identify knowledge and skill gaps to improve treatment for paediatric patients. Detailed information on the injury patterns seen in these patients and their treatment needs is required. However, a recent report from Save the Children International on children in conflict zones between 1989 and 2016 revealed that there is a significant and worrisome gap in child-specific data [29].
The aim of this study is therefore to define patterns of injury and surgical treatment needs for paediatric patients in armed conflict zones. We analysed the demographic and epidemiological characteristics of paediatric patients who were admitted to and treated in eight different ICRC-supported medical facilities (see Table 1) and compared these data with those of adult patients and between treatment facilities. This information can be used for improving the preparation (i.e. medical training and logistics) of organizations providing medical care in conflict areas. The findings of this study could facilitate better preparation of deployed and local healthcare providers and result in more favourable treatment outcomes for young victims of armed conflict.
Materials and methods
This study has been approved by the ICRC, Geneva, Switzerland. A retrospective review was performed of an ICRC database, which contained data from eight field hospitals in the following locations: Kabul, Kao-I-Dang, Lokichogio, Kandahar, Peshawar 1990–1993, Peshawar 2009–2012, Quetta and Goma (Table 1). In the field, these data were registered on paper. All cases were manually digitalized in an anonymous ICRC database using Microsoft Office Excel.
The following data were analysed for all paediatric patients aged < 15 years: sex, age, length of hospital stay (days), time to admission to hospital (hours), mortality, number of surgeries and blood transfusions, mechanism of injury and anatomical site of injury. These data were compared to those of adult patients (age ≥ 15 years) treated in the same treatment facilities.
The sample size was determined by data availability, as a fixed number of cases was available in the dataset. Missing data in this database is considered missing completely and at random; it was dealt with by restricting statistical analyses to individuals with complete data on the variables required for the analysis.
Data concerning paediatric patients were compared between the different treatment facilities and with adults using chi-square tests with post hoc z tests for categorical variables and (pairwise) Mann-Whitney U tests for continuous variables. A Bonferroni correction was used for multiple testing. Descriptive statistics are expressed in frequencies with percentages or medians with interquartile range (IQR). All statistics were calculated using SPSS statistical software (IBM SPSS Statistics for Windows, Version 25.0).
Results
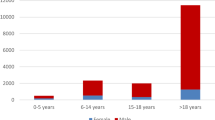
In total, data from 38,088 patients were recorded, of which 5,843 (15.3%) patients were aged < 15 years. Table 2 displays data on age, sex, length of hospital stay and mortality for paediatric patients. In Kabul, paediatric patients made up a greater part of the patient population (2185/6735; 32.4%) compared to other locations (p < 0.05); fewer paediatric patients were treated in Lokichogio (1110/13,406, 8.3%), Kao-I-Dang (97/1079; 9.0%) and Quetta (1043/7379; 14.1%; p < 0.05). Three quarters of the paediatric patients were male, and the male to female ratio was higher in Quetta (male 859/1034; 82.4%) and relatively lower in Goma (male 53/95; 55.8%) and Kao-i-Dang (male 61/97; 63%) compared to ratios from populations in other locations (p < 0.05); this ratio was also higher for adults (male 29,486/32,245; 91.4%) than for children (male 4406/5843; 75.4%; p < 0.05).
Paediatric patients were hospitalized for shorter periods of time than adult patients (median 13 days for paediatric patients vs 17 days for adults; p < 0.05). The length of hospital stays for paediatric patients was significantly longer in Lokichogio (median 33 days; IQR 17–60) compared to all other hospitals (p < 0.05).
The time to admission (Table 3) could not be compared for patients treated in Goma because this variable was divided into different categories than those recorded by the other hospitals. Of all paediatric patients, 28.0% (1611/5,748) reached the treatment facility within 6 h after injury, whereas for adults, this percentage was 12.5% (3938/31,556). More often, it took adult patients over 72 h to reach the hospital (14,560/31,556; 46.1%; p < 0.05). Analysis by hospital showed that a greater proportion of paediatric patients took more than 72 h to reach the hospital in Lokichogio (834/1110; 75.1%) and Peshawar 2009–2012 (130/453; 28.7%; p < 0.05), whereas greater percentages of paediatric patients could reach the hospital within 6 h in Kao-i-Dang (61/97, 62.9%), Kabul (1200/2185; 54.9%) and Kandahar (69/186; 37.1%; p < 0.05). In Goma, most patients (50/95; 52.6%) could reach the treatment facility within 24 h.
Data on the mechanism and anatomical site of injury are displayed in Table 4. A comparison between children and adults demonstrates that paediatric patients were more often seen with fragment injuries (2112/5843; 36.1%), mine injuries (1197/5,843; 20.5%) and burns (195/5843; 3.3%), whereas adults were more frequently injured by gunshots (16,822/32,245; 52.2%; all with p < 0.05). Among paediatric patients, more fragment injuries were seen in Kabul (1246/2,185; 57.0%) and Kao-I-Dang (64/97; 66.0%) compared to other locations (both with p < 0.05); more gunshot wounds were seen in Lokichogio (653/1110; 58.8%) and Goma (59/95; 62.1%; p < 0.05). More mine injuries were seen in Quetta (367/1034; 35.5%), Peshawar 1990–1993 (258/674; 38.3%) and Kandahar (94/186; 50.5%; p < 0.05). However, in the period of 2009–2012, mine injuries were less frequently reported in Peshawar (36/453; 7.9%; p < 0.05).
The extremities were the most commonly injured body part in paediatric patients (3891/5843; 66.6%) as well as in adult patients (23,400/32,245; 72.6%), with the lower limbs (2660/5843; 45.5%) being injured more often than the upper limbs (2005/5843; 34.3%) in paediatric patients. Children more often sustained injuries to the head and neck (1491/5843; 25.5%; p < 0.05) and abdomen (815/5843; 13.9%; p < 0.05) compared to adults (5199/32,245; 16.1% and 2837/32,245; 8.8%, respectively). More limb injuries in paediatric patients were seen in Lokichogio (793/1110; 71.4%) and Peshawar 2009–2012 (340/453; 75.1%; p < 0.05). In Lokichogio, fewer injuries to the head and neck (140/1110; 12.6%), thorax (88/1110; 7.9%) and abdomen (75/1110; 6.8%) were reported (p < 0.05).
A total of 2,234 paediatric patients (38.2%) sustained injuries to multiple body regions; multi-trauma was reported less frequently in adult patients (10,060/32,245; 31.2%; p < 0.05). Fewer paediatric multi-trauma patients were seen in Lokichogio (237/1110; 21.4%; p < 0.05) compared to those seen in other hospitals, whereas more multi-trauma patients were seen in Quetta (459/1034; 44.4%) and Peshawar 2009–2012 (238/453; 52.5%; p < 0.05).
Mortality among paediatric patients (241/5843; 4.1%) was higher compared to adults (873/32,245; 2.7%; p < 0.05). For paediatric patients, mortality was highest in Kandahar (13/186; 7.0%) followed by Kabul (119/2185; 5.4%), and the latter was significantly different from all other locations (p < 0.05). Mortality was significantly lower in Lokichogio (22/1110; 2.0%; p < 0.05).
A total of 13,547 surgeries were performed on 5012 paediatric patients (85.8%) with a median of 2 surgeries per patient (IQR 1–3); 73.0% (3660/5012) of these patients had to undergo 2 or more surgeries. In adults, a total of 75,004 surgeries were performed on 26,853 patients (median 2, IQR 1–3), of which 77.4% (20,797/26,853) had to undergo 2 or more surgeries. Paediatric patients comprised 15.7% (5012/31,865) of the surgical patients; proportionally, paediatric patients were more frequently operated on (5012/5843; 85.8%) than adult patients (26,852/32,245; 83.3%; p < 0.05). Most paediatric patients (4820/5843; 82.5%) and adult patients (28,035/32,245; 87.0%) did not receive any blood transfusions.
Discussion
This multicentre epidemiologic study provides extensive information on the epidemiology and demographics of the paediatric weapon-wounded patient population treated at eight different ICRC-supported medical treatment facilities. As opposed to many previous reports on weapon-wounded children, this study includes patients from multiple conflict zones over time.
This study shows that children make up a significant part of the patient population (15.3%) in ICRC-supported hospitals, have considerable surgery needs and often require multiple surgeries per individual. When compared with adult patients, children are more frequently seen with fragment injuries, burns and mine injuries. Sadly, our data reveal that children, more often than adults, are injured in multiple body regions and have higher in-hospital mortality rates.
The surgical workload for paediatric patients of 15.7% that was found in this study is closer to that in military hospitals (16%) [13, 14], than in other humanitarian efforts (30%) [15,16,17,18,19].This is expected since the ICRC mainly treats weapon-wounded patients. The unequal distribution of sex among children treated in hospitals in conflict areas, with the vast majority being male (overall male to female ratio of 4:1), is widely described in the literature [8, 11, 12, 16, 21, 24, 30, 31]. It has often been speculated that females are less likely to become injured in armed conflicts. However, over the years, females seem to be participating more actively in conflicts [30] and to be markedly affected by armed conflicts [11], which could be reflected in the decrease in the male/female ratio in the most recent time period of our study (Goma).
In the studied areas, paediatric patients often reached the hospital faster than adults. Generally, children are probably less likely to go outside on their own and will often have a supervising adult in close proximity who could take them to the hospital. With limited prehospital medical services and poor infrastructure in conflict areas, there might be more societal support to arrange transport to the hospital for injured children because of the emotional impact this has on witnesses.
Although paediatric patients had significantly shorter hospital stays than adult patients, the median length of hospital stay for children in this study (13 days IQR 6–31) was much longer than those reported in the literature concerning military hospitals (median ranging from 3 to 4 days) [7, 8, 10, 24]. Due to the difference in mandates between military hospitals and the humanitarian ICRC treatment facilities, children are likely to be transferred from a military hospital to a civilian medical facility after emergency care [32], whereas the ICRC treats patients until they are in no further need of in-hospital care.
The difference in the mechanism of injury seen between adults (gunshot wounds) and children (fragments, mines, burns) is also seen in casualties of the ongoing Syrian civil war [12] and could be because adults are more likely to be actively involved in the conflict. A previous study concerning ICRC data stated that during war, mines and fragmenting munitions are more likely than bullets to injure civilians [33].
Significantly more mine injuries were reported among paediatric casualties in Quetta and Peshawar (located in Pakistan close to the Afghan border) during 1990–1993 and Kandahar (Afghanistan) when compared with mine injuries from other locations. Our data from Peshawar 2009–2012 reveal a significant decline in mine injuries compared to those injuries from the early 1990s. We have reported on this previously, and other papers corroborate this finding [11, 32]. This decline in mine injuries was anticipated in Afghanistan, as large areas have been cleared of mines and unexploded ordnance since 1999; the same year, the Mine Ban Treaty came into force [34, 35]. A further decline in mine injuries should, hopefully, be expected from current conflicts in areas around participating states.
Very few paediatric patients had burns reported as the mechanism of injury, which is much less than reported in the literature [8, 10, 21, 24]. This underrepresentation is probably attributable to the high pre-hospital mortality rate of patients who sustained extensive burn injuries. Additionally, in the ICRC’s data, there could be an overlap between fragment, mine and burn injuries due to constraints in the classification of injury mechanisms. For example, a burn could be the most significant injury, but the injury could still be classified as fragments or mine if that was what caused the burn. The prevalence of burns could therefore be underestimated in this material.
Concerning the anatomical site of injury, our study results are in line with those of more recent epidemiological studies on paediatric injuries in Iraq and Afghanistan; the extremities were most frequently injured followed by the head and neck [12, 21, 24].
Regarding the different contexts studied, it is important to consider the possibility of pre-hospital patient selection, meaning that more severely injured children cannot gain access to medical care in time and die in the field. This is reflected by a lower percentage of paediatric patients with fewer critical injuries and a lower in-hospital mortality rate in Lokichogio, which was located further away from the conflict. Although in-hospital mortality rates were therefore generally low, paediatric patients showed a slightly higher mortality rate than adults, which could be explained by various reasons. Mainly, paediatric patients often reach the hospital faster than adults, which reduces the number of patients that deceases in the field. Furthermore, a higher mortality rate might indicate that more skills and expertise are required for this patient category; younger and more severely injured paediatric patients have shown to benefit from a higher level of paediatric expertise at the treatment facility [36]. However, the difference in mortality rate could just as well be caused by differences in body physiology and anatomy, mechanism of injury, and higher in-hospital prevalence of critical (head and neck) injuries in children. It has also been suggested that young children with conflict-related injuries may have an independent increased risk for death [22].
This study analysed differences in the epidemiology and demographics of paediatric patients between hospital locations and their contexts. The main findings may be mostly attributable to the differences in hospital location in relation to the conflict. However, any of the differences between hospital locations found in this study could also be attributed to differences in hospital logistics and the compliance of each individual employee with ICRC treatment protocols.
This study is not without limitations. Foremost, data acquisition can be impeded under field conditions in austere environments, and therefore, the accuracy of these data somewhat relies on the ability of ICRC medical personnel to keep a record of every patient and to thoroughly record every variable for each patient. This difficulty is reflected by the missing data for some variables and could have resulted in missing cases (patients) in our database. Additionally, the paper data were manually transferred into an electronic database, which poses the risk of coding mistakes.
Our data largely corroborate more recent data from military hospitals in conflict zones, but it would be preferable to compare our data with those of other humanitarian organizations located in conflict zones. The varying definitions of a child, ranging from < 15 years to < 19 years, also pose difficulties for comparisons with existing literature; hence, these comparisons should be interpreted with appropriate caution. An age of less than 15 years was used in this study as the definition of a child to ensure that a strictly paediatric population was studied. Additionally, this definition has been used in several previous studies [15, 23, 37, 38].
Although some of the patient data analysed in this study are somewhat dated, they provide a unique opportunity to study the evolution of paediatric injury epidemiology from conflicts over time.
The majority of our study subjects were victims of protracted conflicts in South Sudan (ICRC facility in Lokichogio) and Afghanistan (ICRC facilities in Kabul, Kandahar, Peshawar and Quetta), countries that face ongoing armed violence. During our study period, Afghanistan has been affected by rocket attacks and aerial bombings [39], strategies that are largely still used in modern conflicts [29]. Although the nature of these conflicts is subject to change, recent developments in modern warfare could increasingly affect civilians, including children. First, modern conflicts more often occur in densely populated urban areas [29]. Second, the nature of conflicts has shifted from confrontations between professional armies to one-sided violence, intrastate confrontations between the military and civilians or hostile groups of armed civilians [29]. Last, new technologies in weaponry design are increasing the distance between the user and the victim, which might cause the user to feel less responsible for his or her actions; this, together with the fact that these weapons can easily injure multiple people, could both contribute to the ongoing increase in the proportion of civilian casualties of armed conflict, as previously stated by Coupland et al. [33].
Due to the continued high prevalence of paediatric injuries in conflicts, the ICRC and other humanitarian organizations should deploy medical personnel who are skilled in treating paediatric trauma. This applies not only to surgeons but also to the whole scope of medical professions. The ideal situation would encompass deployment of highly skilled medical professionals with many years of experience in the (surgical) treatment of both paediatric and adult trauma patients. Considering the highly specialized medical professions nowadays, this is generally not feasible. Organizations could consider deployment of medical personnel primarily trained for paediatric trauma patients, but it is just as important to ensure greater participation of non-paediatrically trained personnel in basic courses or master classes focusing on paediatric casualties or to provide them with theoretical learning materials on this topic. Medical equipment on deployment should be suitable for paediatric populations, and deployed personnel should be provided the chance to become familiar with the equipment they will have at their disposal to treat paediatric patients during deployment.
Conclusions
Children made up a significant part of the patient population resulting from war and armed conflict; they had considerable surgery needs, more often sustained injuries to multiple body regions and had higher in-hospital mortality rates than adults. These findings are important when training and preparing healthcare providers of all professions and specialties for work in conflict zones so that the providers can meet the needs of paediatric victims of armed conflict. Medical training and logistics should correspond to the actual treatment needs to optimize care and improve outcomes for the many children afflicted by war and armed violence.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- GOM:
-
Goma
- ICRC :
-
International Committee of the Red Cross
- IQR:
-
Interquartile range
- KAB:
-
Kabul
- KAN:
-
Kandahar
- KAO:
-
Kao-I-Dang
- LOK:
-
Lokichogio
- LOS:
-
Length of (hospital) stay
- PES:
-
Peshawar
- QUE:
-
Quetta
References
Patton GC, Coffey C, Sawyer SM, Viner RM, Haller DM, Bose K, et al. Global patterns of mortality in young people: a systematic analysis of population health data. Lancet. 2009;374(9693):881–92.
Celikel A, Karbeyaz K, Kararslan B, Arslan MM, Zeren C. Childhood casualties during civil war: Syrian experience. J Forensic Leg Med. 2015;34:1–4.
Afghan civilian casualties: a grim reality. Lancet. 2013;382(9891):480.
Wagner Z, Heft-Neal S, Bhutta ZA, Black RE, Burke M, Bendavid E. Armed conflict and child mortality in Africa: a geospatial analysis. Lancet. 2018.
Heller D. Child patients in a field hospital during the 2003 Gulf conflict. J R Army Med Corps. 2005;151(1):41–3.
Beitler AL, Wortmann GW, Hofmann LJ, Goff JM Jr. Operation enduring freedom: the 48th Combat Support Hospital in Afghanistan. Mil Med. 2006;171(3):189–93.
Burnett MW, Spinella PC, Azarow KS, Callahan CW. Pediatric care as part of the US Army medical mission in the global war on terrorism in Afghanistan and Iraq, December 2001 to December 2004. Pediatrics. 2008;121(2):261–5.
Idenburg FJ, van Dongen TT, Tan EC, Hamming JH, Leenen LP, Hoencamp R. Pediatric surgical care in a Dutch Military Hospital in Afghanistan. World J Surg. 2015;39(10):2413–21.
Spinella PC, Borgman MA, Azarow KS. Pediatric trauma in an austere combat environment. Crit Care Med. 2008;36(7 Suppl):S293–6.
Borgman M, Matos RI, Blackbourne LH, Spinella PC. Ten years of military pediatric care in Afghanistan and Iraq. J Trauma Acute Care Surg. 2012;73(6 Suppl 5):S509–13.
Andersson P, Muhrbeck M, Veen H, Osman Z, von Schreeb J. Hospital workload for weapon-wounded females treated by the International Committee of the Red Cross: more work needed than for males. World J Surg. 2018;42(1):93–8.
Bitterman Y, Benov A, Glassberg E, Satanovsky A, Bader T, Sagi R. Role 1 Pediatric trauma care on the Israeli-Syrian border-first year of the humanitarian effort. Mil Med. 2016;181(8):849–53.
Hoencamp R, Tan EC, Idenburg F, Ramasamy A, van Egmond T, Leenen LP, et al. Challenges in the training of military surgeons: experiences from Dutch combat operations in southern Afghanistan. Eur J Trauma Emerg Surg. 2014;40(4):421–8.
Farrow GB, Rosenfeld JV, Crozier JA, Wheatley P, Warfe P. Military surgery in Rwanda. Aust N Z J Surg. 1997;67(10):696–702.
Trelles M, Stewart BT, Hemat H, Naseem M, Zaheer S, Zakir M, et al. Averted health burden over 4 years at Medecins Sans Frontieres (MSF) Trauma Centre in Kunduz, Afghanistan, prior to its closure in 2015. Surgery. 2016;160(5):1414–21.
Woll M, Brisson P. Humanitarian care by a forward surgical team in Afghanistan. Mil Med. 2013;178(4):385–8.
Haddock G, Pollok AJ. Paediatric trauma in northern Iraq: the Kurdish refugee crisis. J R Coll Surg Edinb. 1992;37(4):221–4.
Trelles M, Dominguez L, Tayler-Smith K, Kisswani K, Zerboni A, Vandenborre T, et al. Providing surgery in a war-torn context: the Medecins Sans Frontieres experience in Syria. Confl Health. 2015;9:36.
Trudeau MO, Baron E, Herard P, Labar AS, Lassalle X, Teicher CL, et al. Surgical care of pediatric patients in the humanitarian setting: The Medecins Sans Frontieres Experience, 2012-2013. JAMA surgery. 2015;150(11):1080–5.
Er E, Corbacioglu SK, Guler S, Aslan S, Seviner M, Aksel G, et al. Analyses of demographical and injury characteristics of adult and pediatric patients injured in Syrian civil war. Am J Emerg Med. 2017;35(1):82–6.
Coppola CP, Leininger BE, Rasmussen TE, Smith DL. Children treated at an expeditionary military hospital in Iraq. Archives of pediatrics & adolescent medicine. 2006;160(9):972–6.
Matos RI, Holcomb JB, Callahan C, Spinella PC. Increased mortality rates of young children with traumatic injuries at a US army combat support hospital in Baghdad, Iraq, 2004. Pediatrics. 2008;122(5):e959–66.
Edwards MJ, Lustik M, Burnett MW, Eichelberger M. Pediatric inpatient humanitarian care in combat: Iraq and Afghanistan 2002 to 2012. J Am Coll Surg. 2014;218(5):1018–23.
Creamer KM, Edwards MJ, Shields CH, Thompson MW, Yu CE, Adelman W. Pediatric wartime admissions to US military combat support hospitals in Afghanistan and Iraq: learning from the first 2,000 admissions. J Trauma. 2009;67(4):762–8.
Hoencamp R, Idenburg F, Vermetten E, Leenen L, Hamming J. Lessons learned from Dutch deployed surgeons and anesthesiologists to Afghanistan: 2006-2010. Mil Med. 2014;179(7):711–6.
Kearney SP, Bluman EM, Lonergan KT, Arrington ED, Ficke JR. Preparedness of orthopaedic surgeons for modern battlefield surgery. Mil Med. 2012;177(9):1058–64.
Finnegan A, Finnegan S, Bates D, Ritsperis D, McCourt K, Thomas M. Preparing British Military nurses to deliver nursing care on deployment. An Afghanistan study. Nurse Educ Today. 2015;35(1):104–12.
Haverkamp FJC, Veen H, Hoencamp R, Muhrbeck M, von Schreeb J, Wladis A, et al. Prepared for Mission? A survey of medical personnel training needs within the International Committee of the Red Cross. World J Surg. 2018.
Kirollos M, Anning C, Knag Fylkesnes G, Denselow J. The war on children. Save the Children International: London, United Kingdom; 2018.
Hylden C, Johnson AE, Rivera JC. Comparison of female and male casualty cohorts from conflicts in Iraq and Afghanistan. US Army Med Dep J. 2015:80–5.
Woods KL, Russell RJ, Bree S, Mahoney PF, McNicholas J. The pattern of paediatric trauma on operations. J R Army Med Corps. 2012;158(1):34–7.
McKechnie PS, Wertin T, Parker P, Eckert M. Pediatric surgery skill sets in Role 3: the Afghanistan experience. Mil Med. 2014;179(7):762–5.
Coupland RM, Samnegaard HO. Effect of type and transfer of conventional weapons on civilian injuries: retrospective analysis of prospective data from Red Cross hospitals. BMJ. 1999;319(7207):410–2.
Landmine Monitor 2000 [Available from: http://www.the-monitor.org/en-gb/reports/2000/landmine-monitor-2000/key-developments-since-1999.aspx.
Afghanistan, mine action 2011 [Available from: http://www.the-monitor.org/en-gb/reports/2011/afghanistan/mine-action.aspx.
Densmore JC, Lim HJ, Oldham KT, Guice KS. Outcomes and delivery of care in pediatric injury. J Pediatr Surg. 2006;41(1):92-8; discussion -8.
Beckett A, Pelletier P, Mamczak C, Benfield R, Elster E. Multidisciplinary trauma team care in Kandahar, Afghanistan: current injury patterns and care practices. Injury. 2012;43(12):2072–7.
Edwards MJ, Lustik M, Carlson T, Tabak B, Farmer D, Edwards K, et al. Surgical interventions for pediatric blast injury: an analysis from Afghanistan and Iraq 2002 to 2010. J Trauma Acute Care Surg. 2014;76(3):854–8.
Lansford T. Afghanistan at War: From the 18th-Century Durrani Dynasty to the 21st Century. California: ABC-CLIO; 2017. p. 4–6.
Acknowledgements
Not applicable
Funding
No funding was received for the performance and/or publication of this research.
Author information
Authors and Affiliations
Contributions
This study was conceived by FH and ET. The study design was made by FH, LG, MM, and ET. Data were collected and analysed by FH, LG, and ET. Interpretation of the data was done by FH, LG, MM, HV, AW, and ET. All authors contributed to the drafting and revising of the manuscript. All authors have approved this version of the manuscript to be submitted and published by World Journal of Emergency Surgery.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study has been approved by the International Committee of the Red Cross, Geneva, Switzerland
Consent for publication
Not applicable
Competing interests
Andreas Wladis and Harald Veen have both worked as Chief Surgeon at the International Committee of the Red Cross.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Haverkamp, F.J.C., van Gennip, L., Muhrbeck, M. et al. Global surgery for paediatric casualties in armed conflict. World J Emerg Surg 14, 55 (2019). https://doi.org/10.1186/s13017-019-0275-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13017-019-0275-9