
Abstract
Objectives
To explore an optimal model to predict the response of patients with axillary lymph node (ALN) positive breast cancer to neoadjuvant chemotherapy (NAC) with machine learning using clinical and ultrasound-based radiomic features.
Methods
In this study, 1014 patients with ALN-positive breast cancer confirmed by histological examination and received preoperative NAC in the Affiliated Hospital of Qingdao University (QUH) and Qingdao Municipal Hospital (QMH) were included. Finally, 444 participants from QUH were divided into the training cohort (n = 310) and validation cohort (n = 134) based on the date of ultrasound examination. 81 participants from QMH were used to evaluate the external generalizability of our prediction models. A total of 1032 radiomic features of each ALN ultrasound image were extracted and used to establish the prediction models. The clinical model, radiomics model, and radiomics nomogram with clinical factors (RNWCF) were built. The performance of the models was assessed with respect to discrimination and clinical usefulness.
Results
Although the radiomics model did not show better predictive efficacy than the clinical model, the RNWCF showed favorable predictive efficacy in the training cohort (AUC, 0.855; 95% CI 0.817–0.893), the validation cohort (AUC, 0.882; 95% CI 0.834–0.928), and the external test cohort (AUC, 0.858; 95% CI 0.782–0.921) compared with the clinical factor model and radiomics model.
Conclusions
The RNWCF, a noninvasive, preoperative prediction tool that incorporates a combination of clinical and radiomics features, showed favorable predictive efficacy for the response of node-positive breast cancer to NAC. Therefore, the RNWCF could serve as a potential noninvasive approach to assist personalized treatment strategies, guide ALN management, avoiding unnecessary ALND.
Similar content being viewed by others

Introduction
Breast cancer is a major public health issue, and more than 4.4 million women’s health is threatened by breast cancer worldwide [1]. Since 1894, axillary lymph node (ALN) dissection (ALND) has been regarded as an integral part of surgical treatment and applied in all breast cancer surgeries [2]. However, there are many potential complications of ALND, including postoperative arm pain, nerve injury, lymphedema and significant trauma, limiting its further application [3]. Recently, neoadjuvant chemotherapy (NAC) has been regarded as the preoperative initial systemic treatment and applied for patients with clinically node-positive breast cancer subtypes to improve survival [4, 5]. According to previous studies, more than 50% of patients could achieve pathological complete response (pCR) post-NAC, avoid ALND and receive conservation surgery [6, 7]. However, in the clinic, invasive operations such as ALND and sentinel ALN biopsy, are still regarded as routine methods for assessing the status of the ALN [8].
Therefore, many studies have tried to assess ALN status based on noninvasive approaches, such as clinical prediction models, magnetic resonance imaging (MRI) and ALN ultrasound (ALNU), to reduce unnecessary ALND [9,10,11,12,13]. However, these preoperative prediction models have not yet been used in large-scale clinical practice because of the limited power of these traditional clinical and single imaging characteristics. With the development of radiomics, many radiomics models have shown favorable predictive efficacy and have been applied in clinical decision-making [14, 15]. For example, Dong et al. [16] used the least absolute shrinkage and selection operator (LASSO) and stepwise multivariate logit regression to achieve ultrasound radiomics feature selection and build the model to predict the histological grades and Ki-67 expression of hepatocellular carcinoma. To the best of our knowledge, there have been only limited reports of predictive models combining clinical characteristics and radiomics features to assess ALN status after NAC.
Therefore, we aimed to explore an optimal model to predict ALN status and assess the response of patients with node-positive breast cancer to presurgical NAC with machine learning (ML) using clinical and ALNU-based radiomic features.
Methods
Population
In this study, 1014 patients with ALN-positive breast cancer confirmed by histological examination and received preoperative NAC in the Affiliated Hospital of Qingdao University (QUH) and Qingdao Municipal Hospital (QMH) from July 2016 to September 2022 were initially included. Institutional review board approval of the two hospitals (QUH and QMH) was obtained, and patient informed consent was waived for this retrospective analysis.
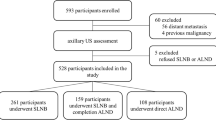
The exclusion criteria were patients with distant metastasis (n = 55); NAC incomplete due to lesion augmentation (n = 71); male breast cancer (n = 4); previous axillary surgery (n = 19); bilateral ALN positivity (n = 11); immunohistochemistry test absence (n = 54); ALNU imaging unavailability (or more than 4 weeks before surgery) (n = 123); no ALND after NAC (n = 48); and images carried with measured traces (which would cause interference to radiomic features extraction (n = 104). The flowchart of inclusion and exclusion is illustrated in Fig. 1.

The detailed flowchart for patient inclusion
Finally, a total of 525 patients were enrolled, and 444 patients from QUH were divided into the training cohort (n = 310) and validation cohort (n = 134) based on the date of ALNU examination to train and validate the ML models. 81 patients from QMH were divided into the external test cohort and used to evaluate the external generalizability of our prediction models.
Diagnosis of ALN status
The final diagnosis of ALN status in all patients was established based on the pathological results of ALND, and the pathological results were confirmed by at least 2 pathologists with more than 5 years of experience.
Clinical and pathologic characteristics
Clinical data and pathologic characteristics were drawn from medical records. The NAC regimens included taxane plus anthracycline and cyclophosphamide (TAC), anthracycline plus cyclophosphamide followed by taxane (AC-T), anthracycline plus taxane (AT), anthracycline plus cyclophosphamide followed by taxane plus trastuzumab (AC-TH), anthracycline plus cyclophosphamide followed by taxane plus trastuzumab and pertuzumab (AC-THP), taxane plus trastuzumab (TH), taxane plus trastuzumab and pertuzumab (THP), taxane plus carboplatin (TCb), taxane plus carboplatin and trastuzumab (TCbH), and taxane and carboplatin plus trastuzumab and pertuzumab (TCbHP). In addition, the details of NAC regimens and course are shown in the Additional file 1.
The status of estrogen receptor (ER), human epidermal growth factor receptor 2 (HER2), and Ki-67 was assessed based on the immunohistochemical staining of breast tumors. The definition of ER-positive (≥ 10% immunostained cells) and HER2 positive (≥ 3+ in hematoxylin–eosin staining, or 2+ with confirmation of HER2 gene amplification by fluorescence in situ hybridization) has been widely reported in previous studies [17]. In the present study, Ki-67 with a proliferation index higher than 20% was considered positive.
ALNU examination
All patients from QUH were using a 5–12 MHz linear-array transducer (Hitachi-EUB7500) or a 5–14 MHz linear-array transducer (Siemens S2000), and ALNU was performed at the end of NAC for response evaluation by four radiologists with 3–15 years of experience.
Patients from QMH were using a 6- to 15-MHz linear-array transducer (GE Logic quasi E9), 5–12 MHz linear-array transducer (Philips EPIQ7) or 5−4 MHz (Hitachi ALOKA), and ALNU was performed at the end of NAC for response evaluation by three radiologists with 4, 7, and 12 years of experience, respectively.
Evaluation of ALNU
The most suspicious ALN was selected and reviewed by two radiologists with 7–10 years of experience in sonography diagnosis who were unknown to surgical and pathological reports with node size and shape measured and evaluated. Hypoechoic cortex and hyperechoic medulla next to it are major features to recognize ALN. The thicker the cortex was, the greater probability of residue disease considered to be. If an ALN presented focal cortical thickening or absence of the echogenic fatty hilum, then it was recorded [18, 19]. When a disagreement occurred, another radiologist participated in the evaluation until a consensus was reached. The ALN maximum long axis was regarded as the long axis, and the perpendicular axis was regarded as the short axis. The ALN axis and cortical thickness were measured well due to the software in the working station with the help of a reference provided by the scale plate from primary images (Fig. 2).

Radiological characteristics of the ALN. A The absence of echogenic fatty hilum; B focal cortical thickening; C the measurement of node cortical thickness; D the measurement for long axis and short axis of axillary nodes
Construction of the clinical model
The significant factors selected in univariable analysis were further incorporated into the multiple analysis. Then, the backward stepwise regression analysis was performed to determine the independent risk factors and build the clinical factor model. Odds ratios (OR) as estimates of relative risk with 95% confidence intervals (CI) were calculated for each independent risk factor.
ALN segmentation
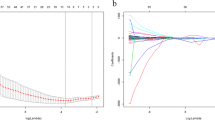
The ROI was segmented manually by two radiologists with at least 10 years of experience from QUH and QMH who were blinded to the ALN status using 3DSlicer software (version 4.8.1). The ROI was drawn along the outline of most suspicious ALN to achieve accurate segmentation and include the whole lesion (Fig. 3A, B).

Construction of radiomics signatures. A, B ROI segmentation; C Cross-validation parameter tuning parameter. The optimal values of the LASSO tuning parameter are indicated by the dotted vertical lines; D LASSO coefficient profiles of the radiomics features. A coefficient profile plot was generated versus the selected value using tenfold cross-validation; the vertical line was plotted with selected radiomics features
Radiomics feature extraction
All radiomics features were extracted from the ROI using the PyRadiomics package (based on Python). 1032 radiomic features of each ROI were extracted using gray level co-occurrence matrix (GLCM), gray level dependence matrix (GLDM), gray level run length matrix (GLRLM), and gray level size zone matrix (GLSZM). In addition, the details of the extraction method and radiomic features are shown in the Additional file 1.
Construction of the radiomics model
Z-score normalization of radiomics features was performed based on the mean and standard deviation from the data. For our high-dimensionality dataset, feature selection and classification were necessary, so the minimal redundancy maximum relevance (MRMR) algorithm was applied to evaluate the feature relevance. The MRMR selected subset of features was enrolled in LASSO regression model to select the most valuable features and build the radiomics model in the training cohort. Fivefold cross-validation was set to finalize candidate features. In addition, the radiomics score for each patient was calculated by the selected features based on their weighted coefficients.
Development of the radiomics nomogram with clinical factors (RNWCF)
The RNWCF was developed by combining the significant clinical factors and radiomics score. The independent risk factors were determined, and the RNWCF was built based on logistic regression analysis.
Evaluation of the performance of different models
For the validation cohort and external test cohort, the accuracy, sensitivity, and specificity of different models were calculated. Receiver operating characteristic (ROC) curves and the area under the ROC curve (AUC) were used to assess the performance of the models and describe their predictive power.
Statistical analysis
Normally distributed continuous variables are shown as the mean ± standard deviation, and categorical variables are shown as percentages (%). Student’s t test, the Chi-square test and Fisher’s exact test were performed by SPSS Statistics software, version 22.0 (SPSS Inc., Chicago, IL, USA). Building and evaluating the performance of different models (including ROC curve analysis, logistic regression analysis, MRMR analysis, LASSO regression, etc.) were performed by Python 3.10.4. The factors with P values < 0.05 in univariable analysis were selected and incorporated into the multiple analysis. P < 0.1 (two-sided) was considered statistically significant in the multiple analysis.
Results
Population characteristics
As shown in Table 1 and 310 patients were enrolled in the training cohort according to the screening criteria, including 221 ALN+ (mean age, 49.74 ± 10.88 years; 63.35% ER+) and 89 ALN− patients (mean age, 49.21 ± 9.76 years; 50.56% ER+); and 134 patients were enrolled in the validation cohort, including 95 ALN+ (mean age, 50.42 ± 9.82 years; 69.47% ER+) and 39 ALN− patients (mean age, 49.54 ± 9.31 years; 46.15% ER+). 81 patients (52 ALN+ and 29 ALN−) from QMH were enrolled in the external test cohort. In addition, there was no significant difference in NAC regimens between ALN+ and ALN− patients in the three cohorts (P > 0.05, respectively).
Clinical model
The results of univariate analysis of clinicopathological variables are shown in Table 2. Table 3 shows that the clinical nodal category (N stage) (P = 0.009, OR = 2.320), long axis (P = 0.056, OR = 0.453), short axis (P = 0.051, OR = 9.142), cortical thickness of ALN (P < 0.001, OR = 1308.975), ER (P = 0.046, OR = 1.883), and Ki-67 (P = 0.024, OR = 0.489) were proven to be independent clinical predictors in the training cohort and input into the model. The AUCs of the clinical model in the training cohort (0.833; 95% CI 0.791–0.872), validation cohort (0.881; 95% CI 0.830–0.930) and external test cohort (0.851; 95% CI 0.773–0.915) are shown in Fig. 5.

The ROC curves of the clinical model, radiomics model and RNWCF in A the training cohort, B the validation cohort and C the external test cohort. The ROC curves of the RNWCF nomogram are outperformed than the radiomics signature in both the validation and external test cohort
Radiomics feature selection and model building
As shown in Table 4; Fig. 3, the nine most valuable radiomics features were selected and used to build the radiomics model. The radiomics signatures were calculated based on the coefficients of the radiomics features (Table 5).
The AUCs of the radiomics model were 0.792 (95% CI 0.748–0.836) in the training cohort, 0.761 (95% CI 0.686–0.829) in the validation cohort and 0.723 (95% CI 0.626–0.816) in the external test cohort (Fig. 5).
Development of RNWCF
The N stage, long axis, short axis, cortical thickness of the ALN, ER, Ki-67, and radiomic signatures were incorporated into the construction of the RNWCF (Table 6; Fig. 4). Compared with the clinical model and radiomics model, the RNWCF showed the favorable AUCs in the training cohort (0.855; 95% CI 0.817–0.893), validation cohort (0.882; 95% CI 0.834–0.928) and external test cohort (0.858; 95% CI 0.782–0.921) (Fig. 5). In addition, the accuracy, sensitivity, and specificity of the different models are shown in Table 7.

The RNWCF nomogram, combining N stage, long axis, short axis, cortical thickness, ER, Ki67 and radiomics signatures, developed in the training set
Discussion
For breast cancer patients with initial positive nodes, the ALN status after NAC is used as an important reference for axilla treatment decision making and may possibly exempt ALND when a negative result is obtained. The diagnostic accuracy of current imaging modalities for ALN status assessment post-NAC is generally inferior to that pre-NAC [20]. Morphologic changes, such as atrophy and fibrosis, in ALN caused by the response to NAC are the main reasons that make it difficult to identify residual metastases [21]. As a result, many researchers focused on using clinical models to predict ALN status after NAC.
However, the diagnostic performance of radiomics model to assess ALN status after NAC has seldomly been reported in previous studies. In this study, three models (clinical model, radiomics model and RNWCF) were built to evaluate post-NAC ALN status, and different algorithms were used respectively. For clinical model, univariate analysis was used to select the risk factors and N stage, long axis, short axis, cortical thickness of ALN, ER, and Ki-67 were identified as independent risk factors. Then backward-stepwise regression was used to build the clinical model with the AUC of 0.851 in external test cohort which was consistent with those of another research. Wang et al. [28] built a clinical model to predict ALN status after NAC with 320 breast cancer patients included, and the AUC value was 0.802. Kim et al. [22] developed a clinical model based on 408 women from one medical institution to predict the ALN response to NAC in node-positive breast cancer patients using MRI and ultrasound, and the AUC value in the validation sets reached 0.78. The small difference between AUC value of clinical models in different studies maybe due to the discrepancy of enrolled and selected the clinical factors. For radiomics model, MRMR and LASSO regression were applied, and nine most valuable radiomics features were selected and put into the model. The AUC value was 0.761 in validation cohort and 0.723 in external test cohort indicating that radiomic model based on AUS is predictive but not reliable. We speculated that morphologic changes in ALN caused by response to NAC might also hinder radiomics model to correctly recognize ALN metastases after NAC. More research could be carried out to overcome this problem. In addition, we also developed RNWCF, an integrated model combining clinical characteristics (N stage, long axis, short axis, cortical thickness of the ALN, ER, Ki-67) and radiomics signatures based on the multivariable logistic regression and had an AUC of 0.858 in the external test cohort. Currently, most studies focused on radiomic models or integrated models involved radiomics features for the prediction of preoperative ALN status in initially diagnosed breast cancer [17, 23,24,25]. Only a few studies have attempted to explore the effective approach involved radiomic signatures to predict ALN status after NAC for breast cancer patients. Zhou et al. [4] determined the feasibility of an integrated model containing radiomic signatures which derived from machine learning for the prediction of ALN pCR after NAC based on 247 patients from two institutions and the AUC value was 0.85 in validation cohort. However, they did not show the single predictive value of radiomic approach for ALN residue disease prediction. In addition, although those predictive models for ALN status evaluation, before or after NAC, achieved fine prediction performance in training and internal validation cohort, they did not have an external test set to investigate the generalizability [17, 23,24,25].
Unsatisfied generalizability in external test would hinder the translation of radiomics model into clinical practice, and the gap between radiomics model research and clinical practice should be filled up. Therefore, the heterogeneity between different ultrasound machines and different ultrasound protocols must be given more attention to. A Z-score normalization approach was applied to ameliorate this problem in our study, and the two-center research protocol and results (patients from 2 institutions and ALNU images from 4 ultrasound machines) proved the reliability of our model.
Consistent with previous studies, N stage and Ki-67 level were selected as independent risk factors and incorporated into the RNWCF in the present study. As an immunohistochemical proliferation marker, Ki67 has been extensively studied and explored to evaluate the ALN response to NAC in breast cancer [26]. It has already been reported that Ki-67 levels indicate proliferating cell levels, so higher Ki-67 levels indicate a higher pCR rate [27]. Cortical thickness also helped to identify pCR in the clinical model and RNWCF. The increase in cortical thickness shown on ALNU was regarded as association with malignancy [28]. Tumor cell infiltration in ALNs could cause cortical thickening. Greater cortical thickness was more likely to be related to a poor response to NAC and therefore less likely to achieve pCR [29].
This study had several limitations. First, selective bias and inherent errors were inevitable in a retrospective study. Second, though our study had a relatively large sample size than those from previous studies, multicenter analyses with a larger sample are required in the future. Finally, all ROIs in this study were drawn manually thus discrepancy between operator was inevitable. Therefore, we plan to conduct automatic segmentation and feature selection to optimize the construction of prediction models in future studies.
Conclusion
In conclusion, we developed the clinical model, radiomics model and integrated model (RNWCF) for the prediction of ALN status after NAC. The RNWCF, combining the clinical characteristics and radiomics features of ALN, showed favorable predictive efficacy for ALN status evaluation. Therefore, the RNWCF could potentially serve as a noninvasive approach to assess the response of ALN to NAC, assisting personalized treatment strategies making, guiding ALN management, and probably avoiding unnecessary ALND. Further studies such as deep learning and prospective studies would be carried out, which could avoid the manual segmentation and determine the clinical feasibility of our predictive model.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALN:
-
Axillary lymph node
- ALND:
-
Axillary lymph node dissection
- NAC:
-
Neoadjuvant chemotherapy
- pCR:
-
Pathological complete response
- MRI:
-
Magnetic resonance imaging
- ALNU:
-
Axillary lymph node ultrasound
- ML:
-
Machine learning
- ER:
-
Estrogen receptor
- HER2:
-
Human epidermal growth factor receptor 2
- OR:
-
Odds ratios
- CI:
-
Confidence intervals
- ROI:
-
Region of interest
- GLCM:
-
Gray level co-occurrence matrix
- GLDM:
-
Gray level dependence matrix
- GLRLM:
-
Gray level run length matrix
- GLSZM:
-
Gray level size zone matrix
- MRMR:
-
Minimal redundancy maximum relevance
- LASSO:
-
Least absolute shrinkage and selection operator
- RNWCF:
-
Radiomics nomogram with clinical factors
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the receiver operating characteristic curve
References
Veronesi U, Boyle P, Goldhirsch A, Orecchia R, Viale G. Breast cancer. Lancet. 2005;365(9472):1727–41.
Noguchi M, Morioka E, Ohno Y, Noguchi M, Nakano Y, Kosaka T. The changing role of axillary lymph node dissection for breast cancer. Breast Cancer. 2013;20(1):41–6.
Sakorafas GH, Peros G, Cataliotti L. Sequelae following axillary lymph node dissection for breast cancer. Expert Rev Anticancer Ther. 2006;6(11):1629–38.
Zhou T, Yang M, Wang M, Han L, Chen H, Wu N, Wang S, Wang X, Zhang Y, Cui D, Jin F, Qin P, Wang J. Prediction of axillary lymph node pathological complete response to neoadjuvant therapy using nomogram and machine learning methods. Front Oncol. 2022;12:1046039.
Hennessy BT, Hortobagyi GN, Rouzier R, Kuerer H, Sneige N, Buzdar AU, Kau SW, Fornage B, Sahin A, Broglio K, Singletary SE, Valero V. Outcome after pathologic complete eradication of cytologically proven breast cancer axillary node metastases following primary chemotherapy. J Clin Oncol. 2005;23(36):9304–11.
Boughey JC, Suman VJ, Mittendorf EA, Ahrendt GM, Wilke LG, Taback B, Leitch AM, Kuerer HM, Bowling M, Flippo-Morton TS, Byrd DR, Ollila DW, Julian TB, McLaughlin SA, McCall L, Symmans WF, Le-Petross HT, Haffty BG, Buchholz TA, Nelson H, Hunt KK. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: the ACOSOG Z1071 (Alliance) clinical trial. JAMA. 2013;310(14):1455–61.
Mougalian SS, Hernandez M, Lei X, Lynch S, Kuerer HM, Symmans WF, Theriault RL, Fornage BD, Hsu L, Buchholz TA, Sahin AA, Hunt KK, Yang WT, Hortobagyi GN, Valero V. Ten-year outcomes of patients with breast cancer with cytologically confirmed axillary lymph node metastases and pathologic complete response after primary systemic chemotherapy. JAMA Oncol. 2016;2(4):508–16.
Lyman GH, Somerfield MR, Bosserman LD, Perkins CL, Weaver DL, Giuliano AE. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology Clinical Practice guideline update. J Clin Oncol. 2017;35(5):561–4.
Vila J, Mittendorf EA, Farante G, Bassett RL, Veronesi P, Galimberti V, Peradze N, Stauder MC, Chavez-MacGregor M, Litton JF, Huo L, Kuerer HM, Hunt KK, Caudle AS. Nomograms for predicting axillary response to neoadjuvant chemotherapy in clinically node-positive patients with breast cancer. Ann Surg Oncol. 2016;23(11):3501–9.
Murphy BL, Heins TLH, Habermann CDN, Boughey EB. Preoperative prediction of node-negative disease after neoadjuvant chemotherapy in patients presenting with node-negative or node-positive breast cancer. Ann Surg Oncol. 2017;24(9):2518–25.
Jin X, Jiang YZ, Chen S, Shao ZM, Di GH. A nomogram for predicting the pathological response of axillary lymph node metastasis in breast cancer patients. Sci Rep. 2016;6:32585.
Ouldamer L, Chas M, Arbion F, Body G, Cirier J, Ballester M, Bendifallah S, Daraï E. Risk scoring system for predicting axillary response after neoadjuvant chemotherapy in initially node-positive women with breast cancer. Surg Oncol. 2018;27(2):158–65.
Turnbull LW. Dynamic contrast-enhanced MRI in the diagnosis and management of breast cancer. NMR Biomed. 2009;22(1):28–39.
Nie P, Yang G, Wang Z, Yan L, Miao W, Hao D, Wu J, Zhao Y, Gong A, Cui J, Jia Y, Niu H. A CT-based radiomics nomogram for differentiation of renal angiomyolipoma without visible fat from homogeneous clear cell renal cell carcinoma. Eur Radiol. 2020;30(2):1274–84.
Chee CG, Yoon MA, Kim KW, Ko Y, Ham SJ, Cho YC, Park B, Chung HW. Combined radiomics-clinical model to predict malignancy of vertebral compression fractures on CT. Eur Radiol. 2021;31(9):6825–34.
Dong Y, Zuo D, Qiu YJ, Cao JY, Wang HZ, Wang WP. Prediction of histological grades and Ki-67 expression of hepatocellular carcinoma based on sonazoid contrast enhanced ultrasound radiomics signatures. Diagnostics (Basel). 2022;12(9):2175.
Wang D, Hu Y, Zhan C, Zhang Q, Wu Y, Ai T. A nomogram based on radiomics signature and deep-learning signature for preoperative prediction of axillary lymph node metastasis in breast cancer. Front Oncol. 2022;12:940655.
Lee B, Lim AK, Krell J, Satchithananda K, Coombes RC, Lewis JS, Stebbing J. The efficacy of axillary ultrasound in the detection of nodal metastasis in breast cancer. AJR Am J Roentgenol. 2013;200(3):W314–20.
Vijayaraghavan GR, Vedantham S, Kataoka M, DeBenedectis C, Quinlan RM. The relevance of ultrasound imaging of suspicious axillary lymph nodes and fine-needle aspiration biopsy in the post-ACOSOG Z11 era in early breast cancer. Acad Radiol. 2017;24(3):308–15.
Skarping I, Förnvik D, Zackrisson S, Borgquist S, Rydén L. Predicting pathological axillary lymph node status with ultrasound following neoadjuvant therapy for breast cancer. Breast Cancer Res Treat. 2021;189(1):131–44.
Viale G. Characterization and clinical impact of residual disease after neoadjuvant chemotherapy. Breast. 2013;22(Suppl 2):88–91.
Kim R, Chang JM, Lee HB, Lee SH, Kim SY, Kim ES, Cho N, Moon WK. Predicting axillary response to neoadjuvant chemotherapy: breast MRI and US in patients with node-positive breast cancer. Radiology. 2019;293(1):49–57.
Liu Y, Ye F, Wang Y, Zheng X, Huang Y, Zhou J. Elaboration and validation of a nomogram based on axillary ultrasound and tumor clinicopathological features to predict axillary lymph node metastasis in patients with breast cancer. Front Oncol. 2022;12:845334.
Han L, Zhu Y, Liu Z, Yu T, He C, Jiang W, Kan Y, Dong D, Tian J, Luo Y. Radiomic nomogram for prediction of axillary lymph node metastasis in breast cancer. Eur Radiol. 2019;29(7):3820–9.
Lee SE, Sim Y, Kim S, Kim EK. Predictive performance of ultrasonography-based radiomics for axillary lymph node metastasis in the preoperative evaluation of breast cancer. Ultrasonography. 2021;40(1):93–102.
Luporsi E, André F, Spyratos F, Martin PM, Jacquemier J, Penault-Llorca F, Tubiana-Mathieu N, Sigal-Zafrani B, Arnould L, Gompel A, Egele C, Poulet B, Clough KB, Crouet H, Fourquet A, Lefranc JP, Mathelin C, Rouyer N, Serin D, Spielmann M, Haugh M, Chenard MP, Brain E, de Cremoux P, Bellocq JP. Ki-67: level of evidence and methodological considerations for its role in the clinical management of breast cancer: analytical and critical review. Breast Cancer Res Treat. 2012;132(3):895–915.
Denkert C, Loibl S, Müller BM, Eidtmann H, Schmitt WD, Eiermann W, Gerber B, Tesch H, Hilfrich J, Huober J, Fehm T, Barinoff J, Jackisch C, Prinzler J, Rüdiger T, Erbstösser E, Blohmer JU, Budczies J, Mehta KM, von Minckwitz G. Ki67 levels as predictive and prognostic parameters in pretherapeutic breast cancer core biopsies: a translational investigation in the neoadjuvant GeparTrio trial. Ann Oncol. 2013;24(11):2786–93.
Morency D, Dumitra S, Parvez E, Martel K, Basik M, Robidoux A, Poirier B, Holloway CMB, Gaboury L, Sideris L, Meterissian S, Boileau JF. Axillary lymph node ultrasound following neoadjuvant chemotherapy in biopsy-proven node-positive breast cancer: results from the SN FNAC study. Ann Surg Oncol. 2019;26(13):4337–45.
Huang JX, Lin SY, Ou Y, Shi CG, Zhong Y, Wei MJ, Pei XQ. Combining conventional ultrasound and sonoelastography to predict axillary status after neoadjuvant chemotherapy for breast cancer. Eur Radiol. 2022;32(9):5986–96.
Acknowledgements
We would like to thank the following authors would participate in the study: Hanzhang Wang, PDx GMS Advanced Applications, GE HealthCare, Shanghai.
Funding
No.
Author information
Authors and Affiliations
Contributions
Literature search: HZ and JF; Study design: HZ and JF; Data collection: WC, LL, and FJ; Data analysis: ZM and NS; Model construction: YM and JF; Manuscript writing: HZ and JF. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Univariate analysis and radiomic features.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, H., Cao, W., Liu, L. et al. Noninvasive prediction of node-positive breast cancer response to presurgical neoadjuvant chemotherapy therapy based on machine learning of axillary lymph node ultrasound. J Transl Med 21, 337 (2023). https://doi.org/10.1186/s12967-023-04201-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-023-04201-8