
Abstract
Among forensic patients with schizophrenia spectrum disorders, the association between symptomatology and violence is still not entirely clear in literature, especially because symptoms shift both during the acute phase of the illness and after. The aims were to investigate the level of symptomatology in forensic patients and to evaluate if there are differences in the level of symptoms between forensic and non-forensic patients. According to PRISMA guidelines, a systematic search was performed in PubMed, Web of Science, and ProQuest, using the following key words: “forensic” AND “Positive and Negative Syndrome Scale” OR “PANSS”. A total of 27 studies were included in the systematic review, while only 23 studies in the meta-analysis. The overall sample included a total of 1702 participants, most commonly male and inpatients in forensic settings. We found that studies with an entirely male sample had significantly lower Positive PANSS ratings than studies with mixed samples. Although both forensic and non-forensic patients were affected by mild psychopathological symptoms, forensic patients presented higher ratings in all four PANSS scales. This meta-analysis shows that forensic patients reported a mild level of symptomatology, as assessed with the PANSS, and therefore might be considered as patients in partial remission. Among patients with schizophrenia, the association between symptoms and violence is very complex: many factors might be considered as key mediators and thus should be taken into account to explain this association. Further studies are needed.
Trial registration all materials and data can be found on the OSF framework: https://osf.io/5ceja (date of registration: 8 September 2021)
Similar content being viewed by others


Background
Many studies on the association between schizophrenia and violence have been published in recent years [1,2,3,4]. These studies showed that violent behaviour is more common during the acute phase of the illness [4,5,6,7,8,9]. A meta-analysis of 110 studies on risk factors for violence in psychosis concluded that higher general symptom ratings and higher total Positive and Negative Syndrome Scale (PANSS [10]) ratings were associated with violence. With regards to specific positive symptoms, violence was associated with higher excitement ratings and higher positive symptoms ratings. According to one meta-analysis, violence was not significantly associated with negative symptomatology [11], while others found that negative symptoms were inversely associated with the risk of violence [12,13,14].
Despite these results, the role played by psychotic symptoms is still not entirely clear in literature, especially because symptoms shift both during the acute phase and later in the course of this disorder [13]. For this reason, it seems important to understand what are the symptom profiles of people at a different time to when they committed violence, particularly in people who have committed crimes and who live in forensic services. Forensic patients are a heterogeneous population who differ widely in diagnoses, crimes committed, and risk factors. All these aspects are important, have treatment implications, and should consequently be accounted for in research. Violent acts are also diverse, whether minimal or homicidal in severity, whether deliberative or impulsive, instrumental or expressive, intoxicated, driven by delusions, or in the absence of an abnormal mental state [15,16,17].
Given the wide interest for the structured clinical assessment of severe mental disorders and the large utilization of PANSS to evaluate symptomatology in patients with Schizophrenia Spectrum Disorders (SSDs), we decided to conduct a systematic review and meta-analysis on PANSS ratings in forensic populations.
Methods
The aims of this systematic review and meta-analysis were (a) to investigate the level of psychotic symptomatology assessed by the PANSS in patients with SSDs in treatment at psychiatric forensic institutions and to identify specific variables associated with symptom severity and (b) to assess differences in symptom severity between forensic and non-forensic patients with SSDs.
The PANSS [10] is a 30-item rating scale on a scale of 1 (absent) to 7 (severe) developed by combining the 18 items of the Brief Psychiatric Rating Scale (BPRS) [18] and 12 items from the Psychopathology Rating Scale (PRS) using clear definitions to tether each gradation of each item; the PANSS overall total score ranges from 30 to 210.
Protocol and registration
In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [19], our systematic review protocol was registered with Open Science Foundation (OSF) database. All materials and data can be found on the OSF framework: https://osf.io/5ceja (date of registration: 8 September 2021).
Eligibility criteria
To be included in the meta-analysis, we defined the following eligibility criteria: (a) studies focusing on adult forensic patients (age > 18 years); (b) studies, including patients suffering from SSDs (at least 50% of the sample); and (c) studies reporting PANSS mean ratings. Since studies on forensic populations are in limited number, we included studies with different designs (randomized clinical trials, observational studies). All studies included patients with mental illness who committed any offences and therefore were in charge of forensic services (including outpatients and inpatients). We excluded case reports, dissertations, protocols, reviews, case series studies, unpublished studies, and studies in languages other than English.
Information sources and search strategy
All published peer-reviewed articles were retrieved through a systematic literature search on PubMed, Web of Science and ProQuest from inception to September 2020, using the following key words: “forensic” AND “Positive and Negative Syndrome Scale” OR “PANSS”.
Study selection
Two authors independently (CB and GS) screened the article titles and abstracts for inclusion and exclusion criteria and extracted data from all full-text articles selected. Any disagreements in data extraction process were negotiated among two authors.
Data collection process
Data were collected in a specific data extraction form, reporting the following items: (a) study characteristics––authorship, year, country of recruitment, and study design; (b) sample characteristics––number of subjects with SSDs who entered the study, mean age, gender, type of treatment (inpatients or outpatients), illness duration, and length of stay; and (c) PANSS mean ratings available (Positive, Negative, General, and Total). When the studies included non-forensic patients, we also collected their data. Moreover, for studies reporting PANSS mean ratings at baseline and follow-up, only baseline ratings were used, in order to exclude the effect of specific treatment on PANSS scores.
Statistical analysis
Data analysis was divided into two parts: the first only included forensic patients, while the second comprised both forensic and non-forensic patients.
Firstly, random-effects meta-analysis was performed to calculate a pooled estimate of the mean PANSS rating for each scale (Positive, Negative, General, and Total) with 95% confidence intervals among forensic patients. We decided for a random-effects approach assuming there would be heterogeneity among the studies included in the analysis [20]. Some characteristics of studies were identified as potential modifiers of the reported results. For this reason, subgroup analysis was performed in order to evaluate the differences in PANSS mean ratings (four scales) among studies with: SSD patients only or also including non-SSD patients; inpatient (In), or outpatient study setting (Out, Mix); males only or also including females; patients older than the first quartile of the age distribution or patients within the first quartile; and high-quality or low-quality studies.
Secondly, random-effects meta-analysis was performed to calculate a pooled estimate of the mean difference between forensic and non-forensic patients in each of the PANSS scales (Positive, Negative, General, and Total rating) with 95% confidence intervals.
In order to measure the heterogeneity among the studies included in the analysis, we used the Q-statistic and I2 index (% of total variability due to heterogeneity): a significant value of Q and an I2 larger than 50% indicate the presence of heterogeneity between the studies in analysis [21]. Publication bias was assessed by performing the rank correlation test–Begg’s test [22].
Data analysis was performed in R: a language and environment for statistical computing, version 4.0.3 [23] by using the “metafor” package [24]. Data and code to replicate the analysis are available here: https://github.com/cstrozza91/Meta-Analysis-PANSS-2021.git.
Results
Study selection
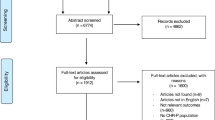
As shown in Fig. 1, out of 1064 articles generated by the preliminary search strategy, 58 were duplicates, and 960 were excluded based on title and abstract as they were irrelevant to study criteria. After reading the full text, a further 19 studies were excluded because they did not report PANSS mean ratings, or because they were based on the five-factor model of the PANSS scoring or on an adapted version of the scale. Several analytic factor solutions have been published and generally supported the presence of five different symptom dimensions: Positive, Negative, Disorganization (often termed “Cognitive”), Affect (often termed “Depression-Anxiety”), and Resistance or Excitement/Activity [25]. However, these studies have shown that the exact composition of the items defining these factors varied [26, 27]. Despite the general similarity of these five-factor models, no single model has achieved broad consensus, and for this reason it is difficult to compare the results of different studies. Therefore, in this systematic review we included only those studies using the original standard PANSS scoring model [10]. This scoring model provides the following scales: Positive, Negative, General, and a Total rating computed using all the 30 items.

Flow chart of the selection process. PRISMA Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Others studies were excluded because they did not report distinct PANSS mean ratings for forensic and non-forensic patients or because they included subjects under 18 years. Finally, when two or more studies reported overlapping samples, priority was given to the study with the largest sample size or to randomized clinical trial (RCT). Finally, 27 studies were included in the systematic review. Of these 27 studies, 4 were excluded from the meta-analytical calculations because they did not report the standard deviations of PANSS ratings, while 23 were used for the meta-analysis: 18 for the Positive scale, 17 for the Negative scale, 15 for General scale, and 17 for the Total rating.
Studies and sample characteristics
Table 1 shows the characteristics of the 27 included studies. Publications were from 13 countries: Brazil, Croatia, Germany, Ireland, Israel, Japan, Kosovo, the Netherlands, Norway, Turkey, UK, USA, and Russia, with Ireland the country with the largest number of studies (N = 9). Studies varied in their sample sizes (from a low of 16 up to 150 forensic patients) and included a total of 1702 participants, most commonly male and inpatients. Sample mean age was 38.4 (SD = 9.6). All studies had samples that included at least 82% of patients with SSD (19 studies 100%), except one study with a percentage of 73.9%. Illness duration and length of stay were reported in only few studies. Regarding PANSS ratings, only 14 studies reported all 4 scales’ ratings: Positive, Negative, General, and Total. In 11 studies there were info about the specific training in PANSS administration received by the assessors [31, 33, 34, 36, 38, 42, 44, 45, 50, 52, 53].
Most studies were aimed at assessing the efficacy of some programmes to reduce violence, such as metacognitive training [28], and other psychosocial and rehabilitation interventions [29,30,31]. Other studies were aimed at investigating neurocognitive functions [32,33,34], neuropsychological impairment [35], facial emotion recognition, neurocognition, and social cognition [36,37,38,39]. Further studies were aimed to investigate patients’ opinions on certain aspects of perceived stigmatization [40], insight deficits [41], working alliance and interpersonal trust in clinicians [42], and decision-making ability [43,44,45]. Additional studies were centred on psychopharmacological treatment [46, 47] or schizophrenia biomarkers [48]. Finally, one study focused on temperament and character [49], one on a validation tool [50], one on the relationships between delusions and violence [51], one on age of onset and violence [52], one on risk stratification and the care pathway [53], and one on new structured professional judgment instruments for assessing need for therapeutic security, treatment completion, and recovery in forensic settings [54].
Methodological quality and risk of bias within studies
Among the studies included in this review, there were 3 RCTs [30, 33, 36] and 24 observational studies [28, 29, 31, 32, 34, 35, 37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54]. Risk bias of randomized studies based on the Cochrane quality assessment tool was low (Additional file 2: Table S1). Only one study had four domains with a high risk [33], showing therefore a low quality. All cohort and case–control studies showed a high quality. With respect to cross-sectional studies only two articles were categorized of low quality [32, 38] (Additional files 3: Table S2 and 4: Table S3).
In the seven studies comparing forensic and non-forensic patients, Frommann et al. [38] reported that subjects were matched for age, intelligence, additional addiction, medication and illness duration; in another study [34] forensic and non-forensic subjects were matched for age. In the remaining five studies there is no clear indication of matching, although in all these studies there was a comparison of basic sociodemographic and clinical features, with tests of significance.
Results of the meta-analysis
Table 2 (the first line called Total for each scale) shows the estimated mean values of the four PANSS scales for the 23 studies included in the meta-analysis: Positive, Negative, General, and Total. The analysis showed significant I2 and Q ratings (with an overall number of studies considered to be greater than 15), indicating a high level of between-study heterogeneity in terms of symptomatology in forensic patients with SSDs, assessed by the four PANSS scales. Figure 2 shows the estimated mean values, using the random-effects model, for each PANSS scale. Forensic patients’ PANSS mean ratings were as follows: Positive 14.6, Negative 16.7, General 31.3, and Total 65.2. Moreover, only seven studies had a control group of non-forensic patients, and their PANSS mean ratings were as follows: Positive 14.4, Negative 14.9, General 29.1, and Total 52.9.

Estimated mean values of PANSS scales in forensic patients
The variables considered in the subgroup analysis were the percentage of patients with SSDs, the percentage of males in the total sample, the setting (inpatients versus outpatients), the mean age and the study quality, assessed by the Newcastle–Ottawa Scale (NOS), and the Cochrane quality assessment tool. Results about the setting and study quality were not included due to the small number of studies related to one of the two subgroups created (inpatients versus outpatients and high versus low study quality). The only statistically significant difference about gender was in the Positive scale: studies including only males reported significantly lower ratings than studies with mixed samples (males and females). Furthermore, the I2 was greater than 95% demonstrating high heterogeneity between the studies analysed.
As regards the comparison between forensic and non-forensic patients, significant differences were found in the mean PANSS scale ratings, as suggested by the p-values with the relative estimate mean difference, except for the “Total scale” for which the number of studies considered was limited (Table 3). Forensic patients showed higher values in Positive, Negative, and General scales, but the analysis about the Negative scale reported non-significant I2 and Q indicating little between-study heterogeneity in terms of negative symptomatology. This was probably due to the limited number of studies analysed (N = 7). Figure 3 shows the estimated mean difference between forensic and non-forensic patients, using the random-effects model, for each PANSS scale.

Estimated mean difference between forensic and non-forensic patients
Discussion
This is the first meta-analysis about the severity of psychopathology as assessed with the PANSS in forensic patients with SSD. Our results show that the studies included in this meta-analysis provide a good picture of the level and severity of the overall psychotic symptomatology to be found among forensic patients with SSD, assessed with the PANSS.
Our data show that forensic patients exhibit a mild psychopathological symptomatology. Leucht et al. [55] have speculated on the clinical meaning of PANSS total ratings and have tried to anchor PANSS ratings to CGI ratings in a large sample of patients with schizophrenia. In this way they have identified the following PANSS levels: ‘normal’ (range < 48), ‘borderline mentally ill’ (range 48–60), ‘mildly ill’ (range 61–78), ‘moderately ill’ (range 79–95), ‘markedly ill’, ‘severely ill’ (range 96–118), and ‘extremely ill’ (range > 118) (Additional file 5: Table S4). Based on these data, the mean Total rating of forensic patients included in our meta-analysis points to a clinical condition that can be labelled as ‘mildly ill’. This would hold true only if ratings on each item were broadly similar, for example, with evidence for a high degree of internal consistency for all items contributing to the total rating. This conflicts with the separation between the scales for Positive, Negative, and General symptoms. The use by Leucht et al. [55] of percentage change in the CGI is also problematic as this may not relate meaningfully to baseline severity of symptoms or of functional impairment, though there is some evidence for this [56].
This result may also suggest that a large proportion of these patients were in remission, where “remission” was defined as a low-mild symptom intensity level [57, 58]. Andreasen et al. [57] set a rigorous standard for response (rating of 3 or less in eight key items P1, P2, P3, N1, N4, N6, G5, and G9) and remission, the same sub-threshold ratings in all eight key items sustained for at least 6 months. Others have used much shorter time periods to define response and remission [59]. It is therefore problematic to define a cut-off based on total ratings of a rating scale, under which a patient is considered to be in remission. Schizophrenia is a heterogeneous disorder characterized by a range of possible different symptoms, especially positive and negative symptoms, and their prevalence also depends on the disorder stage [60]. Schizophrenia can be staged as it develops [61]. Positive symptoms have been regarded as features of early and acute schizophrenia, with negative symptoms developing during later stages of the illness [62].
It is worth noting that our results are very different from data obtained in other studies reporting PANSS values in non-forensic patients with schizophrenia: a recent meta-analysis of Matsusaki et al. [63], including 47 trials comparing antipsychotic medications to placebo found much higher PANSS ratings, ranging from a low of 57.6 to a high of 100.8 with a mean of 92.5 (SD = 7.6). A systematic PubMed advanced search [64] reported much higher PANSS ratings than ours, but many clinical characteristics of patients and the illness phase were not clearly specified. They also excluded studies on patients with schizophrenia in remission, following Andreasen’s criteria [57]. Also, in a recent RCT to evaluate the efficacy and safety of a new compound in adults with an acute exacerbation of schizophrenia, the mean Total rating on the PANSS at baseline was much higher as compared to the mean rating found in our forensic sample [65].
Clinical characteristics of patients studied in forensic settings
Our finding of low PANSS ratings might be explained by sample composition, that is, inpatients living in forensic facilities; these patients may also include patients who were admitted to forensic settings for reasons different from violent offences; while it is impossible to make this discrimination in the selected articles, it is well known that the large majority of people admitted to forensic settings has been admitted specifically because they committed violent offences. Being in a forensic facility implies that patients had guaranteed pharmacological treatment, which promotes clinical stabilization, symptoms reduction, and a better course of the disorder. Moreover, some studies have shown that ensuring treatment compliance decreases the risk of violence [66,67,68].
Nevertheless, many clinical characteristics of patients included in our meta-analysis were unspecified, and this makes it difficult to draw precise conclusions. For example, illness duration may strongly affect clinical assessment in people with SSD. As suggested by Fountoulakis et al. [69], PANSS ratings probably change according to the stage of schizophrenia. Similarly, Zhao et al. [70] have investigated different stages of schizophrenia comparing first episode to chronic patients. The PANSS total rating clearly indicated that in patients with chronic conditions the severity of symptomatology was lower. In fact, while first-episode patients reported a higher PANSS total rating corresponding to ‘moderately ill’ level, chronic patients showed a lower rating corresponding to ‘mildly ill’ level [55]. This result is consistent with our data.
Interestingly, we found that males had lower ratings than mixed samples on the Positive scale, and this may indicate that female forensic patients exhibit more severe psychotic symptoms. Nevertheless, this result should be interpreted with caution, as the percentage of female patients was very low in all mixed-sample studies (below 20%). In international prison surveys women make up only 10–15% of prison populations in cross-sectional or incident samples [71]; population-based surveys of community violence give a more complex picture in which violence is still less common than in men but less often prosecuted [72,73,74]. There are population differences between men and women in violence rates, including intimate partner violence involving not only both mental illnesses and personality traits, such as affective instability [73], but also differential social processes in the criminal justice system. A further exploration of this may be beyond the scope of this review.
Forensic and non-forensic patients with schizophrenia
Another important result of our meta-analysis has to do with the difference between forensic and non-forensic patients: forensic patients had higher ratings than non-forensic patients in all four PANSS scales. While the total rating of forensic patients shows a clinical condition corresponding to ‘mildly ill’ [55], the total rating of non-forensic patients corresponds to ‘borderline mentally ill’. It is important to note that only 7 out of 27 studies included in this meta-analysis reported non-forensic patients. Therefore, the small number of studies does not allow a reliable generalization of this result. Nevertheless, it seems possible to consider that both forensic and non-forensic patients included in these studies were in symptom remission.
Schizophrenia is both a relapsing and remitting illness and a progressive illness that can be staged from prodromal or ‘at risk mental states’ (attenuated psychosis, brief limited intermittent psychosis) with diagnostic criteria that include symptom rating items very similar to PANSS items [75, 76]. These prodromal or ‘at risk’ states can be identified in juvenile forensic populations [77] and may lend themselves to transdiagnostic formulations [78, 79]. Schizophrenia appears to progress through stages from relapsing and remitting to chronic and disabling, and it is unclear whether specific symptom patterns distinguish early stages of illness when violence may be more common [5, 80, 81].
Outcome evaluations in forensic settings
The use of the PANSS to assess the working of a model of care in forensic psychiatry, such as stratified therapeutic security, is well documented and necessary for the delivery of treatment for violent patients with SSD in forensic hospital and community settings [53, 82]. A prospective cross-validation study indicated that PANSS symptom severity correlates with measures of violence proneness, such as the HCR-20 (Assessing Risk of Violence) dynamic scales, and is a medium-term predictor of inpatient violence and self-harm [83]. Treatment response and completion can be related to reductions in violence proneness, although the explanatory model is complex and includes symptom severity (PANSS) and functional neurocognition [31]. Change in symptom severity measured by PANSS is increasingly recognized as just one measure of therapeutic process and outcome for a forensic model of care, one of the four recoveries: forensic recovery, functional recovery, symptomatic recovery and personal recovery [84].
Measures of personal recovery, such as working alliance and interpersonal trust in physician, are partly confounded by symptom severity [85], as is perceived procedural justice and perceived impact of a review board hearing [42]. Measures of subjective experience and appraisals as part of personal recovery should always be adjusted for symptom severity to take account of subjective perceptual bias due to symptoms.
New models of analysis have allowed an understanding of the relationship between symptoms, such as delusions measured with the PANSS, and outcomes, such as violent acts, when causal modelling includes proximity in time and mediation via symptoms such as anger [8, 13, 86]. This should lend a new and valuable function for PANSS items and ratings in repeated measures paradigms of longitudinal research into causes, for example, concerning the relationship between delusions, moral sentiment, and violent acts [87].
Limitations
This review has several limitations. First of all, among 27 studies included in this review, only 3 used random samples. Secondly, many studies had very small samples, which reduces the generalizability of our results. Furthermore, the sample is partially heterogeneous with regard to the diagnosis; however, the majority of the sample analysed had a SSD diagnosis: out of 27 studies, only in one case there was a percentage of 73.9 patients with SSD in the study sample, in 5 studies this percentage exceeded 80%, in 2 studies over 90% while 19 studies report 100% of patients with SSD. Our choice was made to include a larger number of studies (as the literature on this topic is rather limited). Moreover, this meta-analysis included mainly male patients and gender differences must be interpreted with caution. The higher percentage of males than females in the study samples is due to the fact that all studies show that males are more frequently violent than females [88, 89]. Besides, these studies often missed information on how much time passed since the index violence to the admission to a forensic institution: PANSS assessment was done at different times, rather than at the time of the relevant violent offence. This fact makes it difficult to clearly understand the association between psychotic symptoms as picked up by PANSS and violent behaviour when it occurred. Furthermore, the selected studies involved patients who signed an informed consent: thus, some forensic patients who were too symptomatic to be able to understand the information required for informed consent were not studied. The results therefore may not completely represent the population of forensic patients. Finally, since forensic patients follow different care pathways in different countries, it is difficult to draw generalizations given the heterogeneity of the population.
Conclusion
This meta-analysis demonstrates that forensic patients included in studies employing the PANSS for the assessment of psychotic symptoms exhibit a mild symptom severity and therefore may be considered as patients in remission. This result is most likely related to the high compliance to the pharmacological treatments ensured in forensic facilities. This may suggest that treatment is effective in fostering symptom remission even among patients with schizophrenia who committed severe violent acts.
However, it is important to consider that studies included in this meta-analysis do not always define what they mean by violence. Forensic patients are a heterogeneous population and violence can occur in different forms (verbal and/or physical aggression and so on). Additionally, these studies did not report when forensic patients committed the index violence and when they were admitted to forensic services: they may have behaved violently many years ago, and patients’ level of aggressive behaviour at the time of PANSS assessment is not specified. For these latter considerations, it is necessary to be very careful when drawing conclusions about the relationship between symptom severity and violence based on these studies. The association between schizophrenia, and in particular psychotic symptoms, and violence is a very complex phenomenon, and still partially unexplained [86, 87, 90]. In fact, there are many factors that act as key mediators between psychotic symptoms and violence, which should be taken into account to explain this association. For example, a large body of research has identified eight central criminogenic risk factors, including antisocial personality, antisocial attitudes, antisocial peers, substance abuse, history of antisocial behaviour, relationship/familial problems, vocational difficulties, and lack of leisure activities [91]. For all these reasons, further studies on this topic are needed.
Availability of data and materials
The datasets generated and/or analysed during the current study are available here: https://github.com/cstrozza91/Meta-Analysis-PANSS-2021.git.
Abbreviations
- PANSS:
-
Positive and Negative Syndrome Scale
- SSDs:
-
Schizophrenia spectrum disorders
- BPRS:
-
Brief Psychiatric Rating Scale
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- OSF:
-
Open Science Foundation
- RCT:
-
Randomized controlled trials
- NOS:
-
Newcastle–Ottawa Scale
- HCR-20:
-
Assessing risk of violence
References
Barkataki I, Kumari V, Das M, Hill M, Morris R, O’Connell P, et al. A neuropsychological investigation into violence and mental illness. Schizophr Res. 2005;74(1):1–13. https://doi.org/10.1016/j.schres.2004.08.001.
Darrell-Berry H, Berry K, Bucci S. The relationship between paranoia and aggression in psychosis: a systematic review. Schizophr Res. 2016;172(1–3):169–76. https://doi.org/10.1016/j.schres.2016.02.009.
Imai A, Hayashi N, Shiina A, Sakikawa N, Igarashi Y. Factors associated with violence among Japanese patients with schizophrenia prior to psychiatric emergency hospitalization: a case-controlled study. Schizophr Res. 2014;160(1–3):27–32. https://doi.org/10.1016/j.schres.2014.10.016.
Large MM, Nielssen O. Violence in first-episode psychosis: a systematic review and meta-analysis. Schizophr Res. 2011;125(2–3):209–20. https://doi.org/10.1016/j.schres.2010.11.026.
Coid JW, Ullrich S, Kallis C, Keers R, Barker D, Cowden F, et al. The relationship between delusions and violence: findings from the East London first episode psychosis study. JAMA Psychiat. 2013;70(5):465–71. https://doi.org/10.1001/jamapsychiatry.2013.12.
Keers R, Ullrich S, Destavola BL, Coid JW. Association of violence with emergence of persecutory delusions in untreated schizophrenia. Am J Psychiatry. 2014;171(3):332–9. https://doi.org/10.1176/appi.ajp.2013.13010134.
Nielssen O, Large M. Rates of homicide during the first episode of psychosis and after treatment: a systematic review and meta-analysis. Schizophr Bull. 2010;36(4):702–12. https://doi.org/10.1093/schbul/sbn144.
Ullrich S, Keers R, Coid JW. Delusions, anger, and serious violence: new findings from the MacArthur violence risk assessment study. Schizophr Bull. 2014;40(5):1174–81. https://doi.org/10.1093/schbul/sbt126.
Van Dorn RA, Grimm KJ, Desmarais SL, Tueller SJ, Johnson KL, Swartz MS. Leading indicators of community-based violent events among adults with mental illness. Psychol Med. 2017;47(7):1179–91. https://doi.org/10.1017/S0033291716003160.
Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–76. https://doi.org/10.1093/schbul/13.2.261.
Witt K, van Dorn R, Fazel S. Risk factors for violence in psychosis: systematic review and meta-regression analysis of 110 studies. PLoS ONE. 2013;8(2):e55942. https://doi.org/10.1371/journal.pone.0055942.
Bulgari V, Iozzino L, Ferrari C, Picchioni M, Candini V, De Francesco A, et al. Clinical and neuropsychological features of violence in schizophrenia: a prospective cohort study. Schizophr Res. 2017;181:124–30. https://doi.org/10.1016/j.schres.2016.10.016.
Coid JW, Kallis C, Doyle M, Shaw J, Ullrich S. Shifts in positive and negative psychotic symptoms and anger: effects on violence. Psychol Med. 2018;48(14):2428–38. https://doi.org/10.1017/S0033291718000077.
Swanson JW, Swartz MS, Van Dorn RA, Elbogen EB, Wagner HR, Rosenheck RA, et al. A national study of violent behavior in persons with schizophrenia. Arch Gen Psychiatry. 2006;63(5):490–9. https://doi.org/10.1001/archpsyc.63.5.490.
Cornell DG, Warren J, Hawk G, Stafford E, Oram G, Pine D. Psychopathy in instrumental and reactive violent offenders. J Consult Clin Psychol. 1996;64:783. https://doi.org/10.1037//0022-006x.64.4.783.
Meloy JR. Empirical basis and forensic application of affective and predatory violence. Aust N Z J Psychiatry. 2006;2006(40):539–47. https://doi.org/10.1080/j.1440-1614.2006.01837.x.
Tyrer P, Cooper S, Herbert E, Duggan C, Crawford M, Joyce E, et al. The quantification of violence scale: a simple method of recording significant violence. Int J Soc Psychiatry. 2007;53:485–97. https://doi.org/10.1177/0020764007083870.
Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. 1962;10:799–812.
Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA group preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. https://doi.org/10.1136/bmj.b2535.
Hedges LV, Vevea JL. Fixed- and random-effects models in meta-analysis. Psychol Methods. 1998;3(4):486–504. https://doi.org/10.1037/1082-989X.3.4.486.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60. https://doi.org/10.1136/bmj.327.7414.557.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–101. https://doi.org/10.2307/2533446.
R Core Team. R: the R Project for Statistical Computing, 2020.
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010. https://doi.org/10.18637/jss.v036.i03.
Shafer A, Dazzi F. Meta-analysis of the Positive and Negative Syndrome Scale (PANSS) factor structure. J Psychiatr Res. 2019;115:113–20. https://doi.org/10.1016/j.jpsychires.2019.05.008.
Lehoux C, Gobeil MH, Lefebvre AA, Maziade M, Roy MA. The five factor structure of the PANSS: a critical review of its consistency across studies. Clin Schizophr Relat Psychoses. 2009;3(2):103–10.
Wallwork RS, Fortgang R, Hashimoto R, Weinberger DR, Dickinson D. Searching for a consensus five-factor model of the Positive and Negative Syndrome Scale for schizophrenia. Schizophr Res. 2012;137(1–3):246–50. https://doi.org/10.1016/j.schres.2012.01.031.
Naughton M, Nulty A, Abidin Z, Davoren M, O’Dwyer S, Kennedy HG. Effects of group metacognitive training (MCT) on mental capacity and functioning in patients with psychosis in a secure forensic psychiatric hospital: a prospective-cohort waiting list controlled study. BMC Res Notes. 2012. https://doi.org/10.1186/1756-0500-5-302.
Hornsveld RH, Nijman HL. Evaluation of a cognitive-behavioral program for chronically psychotic forensic inpatients. Int J Law Psychiatry. 2005;28(3):246–54. https://doi.org/10.1016/j.ijlp.2004.09.004.
Cullen AE, Clarke AY, Kuipers E, Hodgins S, Dean K, Fahy T. A multisite randomized trial of a cognitive skills program for male mentally disordered offenders: violence and antisocial behavior outcomes. J Consult Clin Psychol. 2012;80(6):1114–20. https://doi.org/10.1037/a0030291.
Richter MS, O’Reilly K, O’Sullivan D, O’Flynn P, Corvin A, Donohoe G, et al. Prospective observational cohort study of ‘treatment as usual’ over four years for patients with schizophrenia in a national forensic hospital. BMC Psychiatry. 2018. https://doi.org/10.1186/s12888-018-1862-0.
Engelstad KN, Vaskinn A, Torgalsbøen AK, Mohn C, Lau B, Rund BR. Impaired neuropsychological profile in homicide offenders with schizophrenia. Compr Psychiatry. 2018;85:55–60. https://doi.org/10.1016/j.comppsych.2018.06.002.
Hundozi Z, Ibishi NF, Musliu NR. Cognitive functions and recidivism of aggressive behavior in schizophrenic inpatients at forensic unit clinic of psychiatry in Kosovo. Cogent Psychol. 2016;3(1):1233650. https://doi.org/10.1080/23311908.2016.1233650.
Kashiwagi H, Kuroki N, Ikezawa S, Matsushita M, Ishikawa M, Nakagome K, et al. Neurocognitive features in male patients with schizophrenia exhibiting serious violence: a case control study. Ann Gen Psychiatry. 2015. https://doi.org/10.1186/s12991-015-0086-7.
Nishinaka H, Nakane J, Nagata T, Imai A, Kuroki N, Sakikawa N, et al. Neuropsychological impairment and its association with violence risk in Japanese forensic psychiatric patients: a case–control study. PLoS ONE. 2016;11(1):e0148354. https://doi.org/10.1371/journal.pone.0148354.
Taylor R, Cella M, Csipke E, Heriot-Maitland C, Gibbs C, Wykes T. Tackling social cognition in schizophrenia: a randomized feasibility trial. Behav Cogn Psychother. 2016;44(3):306–17. https://doi.org/10.1017/S1352465815000284.
Demirbuga S, Sahin E, Ozver I, Aliustaoglu S, Kandemir E, Varkal MD, et al. Facial emotion recognition in patients with violent schizophrenia. Schizophr Res. 2013;144(1–3):142–5. https://doi.org/10.1016/j.schres.2012.12.015.
Frommann N, Stroth S, Brinkmeyer J, Wölwer W, Luckhaus C. Facial affect recognition performance and event-related potentials in violent and non-violent schizophrenia patients. Neuropsychobiology. 2013;68(3):139–45. https://doi.org/10.1159/000353252.
O’Reilly K, Donohoe G, Coyle C, O’Sullivan D, Rowe A, Losty M, et al. Prospective cohort study of the relationship between neuro-cognition, social cognition and violence in forensic patients with schizophrenia and schizoaffective disorder. BMC Psychiatry. 2015. https://doi.org/10.1159/000353252.
Margetić B, Aukst-Margetic B, Ivanec D, Filipcić I. Perception of stigmatization in forensic patients with schizophrenia. Int J Soc Psychiatry. 2008;54(6):502–13. https://doi.org/10.1177/0020764008090842.
Buckley PF, Hrouda DR, Friedman L, Noffsinger SG, Resnick PJ, Camlin-Shingler K. Insight and its relationship to violent behavior in patients with schizophrenia. Am J Psychiatry. 2004;161(9):1712–4. https://doi.org/10.1176/appi.ajp.161.9.1712.
Donnelly V, Lynch A, Mohan D, Kennedy HG. Working alliance, interpersonal trust and perceived coercion in mental health review hearings. Int J Ment Health Syst. 2011;5(1):29.
Dornan J, Kennedy M, Garland J, Rutledge E, Kennedy HG. Functional mental capacity, treatment as usual and time: magnitude of change in secure hospital patients with major mental illness. BMC Res Notes. 2015. https://doi.org/10.1186/s13104-015-1547-4.
Kennedy M, Dornan J, Rutledge E, O’Neill H, Kennedy HG. Extra information about treatment is too much for the patient with psychosis. Int J Law Psychiatry. 2009;32(6):369–76. https://doi.org/10.1016/j.ijlp.2009.09.006.
Rutledge E, Kennedy M, O’Neill H, Kennedy HG. Functional mental capacity is not independent of the severity of psychosis. Int J Law Psychiatry. 2008;31(1):9–18. https://doi.org/10.1016/j.ijlp.2007.11.002.
Vasic N, Segmiller F, Rees F, Jäger M, Becker T, Ormanns N, et al. Psychopharmacologic treatment of in-patients with schizophrenia: comparing forensic and general psychiatry. J Forens Psychiatry Psychol. 2017. https://doi.org/10.1080/14789949.2017.1332773.
Horvath J, Steinert T, Jaeger S. Antipsychotic treatment of psychotic disorders in forensic psychiatry: patients’ perception of coercion and its predictors. Int J Law Psychiatry. 2018;57:113–21. https://doi.org/10.1016/j.ijlp.2018.02.004.
Storozheva ZI, Kirenskaya AV, Novototsky-Vlasov VY, Telesheva KY, Pletnikov M. Startle modification and P50 gating in schizophrenia patients and controls: Russian population. Span J Psychol. 2016;19(e8):1–11. https://doi.org/10.1017/sjp.2016.1.
Margetić B, Margetić BA, Ivanec D. Temperament and character in homicidal patients with schizophrenia. Nord J Psychiatry. 2019;73(6):317–22. https://doi.org/10.1080/08039488.2019.1630482.
Ivgi D, Bauer A, Khawaled R, Rosca P, Weiss JM, Ponizovsky AM. Validation of the HCR-20 scale for assessing risk of violent behavior in Israeli psychiatric inpatients. Isr J Psychiatry Relat Sci. 2015;52(2):121–7.
Teixeira EH, Dalgalarrondo P. Violent crime and dimensions of delusion: a comparative study of criminal and noncriminal delusional patients. J Am Acad Psychiatry Law. 2009;37(2):225–31.
Vinokur D, Levine SZ, Roe D, Krivoy A, Fischel T. Age of onset group characteristics in forensic patients with schizophrenia. Eur Psychiatry. 2014;29(3):149–52. https://doi.org/10.1016/j.eurpsy.2012.11.006.
Pillay SM, Oliver B, Butler L, Kennedy HG. Risk stratification and the care pathway. Ir J Psychol Med. 2008;25(4):123–7. https://doi.org/10.1017/S0790966700011228.
Davoren M, O’Dwyer S, Abidin Z, Naughton L, Gibbons O, Doyle E, et al. Prospective in-patient cohort study of moves between levels of therapeutic security: the DUNDRUM-1 triage security, DUNDRUM-3 programme completion and DUNDRUM-4 recovery scales and the HCR-20. BMC Psychiatry. 2012;12:80.
Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel RR. What does the PANSS mean? Schizophr Res. 2005;79:231–8. https://doi.org/10.1016/j.schres.2005.04.008.
Levine SZ, Rabinowitz J, Engel R, Etschel E, Leucht S. Extrapolation between measures of symptom severity and change: an examination of the PANSS and CGI. Schizophr Res. 2008;98:318–22. https://doi.org/10.1016/j.schres.2007.09.006.
Andreasen NC, Carpenter WT, Kane JM, Lasser RA, Marder SR, Weinberger DR. Remission in schizophrenia: proposed criteria and rationale for consensus. Am J Psychiatry. 2005;62:441–9. https://doi.org/10.1176/appi.ajp.162.3.441.
van Os J, Burns T, Cavallaro R, Leucht S, Peuskens J, Hwelldin L, et al. Standardized remission criteria in schizophrenia. Acta Psychiatr Scand. 2006;113:91–5. https://doi.org/10.1111/j.1600-0447.2005.00659.x.
Lin CH, Lin HS, Lin SC, Kuo CC, Wang FC, Huang YH. Early improvement in PANSS-30, PANSS-8, and PANSS-6 scores predicts ultimate response and remission during acute treatment of schizophrenia. Acta Psychiatr Scand. 2018;137:98–108. https://doi.org/10.1111/acps.12849.
Leucht S, Davis JM, Engel RR, Kissling W, Kane JM. Definitions of response and remission in schizophrenia: recommendations for their use and their presentation. Acta Psychiatr Scand. 2009;119(438):7–14. https://doi.org/10.1111/j.1600-0447.2008.01308.x.
Lavoie S, Polari AR, Goldstone S, Nelson B, McGorry PD. Staging model in psychiatry: review of the evolution of electroencephalography abnormalities in major psychiatric disorders. Early Interv Psychiatry. 2019;13:1319–28. https://doi.org/10.1111/eip.12792.
Vanes LD, Mouchlianitis E, Patel K, Barry E, Wong K, Thomas M, et al. Neural correlates of positive and negative symptoms through the illness course: an fMRI study in early psychosis and chronic schizophrenia. Sci Rep. 2019;2019(9):14444. https://doi.org/10.1038/s41598-019-51023-0.
Matsusaki A, Kaneko M, Narukawa M. Meta-analysis of dropout rates in placebo-controlled randomized clinical trials of atypical antipsychotics assessed by PANSS. Clin Drug Investig. 2019;39:917–26. https://doi.org/10.1007/s40261-019-00813-5.
Nicotra E, Casu G, Piras S, Marchese G. Schizophrenia on the use of the Positive and Negative Syndrome Scale in randomized clinical trials. Schizophr Res. 2015;165:181–7. https://doi.org/10.1016/j.schres.2015.04.006.
Koblan KS, Kent J, Hopkins SC, Krystal JH, Cheng Goldman HR, Loebel A. A non-D2-receptor-binding drug for the treatment of schizophrenia. Engl J Med. 2020;382:1497–506. https://doi.org/10.1056/NEJMoa1911772.
Barlati S, Stefana A, Bartoli F, Bianconi G, Bulgari V, Candini V, et al. Violence risk and mental disorders (VIORMED-2): a prospective multicenter study in Italy. PLoS ONE. 2019;14(4):e0214924. https://doi.org/10.1371/journal.pone.0214924.
de Girolamo G, Buizza C, Sisti D, Ferrari C, Bulgari V, Iozzino L, et al. Monitoring and predicting the risk of violence in residential facilities. No difference between patients with history or with no history of violence. J Psychiatr Res. 2016;80:5–13. https://doi.org/10.1016/j.jpsychires.2016.05.010.
di Giacomo E, Stefana A, Candini V, Bianconi G, Canal L, Clerici M, et al. Prescribing patterns of psychotropic drugs and risk of violent behavior a prospective multicenter study in Italy. Int J Neuropsychopharmacol. 2020;23(5):300–10. https://doi.org/10.1093/ijnp/pyaa005.
Fountoulakis KN, Dragioti E, Theoflidis AT, Wikilund T, Atmatzidis X, Nimatoudis I, et al. Staging of schizophrenia with the use of PANSS: an international multi-center study. Int J Neuropsychopharmacol. 2019;22(11):681–97. https://doi.org/10.1093/ijnp/pyz053.
Zhao C, Zhu J, Liu X, Pu C, Lai Y, Chen L, et al. Structural and functional brain abnormalities in schizophrenia: a cross-sectional study at different stages of the disease. Prog Neuropsychopharmacol Biol Psychiatry. 2018;83:27–32. https://doi.org/10.1016/j.pnpbp.2017.12.017.
Fazel S, Seewald K. Severe mental illness in 33,588 prisoners worldwide: systematic review and meta-regression analysis. Br J Psychiatry. 2012;200(5):364–73. https://doi.org/10.1192/bjp.bp.111.096370.
Coid J, Yang M, Roberts A, Ullrich S, Moran P, Bebbington P, et al. Violence and psychiatric morbidity in a national household population—a report from the British Household Survey. Am J Epidemiol. 2006;164(12):1199–208. https://doi.org/10.1093/aje/kwj339.
Davoren M, Kallis C, González RA, Freestone M, Coid J. Anxiety disorders and intimate partner violence: can the association be explained by coexisting conditions or borderline personality traits? J Forens Psychiatry Psychol. 2017;28(5):639–58. https://doi.org/10.1080/14789949.2016.1172659.
Swanson J, Estroff S, Swartz M, Borum R, Lachicotte W, Zimmer C, et al. Violence and severe mental disorder in clinical and community populations: the effects of psychotic symptoms, comorbidity, and lack of treatment. Psychiatry. 1997;60(1):1–22. https://doi.org/10.1080/00332747.1997.11024781.
McGorry PD, Yung AR, Phillips LJ. The “close-in” or ultra high-risk model: a safe and effective strategy for research and clinical intervention in prepsychotic mental disorder. Schizophr Bull. 2003;29:771–90. https://doi.org/10.1093/oxfordjournals.schbul.a007046.
Yung AR, Nelson B, Stanford C, Simmons MB, Cosgrave EM, Killackey E, et al. Validation of “prodromal” criteria to detect individuals at ultra high risk of psychosis: 2 year follow-up. Schizophr Res. 2008;105:10–7. https://doi.org/10.1016/j.schres.2008.07.012.
Flynn D, Smith D, Quirke L, Monks S, Kennedy HG. Ultra high risk of psychosis on committal to a young offender prison: an unrecognised opportunity for early intervention. BMC Psychiatry. 2012. https://doi.org/10.1186/1471-244X-12-100.
Allott K, Wood SJ, Yuen HP, Yung AR, Nelson B, Brewer WJ, et al. Longitudinal cognitive performance in individuals at ultrahigh risk for psychosis: a 10-year follow-up. Schizophr Bull. 2019;45:1101–11. https://doi.org/10.1093/schbul/sby143.
McGorry PD, Hartmann JA, Spooner R, Nelson B. Beyond the “at risk mental state” concept: transitioning to transdiagnostic psychiatry. World Psychiatry. 2018;17:133–42. https://doi.org/10.1002/wps.20514.
Bhui K, Ullrich S, Coid JW. Which pathways to psychiatric care lead to earlier treatment and a shorter duration of first-episode psychosis? BMC Psychiatry. 2014. https://doi.org/10.1186/1471-244X-14-72.
Bhui K, Ullrich S, Kallis C, Coid JW. Criminal justice pathways to psychiatric care for psychosis. Br J Psychiatry. 2015;207:523–9. https://doi.org/10.1192/bjp.bp.114.153882.
Müller-Isberner R, Webster CD, Gretenkord L. Measuring progress in hospital order treatment: relationship between levels of security and C and R scores of the HCR-20. Int J Forensic Ment Health. 2007;6:113–21. https://doi.org/10.1080/14999013.2007.10471256.
Abidin Z, Davoren M, Naughton L, Gibbons O, Nulty A, Kennedy HG. Susceptibility (risk and protective) factors for in-patient, violence and self-harm: prospective study of structured professional judgement instruments START and SAPROF, DUNDRUM-3 and DUNDRUM-4 in forensic mental health services. BMC Psychiatry. 2013. https://doi.org/10.1186/1471-244X-13-197.
Kennedy HG, O’Reilly K, Davoren M, O’Flynn P, O’Sullivan OP. How to measure progress in forensic care. In: Völlm B, Braun P, editors. Long-term forensic psychiatric care. Cham: Springer; 2019.
Donnelly V, Lynch A, Devlin C, Naughten L, Gibbons O, Mohan D, et al. Therapeutic alliance in forensic mental health: coercion, consent and recovery. Ir J Psychol Med. 2011;28:21–8. https://doi.org/10.1017/S0790966700011861.
Coid JW, Kallis C, Doyle M, Shaw J, Ullrich S. Identifying causal risk factors for violence among discharged patients. PLoS ONE. 2015;10:e0142493. https://doi.org/10.1371/journal.pone.0142493.
O’Reilly K, O’Connell P, Corvin A, O’Sullivan D, Coyle C, Mullaney R, et al. Moral cognition and homicide amongst forensic patients with schizophrenia and schizoaffective disorder: a cross-sectional cohort study. Schizophr Res. 2018;193:468–9. https://doi.org/10.1016/j.schres.2017.07.026.
Dack C, Ross J, Papadopoulos C, Stewart D, Bowers L. A review and meta-analysis of the patient factors associated with psychiatric in-patient aggression. Acta Psychiatr Scand. 2013;127(4):255–68. https://doi.org/10.1111/acps.12053.
Iozzino L, Ferrari C, Large M, Nielssen O, de Girolamo G. Prevalence and risk factors of violence by psychiatric acute inpatients: a systematic review and meta-analysis. PLoS ONE. 2015;10(6):e0128536. https://doi.org/10.1371/journal.pone.0128536.
O’Reilly K, O’Connell P, O’Sullivan D, Corvin A, Sheerin J, O’Flynn P, et al. Moral cognition, the missing link between psychotic symptoms and acts of violence: a cross-sectional national forensic cohort study. BMC Psychiatry. 2019. https://doi.org/10.1186/s12888-019-2372-4.
Andrews DAB. The Psychology of Criminal Conduct. 5th ed. Cincinnati: Anderson Publishing Company; 2010.
Acknowledgements
The authors acknowledge the valuable collaboration of Katharina Nymo Engelstad, Anja Vaskinn, Bjørn Rishovd Rund, Vasic Nenad, Streb Judith, and Dudeck Manuela for providing us adjunctive PANSS ratings not contained in the published articles.
Funding
This study was funded by the EUropean Study on VIOlence Risk and MEntal Disorders (EU-VIORMED) project has received a grant from European Commission (Grant Number PP-2-3-2016, November 2017–October 2020) and is registered on the Research Registry—https://www.researchregistry.com/—Unique Identifying Number 4604. In Italy this study has also been supported by 5 × 1000 (year 2017) funds and Ricerca Corrente funds from the Italian Ministry of Health. The funding source had no role in the design and in the conduct of the study, and will not have any role in data analyses, in the interpretation of results, and in the writing of the study reports.
Author information
Authors and Affiliations
Contributions
CB, VC, and GS contributed to conceptualization, methodology, data curation, original draft, and writing––review & editing. CS was involved in methodology, data curation, formal analysis, original draft, and writing––review & editing. GdG contributed to funding acquisition, conceptualization, original draft, and writing––review & editing. CF and AM were involved in methodology, formal analysis, supervision, original draft, and writing––review & editing. LI contributed to conceptualization, original draft, and writing––review & editing. HK was involved in methodology, supervision, original draft, and writing––review & editing. All the author have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Methodological quality assessment and risk of bias
Additional file 2: Table S1.
Cochrane quality assessment tool.
Additional file 3: Table S2.
NOS Scale for cohort and case-control studies.
Additional file 4: Table S3.
NOS Scale for cross-sectional studies.
Additional file 5: Table S4.
Comparison between PANSS total rating and CGI. ratings, and clinical meaning.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Buizza, C., Strozza, C., Sbravati, G. et al. Positive and negative syndrome scale in forensic patients with schizophrenia spectrum disorders: a systematic review and meta-analysis. Ann Gen Psychiatry 21, 36 (2022). https://doi.org/10.1186/s12991-022-00413-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12991-022-00413-2