
Abstract
Background
Implementation of long-term condition management interventions rests on the notion of whole systems re-design, where incorporating wider elements of health care systems are integral to embedding effective and integrated solutions. However, most self-management support (SMS) evaluations still focus on particular elements or outcomes of a sub-system. A randomised controlled trial of a SMS intervention (WISE—Whole System Informing Self-management Engagement) implemented in primary care showed no effect on patient-level outcomes. This paper reports on a parallel process evaluation to ascertain influences affecting WISE implementation at patient, clinical and organisational levels. Normalisation Process Theory (NPT) provided a sensitising background and analytical framework.
Methods
A multi-method approach using surveys and interviews with organisational stakeholders, practice staff and trial participants about impact of training and use of tools developed for WISE. Analysis was sensitised by NPT (coherence, cognitive participation, collective action and reflective monitoring). The aim was to identify what worked and what did not work for who and in what context.
Results
Interviews with organisation stakeholders emphasised top-down initiation of WISE by managers who supported innovation in self-management. Staff from 31 practices indicated engagement with training but patchy adoption of WISE tools; SMS was neither prioritised by practices nor fitted with a biomedically focussed ethos, so little effort was invested in WISE techniques. Interviews with 24 patients indicated no awareness of any changes following the training of practice staff; furthermore, they did not view primary care as an appropriate place for SMS.
Conclusion
The results contribute to understanding why SMS is not routinely adopted and implemented in primary care. WISE was not embedded because of the perceived lack of relevance and fit to the ethos and existing work. Enacting SMS within primary care practice was not viewed as a legitimate activity or a professional priority. There was failure to, in principle, engage with and identify patients' support needs. Policy presumptions concerning SMS appear to be misplaced. Implementation of SMS within the health service does not currently account for patient circumstances. Primary care priorities and support for SMS could be enhanced if they link to patients' broader systems of implementation networks and resources.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Implementing self-management approaches have the potential to improve health outcomes and reduce the fiscal burden on health care systems [1]. Current adoption of self-management support (SMS) has been mainly directed at patient self-skills training and behaviour change with little consideration of the concurrent activities required of multiple partners in whole health system implementation to ensure adoption and integration into long-term condition management [2]. The disconnection of patient education skills training from chronic disease management located in primary care settings is likely to have contributed to a lack of reach to those most likely to benefit [3],[4]. Whilst primary care has been identified as a key provider of self-management education and support because of its reach and increasingly central role in chronic disease management [5],[6], general practitioners (GPs) have been reluctant to refer to external self-management education programmes because of a fear of fragmenting care and ambiguity over patient benefit [7]. Targeting and personalised management along with patient-mediated strategies are advocated components of future SMS interventions [8],[9].
Long-term condition management currently operates in UK primary care through an increasingly biomedical, bureaucratic, specialised and reductionist framework [10], reinforced by the Quality and Outcomes Framework (QOF) [11] and pay-for-performance schemes [12]. A counter trend is the advocation of empowering and engaging patients in their own care, a more patient-centred, social and psychological model of care. However, an implementation gap has been identified between these national policy aspirations and current means of delivery as patients are not being directed to local resources or engaged in behaviour change [13],[14]. The components of the Whole System Informing Self-management Engagement (WISE) approach to SMS had been firmly established but not implemented in a primary care context. Thus, there is a need to understand how a systemic patient-centred approach to SMS reconfigures existing relationships, communication and practices and how (and if) the principles of a whole systems approach can translate, embed and integrate into routine practice [15],[16]. The implementation literature states the importance of being clear about specifying the implementation strategy used [17]. The whole systems education strategy is outlined in Table 1.
The WISE approach [20] is an intervention with evidence-based components, designed to provide and encourage SMS uptake and delivery across a whole health system [21]. Informed by an understanding of how health care professionals and patients respond to long-term conditions, WISE aspired to engage patients, practitioners and the service organisation using a structured approach (Table 1) [22]. For this paper, we also considered the outer systems which influence implementation [23] and have added to the original model (see Figure 1) [22]. A large-scale randomised controlled trial (RCT) designed to test effectiveness and cost-effectiveness found that WISE had no effect whatsoever on 12-month patient outcomes [22],[24],[25]. The process evaluation explains why this evidence-based approach was not implementable in routine primary care.

Model for WISE approach.
The WISE intervention focussed on training primary care teams (GPs, nurses and administrative staff) over two half-day sessions and providing tools to support self-management. The exemplar conditions for the trial were diabetes, chronic obstructive pulmonary disease (COPD) and irritable bowel syndrome (IBS). A primary care trust (PCT)a was the organisation supporting and investing in its implementation. The PCT employed two experienced lay trainers to deliver and support the training and practices. The PCT is in the North-West of England and serves a socio-economically deprived population. The training is described in detail elsewhere [25]. The tools included PRISMS [26], Guidebooks [18],[19] and an online directory (see Table 1).
Development and evaluation of the intervention followed the MRC framework for complex interventions. The pre-clinical and development phase was informed by theory and evidence set in the context of policy expectations and guidance. There was good evidence of effectiveness for the components of the intervention (patient-centred information, shared decision-making and training of health professional teams in secondary care) [26]-[39]. A formative evaluation was used to evaluate the feasibility of the intervention in a primary care setting and refine training prior to roll-out in an RCT [25]. The process evaluation was pre-specified to complement and provide additional evidence to the main trial [22],[40].
Process evaluation question
What are the barriers and facilitators which affect the implementation of WISE at patient, clinical and organisational levels?
The conceptual framework for development and evaluation was twofold. Firstly, WISE was developed from mixed methods research which investigated the circumstances and components where patient-centred self-management was likely to be most effective [26]-[39]. Secondly, Normalisation Process Theory (NPT) [41] had utility for sensitising the research to the reaction, incorporation or rejection of WISE from a service user and professional perspective.
NPT as a theory of implementation is orientated to explain how new or modified practices of thinking, enacting, and organizing work associated with WISE are operationalized in healthcare. The theory is concerned with three core problems.
-
1.
Implementation—the social organization of bringing practices into action.
-
2.
Embedding—the processes through which practices do or fail to become routinely incorporated in everyday work of individuals and groups.
-
3.
Integration—the processes by which practices are reproduced and sustained among the social matrices of an organization.
Practices become routinely embedded—or normalized as the result of people working, individually and collectively, to enact them. This is promoted or inhibited through the following generative mechanisms through which human agency is expressed:
-
'Coherence' refers to the extent that a technology or health practice must make sense to targeted stakeholders.
-
'Cognitive participation' concerns the commitment and collective engagement of stakeholders.
-
'Collective action' refers to the relationships and work required enabling a new intervention to be taken up in practice and identifying the barriers to implementation and embedding.
-
'Reflexive monitoring' holds that successful embedding of resources and technologies in everyday practice relies upon a continuous process of evaluation to feedback and refine the object of implementation.
A key objective is 'How is this new initiative translated and implemented in practice?' which refers to two key issues: the implementation of training in the WISE approach and the implementation of tools to assess patient priorities (e.g. PRISMS forms).
Where results are positive, evidence is required to identify 'active ingredients' aiding generalisability and facilitating learning and translation into everyday practice. Where results are negative or inconclusive, evidence is needed to identify sources of failure and stasis. In other words, why did promising theory not translate into practice? It is important to identify what works well for which practices, individuals and stakeholders and in what context.
Aims of the process evaluation
-
To explore organisations', professionals' and patients' attitudes and responses to the costs and benefits of implementing WISE
-
To explore patient perspectives about and engagement with existing service management arrangements and the nature of interaction with professionals
-
To explore patient attitudes to engagement with new self-management arrangements
-
To examine changes in personal management arrangements, impact on existing caring relationships and use of additional services and resources
Methods
We viewed each level of implementation as part of a multilevel case study with an overarching analysis. NPT formed the bases of the process evaluation methodology and analysis; the survey questionnaire and the interview schedules were orientated around NPT constructs to gain a view on how WISE was being operationalised and actioned across settings. Responses to the WISE approach were determined at three levels (see the Additional file 1):
-
1.
Organisational level (sub-divided into the health organisation and the general practice)
-
Acceptability to the Health Organisation. Baseline face-to-face interviews with a purposive sample representing PCT governance bodies and those key to the roll-out of WISE were digitally recorded.
-
Acceptability to practices and recruitment to the trial. Assessment methods included contemporaneous trainer and researcher notes, e-mails from practices and minutes from meetings.
-
-
2.
Practice staff level (primary care)
-
Experience of the training-post-training evaluation questionnaire collected immediately after each session.
-
Questionnaire to survey use of tools and enrolment in the WISE approach conducted 6 months post-training and posted out to practices with accompanying pre-paid return envelopes.
-
-
3.
Face-to-face in-depth interviews with practice staff in trained practices. Three to six months following training, all staff were invited to take part in semi-structured interviews, and data collection continued until a broad representation of practice types (based on practice size, population served and number of GPs) was reached. Practice staff interviewed included GPs, nurses, the practice manager and the administrative staff. The interviews were digitally recorded.
-
4.
Patient level. In-depth interviews with a purposefully selected sample of trial participants. Twenty-four patients were selected using a maximum variation sampling strategy based on the trial baseline data: condition, length of time diagnosed, number of GP contacts, self-efficacy scores, help and support from family, choices ever offered by GP (based on the question 'I feel that my doctor has provided me with choices and options'), age and gender.
Interviews lasted between 40 to 90 min.
Analysis
The interviews were transcribed and then read and coded by members of the research team (based on the questions in Table 2) who provided written comments and interpretations of exemplar quotes. In line with how others have used NPT to provide a conceptual framework [42]-[44], coding reliability was established through a series of team meetings. This emergent data was collated to create a wall-chart to map NPT constructs. The adequacy of the mapping and data interpretation were established through discussion with all co-authors and refined in a data analysis workshop with an external expert (Carl May). The chart was finessed to produce the final version of Table 2. A team-based iterative process drawing on the quantitative data allowed an understanding of the implementation at each level. Discussions within the team then contributed to the final overarching analysis.
Ethical considerations
The study was approved by the Salford & Trafford Local Research Ethics Committee, REC reference number 09/H1004/6.
Results
Table 2 summarises the findings across the three levels using NPT constructs to illuminate for whom which elements of WISE did or did not work in practice. This analysis explains why there were no effective changes in personal management arrangements, existing care "as usual" relationships or use of additional services and resources.
Health economy system level readiness for embedding SMS
Seven key individuals were interviewed at the start of the roll-out of WISE. These included three PCT senior managers (including the chief executive), the NIHR programme grant PI and project manager and the two WISE trainers.
Whose idea was this?
The PCT was selected for WISE implementation because of previous support for self-management initiatives and its research-friendly identity. At the time of the study, the PCT operated as a health economy with close geographical and local networks; managers were highly motivated and ambitious, with a strong local identity and not afraid of innovation, key characteristics in facilitating senior management's buy-in to the WISE project.
A piece of work like this is fundamentally important to us. It's pretty good commonsense really isn't it that, you can achieve the win/win of getting the best economic impact of your investments but also getting the best impact in terms of quality of services provided to patients and to citizens to get it right on the preventative aspect of the agenda rather than having to deal constantly with exacerbations and funding expensive health care interventions. (Senior manager)
There were reports of tensions arising from the way involvement in the project had been disseminated from executive level to middle manager level and about ownership and credit. PCT managers at executive level were committed,b but WISE was not established in the Commissioning Directorate (the point in the NHS system where planning, agreeing and monitoring of services occurs) making it difficult to get buy-in from the commissioning managers and for WISE to be integrated with the PCT's annual planning cycle.
In terms of ownership and it's been difficult because once you've got a business plan for the year for your own department and you've got your resources highlighted for where you're going to put your energies that year … It's then very difficult to pull that team of people off that programme work onto something that they've had no involvement or engagement with at the outset and the planning stages. (Senior manager)
The lack of an appropriate 'home' for WISE or a champion working at managerial level had consequences for its profile across the health economy. The status of WISE as a research project (a pilot rather than mainstream activity) meant that managers were uncertain as to its future which resulted in ambivalence to engage with it. The imminent changes around commissioning exacerbated these uncertainties.
WISE was eventually allocated to the long-term conditions commissioning manager. However, this manager did not seem to demonstrate 'ownership' of WISE.
At the moment, I'm just taking a high level view of it, …because it's being steered really and managed through [senior manager], rather than through commissioning. (Senior manager)
The lack of ownership by managers was a challenge for the trainers, who—whilst employed by the PCT—had no managerial support or interest shown in their work.
It has felt to me as if WISE has slipped the radar of somebody…….it's nobody's baby in the PCT. (Trainer)
Breaking the norms of training
The training model was directed at a whole practice using a learning organisation ethos. This differed from traditional professional education [45],[46]. Training was not didactic but facilitative, flexible and encouraging of reflection; for some, this made the WISE approach less likely to be built into practice.
I think the WISE training is a totally different type of training. I don't think it's like any other training you have, so most of the training we have is very factual, it's, "Don't use that for diabetes any more, that's old hat; this is what we want you to do now and these are the new targets." …whereas I suppose your WISE training is a whole different concept, really. I still think there's room for being talked at a little bit, … But I don't think you will change people in just two sessions. (GP practice 22)
Follow-up sessions were intended to ascertain whether the training translated into changed clinical behaviours but trainers had difficulty in getting access to practices.
It was always oh we haven't done anything yet. And we had numerous meetings actually cancelled, so it'd be oh sorry, the doctor's busy, can you make it next week' So there isn't really an interest. (Trainer)
Practice readiness for embedding
Not our priority
Reactions to training ranged from interest and enthusiasm to disinterest and apathy. WISE was not viewed as core or fitting with pay-for-performance targets which did not include delivering SMS. A perceived need for training in SMS was lacking, so the approach to engaging practices stressed that the PCT would meet training costs (funding for locum and out-of-hours cover) and targeting research-friendly practices early on to encourage more reluctant GPs to join the programme. It was often the practice manager who drove the decision to be involved rather than the GPs.
I would have thought it was more [practice manager], if she thinks it's beneficial to the practice she would be on board, if she feels that other surgeries are participating and it helps them then she would be on board. (GP practice 2)
Self-management was not a priority for practices, and there was a lack of conviction that SMS would be effective. Significantly, the WISE approach was not seen as providing anything novel. Staff claimed that they were already providing good care for patients with systems and strategies for long-term conditions in place as evidenced by performance in QOF, so, changing practice offered no tangible benefits to them. This response was seemingly linked to a limited view about what constitutes adequate provision of chronic disease management in primary care which appears to be rationed and focussed on biomedical markers. Additionally, patients were viewed as unlikely to take up or benefit from a self-management approach. References to the responsibility patients take for their care act as a marker about the acceptable division of labour between professionals and patients.
I try and do the self-care management where I possibly can but I only have 15 minutes and in that could have been asthma checks, it could be a BP check bloods, height, weight, BMI, depression screening, geriatric screen. (Nurse practice 2)
They do not want to take the responsibility themselves to say … right I need to address this, this is what I need to do and this is how I'm going to do it. (Nurse practice 12)
There was concern about changes to practice and management that primary care had to incorporate with fears that WISE was yet another initiative that would fizzle out. The training was considered by some to be inappropriate for support staff. Signing up to the training and the link to research meant clinicians expected that they would have to invest additional time with patients generating more work.
They very much operate like businessmen, GPs, in terms of they've got a million and one demands on their time, they've got contracts with the PCT. To hold their contract, they've got to deliver this, and this and this. So when there's something else being thrown in for them to apportion their time and energy to, they're very much going to do a cost-benefit analysis, and if there isn't something very clear, then for some of them, that will just be it. (Manager)
There was negativity towards the inclusion of IBS as some GPs do not code IBS as a diagnosis and reported little difficulty in managing this condition [47]. Additionally, IBS is not a condition within the QOF and thus may not be prioritised by primary care clinicians [48].
Acceptability and utility of training
The delivery of training achieved several aims:
-
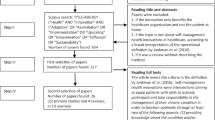
1.
Engaging a high proportion of practices with the programme, from 51 eligible practices, 44 agreed to participate although three withdrew from training.
-
2.
Delivering training to a high proportion of clinicians and other staff, 90% of eligible staff (n?=?179) attended session 1 and 82% (n?=?85) attended session 2.
-
3.
Ensuring training was relevant and acceptable, 76% rated session 1 positively and 89% session 2 (see Table 2).
Seemingly, practices were receptive to training as an opportunity for the whole practice to meet, rather than to engage with SMS.
Well I had no objection to it, it was quite nice to have a little sort of team-building day, because we tend to get…I just sit in this little room on my own …… and occasionally see them when they bring me a coffee in, if they remember I'm here. So it was actually quite nice to all sit round and swap a few ideas, when we're all on kind of an equal footing. (GP practice 22)
The trainers reported (in detailed notes and in interviews) on the positive reception to the training and alluded to the problems in putting it into practice.
They all seem to enjoy the training but it's what they do with it is, perhaps, we're not quite clear. (Trainer)
Embedding SMS in day-to-day routines of primary care: a can of worms
Self-management support was afforded minimal value or priority so little effort was invested by practices in attempting to use the techniques or tools. The guidebooks were reported as being the tools used most regularly in practice, as they fitted with the established role of nurses as educators or 'information-givers' and were minimally disruptive to their consultations.
The PRISMS tool, designed to elicit patients' needs and priorities, was not taken up for regular use—nurses were less likely than GPs to use it. Its use was considered to be too disruptive in terms of QOF tasks (which the practices prioritised) and the maintenance of relationships (which nurses took pride in).
I just think there would be some patients that I'd probably just fear them getting their hands on a PRISMS form, for the amount of work it could create. I know that people have got all these different problems that perhaps we should bring out and try and tackle, but half the time you can't actually tackle those people's problems anyway. And I know that's a fairly negative philosophy on general practice, but there is some truth in it. No, I'm quite fearful of the PRISMS form. (GP, Practice 22)
The online directory was used most by the nurses (see Figure 2). It had been identified by practices as something they needed to help direct patients to appropriate support yet it was infrequently used as it was hard to navigate and too time-consuming within a consultation.

Use of WISE tools by practice staff.
The RCT findings showed no difference between groups in accessing each type of support indicating that the training had no effect on improving support for patients [24].
Clinicians were not convinced that WISE was different enough to warrant engagement in a new way of working, and the indifference was picked up by the trainers.
I don't know that it brought that much to us really. I think it gave us something, but I don't think it's an awful lot different from what everybody else has been telling us. We need to get people to self-manage everything. (Nurse practice 12)
…I think maybe it's because as a concept it's not defined very well, it's all very vague, so people take from it what they want to take from it. Like a lot of GPs think self-management, you know, they're doing it if they just give out the leaflet, … And self-management is not a priority, and it's something that gets bandied around the PCT a lot but, you know, GPs are like their incentives and direct-payment incentives, the incentives that if we do this it will…(Trainer)
Patients' uptake and embedding
Intervention what intervention?
The interviews explored patients' views on the WISE tools and their experiences and expectations of SMS. Patients were purposefully sampled from practices where staff had reported using PRISMS, and all trial intervention group participants had been sent a PRISMS leaflet in the post. However, none recalled seeing the form prior to the interview so the instruments were introduced to patients during the interviews.
Prior experience indicated that 'forms' would be not worth the effort of completing given the burden of previously experienced forms which seemed to have little personal relevance or meaning.
I would think 'why are they doing that' because they have… I had to fill forms in before at the surgery and nothing has ever come off. Never even been mentioned or, you know? So no, I don't think it would be taken into consideration at all. (Diabetes patient)
No patients considered they would use the form, the only utility being as a memory prompt.
Uppermost in patients' minds was the receptivity of GPs to patient-initiated prompts within a consultation and the feasibility of making this work in practice. Patients were rehearsing the needs of professionals and conscious of the problems of disrupting the status quo of engrained consultation practices.
I haven't used it… if you're like me, you keep forgetting, you can go through it, tick it all off and then just hand it in to your GP when you go… rather than trying to remember what you were going to say when you get there… it's a good idea. But, whether the GPs would like it you don't know, they should do.. (IBS patient)
A good relationship, meant being able to raise concerns easily and being listened to, most likely to occur in nurse consultations. However, for most participants, their relationship ranged from ambivalent to negative, and this influenced the perceived acceptability and workability of PRISMS. Patients, it seems, work out what is on offer in the consultation and the limits of their power to change an expected and engrained response developed over years.
None of the participants reported using the online directory or being referred to it by their GP or practice nurse. Patients did not experience any changes in the nature of engagement with primary care professionals as a result of the intervention.
There was scepticism about the merit in seeking self-management advice from a health care professional as that was viewed as within the province of the patient, and there was minimal experience of the health service encouraging or fostering this [49].
I think to myself, well, if I'm the one that's looking after the condition, I'm the one that's got to put… because what can they do to help me? They can't give me tablets to stop me feeling sluggish when I've been to the toilet. (IBS patient)
At my doctor you go for your reviews, or you do your bloods, it's never how are you getting on… (Diabetes patient)
The majority of participants did not recollect being given a guidebook and reported patchy provision of information from their GP or nurse. Patients who had looked through the guidebooks indicated that they found it helpful to learn how others coped with the condition.
You read them and if there's anything that catches the eye, what I'll do, I do take notice of what people say and what advice…Yeah, they're good. They are useful. (IBS patient)
The cycle of a poverty of expectations
There were generally low expectations of support based on previous experiences of difficult and unhelpful relationships and rationed support. People reported avoiding their GPs because of low opinions of the help they would get.
...but when your doctor says something that really doesn't help, you know, and I have had her say "well you just need to control what you put in your bloody mouth" (Diabetes patient)
Review appointments and the focus on monitoring led to expectations that the practice knew about and understood the patient. Reviews were perceived as providing a safety net but there was a lack of shared decision-making.
I just thought hold on a minute there's been no consultation about whether I need to use insulin or not and that just frightened me. (Diabetes patient)
The restrictions imposed by the organisation of primary care militate against meaningful and supportive discussions and add to the lack of confidence in obtaining support:
Apparently you've got ten minutes, but it's like two weeks to get in to see her. So I had a little list, because my memory's not very good with this fibromyalgia. I wanted advice on my IBS, seeing if she could come up with something different while I was in the proceeds of suffering as well as this fibromyalgia, as well as menopause, things like that, but she said right, start with the most important, and then when my ten minutes was up she said would you like to make another appointment please. I thought right, I've got another two weeks to wait. (IBS patient)
In order to obtain appropriate support, patients often had to work hard to persuade the doctor with low expectations of assistance.
I had to go to a pharmacy that does the programme there…you can only purchase it through a pharmacy. And they weigh you every week, they advise you, but they will only let you do the programme with the agreement of the doctor. So they approached my doctor, she was reluctant to do it at first, and it took a month to get her agreement for me to do it. (Diabetes patient)
Trust the experts: where self-management support comes from
A lack of trust was evident in the types of support offered by primary care practitioners, mainly because suggestions were not sufficiently thought through or tailored to people's circumstances. The best advice came from personal contacts who had relevant experience [50],[51].
And then [nurse] was on about exercise, so she said, 'Why not go to the gym?' Anyway, she gave me a letter to go to see… [X]… I went to a class and I thought to myself, 'They're all old people here.' Some of them weren't as old as me but the exercises that they were doing I thought, 'That's not enough for me', because before that, the girl next door had said she had gone to this gym. And she said to me, 'It's ladies only…. How about coming with me?' So I started going there with her and I thoroughly enjoyed it (Diabetes patient)
Pharmacists were named as sources of support about medications, particularly in relation to multi-morbidity, but this resulted in tensions. Where many professionals were involved, patients had to work out whose advice was most relevant to their circumstances and felt uncomfortable challenging their GP.
She's [pharmacist] just got a very good attitude to the customers and the people that go in and so you can talk to her. But I will talk to her if need be or I will say to her I feel like this, and she knows all the medication I'm on because they deliver it for me, and she'll say, really you need to see your GP because you take this and you take that. Oh can't you just give me something so I don't have to go. (COPD patient)
Over-arching analysis of components
The integration and enactment of SMS differed according to context. WISE aligned with delivery of policy guidelines to improve the health of the population thus from a top-down organisation perspective; it was easy to buy into (in NPT terms cognitive participation for initiation). For practitioners, where WISE could have had the most impact, there was no alignment with practice priorities dominated by the business model of QOF and no perceived relevance or use in providing SMS because of the biomedical focus of chronic disease management (no legitimation). Practice nurses performed the prioritised biomedical monitoring tasks related to QOF and could not readily differentiate this from SMS. For patients, the context remained the same—there was no change and 'business as usual' concerning their interactions with primary care (no coherence). Patients did not view SMS as legitimate work to do with their health care professional, so would not initiate discussion or disrupt the status quo.
Expectations of what WISE could deliver were high for the PCT (reduced costs because of a healthier self-managing population (internalisation)) but health professionals and patients had low expectations. Health professionals viewed it as a lot of work with no gain for them or their patients (generally viewed as having too many complex needs to be receptive to self-management) and both patients and practitioners found PRISMS potentially disrupting to consultations and well-established practice systems (poor interactional workability). Patients did not expect to get support from GPs or nurses in managing day-to-day problems of living with a long-term condition—this came from other sources, family or friends and was tempered by prior experiences of lack of help from primary care. This accords with findings that social deprivation is linked to trust and confidence in GPs [52]. The training was seen as a different approach and difficult to operationalize by professionals and middle managers; there was nothing tangible to measure or audit and the individual practice training model viewed as costly and complex, so there were no accounts of reflexive monitoring. Trainers were seen as short-term employees and had no management backup. The merits in bringing a practice together were undoubtedly outweighed by the expense and minimal changes to professional behaviours, and the role of admin staff in the training and in SMS was seldom acknowledged or valued. The guidebooks were viewed as the one aspect of the intervention that all found useful because they fitted well with health education work, and adoption was more likely because they improved the perceived patient-centredness of information-giving (good relational integration) [53].
Overall, there was non-alignment over the aspirations most clearly articulated and adopted at the top—but which were not a priority for practitioners and patients despite national policy.
Discussion
The process evaluation findings help explain why WISE implementation did not lead to SMS becoming embedded in primary care. NPT assisted understanding of what happened across the four levels of WISE: organisational, practice, health professional and patient. Whilst some aspects of implementation worked well (participating in training was a valued opportunity to bring the practice together), the explanations for WISE not embedding at any level were the lack of commitment and views that providing and enacting SMS within primary care practice was not a legitimate activity for patients or clinicians. In addition, during implementation, the PCT was disbanded as part of wider NHS changes so there was a considerable amount of organisational change, loss of staff and shifting priorities. This represented a significant 'outer context' change [23], which could not have been anticipated and had the most impact at the organisational level (where the research team had developed good relationships) but little at the professional or patient levels.
Use of NPT in implementation studies has highlighted similar problems with engaging practitioners in order to embed practice. Lloyd et al. [44] found that work was needed to ensure shared understanding within teams concerning the purpose of shared decision-making with patients. Other process evaluations of RCTs have used NPT to help explain lack of replication of single-centre trials; however, Clarke et al. found that contextual factors including organisational history and team relationships impinged on training implementation, and NPT had limitations in this area because of undue emphasis on individual and collective agency [54]; they also found that an NPT framework does not place 'sufficient emphasis on those who receive complex interventions, especially when the 'service user' is referred to as a 'partner in care.' We would concur with this. There is a need for greater consideration in implementation theory of the importance of the patient role and the implementation work they need to do. Consideration of the Consolidated Framework for implementation [23], in conjunction with NPT, helped in interpreting the wider context—the 'outer setting' in Damschroder's model—and the mismatch between policy and practice.
Why did WISE fail in implementation? The RCT itself was well-implemented, with good reach in terms of practices and patients recruited. How WISE was interpreted and made meaningful in a particular primary care context contributed to a failure to embed the intervention in everyday practice. This came from professional and, to an extent, patient views that self-management support was something that ultimately was not the core business of primary care, and these expectations shaped the fate of the intervention post-training. The challenge is to show how an intervention of greater intensity or duration could enhance effectiveness without compromising reach. The training intervention was well-attended by staff and apparently liked. The complex intervention had good evidence to support its effectiveness. The training was developed with Gask using her evidence-based principles [31],[55]-[57]. However, some of what was done was untested in an RCT, for example, training whole practice teams. Pragmatic changes were needed to roll out the training, namely flexibility, simplification of training and use of lay trainers rather than health professionals—so WISE may have lost potency as an intervention. Unpicking the components of the intervention and considering what was ineffective in the primary care context could enhance understanding. The evidence for training teams in SMS was derived from trials in secondary care. Quality improvement interventions with financial incentives can improve collaboration and patient outcomes in primary care [58],[59]. The training aimed from the outset to instil a learning organisational ethos and to actively engage a range of staff. This was successful as notes from the trainer indicated that in the first WISE sessions, an enjoyable collegial atmosphere was evident which seemingly underpinned the positive scores in the post-training satisfaction survey (Table 3). However, the clear engagement and satisfaction with training did not translate into the practices of everyday working and probably relates to primary care culture and drivers (QOF in the UK). Communication within practices was not changed, and role demarcation and silo working patterns persisted. The lack of didactic direction or direct monitoring may have contributed to lack of uptake together with the lack of identifiable champions in PCT management or in practices to drive the embedding of a culture of SMS [60]. Emerging evidence about implementation has found that audit and feedback are effective in improving quality of care, and such support might be important post-training [61]. The shared decision-making component, PRISMS, was ineffective. Whilst there is evidence that shared decision-making and patient reported outcomes are effective, the obstacle here is the difficulty both clinicians and patients had with integrating PRISMS into consultations.
Conclusion
This study contributes to a better understanding of why SMS is not routinely adopted and implemented in primary care, by illuminating how and why providing and enacting SMS was not viewed as a legitimate activity or priority by professionals and organisations. There was a failure to, in principle, engage with and identify patients' support needs. Thus, policy presumptions concerning SMS within primary care appear to be misplaced. Implementation failure brings with it potential to negatively impact on individuals' opportunities to maximise improvements they can make to quality of life in living with a long-term condition. There are also likely significant fiscal costs to the health system if robust SMS is not adopted in primary care given the expectations of decreased utilisation with increased SMS. Implementation of SMS within the health service is bound to fail if it does not account for and connect to patient circumstances and real-life priorities. Finally, self-management requires resources which extend beyond the immediacy of the practices implicating the need for links to broader networks of care and greater understanding of network mechanisms [62]. It is possible to extend systems of resources that involve other agents, but this requires programmatic change.
Endnotes
aPCTs are now defunct, so the term is a historical reference.
bOne of the senior managers interviewed was the executive responsible for WISE and a member of the steering committee.
Authors' contributions
AK, AR, CCG, TB and JP contributed to the early conception and theoretical framework for the study design. RB, CG, VL and RM collected data for the process evaluation. AK drafted the manuscript. All authors contributed to the design of instruments and schedules used to collect data and analysis and interpretation of the data, contributed to revising the drafts and gave approval to the final version.
Additional file
References
Department of Health: Self care—a real choice: self care support—a practical option.Gateway Ref 2005, 4401.,
Schaefer J, Miller D, Goldstein M, Simmons L: Partnering in Self-Management Support: A Toolkit for Clinicians. 2009, Institute for Healthcare Improvement, Cambridge, MA
Kennedy A, Rogers A, Gately C: Assessing the introduction of the expert patients programme into the NHS: a realistic evaluation of recruitment to a national lay-led self-care initiative. Prim Health Care Res Dev. 2005, 6: 137-148. 10.1191/1463423605pc241oa.
Kennedy A, Reeves D, Bower P, Lee V, Middleton E, Richardson G, Gardner C, Gately C, Rogers A: The effectiveness and cost effectiveness of a national lay-led self care support programme for patients with long-term conditions: a pragmatic randomised controlled trial. J Epidemiol Community Health. 2007, 61: 254-261. 10.1136/jech.2006.053538.
Truglio J, Graziano M, Vedanthan R, Hahn S, Rios C, Hendel-Paterson B, Ripp J: Global health and primary care: increasing burden of chronic diseases and need for integrated training. Mt Sinai J Med. 2012, 79: 464-474. 10.1002/msj.21327.
Royal College of General Practitioners: Care planning improving the lives of people with long term conditions. In Clinical Innovation and Research Centre. 2011.
Sunaert P, Vandekerckhove M, Bastiaens H, Feyen L, Vanden Bussche P, De Maeseneer J, De Sutter A, Willems S: Why do GPs hesitate to refer diabetes patients to a self-management education program: a qualitative study. BMC Fam Pract. 2011, 12: 94. 10.1186/1471-2296-12-94.
Dennis SM, Zwar N, Griffiths R, Roland M, Hasan I, Davies GP, Harris M: Chronic disease management in primary care: from evidence to policy. Med J Aust. 2008, 188: S53-S56.
Tricco AC, Ivers NM, Grimshaw JM, Moher D, Turner L, Galipeau J, Halperin I, Vachon B, Ramsay T, Manns B, Tonelli M, Shojania K: Effectiveness of quality improvement strategies on the management of diabetes: a systematic review and meta-analysis. Lancet. 1916, 379: 2252-2261. 10.1016/S0140-6736(12)60480-2.
Chew-Graham C, Hunter C, Langer S, Stenhoff A, Drinkwater J, Guthrie E, Salmon P: How QOF is shaping primary care review consultations: a longitudinal qualitative study. BMC Fam Pract. 2013, 14: 103. 10.1186/1471-2296-14-103.
The NHS Improvement Plan: Putting People at the Heart of Public Services. 2004, The Stationery Office, London
Doran T, Kontopantelis E, Valderas JM, Campbell S, Roland M, Salisbury C, Reeves D: Effect of financial incentives on incentivised and non-incentivised clinical activities: longitudinal analysis of data from the UK Quality and Outcomes Framework. Br Med J. 2011, 342: d3590. 10.1136/bmj.d3590.
Lee V, Kennedy A, Rogers A: Implementing and managing self management skills training within primary care organisations: a national survey of the expert patients programme within its pilot phase. Implement Sci. 2006, 1: 1-6. 10.1186/1748-5908-1-6.
Rogers A: Advancing the expert patient. Prim Health Care Res Dev. 2009, 10: 167-176. 10.1017/S1463423609001194.
Macdonald W, Rogers A, Blakeman T, Bower P: Practice nurses and the facilitation of self-management in primary care. J Adv Nurs. 2008, 62: 191-199. 10.1111/j.1365-2648.2007.04585.x.
Gray C, Hunt K, Lorimer K, Anderson A, Benzeval M, Wyke S: Words matter: a qualitative investigation of which weight status terms are acceptable and motivate weight loss when used by health professionals. BMC Public Health. 2011, 11: 513. 10.1186/1471-2458-11-513.
Proctor EK, Powell BJ, McMillen J: Implementation strategies: recommendations for specifying and reporting. Implement Sci. 2013, 8: 139. 10.1186/1748-5908-8-139.
Kennedy A, Robinson A, Rogers A: Incorporating patients' views and experiences of life with IBS in the development of an evidence based self-help guidebook. Patient Educ Couns. 2003, 50: 303-310. 10.1016/S0738-3991(03)00054-5.
Kennedy AP, Rogers A: Improving patient involvement in chronic disease management: the views of patients, GPs and specialists on a guidebook for ulcerative colitis. Patient Educ Couns. 2002, 47: 257-263. 10.1016/S0738-3991(01)00228-2.
Kennedy A, Rogers A, Bower P: Support for self care for patients with chronic disease. BMJ. 2007, 335: 968-970. 10.1136/bmj.39372.540903.94.
Grant A, Treweek S, Dreischulte T, Foy R, Guthrie B: Process evaluations for cluster-randomised trials of complex interventions: a proposed framework for design and reporting. Trials. 2013, 14: 15. 10.1186/1745-6215-14-15.
Bower P, Kennedy A, Reeves D, Rogers A, Blakeman T, Chew-Graham C, Bowen R, Eden M, Hann M, Lee V, Morris R, Protheroe J, Richardson G, Sanders C, Swallow A, Thompson D: A cluster randomised controlled trial of the clinical and cost-effectiveness of a 'whole systems' model of self-management support for the management of long-term conditions in primary care: trial protocol. In Implementation Sci. 2012, 7: 7. 10.1186/1748-5908-7-7.
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC: Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science.Implement Sci 2009, 4.,
Kennedy A, Bower P, Reeves D, Blakeman T, Bowen R, Chew-Graham C, Eden M, Fullwood C, Gaffney H, Gardner C, Lee V, Morris R, Protheroe J, Richardson G, Sanders C, Swallow A, Thompson D, Rogers A: Implementation of self management support for long term conditions in routine primary care settings: cluster randomised controlled trial.Br Med J 2013, 346.,
Kennedy A, Chew-Graham C, Blakeman T, Bowen A, Gardner C, Protheroe J, Rogers A, Gask L: Delivering the WISE (Whole Systems Informing Self-Management Engagement) training package in primary care: learning from formative evaluation. Implement Sci. 2010, 5: 7. 10.1186/1748-5908-5-7.
Protheroe J, Blakeman T, Bower P, Chew-Graham C, Kennedy A: An intervention to promote patient participation and self-management in long term conditions: development and feasibility testing. BMC Health Serv Res. 2010, 10: 206. 10.1186/1472-6963-10-206.
Bodenheimer T, Wagner EH, Grumbach K: Improving primary care for patients with chronic illness. JAMA. 2002, 288: 1775-1779. 10.1001/jama.288.14.1775.
Charles C, Gafni A, Whelan T, O'Brien MA: Treatment decision aids: conceptual issues and future directions. Health Expect. 2005, 8: 114-125. 10.1111/j.1369-7625.2005.00325.x.
Haywood K, Marshall S, Fitzpatrick R: Patient participation in the consultation process: a structured review of intervention strategies. Patient Educ Couns. 2006, 63: 12-23. 10.1016/j.pec.2005.10.005.
Blickem C, Bower P, Protheroe J, Kennedy A, Vassilev I, Sanders C, Kirk S, Chew-Graham C, Rogers A: The role of information in supporting self-care in vascular conditions: a conceptual and empirical review. Health Soc Care Community. 2011, 19: 449-459. 10.1111/j.1365-2524.2010.00975.x.
Kennedy A, Gask L, Rogers A: Training professionals to engage with and promote self-management. Health Educ Res. 2005, 20: 567-578. 10.1093/her/cyh018.
Kennedy AP, Robinson A, Hann M, Thompson DG, Wilkin D: A cluster-randomised controlled trial of a patient-centred guidebook for patients with ulcerative colitis: effect on knowledge, anxiety and quality of life. Health Soc Care Community. 2003, 11: 64-72. 10.1046/j.1365-2524.2003.00399.x.
Kennedy AP, Nelson E, Reeves D, Richardson G, Robinson A, Rogers A, Sculpher M, Thompson D: A randomised controlled trial to assess effectiveness and cost of a patient orientated self-management approach to chronic inflammatory bowel disease. Gut. 2004, 53: 1639-1645. 10.1136/gut.2003.034256.
Morriss R, Dowrick C, Salmon P, Peters S, Dunn G, Rogers A, Lewis B, Charles-Jones H, Hogg J, Clifford R, Rigby C, Gask L: Cluster randomised controlled trial of training practices in reattribution for medically unexplained symptoms. Br J Psychiatry. 2007, 191: 536-542. 10.1192/bjp.bp.107.040683.
Protheroe J, Rogers A, Kennedy A, Macdonald W, Lee V: Promoting patient engagement with self-management support information: a qualitative meta-synthesis of processes influencing uptake. Implement Sci. 2008, 3: 44. 10.1186/1748-5908-3-44.
Robinson A, Lee V, Kennedy A, Middleton E, Rogers A, Thompson DG, Reeves D: A randomised controlled trial of self-help interventions in patients with a primary care diagnosis of IBS. Gut. 2006, 55: 643-648. 10.1136/gut.2004.062901.
Sikorski C, Luppa M, Konig HH, van den Bussche H, Riedel-Heller S: Does GP training in depression care affect patient outcome? - A systematic review and meta-analysis. BMC Health Serv Res. 2012, 12: 10. 10.1186/1472-6963-12-10.
Thompson C, Kinmonth AL, Stevens L, Peveler RC, Stevens A, Ostler KJ, Pickering R, Baker N, Henson A, Preece J, Cooper D, Campbell M: Effects of a clinical-practice guideline and practice-based education on detection and outcome of depression in primary care: Hampshire depression project randomised controlled trial. Lancet. 2000, 355: 185-191. 10.1016/S0140-6736(99)03171-2.
Wensing M, van der Weijden T, Grol R: Implementing guidelines and innovations in general practice: which interventions are effective?. Br J Gen Pract. 1998, 48: 991-997.
Oakley A, Strange V, Bonell C, Allen E, Stephenson J: Process evaluation in randomised controlled trials of complex interventions. Br Med J. 2006, 332: 413-416. 10.1136/bmj.332.7538.413.
May C, Finch T: Implementation, embedding, and integration: an outline of normalization process theory. Sociology. 2009, 43: 535-554. 10.1177/0038038509103208.
MacFarlane A, O'Reilly-de Brun M: Using a theory-driven conceptual framework in qualitative health research. Qual Health Res. 2012, 22: 607-618. 10.1177/1049732311431898.
Ong BN, Morden A, Brooks L, Porcheret M, Edwards JJ, Sanders T, Jinks C, Dziedzic K: Changing policy and practice: making sense of national guidelines for osteoarthritis. Soc Sci Med. 2014, 106: 101-109. 10.1016/j.socscimed.2014.01.036.
Lloyd A, Joseph-Williams N, Edwards A, Rix A, Elwyn G: Patchy 'coherence': using normalization process theory to evaluate a multi-faceted shared decision making implementation program (MAGIC). Implement Sci. 2013, 8: 102. 10.1186/1748-5908-8-102.
Freeman AC, Sweeney K: Why general practitioners do not implement evidence: qualitative study. BMJ. 2001, 323: 1100. 10.1136/bmj.323.7321.1100.
Sheaff R, Pilgrim D: Can learning organizations survive in the newer NHS?. Implement Sci. 2006, 1: 27.c 10.1186/1748-5908-1-27.
Harkness EF, Harrington V, Hinder S, O'Brien SJ, Thompson DG, Beech P, Chew-Graham C: GP perspectives of irritable bowel syndrome - an accepted illness, but management deviates from guidelines: a qualitative study.BMC Fam Pract 2013, 14.,
Lester HE, Hannon KL, Campbell SM: Identifying unintended consequences of quality indicators: a qualitative study. BMJ Qual Saf. 2011, 20: 1057-1061. 10.1136/bmjqs.2010.048371.
Rogers A, Lee V, Kennedy A: Continuity and change? Exploring reactions to a guided self-management intervention in a randomised controlled trial for IBS with reference to prior experience of managing a long term condition.Trials 2007, 8. doi:10.1186/1745-6215-8-6.,
Vassilev I, Rogers A, Blickem C, Brooks H, Kapadia D, Kennedy A, Sanders C, Kirk S, Reeves D: Social networks, the 'work' and work force of chronic illness self-management: a survey analysis of personal communities. PLoS One. 2013, 8: e59723. 10.1371/journal.pone.0059723.
Blickem C, Kennedy A, Vassilev I, Morris R, Jariwala P, Blakeman T, Rogers A: Linking people with long-term health conditions to healthy community activities: development of Patient-Led Assessment for Network Support (PLANS). Health Expect. 2013, 16 (3): e48-e59. 10.1111/hex.12088. doi:10.1111/hex.12088. Epub 2013 Jun 3
Croker JE, Swancutt DR, Roberts MJ, Abel GA, Roland M, Campbell JL: Factors affecting patients trust and confidence in GPs: evidence from the English national GP patient survey.BMJ Open 2013, 3.,
Rogers A, Kennedy A, Nelson E, Robinson A: Uncovering the limits of patient centredness: a qualitative investigation of implementing a self-management trial for chronic illness. Qual Health Res. 2005, 15: 224-239. 10.1177/1049732304272048.
Clarke D, Godfrey M, Hawkins R, Sadler E, Harding G, Forster A, McKevitt C, Dickerson J, Farrin A: Implementing a training intervention to support caregivers after stroke: a process evaluation examining the initiation and embedding of programme change. Implement Sci. 2013, 8: 96. 10.1186/1748-5908-8-96.
Gask L, Ludman E, Schaefer J: Qualitative study of an intervention for depression among patients with diabetes: how can we optimize patient–professional interaction?. Chronic Illn. 2006, 2: 231-242.
Gask L, Usherwood T, Thompson H, Williams B: Evaluation of a training package in the assessment and management of depression in primary care. Med Educ. 1998, 32: 190-198. 10.1046/j.1365-2923.1998.00195.x.
Gask L: Small group interactive techniques utilizing video feedback. Int J Psychiatr Med. 1998, 28: 97-113. 10.2190/U8MM-JX7Y-LT0T-RKPX.
Hull S, Chowdhury TA, Mathur R, Robson J: Improving outcomes for patients with type 2 diabetes using general practice networks: a quality improvement project in east London. BMJ Qual Saf. 2014, 23: 171-176. 10.1136/bmjqs-2013-002008.
Lemak CH, Cohen GR, Erb N: Engaging primary care physicians in quality improvement: lessons from a payer-provider partnership. J Healthc Manag. 2013, 58: 429-443.
Schein EH: Organization Culture and Leadership. 2010, John Wiley and Sons, San Francisco
Ivers N, Sales A, Colquhoun H, Michie S, Foy R, Francis J, Grimshaw J: No more 'business as usual' with audit and feedback interventions: towards an agenda for a reinvigorated intervention. Implement Sci. 2014, 9: 14. 10.1186/1748-5908-9-14.
Vassilev I, Rogers A, Kennedy A, Koetsenruijter J: The influence of social networks on self-management support: a metasynthesis. BMC Public Health. 2014, 14 (1): 719. 10.1186/1471-2458-14-719.
Acknowledgements
We would like to thank and acknowledge the contribution of participating practices, staff and patients and members of the Salford NIHR GI programme Grant Research Group who are Karen Armstrong, David Backhouse, Paula Beech, Peter Bower, Carolyn Chew-Graham, Andrew Clough/Karen Proctor (Chair), Anne Kennedy, Karina Lovell, Jim Nuttall, Sarah O'Brien, David Reeves, Gerry Richardson, Anne Rogers, David Thompson and Peter Whorwell. Stephanie Snow also contributed to the data collection and analysis. The study was funded by the National Institute for Health Research and The National Primary Care Research and Development Centre (funded by the Department of Health). This paper presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research funding scheme (RP-PG-0407-10136). The views expressed in this paper are those of the authors and not necessarily those of the NHS, NIHR or the Department of Health.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

{kind=link}
{kind=link}
Cite this article
Kennedy, A., Rogers, A., Chew-Graham, C. et al. Implementation of a self-management support approach (WISE) across a health system: a process evaluation explaining what did and did not work for organisations, clinicians and patients. Implementation Sci 9, 129 (2014). https://doi.org/10.1186/s13012-014-0129-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13012-014-0129-5