
Abstract
Background
ETS2 is a downstream effector of the RAS/RAF/ERK pathway, which plays a critical role in the development of malignant tumor. However, the clinical impact of ETS2 expression in AML remains unknown.
Methods
In this study, we evaluated the prognostic significance of ETS2 expression using two relatively large cohorts of AML patients.
Results
In the first cohort, compared to low expression of ETS2 (ETS2 low), high expression of ETS2 (ETS2 high) showed significant shorter OS, EFS and RFS in the current treatments including the allogeneic HCT group (n = 72) and the chemotherapy group (n = 100). Notably, among ETS2 high patients, those received allogeneic HCT had longer OS, EFS and RFS than those with chemotherapy alone (allogeneic HCT, n = 39 vs. chemotherapy, n = 47), but treatment modules play insignificant role in the survival of ETS2 low patients (allogeneic HCT, n = 33 vs. chemotherapy, n = 53). Moreover, gene/microRNA expression data provides insights into the biological changes associated with varying ETS2 expression levels in AML. The prognostic value of ETS2 was further validated in the second AML cohort (n = 329).
Conclusions
Our results indicate that ETS2 high is a poor prognostic factor in AML and may guide treatment decisions towards allogeneic HCT.
Similar content being viewed by others


Background
Acute myeloid leukemia (AML) represents a group of myeloid malignancies with remarkably heterogeneous outcomes [1]. Finding effective prognostic biomarkers has been one of the most urgent clinical needs and research hotspots. So far, a few prognosticators have been established, including mutations in NPM1 and double CEBPA that are associated with favourable outcomes; whereas FLT3-ITD is associated with poor prognosis. High expression levels of WT1 [2], miR-155 [3, 4], ERG [5, 6], BAALC [6], and MN1 [7] have also been shown to be poor prognostic factors in AML.
V-ets avian erythroblastosis virus E26 oncogene homolog 2 (ETS2), a downstream target for both the Ras/Raf/MAP kinase and phosphatidylinositol 3-kinase/Akt pathways. ETS2 is one of the founder members of the E26 transformation-specific (ETS) family located on human chromosome 21 [8]. ERG, one of the classic prognostic markers in AML, also belongs to the ETS family. ETS2 and ERG had been shown to be overexpressed in AML patients with complex karyotypes involving chromosome 21 [9]. Although ETS2 was initially characterized as a proto-oncogene acute megakaryocytic leukemia (AMKL) [10], however, the clinical impact of ETS2 expression in AML remains unknown.
In recent years, many studies suggest that ETS2 exhibit both tumor-promoting and tumor-suppressive effects in malignancies. For example, ETS2 has been found to be an oncogene in patients with AML [11], but it also has tumor-suppressive effects in non-small cell lung cancer [12]. Here, we demonstrate ETS2 high as an adverse prognostic biomarker for AML based on analysis of two separate datasets and indicate ETS2 high may guide treatment decisions towards allogeneic HCT; we also explore the distinctive gene/microRNA patterns associated with ETS2 expression.
Methods
Patients
The first cohort was derived from The Cancer Genome Atlas (TCGA) dataset, including 200 clinically annotated adult de novo AML samples [13]. In this cohort, RNA sequencing for 179 samples and microRNA sequencing for 194 samples had been previously reported. Detailed descriptions of clinical and molecular characteristics were also provided. All these data were publicly accessible from the TCGA website. The study was approved by the human studies committee at Washington University with written informed consent obtained from all patients.
The second cohort was derived from a whole AML cohort (n = 329) diagnosed and collected at Erasmus University Medical Center (Rotterdam) between 1990 and 2008, approved by the institutional review boards at Weill Cornell Medical College and Erasmus University Center, and all subjects provided written informed consent in accordance with the Declaration of Helsinki. Microarray expression profiles were obtained by Affymetrix Human Genome 133 plus 2.0 and U133A Gene Chips from GSE6891 data. All experiments’ design, quality control and data normalization were in line with the standard Affymetrix protocols. All clinical, cytogenetic and molecular information as well as microarray data of these patients were publicly accessible at the Gene Expression Omnibus (GSE6891, http://www.ncbi.nlm.nih.gov/geo) [14]. All patients were uniformly treated under the study protocols of Dutch-Belgian Cooperative Trial Group for Hematology Oncology (HOVON, details of therapeutic protocol available at http://www.hovon.nl).
Statistical analyses
OS was defined as the time from the date of diagnosis to death due to any cause. EFS was defined as the time from the date of diagnosis to removal from the study due to the absence of complete remission, relapse or death. RFS was defined as the time from the date of diagnosis to removal from the study due to relapse.
Patients with higher than median ETS2 expression values of all patients were classified as ETS2 high, and those with lower than median expression values were classified as ETS2 low. To investigate the associations between ETS2 expression levels and clinical, molecular characteristics, the Fisher exact and Wilcoxon rank-sum tests were used for hypothesis testing with categorical and continuous variables, respectively. The associations between ETS2 expression and the OS, EFS and RFS were analyzed by the Kaplan–Meier method and the log-rank test. Multivariate Cox proportional hazard models were employed to study the associations between ETS2 expression levels and OS, EFS and RFS in the presence of other known risk factors. Student’s t test and multiple hypothesis correction (False Discovery Rate, FDR) was used to identify different gene/microRNA between ETS2 high and ETS2 low groups. The statistical cutoff values were an absolute fold-change (FC) ≥1.5 and an adjusted P value ≤0.05. All analyses were performed by the R 3.1.1 software packages.
Results
Expression of ETS2 in AML patients and normal controls
A microarray dataset of bone marrow (BM) samples was used for differential expression analysis, including 30 AML BM and 17 normal BM (NBM) samples (GSE37307, http://www.ncbi.nlm.nih.gov/geo), and 62 AML BM and 42 NBM samples (GSE63270, http://www.ncbi.nlm.nih.gov/geo). Higher expression of ETS2 was shown significantly in AML BM than NBM (P = 0.01, Fig. 1a and P = 0.05, Fig. 1b).

Differences in the expression of ETS2 in AML. a AML-BM cases (n = 30) compared with NBM samples (n = 17), b AML-BM cases (n = 62) compared with NBM samples (n = 42), c relative expression of ETS2 in the different NCCN-risk subgroup (good, intermediate and poor) of AML cases, d associations between ETS2 expression and other classic prognostic biomarkers in AML cases (FLT3-ITD and the mutation of NPM1 and CEBPA)
Relative expression of ETS2 in different National Comprehensive Cancer Network (NCCN) risk subgroups
In the first cohort, ETS2 showed averagely higher expression in the NCCN poor- and intermediate-risk patients than that in the good-risk group (good vs. intermediate P = 0, intermediate vs. poor P = 0.0181, and good vs. poor P = 0, respectively; Fig. 1c).
Associations between ETS2 expression and other classic prognostic biomarkers in AML
The first cohort were further divided into subgroups by the presence of FLT3-ITD and mutation status of NPM1 and CEBPA. Levels of ETS2 expression were compared among different subgroups. ETS2 showed significantly higher expression in samples with FLT3-ITD compared than samples without FLT3-ITD (P = 0.006, Fig. 1d). No significant differences were revealed between NPM1-mutated and wild-type samples (P = 0.0657) or between CEBPA-mutated and wild-type samples (P = 0.2977, Fig. 1d).
Differences in clinical and molecular characteristics between ETS2 high and ETS2 low groups
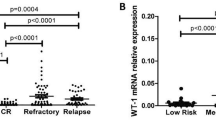
In the first cohort, ETS2 high patients were more likely to be ≥60-year-old, and had higher WBC count, higher peripheral blood blasts, more diagnosed with M0, M1, M3, or M5 FAB subtypes, and more FLT3-ITD and TP53 mutation (P = 0.004, P = 0.05, P = 0.01, P = 0.001, P = 0.005, P < 0.001, P = 0.04, P = 0.01, P = 0.016, respectively) comparing with ETS2 low patients. No other associations between ETS2 expression and other mutations were found. Additionally, ETS2 high patients with AML were more likely to have a higher expression of MN1, miR155HG and WT1 than ETS2 low patients (P = 0.04, P < 0.001, and P = 0.009, respectively). See Table 1.
ETS2 high was associated with adverse outcomes
ETS2 high patients had markedly shorter OS (Fig. 2a, P = 2e−6), EFS (Fig. 2b, P = 1e−6) and RFS (Fig. 2c, P = 3.8e−5) comparing with ETS2 low patients. Associations between ETS2 expression and prognostic significance within the allogeneic HCT group and chemotherapy group were also separately analyzed. Within the allogeneic HCT group (n = 72), significant differences were observed in OS (Fig. 2d, P < 0.001), EFS (Fig. 2e, P = 0.002) and RFS (Fig. 2f, P = 0.012) between the ETS2 high and ETS2 low patients. In the chemotherapy group (n = 99), ETS2 high patients had significantly shorter OS (Fig. 2d, P < 0.001), EFS (Fig. 2e, P < 0.001) and RFS (Fig. 2f, P = 0.002) than ETS2 low patients. Moreover, ETS2 high patients who received allogeneic HCT had significantly longer OS and EFS than chemotherapy-only (OS, P < 0.002; EFS, P = 0.029, respectively), whereas treatment modules play insignificant role in the survival of ETS2 low patients (allogeneic HCT vs. chemotherapy-only; OS, P = 0.067; EFS, P = 0.774; RFS, P = 0.148, respectively).

The prognostic value of ETS2 expression in AML patients from TCGA data. a OS and b EFS and c RFS of the entire AML patients (n = 179). d OS and e EFS and f RFS of the AML patients of ETS2 high group (n = 86), ETS2 low group (n = 88), allogeneic HCT group (n = 72) and chemotherapy-only group (n = 100). Allo allogeneic HCT, Chemo chemotherapy
ETS2 expression was associated with shorter OS, EFS and RFS in multivariate analyses
To adjust for the impact of known clinical and molecular risk factors, we performed multivariate analyses to confirm the prognostic significance of ETS2 expression (Table 2). In the multivariate models for OS, EFS and RFS, ETS2 high had adverse impacts on OS (P = 0.002), EFS (P < 0.001) as well as RFS (P < 0.001). Age was the only other factor negatively correlated with OS (P < 0.001) and EFS (P < 0.001).
Associations between genome-wide gene-expression profiles and ETS2 expression
To further assess the role of ETS2 in AML, we derived ETS2-associated gene expression profiles by high throughput sequencing from TCGA data. We first identified 368 up-regulated and 171 down-regulated genes that were significantly associated with ETS2 expression (P < 0.05, fold change = 1.5, Fig. 3a). With a more rigorous analysis (fold change = 2, and profiles without applicable values were all deleted), 359 genes were filtered out and the rest 180 genes were presented in an aberrant expression heat map (Fig. 3b).

Genome-wide genes/microRNAs associated with ETS2 expression. a Volcano plot of different gene-expression profiles between ETS2 high and ETS2 low; ETS2 high and ETS2 low were marked by red and green circles, respectively. b Expression heatmap of ETS2-associated genes. c Expression heatmap of associated microRNAs. Patients are ordered from left to right by increasing ETS2 expression. Expression values of the gene and microRNA probe sets are represented by color, with green indicating expression less than and red indicating expression greater than the value for the given gene and microRNA probe set. For the gene and miR-RNA expression heat map, up- and down-regulated genes and miR-RNAs mentioned in the text are indicated. d Boxplots of miR-155-5p and miR-155-3p expression associated with ETS2 expression
Many genes known as unfavorable biomarkers were up-regulated, including leukemia-associated molecules, such as: (1) genes (Wnt2B and Wnt9A) of Wnt signaling pathway involved in leukemogenesis; (2) independent adverse prognostic factors in AML including WT1, miR-155HG [3, 4], SOCS2 [15], TCF4 [16], MAP7 [17], ID1 [18] and MSI2 [19]. However, some tumor suppressors were down-regulated, such as: (1) CDH13, silenced by aberrant promoter methylation, similar silencing had been found to be involved in the pathogenesis in chronic myeloid leukemia (CML) [20]; (2) VSTM1, which had also been found down-regulated in bone marrow cells from leukemia patients and played an important role in the pathogenesis of leukemia [21]; (3) CEBPA-dependent HK3 expression, its decrease promoted primary AML [22]; (4) Fez1, its absence impaired Cdk1/Cdc25C interaction during mitosis and in mouse models could predispose mice to cancer development [23]; (5) TGM3, a candidate tumor suppressor gene that contributed to human head and neck cancer [24]; (6) ITPKA, its down-regulation by early aberrant DNA methylation was also found in a mouse model of acute myeloid leukemia [25].
Associations between genome-wide microRNA profiles and ETS2 expression
An analysis of microRNA genome-wide profiles revealed 145 microRNAs that were strongly associated with ETS2 expression (P < 0.05, Fig. 3c). ETS2 high was positively correlated with levels of miR-10a, miR-155, miR-146b and miR-1. Notably, in the profiles we generated, miR-155-3p and miR-155-5p were up-regulated (Fig. 3d). In previous reports, these microRNAs were shown to have important tumor-promoting properties. For example, overexpression of miR-10a was associated with poor OS in AML patients [26]. Up-regulation of miR-155 was an independent risk factor associated with an unfavorable clinical outcome in cytogenetically normal-AML (CN-AML) [3]. Knockdown of endogenous miR-146b would result in increased transcription of tumor suppressors and inhibition of cell proliferation in chronic lymphocytic leukemia (CLL) [27]. MiR-1-2 modulation was vital for EVI1-associated tumor proliferation in acute myeloid leukemia [28].
ETS2 high was negatively correlated with levels of miR-223, miR-142, miR-30e and miR-197. These microRNAs had been shown to exhibit tumor suppressive properties. Low miR-223 expression was associated with worse outcome in AML [29]. MiR-142-3p was a key regulator of normal myeloid differentiation; its reduced expression was involved in the leukemogenesis of AML [30]. MiR-30e induced apoptosis and could sensitize cell lines to imatinib via regulation of the BCR-ABL protein [31]. MiR-197 induced apoptosis and suppressed multiple myeloma by targeting MCL-1 [32].
Association between ETS2 high and adverse outcomes was confirmed by the second cohort
We studied the second cohort of 329 previously untreated AML patients. Firstly, ETS2 high AML patients (n = 164) had significantly shorter OS (P = 0.006, Fig. 4a) and EFS (P = 0.001, Fig. 4b) than ETS2 low patients (n = 165). Secondly, in the NCCN intermediate-risk AML patients, ETS2 high (n = 86) also had significantly shorter OS (P = 0.049, Fig. 4a) and EFS (P = 0.045, Fig. 4b) than ETS2 low patients (n = 87). Thirdly, ETS2 high CN-AML patients (n = 78) had significantly shorter OS (P = 0.02, Fig. 4c) and EFS (P = 0.004, Fig. 4d) than ETS2 low patients (n = 78). Fourthly, for patients in the European Leukemia Net (ELN) Intermediate-I category, ETS2 high (n = 60) also had significantly shorter OS (P = 0.01, Fig. 4c) and EFS (P = 0.008, Fig. 4d) than ETS2 low patients (n = 61).

The prognostic value of ETS2 expression in the second cohort. a OS and b EFS of 329 AML patients and the subgroup of 173 patients with NCCN intermediate-risk. c OS and d EFS of the 156 CN-AML patients and 121 AML patients in the ELN Intermediate-I category
Discussion
Identifying the prognostic factors for AML is important for the development of new targeted therapies and risk-stratified treatment strategies. Recent studies had shown that high expression of ERG and ERG amplification, the most frequent copy-number alteration (CNA), are all the worse prognostic markers in AML patients [5, 6, 33]. ETS2, one of the members of the ETS family as ERG, was previously characterized as a proto-oncogene in AMKL children that is Down-syndrome and non-Down-syndrome-related [10], but the expression and clinical prognosis of ETS2 in AML remains unknown. Here, we have demonstrated the aberrant expression of ETS2 in AML patients. First, we found that ETS2 expression was up-regulated in AML cohorts and was overexpressed in the NCCN intermediate- and poor-risk groups of patients, compared to the good-risk group. These findings indicated that ETS2 might promote leukemogenesis. We also found that ETS2 showed higher expression in monocytes using publicly available expression data which suggest that ETS2 might play an important role in the function of monocytes [34] (Additional file 1: Figure S1). Second, in the first cohort, our study demonstrated that ETS2 high was associated with shorter OS and EFS. Notably, ETS2 high patients had longer OS and EFS after receiving allogeneic HCT than chemotherapy-only, but similar differences between treatment modules were not observed in ETS2 low patients. Its presence may direct treatment decisions towards allogeneic HCT.
To further confirm the prognostic significance of ETS2, we analyzed the second cohort of uniformly treated AML patients. ETS2 high also acted as an independent poor prognostic factor in the entire cohort, NCCN Intermediate-risk subgroup, CN-AML subgroup, as well as the ELN Intermediate-I subgroup. The above results denoted that ETS2 high was an independent, poor prognostic factor in AML. It could be employed to improve the risk stratification of ELN Intermediate-I category and NCCN Intermediate-Risk group.
Gene and microRNA-expression profiles derived from the first cohort gave us some insight regarding the role of ETS2 in AML leukemogenesis. Tumor protein 53 (TP53) is one of the most frequently inactivated tumor suppressor genes in human cancer and its mutations predict a poor prognosis in patients with acute myeloid leukemia (AML) [35]. Recent studies have shown that mutations in the TP53 (mTP53) protects ETS2 from degradation and mTP53 disrupts ETS family target gene regulation, promoting cancer [36]. In our study, we found that ETS2 high was associated with mTP53.
The expression of miR-155 has been found to be independently associated with poor clinical outcome in AML [3, 4]. In addition, we found that ETS2 high was associated with over-expression of miR-155HG, miR-155-3p and miR-155-5p. This result is in accordance with recent studies which have found that ETS2 is an important transcription factor regulating miR-155 [37].
Conclusions
In summary, ETS2 high is an independent poor prognostic factor in AML patients and its presence should favor allogeneic HCT over chemotherapy-only in AML. In AML patients, distinctive gene/microRNA expression profiles associated with ETS2 expression may explain the role of ETS2 in the leukemogenic process.
Abbreviations
- ETS :
-
E26 transformation-specific
- ETS2 :
-
V-ets avian erythroblastosis virus E26 oncogene homolog 2
- AML:
-
acute myeloid leukemia
- AMKL:
-
acute megakaryocytic leukemia
- OS:
-
overall survival
- EFS:
-
event-free survival
- RFS:
-
relapse-free survival
- HCT:
-
hematopoietic cell transplantation
- FAB:
-
French–American–British classification
- FLT3-ITD:
-
internal tandem duplication of the FLT3 gene
- MLL-PTD:
-
partial tandem duplication of the MLL gene
- HR:
-
hazard ratio
- CI:
-
confidence interval
References
Dohner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. N Engl J Med. 2015;373(12):1136–52.
Lyu X, et al. Overexpression of Wilms tumor 1 gene as a negative prognostic indicator in acute myeloid leukemia. PLoS ONE. 2014;9(3):e92470.
Marcucci G, et al. Clinical role of microRNAs in cytogenetically normal acute myeloid leukemia: miR-155 upregulation independently identifies high-risk patients. J Clin Oncol. 2013;31(17):2086–93.
Xu LH, et al. Overexpressed miR-155 is associated with initial presentation and poor outcome in Chinese pediatric acute myeloid leukemia. Eur Rev Med Pharmacol Sci. 2015;19(24):4841–50.
Marcucci G, et al. Overexpression of the ETS-related gene, ERG, predicts a worse outcome in acute myeloid leukemia with normal karyotype: a cancer and leukemia group B study. J Clin Oncol. 2005;23(36):9234–42.
Schwind S, et al. BAALC and ERG expression levels are associated with outcome and distinct gene and microRNA expression profiles in older patients with de novo cytogenetically normal acute myeloid leukemia: a cancer and leukemia group B study. Blood. 2010;116(25):5660–9.
Langer C, et al. Prognostic importance of MN1 transcript levels, and biologic insights from MN1-associated gene and microRNA expression signatures in cytogenetically normal acute myeloid leukemia: a cancer and leukemia group B study. J Clin Oncol. 2009;27(19):3198–204.
Wasylyk B, Hagman J, Gutierrez-Hartmann A. Ets transcription factors: nuclear effectors of the Ras-MAP-kinase signaling pathway. Trends Biochem Sci. 1998;23(6):213–6.
Baldus CD, et al. Acute myeloid leukemia with complex karyotypes and abnormal chromosome 21: amplification discloses overexpression of APP, ETS2, and ERG genes. Proc Natl Acad Sci USA. 2004;101(11):3915–20.
Ge Y, et al. The role of the proto-oncogene ETS2 in acute megakaryocytic leukemia biology and therapy. Leukemia. 2008;22(3):521–9.
Santoro A, et al. Amplification of ETS2 oncogene in acute nonlymphoblastic leukemia with t(6;21;18). Cancer Genet Cytogenet. 1992;58(1):71–5.
Kabbout M, et al. ETS2 mediated tumor suppressive function and MET oncogene inhibition in human non-small cell lung cancer. Clin Cancer Res. 2013;19(13):3383–95.
The Cancer Genome Atlas Research Network. Genomic and epigenomic landscapes of adult de novo acute myeloid leukemia. N Engl J Med. 2013;368(22):2059–74.
Verhaak RG, et al. Prediction of molecular subtypes in acute myeloid leukemia based on gene expression profiling. Haematologica. 2009;94(1):131–4.
Laszlo GS, et al. High expression of suppressor of cytokine signaling-2 predicts poor outcome in pediatric acute myeloid leukemia: a report from the Children’s Oncology Group. Leuk Lymphoma. 2014;55(12):2817–21.
van der Reijden BA, Monteferrario D, Jansen JH, Huls G. High expression of transcription factor 4 (TCF4) is an independent adverse prognostic factor in acute myeloid leukemia that could guide treatment decisions. Haematologica. 2014;99(12):e257–9.
Fu L, et al. High expression of MAP7 predicts adverse prognosis in young patients with cytogenetically normal acute myeloid leukemia. Sci Rep. 2016;6:34546.
Zhou JD, et al. Clinical significance of up-regulated ID1 expression in Chinese de novo acute myeloid leukemia. Int J Clin Exp Pathol. 2015;8(5):5336–44.
Byers RJ, et al. MSI2 protein expression predicts unfavorable outcome in acute myeloid leukemia. Blood. 2011;118(10):2857–67.
Roman-Gomez J, et al. Cadherin-13, a mediator of calcium-dependent cell–cell adhesion, is silenced by methylation in chronic myeloid leukemia and correlates with pretreatment risk profile and cytogenetic response to interferon alfa. J Clin Oncol. 2003;21(8):1472–9.
Zhou J, et al. Synergistic antitumor activity of triple-regulated oncolytic adenovirus with VSTM1 and daunorubicin in leukemic cells. Apoptosis. 2016;21(10):1179–90.
Federzoni EA, et al. CEBPA-dependent HK3 and KLF5 expression in primary AML and during AML differentiation. Sci Rep. 2014;4:4261.
Vecchione A, et al. Fez1/Lzts1 absence impairs Cdk1/Cdc25C interaction during mitosis and predisposes mice to cancer development. Cancer Cell. 2007;11(3):275–89.
Wu X, et al. TGM3, a candidate tumor suppressor gene, contributes to human head and neck cancer. Mol Cancer. 2013;12(1):151.
Sonnet M, et al. Early aberrant DNA methylation events in a mouse model of acute myeloid leukemia. Genome Med. 2014;6(4):34.
Zhi Y, et al. Serum level of miR-10-5p as a prognostic biomarker for acute myeloid leukemia. Int J Hematol. 2015;102(3):296–303.
Saleh LM, et al. Ibrutinib downregulates a subset of miRNA leading to upregulation of tumor suppressors and inhibition of cell proliferation in chronic lymphocytic leukemia. Leukemia. 2017;31:340–49.
Gomez-Benito M, et al. EVI1 controls proliferation in acute myeloid leukaemia through modulation of miR-1-2. Br J Cancer. 2010;103(8):1292–6.
Gentner B, et al. MicroRNA-223 dose levels fine tune proliferation and differentiation in human cord blood progenitors and acute myeloid leukemia. Exp Hematol. 2015;43(10):858–868.e7.
Wang XS, et al. MicroRNA-29a and microRNA-142-3p are regulators of myeloid differentiation and acute myeloid leukemia. Blood. 2012;119(21):4992–5004.
Hershkovitz-Rokah O, et al. MiR-30e induces apoptosis and sensitizes K562 cells to imatinib treatment via regulation of the BCR-ABL protein. Cancer Lett. 2015;356(2 Pt B):597–605.
Yang Y, et al. miR-137 and miR-197 induce apoptosis and suppress tumorigenicity by targeting MCL-1 in multiple myeloma. Clin Cancer Res. 2015;21(10):2399–411.
Nibourel O, et al. Copy-number analysis identified new prognostic marker in acute myeloid leukemia. Leukemia. 2017;31(3):555–64.
Corces MR, et al. Lineage-specific and single-cell chromatin accessibility charts human hematopoiesis and leukemia evolution. Nat Genet. 2016;48(10):1193–203.
Kadia TM, et al. TP53 mutations in newly diagnosed acute myeloid leukemia: clinicomolecular characteristics, response to therapy, and outcomes. Cancer. 2016;122(22):3484-91.
Martinez LA. Mutant p53 and ETS2, a tale of reciprocity. Front Oncol. 2016;6:35.
Quinn SR, et al. The role of Ets2 transcription factor in the induction of microRNA-155 (miR-155) by lipopolysaccharide and its targeting by interleukin-10. J Biol Chem. 2014;289(7):4316–25.
Authors’ contributions
JS, LF, KX and XK designed the study and wrote the manuscript. HF, QW and YP performed statistical analyses. KX, LZ and JQ analyzed the data. XK, KX and JS coordinated the study over the entire time. All authors read and approved the final manuscript.
Acknowledgements
The authors thank all of the doctors at the institute who participated in this study for providing the follow-up samples and information.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets of this article were generated by TCGA and GEO dataset.
Ethics approval and consent to participate
Written informed consent was obtained from all patients, and was approved by the human studies committee at Washington University.
Funding
This work was supported by grants from the National Natural Science Foundation of China (81500118, 61501519), the China Postdoctoral Science Foundation funded project (Project No. 2016M600443) and PLAGH project of Medical Big Data (Project No. 2016MBD-025).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding authors
Additional file
12967_2017_1260_MOESM1_ESM.pdf
Additional file 1. The hierarchical differentiation tree of relationship between ETS2 expression level and hematopoietic cell differentiation.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Fu, L., Fu, H., Wu, Q. et al. High expression of ETS2 predicts poor prognosis in acute myeloid leukemia and may guide treatment decisions. J Transl Med 15, 159 (2017). https://doi.org/10.1186/s12967-017-1260-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-017-1260-2