
Abstract
Background
Exoskeleton-assisted walking (EAW) is expected to improve the gait of spinal cord injury (SCI) individuals. However, few studies reported the changes of pulmonary function (PF) parameters after EAW trainings. Hence, we aimed to explore the effect of EAW on PF parameters, 6-min walk test (6MWT) and lower extremity motor score (LEMS) in individuals with SCI and to compare those with conventional trainings.
Methods
In this prospective, single-center, single-blinded randomized controlled pilot study, 18 SCI participants were randomized into the EAW group (n = 9) and conventional group (n = 9) and received 16 sessions of 50–60 min training (4 days/week, 4 weeks). Pulmonary function parameters consisting of the forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), forced expiratory flow (FEF), peak expiratory flow, and maximal voluntary ventilation, 6MWT with assisted devices and LEMS were reported pre- and post-training.
Results
Values of FVC (p = 0.041), predicted FVC% (p = 0.012) and FEV1 (p = 0.013) were significantly greater in EAW group (FVC: 3.8 ± 1.1 L; FVC% pred = 94.1 ± 24.5%; FEV1: 3.5 ± 1.0 L) compared with conventional group (FVC: 2.8 ± 0.8 L; FVC% pred = 65.4 ± 17.6%; FEV1: 2.4 ± 0.6 L) after training. Participants in EAW group completed 6MWT with median 17.3 m while wearing the exoskeleton. There was no difference in LEMS and no adverse event.
Conclusions
The current results suggest that EAW has potential benefits to facilitate PF parameters among individuals with lower thoracic neurological level of SCI compared with conventional trainings. Additionally, robotic exoskeleton helped walking. Trial registration: Registered on 22 May 2020 at Chinese Clinical Trial Registry (ChiCTR2000033166). http://www.chictr.org.cn/edit.aspx?pid=53920&htm=4.
Similar content being viewed by others


Background
Spinal cord injury (SCI) is a worldwide life-disrupting pathological condition with estimated 17,810 injuries occurred in the United States in 2017 [1, 2], and 3.5 per million in the United Kingdom each year [3]. Respiratory complications are common after SCI that account for 5.4% of the causes of death [4] and have a great impact on reducing quality of life and life expectancy. On the other hand, pulmonary capacity may have implications for exercise performance because oxygen is essential for organ system metabolism [5]. Hence, a good pulmonary function (PF) is of vital importance for individuals with SCI.
Pulmonary function parameters are affected by the paralyzed degree (complete or partial) of the respiratory muscles [6] which consist of diaphragm, intercostal muscles, accessory respiratory muscles, and abdominal muscles. Moreover, PF parameters are associated with the level of damaged spinal cord [7, 8]. Therefore, doctors and therapists concerned more about the PF among higher injury level individuals. Specific trainings, such as respiratory muscle training [9] and abdominal drawing-in maneuver [10] are frequently used for them. Unfortunately, SCI individuals with lower injury level also complained about the bad results of pulmonary function test (PFT) [11]. Walking and running are key elements of an aerobic exercise program. Additionally, they are useful to keep pulmonary and exercise capacity [12, 13]. However, the paralysis of lower limb and osteoporosis after SCI would make individuals difficult to walk or run. Instead, upper limb aerobic exercise [14], strength training [15], and balance training [16,17,18] are common exercises to maintain exercise capacity for these individuals. Nonetheless, previous study reported that these were hard to improve the resting lung function or exercise performance [19]. Hence, individuals assessed as lower extremity motor complete lesions need assisted devices to complete walking and that may result in improvement in the pulmonary and exercise capacity.
Recently, exoskeleton-assisted walking (EAW) has been confirmed to help individuals with thoracic and lumbar SCI to walk safely [20,21,22]. Despite the potential walking benefits of EAW, there are few studies manifested that used EAW trainings for PF improving. A quantity of studies has manifested the improvements of metabolic responses, such as heart rate and VO2 max [23,24,25] during the training program. Nevertheless, none of them has focused on the changes of PF parameters by PFT which contained the vital capacity, forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), forced expiratory flow (FEF25/50/75), peak expiratory flow (PEF), and maximal voluntary ventilation (MVV). Besides this, previous trials were non-randomized controlled trials. Therefore, this randomized controlled study primarily aimed at finding out whether the EAW trainings are different from conventional rehabilitation trainings in improving PF parameters among SCI individuals. Our hypotheses were that EAW training can improve the PF parameters and maintain the lower extremity motor score (LEMS) which does not make a difference relative to that made by conventional training. Second, individuals could complete walking while wearing the exoskeleton. To our knowledge, this is the first clinical trial to concern about the PF parameters by EAW training.
Methods
Study design and ethics statement
This was a single-blinded, randomized controlled efficacy trial with 2 parallel groups and intention-to-treat analysis. The study protocol has been registered at Chinese Clinical Trial Registry (ChiCTR2000033166) and approved by the medical ethics committee of West China Hospital of Sichuan University (#19-667). All patients were informed of the procedure, the use of their data and images for research. They understood the purposes and provided written informed consent according to the 1964 Declaration of Helsinki prior to their participation.
Participant recruitment
From May 2020 to August 2020, we prospectively enrolled all adult individuals with a diagnosed SCI below T3 and above L2 at least 1 month. Participants were recruited from inpatients in 3 units of Rehabilitation center, West China Hospital, Sichuan University. None of them had EAW training experience before. In addition, the eligible individuals met the following inclusion criteria: (1) American spinal injuries association impairment scale [26] (ASIA) classified with A, B or C, (2) the height was between 1.50 m and 1.85 m and (3) stopped smoking for over 6 months. Individuals were excluded if: (1) spasticity of any the lower extremity muscle scored over 2 according to the Modified Ashworth Scale [27], (2) with unstable fracture, (3) diagnosed with severe osteoporosis (bone mineral density t-score < − 3.5), (4) with any respiratory or other neurological diseases.
Randomization and blinding
The individuals were randomly divided into the EAW group or conventional group in a 1:1 ratio by simple randomization method, using computer-generated simple random tables. The sequences were preserved using closed envelop method by one researcher who did not participant in the trainings and assessments (H.C.H). PFT and LEMS assessment of individuals pre- and post-training were performed by the same two clinical researchers (X.Y. and Y.O) who were blinded and did not know whether the individual was in EAW or conventional group. 6MWT was performed by two researchers who participated in EAW training (H.C and C.P.D) and conventional training (H.Y.Z). Clinical data was recorded after averaging.
Interventions
The AIDER (AssItive DEvice for paRalyzed patient) powered robotic exoskeleton (generation IV, Buffalo Robot Technology Co. Ltd, Chengdu, China) was used for the EAW training. All subjects were individually fitted to the robotic exoskeleton according to pelvic width, thigh length, and shank length. Exoskeleton-assisted walking training program was conducted consecutive 4 days a week, 16 training sessions in total. Every training session lasted 50–60 min containing interval rest as needed by standing, leaning on the wall, or sitting while wearing the device. Training session included sitting, standing, walking, climbing stairs and slope with maximal assistance-walking mode (Fig. 1) and reaching 40–60% maximal heart rate (HR, HRmax = 220—age)[28] that is checked with the values of a heart rate sensor (Polar H10, POLAR® China).

AIDER powered exoskeleton illustration used in this study. A Walk in exoskeleton; B go upstairs in exoskeleton; C go downstairs in exoskeleton
For the conventional group, the rehabilitation program included strength training using dumbbell between 5 and 20 kg, aerobic exercise, such as walking training with brace as well as static and dynamic balance training in sitting or standing position. The conventional rehabilitation training had the same intensity, duration, and frequency as EAW training (40–60% HRmax, 50–60 min/session, 4 days/week, 4 weeks). Medications and rehabilitation nursing were ordered based on the medical condition.
Measures
Outcome measures were collected and analyzed at the baseline and end of 16-session intervention period.
Primary outcome
Pulmonary function test was completed with a computerized spirometer (Vyntus™ SPIRO PC Spirometer, Vyaire Medical Inc., Mettawa, US) based onthe standardized procedures as the American Thoracic Society [29] described. To determine PF parameters, participants performed PFT seating in the wheelchair and were forbidden to disclose their intervention assignment to the assessor. The PFT was performed with the participants wearing a nose clip. If the participant coughed or made a mistake, the numerical values were not recorded. Three repeated maneuvers were performed, separated by a five-minute rest and the best result was recorded automatically. The PFT consisted of the assessments of FVC, FEV1, FEF25/50/75, PEF, and MVV.
Forced vital capacity refers to the total capacity of air that can be blown out by maxima forced expiration following maximal inspiration. Forced expiratory volume in 1 s refers to the capacity of air that is blown out for a single second. Force expiratory flow25/50/75 means forced expiratory flow at 25, 50 and 75% of the FVC. Peak expiratory flow reflects the intensity of respiratory muscles. Maximal voluntary ventilation refers to the maximum volume of air, a subject can breathe over a specified period [30].
Secondary outcomes
The 6MWT (6-min walk test) was performed in door that is aimed to determine walking ability. Additionally, it can manifest cardiorespiratory endurance through evaluating the walking distance in accordance with the guidelines of the American Thoracic Society [31]. At the beginning and end of the test, clinical researchers recorded the participant’s HR, and peripheral oxygen saturation (SpO2). In additional, the level of effort at the end of the test was reported by the rate of perceived exertion (RPE) based on the Borg scale [32]. Participants ambulated using their preferred stability aid (either crutches or walker). Individuals in EAW group were allowed to wear the exoskeleton, while those in conventional group using the knee-ankle–foot orthoses if they had one. The outcome of distance will be recorded as 0 and others be recorded according to the facts, if the individuals cannot walk. Moreover, lower extremity motor score [33] and ASIA scores were reported to demonstrate the recovery of muscle strength and neurological level.
Data analysis
The statisticians (X.N.X and J.D) were blinded to the program and completed analyses utilized SPSS version 25 (SPSS Inc, Chicago, Illinois). The Shapiro–Wilk test was used to determine if data were normally distributed. These were recorded as means ± standard deviations (SDs), others were described as median and inter quartile range (IQR) where necessary. The mean values (Δ) of post-intervention minus pre-intervention were recorded. Independent Student t-test was used to compare continuous data related to clinical features between two groups. Paired Test Student t-test was used to compare varies between pre- and post-intervention. Furthermore, the Fisher’s exact and Pearson’s Chi-square tests were used if the data were categorical variables. Wilcoxon rank-sum test and Mann–Whitney U test were used if the data was not normally distributed. Pearson correlation test was performed to discuss the relation between the distance of 6MWT and changes of PF parameters. In all statistical tests, p < 0.05 was defined as significant.
Results
Participants
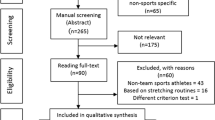
A total of 87 individuals with SCI were screened enrollment, of which 69 were excluded as per exclusion criteria (n = 61) or declining to commit the full participation (n = 8). Eighteen eligible individuals were randomized to either EAW group (n = 9) or conventional group (n = 9). The Consolidated Standards of Reporting Trials (CONSORT) diagram is showed in Fig. 2. Of the 9 individuals randomized to the EAW group, 8 have completed the EAW intervention training sessions but one individual refused to continue participating after experiencing severe anxiety episodes in the robotic exoskeleton. In the conventional group, one individual did not accept the final assessment because of own desire to be discharged from hospital. Two groups were comparable on the baseline characteristics (Table 1). At the end point of the final training session, rehabilitation evaluation and assessments were performed and no change in level and classification of neurological injury were detected.

CONSORT diagram of enrollment of participants into the study
Adverse events
There were no adverse events related to treatment in either group.
Primary outcome
The primary outcome was measured based on PFT. Detail numerical results of PFT are provided in Table 2. The results of FVC (t = 2.224; p = 0.041) and predicted FVC% (t = 2.848, p = 0.012) showed significant differences between EAW group and conventional group. Moreover, there was statistically significant difference in FEV1 (t = 2.779; p = 0.013) between groups. Nevertheless, there were no statistically significant differences in FEF75 (t = 0.803; p = 0.434), FEF50 (Z = 0.927; p = 0.354), FEF25 (t = 0.834; p = 0.417), PEF (t = 1.097; p = 0.289), and MVV (t = 0.935; p = 0.364) (Fig. 3).

Comparisons of the improvements in pulmonary function test (PFT) between two groups. A Results of FVC, FEV1, FEF75, FEF25, and PEF; B result of MVV; C result of FEF50. PFT pulmonary function test, *p < 0.05, EAW exoskeleton-assisted walking group, FVC forced vital capacity, FEV1 forced expiratory volume in 1 s, FEF forced expiratory flow, PEF peak expiratory flow, MVV maximal voluntary ventilation
Participants who treated with EAW training had statistical improvements from pre- to post-intervention in mean change in predicted FVC% (Δ = 17.2%; t = 2.445; p = 0.040), FEV1 (Δ = 0.8 L; t = 3.359; p = 0.010), FEF75 (Δ = 1.7 L/s; t = 3.268; p = 0.011), PEF (Δ = 1.8 L/s; t = 3.381; p = 0.010), and MVV (Δ = 19.3 L; t = 3.274; p = 0.017). Howbeit, there was no statistically significant differences in FVC (Δ = 0.7 L; t = 2.275; p = 0.052), FEF50 (Δ = 0.6 L/s; t = 1.917; p = 0.092), and FEF25 (Δ = 0.2 L/s; t = 0.575; p = 0.581). Nonetheless, there was no evidence of statistical improvements from pre- to post-intervention for individuals who received conventional training in FVC (Δ = − 0.2 L; t = − 1.146; p = 0.285), predicted FVC% (Δ = − 4.1% L; t = − 1.057; p = 0.321), FEV1 (Δ = − 0.1 L; t = − 0.544; p = 0.601), FEF75 (Δ = 1.0 L/s; t = 1.865; p = 0.099), FEF50 (Z = − 0.70; p = 0.944), FEF25 (Δ = − 0.2 L/s; t = − 0.758; p = 0.470), PEF (Δ = 0.9 L/s; t = 1.383; p = 0.204), and MVV (Δ = 7.3 L; t = 1.364; p = 0.204).
Secondary outcomes
Of the 10 participants who completed the final 6MWT, 2 were in the conventional group. All participants in EAW group completed it while wearing the exoskeleton in door. A summary of secondary outcomes is provided in Table 3. The outcomes of distance recording as medians (IQR) were 17.3 (11.9) meters and 0 (16.0) meter for EAW and conventional group, respectively. Nonetheless, EAW training produced no statistical improvements in distance (Z = 1.756; p = 0.079) and SpO2 (− 2%; t = 2.032; p = 0.059) than conventional group. There were differences in HR (Z = 2.311; p = 0.021), and RPE (Z = 2.330; t = 0.020) between groups. Moreover, participants who treated with EAW training had differences from pre- to post- intervention in HR (Δ = 20.2; t = 4.293; p = 0.003), and PRE (Z = 2.558; p = 0.011). Howbeit, distance (Z = 1.400; p = 0.161) and SpO2 (Δ = 3.8%; t = − 1.474; p = 0.179) showed no differences. For conventional group, no statistical differences were reported for distance (Z = 1.342; t = 0.180), HR (Z = 0.351 = 0.725), SpO2 (Δ = 1.7%; t = 2.236; p = 0.056) and RPE (Z = 0.447; p = 0.655). The outcomes of correlation between the distance of 6MWT and evert item of PFT are shown in Additional file 1: Appendix 1. The distance showed a significant positive correlation with FEV1 (Pearson correlation coefficient 0.741, p = 0.022) and FEF75 (Pearson correlation coefficient 0.688, p = 0.040).
For LEMS, there was no statistical difference between two groups (Z = 0.283; p = 0.777). Additionally, neither groups showed improvement in LEMS (Z = 1.342; p = 0.180 in EAW group; Z = 1.826; p = 0.068 in conventional group). More detailed data are provided in Additional file 2.
Discussion
This study focused on the changes of PFT and 6MWT using EAW and conventional trainings in individuals with T4 to L1 SCI. Robotic exoskeleton has been explored and applied in rehabilitation treatment after SCI. At present, the robotic exoskeleton has demonstrated some advantages in assisting walking and improving physical functions [34, 35]. We found that EAW trainings provided statistically significant improvement in FVC, predicted FVC% and FEV1 compared with conventional trainings. Nonetheless, there were no differences in FEF, PEF, and MVV between two groups. Moreover, EAW trainings offered statistically different results of PFT than the beginning, except FVC, FEF50 and FEF25.
Exoskeleton-assisted walking training enhanced the pulmonary function parameters among individuals with spinal cord injury
Some previous studies [23,24,25, 35] have shown that robotic exoskeletons provide improvement in VO2 peak among the incomplete SCI individuals during gait training. We reported changes in PF parameters among complete and incomplete SCI individuals. In the present study, it was reported better results in FVC, predicted FVC% and FEV1 compared with the conventional trainings that were widely used in SCI rehabilitation program. There were statistical differences in post-predicted FVC%, FEV1, FEF75, PEF and MVV after EAW compared with pre-outcomes. The improvements in PF parameters might reflect the increasing of respiratory muscle strength and pulmonary ventilation. Alamro et al. [36] has demonstrated that overground walking by exoskeleton elicits greater activation of trunk muscles compared with treadmill walking, even after controlling for the use of hand-held assistive devices. Moreover, Guan et al. [37] also reported EAW had advantages over conventional gait orthosis on recruiting muscles. Hence, the underlying mechanisms of how EAW improved the PF parameters might be the potential to recruit trunk muscles. The improvements of trunk muscles in SCI individuals resulted in better pulmonary function [38, 39].
The increasing or maintenance of PF parameters has crucial meanings for many patients with SCI. Hart et al. [40] has reported that lower FEV1 and FVC associate with higher inflammatory factors that reflect systemic inflammation. Hence, better results of FEV1 and FVC are beneficial to reduce systemic inflammation and manifested better functions of principal bronchus. Although there was no difference in pre- and post- FVC in 2 groups, we reported a higher mean value after EAW training. At least, both trainings helped to maintain the FVC, and EAW might improve the FVC. Moreover, the minimal clinically important difference for predicted FVC% is 2–6% by distribution-based method [41]. The mean changes of difference between groups and from pre- to post-intervention in EAW group were beyond the threshold which were 28.7% and 17.2%, respectively. Additionally, the minimal important difference of FEV1 is 0.1 L according to previous study by the anchor-based method [42], which is smaller than our results (1.1 L between groups; 0.8 L in EAW group). Therefore, EAW training has potential benefits of both clinical and statistical meanings for PF parameters.
As for the conventional trainings which are recommended and wildly used for many years [43,44,45], this study only demonstrated the capability to keep PFT among individuals with SCI. Nevertheless, the changes could be secondary to natural recovery since all participants in conventional group were in acute stage. In spite of that, the differences between groups still proved the advantages of EAW. Nonetheless, Akkurt et al. [46] reported that upper extremity aerobic exercise aimed at 50–70% VO2 max improves exercise capacity among individuals with C7 to L5 SCI. In this study, the HR values during the trainings reached a moderate-intensity level based on the ACSM guidelines for exercise testing and prescription [47]. The inconsistent results may be caused by different intensities and ranges of included injury level.
Robotic exoskeleton improved walking ability
Robotic exoskeleton was achievable to enhance the walking capacity. Furthermore, no improvement in LEMS also manifested that EAW effect on walking capacity, not no motor function or lower limb muscle performance. Our result of 6MWT was similar to McIntosh et al. [48] and Sale et al. [49]. All participants were able to perform walking while wearing the exoskeleton. Nevertheless, only two participants in conventional group had knee-ankle–foot orthoses and completed the 6MWT. Others were limited to the access of brace in this study.
For individuals with SCI, the results of 6MWT might not report the cardiopulmonary endurance completely. In this study, the distance was partially related to PFT. There was no statistically significant collection between the distance and most item of PFT. This might be influenced by the primary disease, different assisted devices and the using duration. Longer using duration may result in longer distance. Benson et al. [50] found the minimal distance of 6MWT after 10-week trainings was 91 m which was more than 5 times than our average distance. Additionally, we found that individuals with lower injury level (T11–L1) had better improvements (17.7 ± 4.3 m) than others (14.3 ± 7.7 m) in distance which did not provide statistical difference (p = 0.481). This was partly confirmed by Louie et al. [51] and Guanziroli et al. [52] who reported walking speed and performances were significantly associated with injury level. Additionally, we did not report any adverse event, even more than half of the individuals in EAW group was acute inpatient.
Study limitations
This study was limited to the small sample size and number of training session, although our feasibility study has proved this training period realized the application of EAW and was most achievable in inpatient rehabilitation in the health care system. The results in this study may not be generalized to larger population. It is necessary to explore the sample size and future investigation on the effectiveness of EAW. Although we tried to avoid the detection bias, it was inevitable during the 6MWT. A majority of subjects from the EAW group was AIS A level that may influence the results of 6MWT, although there was no difference of LEMS at the baseline. Moreover, further study needs to have control groups composed of healthy participants with EAW training or conventional training, and compare with individuals with SCI.
Furthermore, the intensity calculated by the HR was rough and imprecise in some degree. The predict HRmax by the formula: HRmax = 220—age might be inaccurate. HRmax is individual and related to sex and physical activity status [53]. In this study, the range of age is 40 and the used equation underestimates the HRmax in older adults [28]. Moreover, the validity of equation has not been established in a study sample that included an adequate number of individuals with SCI. This might have resulted in misestimation of the training intensity, which in turn, result in comparison of PFT. Hence, cardiopulmonary exercise test is needed possibly for accurate cardiopulmonary performance parameters. Last, gait parameters should be recorded and compared while walking without the exoskeleton for participants who had the capacity for walking.
Conclusions
The study successfully manifested that EAW training has the potential to improve performance in PF parameters among individuals with SCI, especially in ventilation. Additionally, robotic exoskeleton is a device that can assist individuals with SCI to stand up and walk. The results suggested that the effectiveness of EAW might be similar, or better than conventional training. Further research is essential to confirm these results in a larger sample size and better study protocols. The data in this study will be helpful for further efforts towards improving the design and clinical application of EAW.
Availability of data and materials
The dataset used in the study is available from the corresponding author on reasonable request.
Abbreviations
- SCI:
-
Spinal cord injury
- PF:
-
Pulmonary function
- EAW:
-
Exoskeleton-assisted walking
- FVC:
-
Forced vital capacity
- FEV1 :
-
Forced expiratory volume in 1 s
- MVV:
-
Maximal voluntary ventilation
- ASIA:
-
American spinal injuries association impairment scale
- AIDER:
-
AssItive DEvice for paRalyzed patient
- HR:
-
Heart rate
- PFT:
-
Pulmonary function test
- FEF:
-
Forced expiratory flow
- PEF:
-
Peak expiratory flow
- SpO2 :
-
Peripheral oxygen saturation
- RPE:
-
Rate of perceived exertion
- 6MWT:
-
6-Minute walk test
- LEMS:
-
Lower extremity motor score
- CI:
-
Confidence intervals
- IQR:
-
Inter quartile range
References
Ge L, Arul K, Ikpeze T, Baldwin A, Nickels JL, Mesfin A. Traumatic and nontraumatic spinal cord injuries. World Neurosurg. 2018;111:e142–8.
Jain NB, Ayers GD, Peterson EN, Harris MB, Morse L, O’Connor KC, et al. Traumatic spinal cord injury in the United States, 1993–2012. JAMA. 2015;313(22):2236–43.
Bao FP, Zhang HG, Zhu SM. Anesthetic considerations for patients with acute cervical spinal cord injury. Neural Regen Res. 2017;12(3):499–504.
Garshick E, Kelley A, Cohen SA, Garrison A, Tun CG, Gagnon D, et al. A prospective assessment of mortality in chronic spinal cord injury. Spinal Cord. 2005;43(7):408–16.
Astorino TA, Bediamol N, Cotoia S, Ines K, Koeu N, Menard N, et al. Verification testing to confirm VO2max attainment in persons with spinal cord injury. J Spinal Cord Med. 2019;42(4):494–501.
van den Berg ME, Castellote JM, de Pedro-Cuesta J, Mahillo-Fernandez I. Survival after spinal cord injury: a systematic review. J Neurotrauma. 2010;27(8):1517–28.
Schilero GJ, Radulovic M, Wecht JM, Spungen AM, Bauman WA, Lesser M. A center;s experience: pulmonary function in spinal cord injury. Lung. 2014;192(3):339–46.
Bluechardt MH, Wiens M, Thomas SG, Plyley MJ. Repeated measurements of pulmonary function following spinal cord injury. Paraplegia. 1992;30(11):768–74.
Berlowitz DJ, Tamplin J. Respiratory muscle training for cervical spinal cord injury. Cochrane Database Syst Rev. 2013;(7):CD008507.
Kim CY, Lee JS, Kim HD, Lee DJ. Short-term effects of respiratory muscle training combined with the abdominal drawing-in maneuver on the decreased pulmonary function of individuals with chronic spinal cord injury: a pilot randomized controlled trial. J Spinal Cord Med. 2017;40(1):17–25.
Malas FÜ, Köseoğlu F, Kara M, Ece H, Aytekin M, Öztürk GT, et al. Diaphragm ultrasonography and pulmonary function tests in patients with spinal cord injury. Spinal cord. 2019;57(8):679–83.
Bossers WJR, van der Woude LHV, Boersma F, Hortobágyi T, Scherder EJA, van Heuvelen MJG. A 9-week aerobic and strength training program improves cognitive and motor function in patients with dementia: a randomized, controlled trial. Am J Geriatr Psychiatry. 2015;23(11):1106–16.
Saunders DH, Sanderson M, Hayes S, Kilrane M, Greig CA, Brazzelli M, et al. Physical fitness training for stroke patients. Cochrane Database Syst Rev. 2016;3:CD003316.
Battikha M, Sa L, Porter A, Taylor JA. Relationship between pulmonary function and exercise capacity in individuals with spinal cord injury. Am J Phys Med Rehabil. 2014;93(5):413–21.
Lemos JR, da Cunha FA, Lopes AJ, Guimaraes FS, do Amaral Vasconcellos FV, Dos Santos Vigario P. Respiratory muscle training in non-athletes and athletes with spinal cord injury: a systematic review of the effects on pulmonary function, respiratory muscle strength and endurance, and cardiorespiratory fitness based on the FITT principle of exercise prescription. J Back Musculoskelet Rehabil. 2020;33(4):655–67.
Gaffurini P, Bissolotti L, Calza S, Calabretto C, Orizio C, Gobbo M. Energy metabolism during activity-promoting video games practice in subjects with spinal cord injury: evidences for health promotion. Eur J Phys Rehabil Med. 2013;49(1):23–9.
Neville BT, Murray D, Rosen KB, Bryson CA, Collins JP, Guccione AA. Effects of performance-based training on gait and balance in individuals with incomplete spinal cord injury. Arch Phys Med Rehabil. 2019;100(10):1888–93.
Liu H, Li J, Du L, Yang M, Yang D, Li J, et al. Short-term effects of core stability training on the balance and ambulation function of individuals with chronic spinal cord injury: a pilot randomized controlled trial. Minerva Med. 2019;110(3):216–23.
Fischer G, Tarperi C, George K, Ardigo LP. An exploratory study of respiratory muscle endurance training in high lesion level paraplegic handbike athletes. Clin J Sport Med. 2014;24(1):69–75.
Kozlowski AJ, Bryce TN, Dijkers MP. Time and effort required by persons with spinal cord injury to learn to use a powered exoskeleton for assisted walking. Top Spinal Cord Inj Rehabil. 2015;21(2):110–21.
Birch N, Graham J, Priestley T, Heywood C, Sakel M, Gall A, et al. Results of the first interim analysis of the RAPPER II trial in patients with spinal cord injury: ambulation and functional exercise programs in the REX powered walking aid. J Neuroeng Rehabil. 2017;14(1):60.
Xiang XN, Ding MF, Zong HY, Liu Y, Cheng H, He CQ, et al. The safety and feasibility of a new rehabilitation robotic exoskeleton for assisting individuals with lower extremity motor complete lesions following spinal cord injury (SCI): an observational study. Spinal Cord. 2020;58(7):787–94.
Evans N, Hartigan C, Kandilakis C, Pharo E, Clesson I. Acute cardiorespiratory and metabolic responses during exoskeleton-assisted walking overground among persons with chronic spinal cord injury. Top Spinal Cord Inj Rehabil. 2015;21(2):122–32.
Jang YC, Park HK, Han JY, Choi IS, Song MK. Cardiopulmonary function after robotic exoskeleton-assisted over-ground walking training of a patient with an incomplete spinal cord injury: case report. Medicine (Baltimore). 2019;98(50):e18286.
Escalona MJ, Brosseau R, Vermette M, Comtois AS, Duclos C, Aubertin-Leheudre M, et al. Cardiorespiratory demand and rate of perceived exertion during overground walking with a robotic exoskeleton in long-term manual wheelchair users with chronic spinal cord injury: a cross-sectional study. Ann Phys Rehabil Med. 2018;61(4):215–23.
Roberts TT, Leonard GR, Cepela DJ. Classifications in brief: American Spinal Injury Association (ASIA) impairment scale. Clin Orthop Relat Res. 2017;475(5):1499–504.
Meseguer-Henarejos AB, Sanchez-Meca J, Lopez-Pina JA, Carles-Hernandez R. Inter- and intra-rater reliability of the Modified Ashworth Scale: a systematic review and meta-analysis. Eur J Phys Rehabil Med. 2018;54(4):576–90.
Tanaka H, Monahan KD, Seals DR. Age-predicted maximal heart rate revisited. J Am Coll Cardiol. 2001;37(1):153–6.
Graham BL, Steenbruggen I, Miller MR, Barjaktarevic IZ, Cooper BG, Hall GL, et al. Standardization of spirometry 2019 update. An official American thoracic society and European respiratory society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70–88.
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–38.
ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–7.
Holmlund T, Ekblom-Bak E, Franzen E, Hultling C, Wahman K. Intensity of physical activity as a percentage of peak oxygen uptake, heart rate and Borg RPE in motor-complete para- and tetraplegia. PLoS ONE. 2019;14(12):e0222542.
Wilson JR, Jaja BNR, Kwon BK, Guest JD, Harrop JS, Aarabi B, et al. Natural history, predictors of outcome, and effects of treatment in thoracic spinal cord injury: a multi-center cohort study from the north american clinical trials network. J Neurotrauma. 2018;35(21):2554–60.
Cheung EYY, Ng TKW, Yu KKK, Kwan RLC, Cheing GLY. Robot-assisted training for people with spinal cord injury: a meta-analysis. Arch Phys Med Rehabil. 2017;98(11):2320–31.
Gorman PH, Scott W, VanHiel L, Tansey KE, Sweatman WM, Geigle PR. Comparison of peak oxygen consumption response to aquatic and robotic therapy in individuals with chronic motor incomplete spinal cord injury: a randomized controlled trial. Spinal Cord. 2019;57(6):471–81.
Alamro RA, Chisholm AE, Williams AMM, Carpenter MG, Lam T. Overground walking with a robotic exoskeleton elicits trunk muscle activity in people with high-thoracic motor-complete spinal cord injury. J Neuroeng Rehabil. 2018;15(1):109.
Guan X, Kuai S, Ji L, Wang R, Ji R. Trunk muscle activity patterns and motion patterns of patients with motor complete spinal cord injury at T8 and T10 walking with different un-powered exoskeletons. J Spinal Cord Med. 2017;40(4):463–70.
Triolo RJ, Boggs L, Miller ME, Nemunaitis G, Nagy J, Bailey SN. Implanted electrical stimulation of the trunk for seated postural stability and function after cervical spinal cord injury: a single case study. Arch Phys Med Rehabil. 2009;90(2):340–7.
Hart N, Laffont I, de la Sota AP, Lejaille M, Macadou G, Polkey MI, et al. Respiratory effects of combined truncal and abdominal support in patients with spinal cord injury. Arch Phys Med Rehabil. 2005;86(7):1447–51.
Hart JE, Goldstein R, Walia P, Teylan M, Lazzari A, Tun CG, et al. FEV1 and FVC and systemic inflammation in a spinal cord injury cohort. BMC Pulm Med. 2017;17(1):113.
du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov A, et al. Forced vital capacity in patients with idiopathic pulmonary fibrosis: test properties and minimal clinically important difference. Am J Respir Crit Care Med. 2011;184(12):1382–9.
Gompelmann D, Kontogianni K, Schuhmann M, Eberhardt R, Heussel CP, Herth FJ. The minimal important difference for target lobe volume reduction after endoscopic valve therapy. Int J Chron Obstruct Pulmon Dis. 2018;13:465–72.
Tweedy SM, Beckman EM, Geraghty TJ, Theisen D, Perret C, Harvey LA, et al. Exercise and sports science Australia (ESSA) position statement on exercise and spinal cord injury. J Sci Med Sport. 2017;20(2):108–15.
Bye EA, Harvey LA, Gambhir A, Kataria C, Glinsky JV, Bowden JL, et al. Strength training for partially paralysed muscles in people with recent spinal cord injury: a within-participant randomised controlled trial. Spinal Cord. 2017;55(5):460–5.
Tse CM, Chisholm AE, Lam T, Eng JJ, Team SR. A systematic review of the effectiveness of task-specific rehabilitation interventions for improving independent sitting and standing function in spinal cord injury. J Spinal Cord Med. 2018;41(3):254–66.
Akkurt H, Karapolat HU, Kirazli Y, Kose T. The effects of upper extremity aerobic exercise in patients with spinal cord injury: a randomized controlled study. Eur J Phys Rehabil Med. 2017;53(2):219–27.
Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, American College of Sports Medicine position stand, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334–59.
McIntosh K, Charbonneau R, Bensaada Y, Bhatiya U, Ho C. The safety and feasibility of exoskeletal-assisted walking in acute rehabilitation after spinal cord injury. Arch Phys Med Rehabil. 2020;101(1):113–20.
Sale P, Russo EF, Scarton A, Calabro RS, Masiero S, Filoni S. Training for mobility with exoskeleton robot in spinal cord injury patients: a pilot study. Eur J Phys Rehabil Med. 2018;54(5):745–51.
Benson I, Hart K, Tussler D, van Middendorp JJ. Lower-limb exoskeletons for individuals with chronic spinal cord injury: findings from a feasibility study. Clin Rehabil. 2016;30(1):73–84.
Louie DR, Eng JJ, Lam T, Spinal Cord Injury Research Evidence Research T. Gait speed using powered robotic exoskeletons after spinal cord injury: a systematic review and correlational study. J Neuroeng Rehabil. 2015;12:82.
Guanziroli E, Cazzaniga M, Colombo L, Basilico S, Legnani G, Molteni F. Assistive powered exoskeleton for complete spinal cord injury: correlations between walking ability and exoskeleton control. Eur J Phys Rehabil Med. 2019;55(2):209–16.
Roy SMJ. Validation of maximal heart rate prediction equations based on sex and physical activity status. Int J Exerc Sci. 2015;8(4):318–30.
Acknowledgements
The authors are grateful for the assistance from Professor Jing Qiu, Professor Quan Wei and Doctor Ming-Fu Ding during data collection. Additionally, we also thank Dr. Jie Deng for data analysis.
Funding
This research study was supported by the National Key R&D Program of China (2017YFB1302305).
Author information
Authors and Affiliations
Contributions
X-NX: PT. Xiang analyzed the clinical data and drafted the initial manuscript. H-YZ: PT. Zong provided conventional intervention services. XY: Dr.Yu was an outcome assessor. YO: PT. Ou was an outcome assessor. HC: Prof. Cheng provided EAW intervention services. C-PD: Prof. Du participated in study design and provided EAW intervention services. H-CH: Prof. He participated in study design, supervised case enrollment, and approved the final manuscript as submitted. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study received approval from the Ethics Committee of West China Hospital of Sichuan University and there was no deviation from the original protocol. This study protocol is registered at the Chinese Clinical Trial Registry with the following identifier: ChiCTR2000033166.
Consent for publication
No identifiable information is contained in this paper.
Competing interests
The authors report no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Outcomes of correlation between the distance of 6-minute walk test (6MWT) and every item of pulmonary function test (PFT).
Additional file 2.
Individual-participant data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xiang, XN., Zong, HY., Ou, Y. et al. Exoskeleton-assisted walking improves pulmonary function and walking parameters among individuals with spinal cord injury: a randomized controlled pilot study. J NeuroEngineering Rehabil 18, 86 (2021). https://doi.org/10.1186/s12984-021-00880-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12984-021-00880-w