
Abstract
Background
There is limited research with inconsistent findings on differences between female and male offender patients with a schizophrenia spectrum disorder (SSD), who behave aggressively towards others. This study aimed to analyse inhomogeneities in the dataset and to explore, if gender can account for those.
Methods
Latent class analysis was used to analyse a mixed forensic dataset consisting of 31 female and 329 male offender patients with SSD, who were accused or convicted of a criminal offence and were admitted to forensic psychiatric inpatient treatment between 1982 and 2016 in Switzerland.
Results
Two homogenous subgroups were identified among SSD symptoms and offence characteristics in forensic SSD patients that can be attributed to gender. Despite an overall less severe criminal and medical history, the female-dominated class was more likely to receive longer prison terms, similarly high antipsychotic dosages, and was less likely to benefit from inpatient treatment. Earlier findings were confirmed and extended in terms of socio-demographic variables, diseases and criminal history, comorbidities (including substance use), the types of offences committed in the past and as index offence, accountability assumed in court, punishment adjudicated, antipsychotic treatment received, and the development of symptoms during psychiatric inpatient treatment.
Conclusions
Female offender patients with schizophrenia might need a more tailored approach in prevention, assessment and treatment to diminish tendencies of inequity shown in this study.
Similar content being viewed by others


Background
An increase in the number of females entering forensic mental health care and the penitentiary system has been observed in many countries (for reviews, see [1,2,3]. Gender differences were found in both criminal behaviour and various aspects of schizophrenia. The present study aims to explore without (even statistical) preconceptions if gender may explain relevant differences in the histories and treatment needs of patients with schizophrenia spectrum disorder (SSD) who underwent forensic psychiatric inpatient treatment.
Psychiatric research found gender-based differences regarding onset and course of SSD [4,5,6]: Women were found to become affected 4–6 years later than men, to experience more comorbidities, but less alcohol and illicit drug use, to benefit from better socio-economic circumstances (e.g. being in a relationship, employed) and to better respond to treatment, often requiring lower antipsychotic dosages.
Criminological research has also identified a gender gap [7,8,9,10,11,12,13,14,15,16]: women display less violence and aggressive behaviour overall and engage in less serious crimes. However, some studies have argued that female aggressive behaviour is not as overt as similar behaviour in males and is, therefore, less likely to lead to prosecution, which may lead to inaccurate estimates of female violence [12]. Others suggested that the gender gap in violence is largely due to males being more prone to neurocognitive deficits, difficult temperament and hyperactivity paired with poor parenting skills [11], excessive androgen production, thyroid dysfunction, Cushing’s syndrome and congenital adrenal hyperplasia [17].
Research on individuals with severe mental illness (SMI) in particular evidenced higher rates of violent behaviour (odds ratio (OR) 2.49–6.6 for men; OR 14.9–23.2 for women), any convictions (OR 2.15–3.4 for men; OR 2.85–3.7 for women) and also victimisation (87% lifetime prevalence for both men and women) in comparison to the general population [18,19,20,21,22,23]. In addition, substance use disorders were found to be a major risk factor for violence in individuals with SMI [24,25,26]. Similarly, conduct disorder prior to age 15 and antisocial personality disorder during adulthood were identified as major risk factors, even after controlling for alcohol and illicit drug use [27,28,29,30].
Offending women with SMI were found to start committing crimes at a later average age (24.9 years) than men (20.8 years), receive less severe punishment or shorter prison terms (18.4 months for women, 23.4 months for men) or were more likely to be considered to have diminished or no responsibility due to mental illness (28% women, 12% men; [31]. As for the type of crime, a study comparing male and female homicide offenders with SMI reported a four to one ratio of males to females [16]. In contradiction, other studies found that women with SMI committed more serious crimes than men, more frequently including arson (27.5% women, 12.4% men) and homicide (28.1% women, 15.1% men; [31], and were primarily admitted for such crimes [32, 33]. Female offenders with SMI were found to engage in more self-harming (women 22–33%, men 8–13%) and to have comorbid personality disorders [34]. Several studies found female offender patients with SMI to be more likely to target close family members [16, 31], which has not been found in female offenders without SMI. In contrast to non-offending women with SSD [5, 6], many female offender patients with SMI did abuse alcohol (34–48%) or illicit drugs (35–44%), suffered from socio-economic adversity [32, 33] and had a higher number of forensic and general psychiatric hospitalizations than men [34]. The few studies explicitly focusing on female offender patients with SMI [31,32,33,34] did not distinguish between different mental disorders and often presented descriptive accounts only. While SSD was a frequent diagnosis in these studies, only one study in Hunan Province, China, (to our knowledge) explored female (homicide) offenders with SSD [16]. Results may not generalise to western societies, but indicated a 4:1 male to female ratio of homicide with males being more influenced by delusions (46% vs. 35%) and females more frequently targeting close family members (62% vs. 41%).
Overall, there is a need for further research on differences between specific subgroups of patients with SSD who have committed criminal offences. For this purpose, variables similar to those in the reviewed findings, augmented by detail in their categorization, are to be analysed using latent class analysis (LCA). LCA is a statistical approach specifically designed for the identification of inherent unobservable (i.e. latent) classes within a particular dataset. Another objective is to explore the understudied topic of treatment outcome in offender patients with SSD [35] Results should allow for new insights into criminal behaviour of forensic patients with SSD and offer implications for increased efficacy in treatment and risk management.
Methodology
Source and primary processing of data
The study was approved by the Zurich Cantonal Ethics Committee (Ref.-No. KEK-ZH-NR 2014-0480). Medical files of all 370 offender patients with a schizophrenia spectrum disorder (31 female, 339 male), as defined in chapters 295.0 to 295.9 of the 9th revision of the international classification of diseases (ICD-9) [36] and chapters F20.0 to F25.9 of the 10th revision of the international statistical classification of diseases (ICD-10) [37], who were admitted to the Centre for Inpatient Forensic Therapies at the Zurich University Hospital of Psychiatry between 1982 and 2016, were analysed retrospectively. No files were excluded. As an institution run by the Zurich health authorities, the centre provides treatment for both men and women, who have committed a crime that is related to a mental disorder and for whom an expert opinion has concluded that psychiatric treatment can reduce the risk of future crimes. Files were reviewed with regard to criminal and medical histories, psychiatric inpatient and outpatient reports, police reports, court proceedings (including testimonies), reports from social workers, and biannual reports from physicians and nursing staff during forensic inpatient treatment. The composition and categorization of the final set of 63 variables for quantitative analysis was informed by prior research reviewed in the introduction and can be found in Table 2. For conversion of cumulative antipsychotic dosages into olanzapine equivalents, the classical weighted mean dose method [38] was employed. If older antipsychotics were prescribed, the minimum effective dose method [39] or international experts’ consensus based olanzapine equivalents [40] provided the necessary converting factors. Changes in psychopathology over forensic inpatient treatment were assessed using the cumulative difference between positive, negative and general psychopathology between admission and discharge.
A close adoption of the Positive and Negative Symptom Scale (PANSS) was used to categorise and quantify psychopathological symptoms (30 subcategories; symptom being fully present, somewhat present, or absent) during content analysis [41].
Retrospective file analysis by means of directed qualitative content analysis [42] used a standardised questionnaire and rating protocol [43, 44] adopted from a set of criteria first established by Seifert [45]. A trained independent physician systematically reviewed all case files and a second similarly trained independent rater encoded a random subsample of 10% of cases assuring inter-rater reliability, Cohen’s Kappa [46] being 0.78.
Data analysis
Background on latent class analysis (LCA)
Supervised statistical techniques have to be distinguished from unsupervised techniques.
Supervised methods, such as linear/logistic regressions, trees, supported vector machines, naïve Bayes and other, define an outcome a priori (e.g. male/female). They also define possible predictors (e.g. violent behaviour yes/no) for that outcome and explore their significance. This means, it is crucial to define a hypothesis beforehand, which is mostly derived from existing literature or past observations (e.g. men show more violent behaviour than women). The supervised mathematical model is calculated to asses if the predictor variable can significantly distinguish between outcomes and if this corresponds to the hypothesis (e.g. aggressive behaviour does significantly distinguish between men/women and men show significantly more of it).
By contrast, unsupervised methods, such as principle component analysis, cluster analysis and LCA (LCA, even though more progressive, has many similarities to cluster analysis in its way of identifying classes instead of clusters) do not require the definition of a hypothesis in advance (e.g. there are differences due to gender). This means there are no statistical prejudices before data analysis (LCA rather explores how many homogenous subgroups the dataset is composed of). All possible variables (e.g. aggressive behaviour, age of illness onset) are entered into the mathematical modelling process. Then homogenous groups/clusters/classes are extracted so that the homogeneity within a class is maximised and inter-class differences are also maximised. The result can be only one group, meaning the variables are not helpful in distinguishing classes. The result can also be two classes or more, meaning the variables are indeed helpful in defining different classes. For each class, the LCA model calculates class conditional item response probabilities—describing the probability of how often a given variable category is represented within a class. After this step, one can further explore, which external variable might best explain why the groups identified in LCA differ from each other. E.g. based on hypotheses, we can select a specific covariate (e.g. gender) and verify if the same classes are identified. If the same set of classes can be explained by the covariate (similar to a regression analysis for this particular number of classes), this is providing evidence that this variable (e.g. gender) is indeed distinguishing groups.
In contrast to supervised methods, unsupervised methods such as LCA have hardly any assumptions a priori and are, therefore, mainly used for explorative research. Thus, they impose less prejudice on data analysis.
Specific technical procedures used
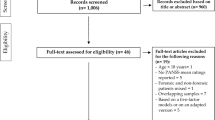
The specifics of data analysis are summarised in Fig. 1.

Flow chart of methodology. Note. SSD = schizophrenia spectrum disorder; LCA = latent class analysis
R Studio version 1.1.383 was used in conjunction with the poLCA package for latent class analysis (LCA). LCA is a type of finite mixture model designed for the analysis of multivariate categorical (instead of just dichotomous or continuous) data grouping all observations into unobserved (= latent) homogenous nominal classes by probability, while minimising confounding between observations.
To find the most parsimonious (i.e. balancing the goodness of fit with the number of model parameters involved) model representing the entire dataset of 63 items and 370 observations, solutions with one, two, and three classes were evaluated. [Solutions with more than three classes were not evaluated because results on the three class solution indicated, that a smaller number of classes (i.e. two classes) would be more parsimonious (see Table 1).] Based on presentations in extant literature employing LCAs [47, 48], the following criteria were estimated to evaluate model fit: maximum log-likelihood, log-likelihood Chi-square (G2) statistics, Bayesian Information Criterion (BIC), Akaike Information Criterion (AIC) and entropy. Each of these criteria has different strengths and weaknesses in assessing validity and reliability of the final model. While BIC and AIC are parsimony measures aiming to avoid overfitting, maximum log-likelihood and G2 are measures of goodness of model fit only. Entropy is a measure of classification uncertainty, with values of > 0.8 being suggested for a good separation between classes [49]. AIC and BIC have both been used as criteria to select the optimal number of (latent) classes in the past [50]. BIC measures the trade-off between model fit and complexity of the model and penalises additional model parameters stronger than AIC, which is why it can be considered to be more conservative by preventing that a better model fit is achieved by simply increasing model complexity. Since AIC may overestimate the correct number of components in a finite mixture model [51], BIC is more suitable in selecting the best fitting model [50]. The sample-size-corrected BIC (scBIC) is a value computed for completeness. For better comparison with previous literature, different model evaluation criteria are reported even though BIC is given highest priority.
For a given number of classes, the aim of the statistical process was to find the best fitting model by maximising the log-likelihood function via an expectation maximisation (EM) algorithm. The process was repeated 500 times for each number of classes evaluated with different starting values to avoid local extrema.
To investigate the hypothesis that the identified classes are a function of gender, a latent class regression model was fitted to the dataset in addition to the basic latent class model described above. The regression model was implemented by including a covariate (i.e. gender) in the LCA analysis, which accounts for a potential predictor variable of class membership. In contrast to the basic latent class model, where each patient has the same prior probability of class membership, in the latent class regression model, the prior probability of belonging to a particular class is allowed to vary based on the covariate [52]. The last step, exploring a latent class regression model based on the covariate gender, was used to confirm that the two-class solution is best explained by gender. It is inherent to this methodology, that the number of male and female subjects responsible for variable observations do not need to be balanced.
Results
Based on the criteria discussed above, the two-class-model (with and without covariate) was identified to represent the most parsimonious model fit as measured by the lowest BIC value among the tested models (Fig. 2, Table 1). The two-class-model with gender as a covariate had the same parsimonious model fit (BIC value), thus indicating no relevant difference between both two-class models. This means, the model without covariate evidenced that two separate classes are identifiable. The model with covariate confirmed that gender is an adequate predictor of class membership. Figure 2 visualises the probability of male and female offender patients in the two identified groups. It shows that gender can account for some differences between the two identified classes. LCA identified the two groups based on all specified variables. Subsequent results and discussion are based on the two-class model with gender as a covariate.

Differentiability of two distinct offender subgroups. Note. X-axis: subgroups suggested by LCA with covariate (female/ male gender); Y-axis: probability of subgroup membership based on manifestations of all variables explored on a scale from 0 to 1. Dashed line represents class 1, continuous line class 2
LCA provided the item response probabilities of their categories for a given variable and class. All results are presented in Table 2. Differences in probability of a given category between the two classes of above 10% are considered clinically most relevant, as previously done in similar research [53], and have been set in bold type in Table 2.
Present findings indicated that compared to the male-dominated class, offender patients in the female-dominated class were less likely to be single and have experienced homelessness, but more likely to have a higher level of formal education. The female-dominated class was more likely to have fewer criminal registry entries, fewer criminal convictions, and started to commit crimes at an older age. For previous offences, the female-dominated class was less likely to commit property crimes, criminal damage, traffic offences, or offences against the narcotics act. For index offences, it was somewhat more likely to attempt or commit homicide, but less likely to commit non-violent property crimes, or offences against the narcotics act. Victims of the female-dominated class were more likely to have had a close relationship to the offender patients. The female-dominated class was more likely to be themselves victims of sexual traumatisation inflicted by a related person, but not of any other type of crime. This class was similarly likely to be judged responsible for their offence, but more likely to receive a longer sentence for their index offence than the male-dominated class.
Results on medical histories showed the female-dominated class to be diagnosed with SSD and be admitted to their first psychiatric inpatient treatment at an older age. This class was more likely to have fewer psychiatric inpatient treatments, less likely to misuse or abuse alcohol and much less likely to use illegal substances. Male- and female-dominated classes showed no relevant difference in terms of self-injurious behaviour, attempted suicide, suicidal ideation during treatment, or the diagnosis of a personality disorder. The female-dominated class was less likely to undergo long-term forensic psychiatric treatment, but equally likely to receive high doses of antipsychotics. Women were less likely to benefit from forensic inpatient treatment regarding remission of psychopathological symptoms of SSD.
Discussion
Results confirmed a tendency towards inequality between female and male offender patients suffering from SSD and provided new details using more narrowly defined variables instead of broad categories used in existing literature. Prior research provided inconsistent results on whether women were held insufficiently [31] or excessively [33] accountable for their offending and the amount of punishment (prison term) received. Present results indicated the female-dominated class was similarly likely to be judged accountable for their offence as the male-dominated class, but more likely to receive a longer prison sentence than men. The latter may be influenced by the higher probability of the female-dominated class to attempt or commit homicide. The female-dominated class also tended to more frequently target individuals to whom they had a close relationship, including their own children (5% difference in probability). This may be considered to be particularly atrocious in the legal culture the present study was set in and may have been penalised with longer prison sentences [54]. As in prior reports [31, 34], the female-dominated class seemed less likely to commit sexual offences. A higher prevalence of arson [31, 34] could not be confirmed in the female-dominated class, which may be caused by the low prevalence of female arsonists in the present sample. Similar to one study on offender patients with SMI in the Netherlands [31], but in contrast to a study set in China [16] and research on non-mentally ill offenders in the US and UK [7, 14], present results indicated a higher probability for the female-dominated class to engage in homicide or attempted homicide. Besides cultural aspects, present findings may have been skewed by not including offender patients with SSD waiting in prisons to be transferred into forensic psychiatric treatment [55, 56] and who may be more likely to have committed less serious crimes.
Previous findings reported non-offending female patients with SSD to better maintain intimate relationships [5, 6]. Yet, in our sample, the female-dominated class also seemed less likely to be single than males, but they more frequently lived in separation from their spouse or had been divorced, as has been described for offenders in general regardless of a mental disorder [57]. Maintaining relationships might be a skill needing more therapeutic attention in offending women versus non-offending women with SSD. Similar to results in reviews on gender differences among non-offending patients with SSD [5, 6, 58], female offender patients in the present study were also likely to be older at first diagnosis of SSD and first inpatient treatment, have experienced fewer psychiatric inpatient treatments, have fewer comorbidities, have been married, have a higher level of formal education and have not been homeless. Previous findings suggested that female offenders with SMI are more likely to abuse alcohol and illegal substances [32], have more prior inpatient treatments and have a higher probability of being diagnosed with a personality disorder and self-harm [34]. This could not be confirmed here and may reflect particularities in the psychiatric understanding of the role of personality traits either as chronic symptoms of SSD or as discrete comorbidity [34]. Discrepant results may also reflect the inclusion of a wide spectrum of psychiatric diagnoses in the samples explored in past research [32].
Females in our sample were less likely than men to experience remission in psychopathology over inpatient treatment. Similar gender differences have been reported for non-offending patients with SSD [5, 6]. While treatment objectives in offender patients include the prevention of further violence in addition to a remission of psychopathology [59], the latter may be an important mediator in this respect [60]. Clinicians should consider prescribing lower antipsychotic dosages, as was recommended for non-violent women with SSD due to differences in absorption and metabolism between the sexes, resulting in women being overdosed at standard doses and consequently experiencing more side effects [5, 6]. In addition, adjunctive treatment with oestrogen may yield ameliorated treatment outcomes due to its neuroprotective effects [61, 62].
Many female offenders experienced psychological, physical or sexual violence, often in connection with relationships, especially with men (relatives and partners). This is also the case with the female-dominated class in the current study (see Table 2). Recent research confirmed violent victimisation to be a better predictor of violent behaviour than current psychopathology [63]. The current and extant studies evidence that patients with SSD tend to act against those with whom they have a close relationship—oftentimes their mothers (in male offender patients) or their children (in female offender patients) [31], which may be due to unwanted childbirth [5, 33], or serious post-partum depression and psychosis [64].
Violence against family or close acquaintances in the past will pose particular challenges to inpatient treatment of offender women with SSD in comparison to non-offending women with SSD because it complicates treatment programs aiming at social reintegration [65]. For instance, family therapy sessions may be difficult or impossible after serious violence of a patient against a family member and/ or abuse through a family member—both of which occurred more frequently in the female-dominated group in the present study (see Table 2). Further, a history of violence in close relationships may render both offender female patients with SSD and the psychiatric team treating them more reluctant to form therapeutic alliances out of fear of recurrence of such violent and hurtful phenomena. Gender-specific training of staff, raising awareness for such challenges, can help to master them and significantly improve the recovery process of patients [66]. In addition, women may benefit from more trauma-specific interventions—especially since histories of abuse impeding treatment success are frequently overlooked [32, 33]. Women were found to favour being in a single-gender environment since they may feel safer and more comfortable talking to other women about their experiences [67], which should encourage forensic mental health institutions to build separate women’s wards. Since women may process violent victimisation differently than men and to overcome risk-relevant behaviour patterns, treatment in a specially protected and protecting environment is necessary. Current forensic psychiatry (in which patients of the present study were treated) may fail to recognise and respond to specific treatment needs of female patients with SSD, which might provide additional explanation as to why the female-dominated group experienced less of a remission of positive and negative psychopathology in comparison to the male-dominated group. More gender-sensitive treatment [61, 62], which requires a better understanding regarding the different needs of male and female offender patients, should be provided.
Thus, the findings of this study may be of use to researchers and institutions interested in developing a more gender-sensitive approach to female forensic patients with SSD. Future research should further explore specific treatment needs in the management of patients with SSD and evaluate the benefits of specialised treatment facilities providing highly specific treatment, often referred to as personalised medicine, which may account for other differences between offending patient subgroups beyond gender [53].
Limitations
Limitations have already been addressed in the interpretation of results and in the “Methods”. They involve the known weaknesses of retrospective file analysis, including human error in the documentation of events, recording of events over a prolonged period of time with changing cultural aspects and treatment options, the selection and categorization of screening parameters for coding and coding itself. Further limitations involve selection effects (one forensic psychiatric institution in Switzerland) and the limited number of patients explored. In addition, the assessment of antipsychotic dosing might be biased by differences in age, weight and PANSS values among the two identified classes. Furthermore, the dataset had relatively unequal sample sizes with respect to gender (339 male vs 31 female). While similar sample size is not a prerequisite for LCA, at relatively small overall sample sizes (< 500), the associated danger is a worse detectability of the class with low prevalence [68]. The fact that the two-class solution was identified as the best fitting model, and that there was no other underlying latent parameter that could explain the difference between the two classes, however, strongly suggests that the model correctly identified gender. It might yet explain why the model did not achieve a perfect separation between male and female. Future studies balancing out these factors are needed.
Conclusion
Capitalising on LCA without any a priori assumptions, this study provides evidence that the investigated dataset on SSD symptoms and offence characteristics of forensic patients with SSD consists of two homogenous groups and shows that these subgroups can in part be attributed to gender. Results confirmed recently summarised differences between male and female patients with SSD [5, 6] for the largely unexplored subgroup of female-dominated offender patients and addressed inconsistencies raised in a scarce body of research on this subgroup [16, 31,32,33,34]. It calls upon clinicians to help reduce any disadvantage for female offender patients with SSDs by acknowledging that women have different treatment needs from men in a number of aspects and by adopting new treatment approaches to address specific treatment needs.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Nicholls TL, Cruise KR, Greig D, Hinz H. Female offenders. In: Zapf BLCPA, eds. APA handbook of forensic psychology: Criminal investigation, adjudication, and sentencing outcomes. 2. Washington, DC: American Psychological Association; 2015. pp. 79–123; doi: https://doi.org/10.1037/14462-004.
Odgers CL, Moretti MM, Reppucci ND. Examining the science and practice of violence risk assessment with female adolescents. Law Hum Behav. 2005;29(1):7. https://doi.org/10.1007/s10979-005-1397-z.
World female imprisonment list: women and girls in penal institutions, including pre-trial detainees/remand prisoners. 2015 (cited 2020.12.22). www.prisonstudies.org/sites/default/files/resources/downloads/world_female_imprisonment_list_third_edition_0.pdf.
Louzã MR, Elkis H. Schizophrenia in Women. Women's Mental Health: Springer; 2020. pp. 49–58; https://doi.org/10.1007/978-3-030-29081-8_5.
Seeman MV. Women and psychosis. Women’s Health. 2012;8(2):215–24. https://doi.org/10.2217/WHE.11.97.
Seeman MV. Schizophrenia in women as compared to men. Women & psychosis: multidisciplinary perspectives. 2019:187.
Cooper A, Smith EL. Homicide trends in the United States, 1980–2008: BiblioGov; 2012.
Durrant R. Evolutionary approaches to understanding crime: explaining the gender gap in offending. Psychology, Crime Law. 2019;25(6):589–608. https://doi.org/10.1080/1068316X.2018.1558224.
Gartner R. Sex, gender, and crime. In: Tonry M, editor. The Oxford handbook of crime and criminal justice. Oxford: Oxford University Press; 2011. p. 349–84.
Krakowski M, Czobor P. Gender differences in violent behaviors: relationship to clinical symptoms and psychosocial factors. Am J Psychiatry. 2004;161(3):459–65. https://doi.org/10.1176/appi.ajp.161.3.459.
Moffitt T, Caspi A, Rutter M, Silva P. Sex differences in antisocial behaviour: Conduct disorder, delinquency, and violence in the Dunedin Longitudinal Study. New York, NY, US: Cambridge University Press; 2001.
Odgers CL, Moffitt TE, Broadbent JM, Dickson N, Hancox RJ, Harrington H, et al. Female and male antisocial trajectories: from childhood origins to adult outcomes. Dev Psychopathol. 2008;20(2):673–716. https://doi.org/10.1017/S0954579408000333.
Rossegger A, Wetli N, Urbaniok F, Elbert T, Cortoni F, Endrass J. Women convicted for violent offenses: adverse childhood experiences, low level of education and poor mental health. BMC Psychiatry. 2009;9(1):81.
Shaw J, Hunt IM, Flynn S, Meehan J, Robinson J, Bickley H, et al. Rates of mental disorder in people convicted of homicide: national clinical survey. Br J Psychiatry. 2006;188(2):143–7. https://doi.org/10.1192/bjp.188.2.143.
Steffensmeier D, Allan E. Gender and crime: toward a gendered theory of female offending. Ann Rev Sociol. 1996;22(1):459–87. https://doi.org/10.1146/annurev.soc.22.1.459.
Wang J, Zhang S-M, Zhong S-L, Mellsop G, Guo H-J, Li Q-G, et al. Gender differences among homicide offenders with schizophrenia in Hunan Province, China. Psychiatry Res. 2019;271:124–30. https://doi.org/10.1016/j.psychres.2018.11.039.
Fishbein DH. The psychobiology of female aggression. Criminal Justice Behav. 1992;19(2):99–126.
Fazel S, Gulati G, Linsell L, Geddes JR, Grann M. Schizophrenia and violence: systematic review and meta-analysis. PLoS Med. 2009;6(8):e1000120. https://doi.org/10.1371/journal.pmed.1000120.
Fazel S, Wolf A, Palm C, Lichtenstein P. Violent crime, suicide, and premature mortality in patients with schizophrenia and related disorders: a 38-year total population study in Sweden. Lancet Psychiatry. 2014;1(1):44–54. https://doi.org/10.1016/S2215-0366(14)70223-8.
Hodgins S, Alderton J, Cree A, Aboud A, Mak T. Aggressive behaviour, victimisation and crime among severely mentally ill patients requiring hospitalisation. Br J Psychiatry. 2007;191(4):343–50. https://doi.org/10.1192/bjp.bp.106.06.029587.
Hodgins S, Klein S. New clinically relevant findings about violence by people with schizophrenia. Canadian J Psychiatry. 2017;62(2):86–93. https://doi.org/10.1177/0706743716648300.
Stevens H, Laursen TM, Mortensen PB, Agerbo E, Dean K. Post-illness-onset risk of offending across the full spectrum of psychiatric disorders. Psychol Med. 2015;45(11):2447–57. https://doi.org/10.1017/S0033291715000458.
Wallace C, Mullen PE, Burgess P. Criminal offending in schizophrenia over a 25-year period marked by deinstitutionalization and increasing prevalence of comorbid substance use disorders. Am J Psychiatry. 2004;161(4):716–27. https://doi.org/10.1176/appi.ajp.161.4.716.
Drake RE, Mueser KT. Managing comorbid schizophrenia and substance abuse. Curr Psychiatry Rep. 2001;3(5):418–22. https://doi.org/10.1007/s11920-996-0037-8.
Drake RE, Mueser KT. Co-occurring alcohol use disorder and schizophrenia. Alcohol Res Health. 2002;26(2):99.
Drake RE, Mueser KT, Clark RE, Wallach MA. The course, treatment, and outcome of substance disorder in persons with severe mental illness. Am J Orthopsychiatry. 1996;66(1):42–51. https://doi.org/10.1037/h0080153.
Hodgins S, Cree A, Alderton J, Mak T. From conduct disorder to severe mental illness: associations with aggressive behaviour, crime and victimization. Psychol Med. 2008;38(7):975–87. https://doi.org/10.1017/S0033291707002164.
Mueser KT. Screening and assessment of substance use disorder in psychosis. A Clinical introduction to psychosis: Elsevier; 2020. p. 295–318; doi: https://doi.org/10.1016/B978-0-12-815012-2.00013-4.
Mueser KT, Drake RE, Ackerson TH, Alterman AI, Miles KM, Noordsy DL. Antisocial personality disorder, conduct disorder, and substance abuse in schizophrenia. J Abnorm Psychol. 1997;106(3):473. https://doi.org/10.1037/0021-843X.106.3.473.
Mueser KT, Rosenberg SD, Drake RE, Miles KM, Wolford G, Vidaver R, et al. Conduct disorder, antisocial personality disorder and substance use disorders in schizophrenia and major affective disorders. J Stud Alcohol. 1999;60(2):278–84. https://doi.org/10.15288/jsa.1999.60.278.
de Vogel V, de Spa E. Gender differences in violent offending: results from a multicentre comparison study in Dutch forensic psychiatry. Psychol Crime Law. 2018. https://doi.org/10.1080/1068316X.2018.1556267.
Krammer S, Eisenbarth H, Fallegger C, Liebrenz M, Klecha D. Sociodemographic information, aversive and traumatic events, offence-related characteristics, and mental health of delinquent women in forensic-psychiatric care in Switzerland. Int J Offender Ther Comp Criminol. 2018;62(12):3815–33. https://doi.org/10.1177/0306624X17749638.
Nagdee M, Artz L, Corral-Bulnes C, Heath A, Subramaney U, de Clercq HG, et al. The psycho-social and clinical profile of women referred for psycho-legal evaluation to forensic mental health units in South Africa. South Afr J Psychiatry. 2019. https://doi.org/10.4102/sajpsychiatry.v25i0.1230.
Coid J, Kahtan N, Gault S, Jarman B. Women admitted to secure forensic psychiatry services: I. Comparison of women and men. J Forensic Psychiatry. 2000;11(2):275–95. https://doi.org/10.1080/09585180050142525.
Morgan RD, Flora DB, Kroner DG, Mills JF, Varghese F, Steffan JS. Treating offenders with mental illness: a research synthesis. Law Hum Behav. 2012;36(1):37. https://doi.org/10.1037/h0093964.
(WHO) WHO. ICD-9: International classification of diseases (9th revision). Geneva: World Health Organization; 1978.
World Health Organization (WHO). ICD-10: International statistical classification of diseases and related health problems: Tenth revision, 5th ed. Geneva: World Health Organization; 2016.
Leucht S, Samara M, Heres S, Patel MX, Furukawa T, Cipriani A, et al. Dose equivalents for second-generation antipsychotic drugs: the classical mean dose method. Schizophr Bull. 2015;41(6):1397–402. https://doi.org/10.1093/schbul/sbv037.
Leucht S, Samara M, Heres S, Patel MX, Woods SW, Davis JM. Dose equivalents for second-generation antipsychotics: the minimum effective dose method. Schizophr Bull. 2014;40(2):314–26. https://doi.org/10.1093/schbul/sbu001.
Gardner DM, Murphy AL, O’Donnell H, Centorrino F, Baldessarini RJ. International consensus study of antipsychotic dosing. Am J Psychiatry. 2010;167(6):686–93. https://doi.org/10.1176/appi.ajp.2009.09060802.
Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for Schizophrenia. Schizophr Bull. 1987;13(2):261–76. https://doi.org/10.1093/schbul/13.2.261.
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88. https://doi.org/10.1177/1049732305276687.
Habermeyer E, Wolff R, Gillner M, Strohm R, Kutscher S. Patienten mit schizophrenen Störungen im psychiatrischen Maßregelvollzug. Nervenarzt. 2010;81(9):1117–24.
Kutscher S, Schiffer B, Seifert D. Schizophrene Patienten im psychiatrischen Maßregelvollzug (§ 63 StGB) Nordrhein-Westfalens. Fortschritte der Neurologie· Psychiatrie. 2009;77(02):91–6; doi: https://doi.org/10.1055/s-0028-1109080.
Seifert D. Die Entwicklung des psychiatrischen Massregelvollzzugs (§ 63StGB) in Nordrhein-Wesfalen. Psychiat Prax. 1997;24:237–44.
Brennan PF, Hays BJ. Focus on psychometrics the kappa statistic for establishing interrater reliability in the secondary analysis of qualitative clinical data. Res Nurs Health. 1992;15(2):153–8. https://doi.org/10.1002/nur.4770150210.
Schreiber JB. Latent class analysis: an example for reporting results. Res Social Adm Pharm. 2017;13(6):1196–201. https://doi.org/10.1016/j.sapharm.2016.11.011.
Völlm B, Edworthy R, Holley J, Talbot E, Majid S, Duggan C, et al. A mixed-methods study exploring the characteristics and needs of long-stay patients in high and medium secure settings in England: implications for service organisation. Health Service Deliv Res. 2017;5:1.
Asparouhov T, Muthén B. Variable-specific entropy contribution. 2018. http://www.statmodel.com/download/UnivariateEntropy.pdf; (Cited 2020.12.22)
Roeder K, Wasserman L. Practical Bayesian density estimation using mixtures of normals. J Am Stat Assoc. 1997;92(439):894–902. https://doi.org/10.1080/01621459.1997.10474044.
Soromenho G. Comparing approaches for testing the number of components in a finite mixture model. Comput Statistics. 1994;9(1):65–78.
Linzer DA, Lewis JB. poLCA: an R package for polytomous variable latent class analysis. J Stat Softw. 2011;42(10):1–29.
Lau S, Günther MP, Kling S, Kirchebner J. Latent class analysis identified phenotypes in individuals with schizophrenia spectrum disorder who engage in aggressive behaviour towards others. Eur Psychiatry. 2019;60:86–96. https://doi.org/10.1016/j.eurpsy.2019.05.005.
Cross TP, Walsh WA, Simone M, Jones LM. Prosecution of child abuse: a meta-analysis of rates of criminal justice decisions. Trauma Violence Abuse. 2003;4(4):323–40. https://doi.org/10.1177/1524838003256561.
Ujeyl M, Habermann N, Briken P, Berner W, Hill A. Sexuelle Tötungsdelikte [Comparison of sexual murderers in forensic psychiatric hospitals and in prison]. Nervenarzt. 2008;79(5):587–93. https://doi.org/10.1007/s00115-007-2394-x.
Steinau S, Brackmann N, Sternemann U, Biller-Andorno N, Habermeyer E. Conflicting priorities between risk management and mental health treatment–a case report. Front Psychiatry. 2018;9:680. https://doi.org/10.3389/fpsyt.2018.00680.
Andrews DA, Bonta J. The psychology of criminal conduct: Routledge; 2010.
Riecher-Rössler A. Vulnerability and protective factors for mental health: a rereading in gender perspective. Health and Gender: Springer; 2019. p. 25–36.
Howner K, Andiné P, Bertilsson G, Hultcrantz M, Lindström E, Mowafi F, et al. Mapping systematic reviews on forensic psychiatric care: identifying knowledge gaps. Front Psychiatry. 2018;9:452. https://doi.org/10.3389/fpsyt.2018.00452.
Witt K, Van Dorn R, Fazel S. Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies. PLoS ONE. 2013;8(2):e55942. https://doi.org/10.1371/journal.pone.0055942.
Kulkarni J, Butler S, Riecher-Rössler A. Estrogens and SERMS as adjunctive treatments for schizophrenia. Front Neuroendocrinol. 2019. https://doi.org/10.1016/j.yfrne.2019.03.002.
Riecher-Rössler A, Häfner H. Gender aspects in schizophrenia: bridging the border between social and biological psychiatry. Acta Psychiatr Scand. 2000;102:58–62. https://doi.org/10.1034/j.1600-0447.2000.00011.x.
Buchanan A, Sint K, Swanson J, Rosenheck R. Correlates of future violence in people being treated for schizophrenia. Am J Psychiatry. 2019;176(9):694–701. https://doi.org/10.1176/appi.ajp.2019.18080909.
Motz A. The psychology of female violence: Crimes against the body. Routledge; 2016.
Long CG, Fulton B, Hollin CR. The development of a ‘best practice’service for women in a medium-secure psychiatric setting: treatment components and evaluation. Clin Psychol Psychotherapy. 2008;15(5):304–19. https://doi.org/10.1002/cpp.591.
Archer M, Lau Y, Sethi F. Women in acute psychiatric units, their characteristics and needs: a review. BJPsych bulletin. 2016;40(5):266–72.
Määttä S. Exploring male and female patients’ experiences of psychiatric hospital care: a critical analysis of the literature. Issues Mental Health Nursing. 2009;30(3):174–80.
Nylund-Gibson K, Choi AY. Ten frequently asked questions about latent class analysis. Transl Issues Psychol Sci. 2018;4(4):440. https://doi.org/10.1037/tps0000176.
Acknowledgements
Not applicable.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MG, JK and SL conceived and designed the study. Data collection was performed by JK and SL. Material preparation and analysis were performed by MG and SK. The first draft of the manuscript was done by MG. All the authors edited multiple drafts and supervised the statistical analyses. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was reviewed and approved by the Cantonal Ethics committee of Zurich, Switzerland (Ref.-No. KEK-ZH-NR 2014-0480). This is a retrospective study. For this type of study, formal consent is not required. The authors assert that all the procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Günther, M.P., Lau, S., Kling, S. et al. Different needs in patients with schizophrenia spectrum disorders who behave aggressively towards others depend on gender: a latent class analysis approach. Ann Gen Psychiatry 20, 20 (2021). https://doi.org/10.1186/s12991-021-00343-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12991-021-00343-5