
Abstract
Background
The Triglyceride glucose-body mass index (TyG-BMI) and hemoglobin glycation index (HGI) are well-established surrogate markers for insulin resistance. Nevertheless, the extent to which these markers offer additive predictive value for heart failure (HF) prevalence in hypertensive populations, and their predictive utility across various diabetic statuses, remains to be clarified. Consequently, this study aimed to explore the independent and synergistic effects of TyG-BMI and HGI on HF risk among individuals with different diabetic statuses.
Methods
Data from the study population (n = 9847) were obtained from the National Health and Nutrition Examination Survey (NHANES). Multivariable logistic regression models were employed to estimate odds ratios (ORs) and 95% confidence intervals (CIs) to assess the combined associations between TyG-BMI and HGI and the prevalence of HF across various diabetic statuses.
Results
In the total population, compared to the reference group (low TyG-BMI and low HGI), the OR (95% CI) for HF prevalence was 1.30 (1.04, 1.64) for the combination of low TyG-BMI and high HGI, 2.40 (1.76, 3.29) for high TyG-BMI and low HGI, and 3.47 (2.41, 4.99) for high TyG-BMI and high HGI. Interestingly, among normoglycemic individuals, higher TyG-BMI and HGI did not significantly increase the prevalence of HF. Conversely, in the prediabetic population, the OR (95%CI) for HF prevalence was 2.42 (1.69, 3.48) for the combination of high TyG-BMI and low HGI, and 4.30 (2.45, 7.54) for high TyG-BMI and high HGI. Similarly, in the diabetic population, the OR (95%CI) for HF prevalence was 2.22 (1.43, 3.45) for low TyG-BMI and high HGI, 4.04 (2.43, 6.73) for high TyG-BMI and low HGI, and 4.13 (2.25, 7.59) for high TyG-BMI and high HGI, compared to low TyG-BMI and low HGI.
Conclusion
This study reveals that elevated TyG-BMI and HGI levels exert a synergistic impact on the prevalence of HF in hypertensive adults, especially in those with prediabetes and diabetes. Additionally, the presence of prediabetes and diabetes may amplify the detrimental combined effect of TyG-BMI and HGI on HF prevalence.
Similar content being viewed by others

Background
Heart failure (HF) is a prevalent and serious cardiovascular condition associated with significant morbidity and mortality worldwide [1]. Early identification of individuals at an high risk for HF is crucial for timely interventions and the development of effective preventive strategies [2]. Hypertensive adults with prediabetes and diabetes form a vulnerable population that experiences an increased risk of HF due to the complex interplay of various shared mechanisms, such as insulin resistance (IR), cardiac remodeling and fibrosis, inflammation, oxidative stress, vascular complications, and other common risk factors [3,4,5].
Recently, there has been a growing interest in novel indices that integrate multiple metabolic parameters to comprehensively assess cardiometabolic risk and predict adverse cardiovascular outcomes. Notably, the triglyceride glucose-body mass index (TyG-BMI) and the hemoglobin glycation index (HGI) stand out in this context [6, 7]. The TyG-BMI, a composite marker, is formulated through the integration of measurements of insulin resistance (TyG) and BMI as a measure of adiposity [6, 8]. Research has demonstrated that elevated levels of TyG-BMI have been associated with an increased risk of various cardiometabolic abnormalities, including IR, diabetes, dyslipidemia, obesity, and cardiovascular disease (CVD) [9,10,11]. Concurrently, the HGI offers insights into the extent of glycosylated hemoglobin (HbA1c) exceeding the levels anticipated based on glucose levels [12]. It has been proposed as an indicator of glycemic variability and has shown associations with the risk of IR, complications related to diabetes, and CVD [13,14,15].
Previous research has examined these indices in isolation, frequently neglecting their collective influence, especially in hypertensive adults with prediabetes and diabetes. This oversight is significant, as these populations are particularly vulnerable to HF due to interconnected metabolic, inflammatory, and cardiovascular processes [16]. The study addresses this by assessing how the interplay between IR (TyG-BMI) and glycemic control variability (HGI) contributes to HF risk, thus providing a more comprehensive risk assessment tool for these high-risk groups [17, 18]. This approach not only fills a critical gap in understanding the multifactorial nature of HF but also aids in the development of targeted preventive and management strategies for HF in hypertensive individuals with varying diabetic statuses. Moreover, the onset and progression of HF are influenced by various factors, including IR, lipid metabolism, and adiposity, which are recognized as primary pathophysiological mechanisms [19, 20]. Therefore, investigating the combined effect of TyG-BMI and HGI on HF can provide valuable insights into their synergistic effects on the development of HF and assist in identifying individuals at the highest risk.
The objective of this study is to examine the combined effect of TyG-BMI and HGI on the prevalence of HF in hypertensive adults with prediabetes and diabetes. By assessing these biomarkers, the goal is to enhance risk stratification and facilitate the development of personalized preventive and management strategies for HF in this vulnerable population.
Methods
Study population
This study utilized data obtained from the National Health and Nutrition Examination Survey (NHANES), a comprehensive program conducted by the Centers for Disease Control and Prevention (CDC) and the National Centers for Health Statistics (NCHS) in the United States. NHANES is designed to assess the health and nutritional status of the U.S. population, following the STROBE guidelines for reporting observational studies. The NHANES study protocol was sanctioned by the NCHS Research Ethics Review Board, and all participants provided written informed consent. Our study extracted data from the NHANES website (https://www.cdc.gov/nchs/nhanes/index.htm), which encompassed ten survey cycles conducted between 1999 and 2018. After excluding individuals with incomplete data, the final study population comprised 9847 adults aged 20 years or older who had been diagnosed with hypertension and had participated in NHANES across various survey cycles: 1999–2000 (n = 867), 2001–2002 (n = 943), 2003–2004 (n = 897), 2005–2006 (n = 816), 2007–2008 (n = 1077), 2009–2010 (n = 1102), 2011–2012 (n = 1006), 2013–2014 (n = 1085), 2015–2016 (n = 972), and 2017–2018 (n = 1082). The analysis focused on NHANES participants with hypertension, defined as having a systolic blood pressure of 140 mmHg or higher and/or a diastolic blood pressure of 90 mmHg or higher, taking antihypertensive medications, or having a self-reported history of hypertension [21]. Figure 1 presents a flowchart illustrating the selection process of the study population.

Flow chart of study population
Data collection and definitions
This study utilized a comprehensive set of covariates encompassing demographic information, medical history, and laboratory tests to comprehensively explore the research question. Demographic data, collected via self-report NHANES questionnaires, such as age, sex, racial/ethnic background, educational attainment, smoking status, and alcohol consumption. The calculation of BMI involved utilizing participants’ weight and height measurements. Information reported by the participants was utilized to identify individuals with physician-diagnosed coronary heart disease (CHD), HF, as well as the use of hypoglycemic drugs, lipid-lowering drugs, and antihypertensive drugs. Fasting venous blood samples were collected on-site during the survey and then sent to the Lipoprotein Analytical Laboratory at Johns Hopkins University School of Medicine. Lipid parameters, including total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) concentrations, were measured using the Hitachi 704 Analyzer. Fasting blood glucose (FBG) concentration was determined using a complete blood count (CBC) identification procedure. HbA1c levels, which provide a measure of long-term blood glucose control, were measured using high-performance liquid chromatography (HPLC) in a centralized laboratory. Hemoglobin concentrations were determined by analyzing whole blood with the Beckman Coulter MAXM instrument using a five-part differential complete blood count method. Albumin concentration was evaluated using specific antibodies that interact with albumin through an immunoturbidimetric assay. The estimated glomerular filtration rate (eGFR) was determined by applying the simplified Modification of Diet in Renal Disease (MDRD) formula, which yields an estimate of kidney function [22].
The participants were classified into three groups based on their diabetic status using the criteria provided by the American Diabetes Association (ADA): normoglycemia, which included individuals with both FBG levels below 5.6 mmol/L and HbA1c levels below 5.7%, and no prescription of hypoglycemic drugs; prediabetes, which was defined by FBG levels ranging from 5.6 to 6.9 mmol/L or HbA1c levels between 5.7 and 6.4%, or both, and no prescription of hypoglycemic drugs. Diabetes was defined as FBG levels equal to or greater than 7.0 mmol/L or HbA1c levels equal to or greater than 6.5%, or both. Additionally, individuals with a prescription of hypoglycemic drugs were classified as diabetic, irrespective of their FBG or HbA1c values [23].
The TyG-BMI index was calculated using the formula: ln [TG (mg/dL) × FBG (mg/dL)/2] × BMI [6]. The HGI value was determined by subtracting the predicted HbA1c value from the observed HbA1c value [7]. The predicted HbA1c in this study was calculated using a correlation regression equation based on the FBG and HbA1c values measured at baseline: Predicted HbA1c level = 3.212 + 0.431 × FBG (mmol/L) (r = 0.826; P < 0.001), as illustrated in Fig. 2.

A linear correlation was observed between the levels of FBG and HbA1c. The predicted HbA1c level, determined through linear regression analysis (represented by the red solid line), was calculated using the equation: Predicted HbA1c level = 3.212 + 0.431 × FBG (mmol/L)
Ascertainment of outcome
The occurrence of HF events in NHANES was determined using a combination of self-reported data and clinical assessments. NHANES incorporates a comprehensive questionnaire component that inquires about participants’ medical history, including prior HF diagnoses. Participants are explicitly queried regarding whether a healthcare professional has ever diagnosed them with HF. Upon confirmation of the initial HF diagnosis, NHANES performs comprehensive medical examinations encompassing various assessments associated with cardiovascular health. Additionally, NHANES may obtain participants’ medical records with their consent. This integrative approach, combining self-reported data, clinical assessments, and the review of medical records, aims to enhance the accuracy and validity of HF determination in NHANES.
Statistical analysis
This study adhered to the statistical analysis guidelines provided by the CDC, which can be accessed at https://wwwn.cdc.gov/nchs/nhanes/tutorials/default.aspx. Given the complex multistage stratified probability survey design employed in NHANES, our statistical analysis incorporated sample weights, clustering, and stratification to account for these factors. The baseline characteristics of the study population were presented according to their diabetes status (normoglycemia, prediabetes, diabetes) and HF status (with HF, without HF). Survey-weighted means or medians were employed to report continuous variables, whereas survey-weighted percentages were utilized for categorical variables. Receiver operating characteristic (ROC) analysis was utilized to identify the optimal thresholds of TyG-BMI and HGI for detecting HF prevalence in the total population and across different diabetes statuses. Multivariable logistic regression models were used to estimate odds ratios (ORs) and their corresponding 95% confidence intervals (CIs) to assess the independent and combined associations of TyG-BMI and HGI with HF prevalence, both for the total population and within specific diabetic subgroups. The selection of adjustment confounders was based on clinical relevance, candidate variables with a P-value of < 0.05 in univariate analysis, and the availability of events [24]. The statistical analyses were performed using R version 4.0.2 and SPSS (IBM) version 23. Statistical significance was determined based on a two-tailed P-value below 0.05.
Results
Baseline characteristics
A total of 9847 adults with hypertension were included in this study, with a mean age of 58 years. Among the participants, 51.4% were male, 32.3% had normoglycemia, 51.7% had prediabetes, 16% had diabetes, and 5.4% had HF. The baseline characteristics of the study population are presented in Tables 1 and 2, reflecting the participants’ diabetes and HF statuses, respectively. Table 1 demonstrates that patients with prediabetes and diabetes were older, more likely to be male, of Hispanic ethnicity, less educated, and had a higher prevalence of obesity. Additionally, they exhibited elevated levels of TG, FBG, TyG-BMI, HbA1c, predictive HbA1c, and HGI, as well as lower levels of HDL-C, LDL-C, albumin, and eGFR. These patients also had higher rates of hypoglycemic drugs, lipid-lowering drugs, and antihypertensive drugs, along with a higher prevalence of CHD and HF, compared to those with normoglycemia (P < 0.001). Furthermore, the hypertensive population with HF was characterized by older age, lower educational attainment, higher TG, FBG, TyG, TyG-BMI, HbA1c, predictive HbA1c, and HGI levels, as well as lower TC, HDL-C, LDL-C, hemoglobin, albumin, and eGFR levels, and a higher prevalence of hypoglycemic drugs, lipid-lowering drugs, antihypertensive drugs, CHD, and diabetes when compared to individuals without HF (P < 0.001) (Table 2).
Determination of the optimal thresholds for TyG-BMI and HGI to detect HF
Additional file 1: Table S1 displays the optimal thresholds for TyG-BMI and HGI as determined by ROC analysis. In the total population, the optimal thresholds for detecting TyG-BMI and HGI for HF were 342.89 and 0.25, respectively. Among hypertensive subjects with normoglycemia, the optimal thresholds for TyG-BMI and HGI were determined as 194.27 and − 0.19, respectively. In the prediabetic group, the optimal threshold values for TyG-BMI and HGI were 326.08 and 0.47, respectively. In the diabetic group, the optimal threshold values for TyG-BMI and HGI were 342.88 and 0.41, respectively.
Association between TyG-BMI and HGI and the prevalence of HF
The multivariate adjusted model presented in Table 3 depicts the respective associations of TyG-BMI and HGI with the prevalence of HF. In the general population, individuals with high TyG-BMI exhibited an elevated prevalence of HF (OR, 2.50; 95%CI, 1.95–3.20). Similarly, an increased prevalence of HF was observed with high HGI (OR, 1.33; 95%CI, 1.08–1.63). Among individuals in the normoglycemic group, elevated TyG-BMI and HGI did not significantly increase the prevalence of HF when compared to those with low TyG-BMI or HGI levels. Among the prediabetic population, individuals with high TyG-BMI (OR, 2.60; 95%CI, 1.89–3.58) and high HGI (OR, 1.59; 95%CI, 1.15–2.20) exhibited an elevated prevalence of HF. Likewise, diabetic patients with high TyG-BMI (OR, 2.76; 95%CI, 1.86–4.08) and high HGI (OR, 1.61; 95%CI, 1.14–2.28) displayed an increased prevalence of HF.
Combined association of TyG-BMI and HGI with the prevalence of HF
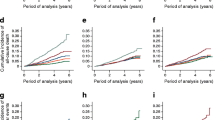
The multivariate-adjusted model presented in Table 4 illustrates the combined association of TyG-BMI and HGI with the prevalence of HF. In the joint analysis, using low TyG-BMI and low HGI as the reference, the OR and corresponding 95% CI for the combination of low TyG-BMI and high HGI, high TyG-BMI and low HGI, and high TyG-BMI and high HGI in the total population were 1.30 (1.04, 1.64), 2.40 (1.76, 3.29), and 3.47 (2.41, 4.99), respectively. Furthermore, there was a gradual increase in the prevalence of HF across all four groups, as demonstrated in Fig. 3A (P for trend < 0.001). In the normoglycemic population, higher TyG-BMI and HGI, as well as their combination, did not elevate the prevalence of HF, as depicted in Table 4; Fig. 3B. However, among individuals with prediabetes, compared to the combination of low TyG-BMI and low HGI, a higher prevalence of HF was observed in the combination of high TyG-BMI and low HGI (OR, 2.42; 95% CI, 1.69–3.48) and the combination of high TyG-BMI and high HGI (OR, 4.30; 95% CI, 2.45–7.54) (Fig. 3C, P for trend < 0.001). Similarly, in the diabetic population, the combination of low TyG-BMI and high HGI, high TyG-BMI and low HGI, and high TyG-BMI and high HGI yielded ORs (95% CI) of 2.22 (1.43, 3.45), 4.04 (2.43, 6.73), and 4.13 (2.25, 7.59), respectively, in comparison to the combination of low TyG-BMI and low HGI. Notably, a significant trend towards an increased prevalence of HF was also observed in the combination group among the diabetic population (Fig. 3D, P for trend < 0.001).

Combined association of TyG-BMI and HGI with risk of HF across the total population (A), normoglycemic individuals (B), prediabetic individuals (C), and diabetic individuals (D). The solid symbols and error bars represent the odds ratios and their corresponding 95% confidence intervals. Adjusted for survey cycle, age, sex, race, education, smoking, LDL-C, eGFR, CHD, hemoglobin, and albumin
Discussion
This study is the first to investigate the combined association of TyG-BMI and HGI with the prevalence of HF in a US representative hypertensive population, stratified based on diabetes status. The main findings are as follows: (1) Prediabetes and diabetes were characterized by unfavorable baseline factors, such as advanced age, a higher prevalence of obesity, and adverse metabolic profiles; (2) In the overall population, individuals with high TyG-BMI or high HGI had an increased prevalence of HF, with their combination demonstrating the highest prevalence; (3) Among normoglycemic populations, individuals with high TyG-BMI or high HGI did not show an increased prevalence of HF, and their combination did not result in cumulative risk effects; (4) Prediabetic and diabetic individuals with high TyG-BMI or high HGI were at a greater prevalence of HF. In the joint analysis, the combination of high TyG-BMI and high HGI was significantly associated with a higher prevalence of HF compared to other combinations.
Kiaw Er et al. [6] initially proposed the TyG-BMI and conducted a comparative analysis of TyG-BMI, TyG, and lipid-related parameters in a non-diabetic population, revealing that TyG-BMI exhibited superior diagnostic capabilities for IR. Subsequent studies have demonstrated a positive correlation between elevated TyG-BMI levels and an increased risk of various conditions, including prediabetes, hypertension, hyperuricemia, metabolic syndrome, nonalcoholic liver disease, stroke, and cardiovascular events [9, 11, 25,26,27]. Nevertheless, limited research has examined the impact of TyG-BMI on occurrence of HF among hypertensive individuals with diabetes and prediabetes. The study suggests that hypertensive individuals with elevated TyG-BMI levels may have a greater likelihood of developing HF, with this association being influenced by the presence of diabetes. Moreover, this connection was observed exclusively in individuals with prediabetes and diabetes. TyG-BMI incorporates multiple factors into a single index, thereby offering a more comprehensive assessment of metabolic health compared to relying solely on individual biomarkers. It captures the interplay among lipid metabolism, glucose homeostasis, and adiposity, all of which play a crucial role in the pathogenesis of HF [28, 29]. Moreover, the practicality, accessibility, and predictive value of TyG-BMI further strengthen its utility in investigating the association with HF and potentially enhancing risk assessment and management strategies in clinical settings.
HbA1c serves as the primary criterion for diagnosing diabetes and prediabetes [30]. However, the HbA1c level measured by the analyzer reflects only 60–80% of the average blood glucose level, and the remaining 20–40% of HbA1c variation may not be accounted for by the observed HbA1c values [31,32,33]. To provide a comprehensive reflection of the blood glucose metabolic state, Hempe et al. proposed HGI, which quantifies interindividual variations in HbA1c resulting from factors beyond blood glucose concentration [34]. While previous studies have established an association between elevated HGI and an increased risk of prediabetes, diabetes, related complications, and CVD, there is limited research exploring the relationship between HGI and the risk of HF [13, 14]. Additionally, since HGI serves as an indicator of blood glucose metabolism variations, its applicability may be influenced by the individual’s diabetes status [35]. Hence, it is imperative to evaluate the clinical significance of HGI across various blood glucose states. This study is the first to examine the association between HGI and HF across various diabetic states. The findings indicate that elevated HGI levels are linked to an increased prevalence of HF among individuals with hypertension, although this relationship is influenced by diabetes status. In particular, the positive association between HGI and the prevalence of HF was observed exclusively in individuals with prediabetes and diabetes, while no such association was found in those with normoglycemia. An examination of the relationship between HGI and HF across different diabetic statuses enables clinicians to enhance their understanding of the cardiovascular risk profile among patients with diabetes and adapt their management strategies accordingly. HGI offers supplementary information beyond conventional glycemic markers and has the potential to identify individuals in need of intensive monitoring and more aggressive interventions to prevent or manage HF. Nevertheless, additional research is necessary to validate these findings and ascertain the optimal clinical utilization of HGI in the context of managing HF.
TyG-BMI and HGI were selected as combined variables due to several clinically relevant reasons. First, TyG-BMI combines measurements of triglycerides, glucose, and BMI, all of which are established prevalence factors for HF [36]. This compound variable enables a more comprehensive evaluation of metabolic health and IR [37]. Moreover, HGI reflects the variability in glycemic control and the glycation of hemoglobin [7]. By integrating these variables, researchers intend to encompass multiple dimensions of metabolic dysfunction and assess their influence on the risk of HF. In addition, the findings demonstrated an independent association between elevated TyG-BMI and HGI values and an increased prevalence of HF. The simultaneous consideration of both variables allows clinicians to achieve a more precise assessment of HF risk and customize management strategies accordingly. Furthermore, examining the relationship between TyG-BMI, HGI, and HF across different diabetic statuses facilitates the identification of high-risk subgroups. The findings indicate that individuals in a prediabetic state who display anomalies in both metabolic markers may necessitate intensified monitoring and early intervention to avert the onset of HF. The identification of individuals exhibiting elevated combined TyG-BMI and HGI values empowers healthcare providers to introduce lifestyle modifications, optimize glycemic control, and initiate preventive measures to mitigate the risk of HF. Early intervention plays a vital role in enhancing outcomes and alleviating the burden of HF in individuals with diabetes.
Notably, gender-related differences significantly influence the prognosis of patients with these conditions. Studies, such as the one indicated by Calabrò P et al [38], have explored these differences, highlighting how gender can affect disease manifestation, progression, and response to treatment. This study, which examines the association of TyG-BMI and HGI with HF risk in hypertensive populations, can benefit from acknowledging these differences. Especially, gender may modulate the risk factors and predictive values of these indices, potentially influencing HF risk. Therefore, future research should consider gender as a critical variable in understanding and managing cardiovascular and metabolic diseases.
The biological mechanisms underlying the independent and combined associations of TyG-BMI and HGI with the prevalence of HF, as well as the modifying effect of diabetes status, are complex and not fully understood. However, there are several plausible explanations. First, TyG-BMI, which combines measures of triglycerides, glucose, and BMI, is considered a marker of IR and metabolic dysfunction [6]. IR, characterized by impaired insulin action and elevated glucose levels, leads to dysregulated lipid metabolism, inflammation, endothelial dysfunction, and oxidative stress [39, 40]. These mechanisms contribute to the development and progression of HF [41, 42]. Elevated TyG-BMI reflects these underlying metabolic abnormalities and can independently increase the prevalence of HF. Second, HGI, which measures the variability in glycemic control and glycation of hemoglobin, reflects long-term glycemic fluctuations and glycation patterns [7]. Chronic hyperglycemia in prediabetes and diabetes can result in the formation of advanced glycation end products and increased oxidative stress, promoting endothelial dysfunction, inflammation, fibrosis, and cardiac remodeling [5, 43]. These pathological processes can contribute to the development and progression of HF. Higher HGI values, indicating poorer glycemic control and increased glycation, have been associated with an independent prevalence of HF. Third, the combined effecct of TyG-BMI and HGI on HF suggests synergistic interactions between IR, metabolic dysfunction, and glycemic variability. IR and hyperglycemia can potentiate each other’s deleterious effects, leading to a more pronounced cardiac damage [44]. This synergy may result from the cumulative impact of dysregulated glucose and lipid metabolism, oxidative stress, chronic inflammation, and endothelial dysfunction [45]. The combined effects of TyG-BMI and HGI may amplify these underlying mechanisms, ultimately increasing the prevalence of HF. Fourth, diabetes status, including prediabetes and established diabetes, can modify the relationship between TyG-BMI, HGI, and HF. In individuals with prediabetes and diabetes, the presence of IR, hyperglycemia, and chronic glycemic fluctuations further exacerbates the risk of HF [46]. The modifying effect of diabetes status implies that the combined association of TyG-BMI and HGI may be more pronounced in individuals with prediabetes or established diabetes compared to those with normoglycemia. Overall, the explanations provided here are based on the current understanding of IR, metabolic dysfunction, glycemic control, and cardiac pathology. Further studies are needed to unravel the intricate interplay between these factors and to elucidate the underlying mechanisms in greater detail.
Strengths and limitations
To the best of our knowledge, this study is the first to investigate the combined association of TyG-BMI and HGI with the prevalence of HF, stratified by diabetes status. However, several limitations should be noted. First, the cross-sectional design limits the ability to establish a cause-and-effect relationship between TyG-BMI, HGI, and the prevalence of HF. It only allows for the assessment of associations at a single time point, without providing information on temporal relationships or the possibility of reverse causality. Second, without longitudinal data, it is challenging to determine whether TyG-BMI and HGI preceded the development of HF or were a consequence of it. Longitudinal studies are better suited for reexamining temporal relationships. Third, despite a large sample size, the generalizability of the findings may be limited to the US adults with hypertension under study. Fourth, the NHANES study’s limitation of only providing fasting glucose data without postprandial glucose. It prevents us from fully differentiating between the prediabetes subcategories based on impaired glucose tolerance (IGT). This finding primarily pertains to the impaired fasting glucose (IFG) aspect of prediabetes, and caution should be exercised when generalizing the results to all prediabetic states. Fifth, despite adjusting for enough confounding variables, the possibility of residual confounding and known CVD effect remains. Unmeasured or inadequately measured factors could still influence the observed associations. Finally, the study relied on self-reported data for recording outcomes, medical history, lifestyle factors, and medication use. Self-reporting introduces potential recall bias and data collection inaccuracies. However, NHANES employs rigorous quality control measures and standardized protocols to ensure the reliability and accuracy of the collected data.
Conclusions
In a nationally representative cohort of hypertensive US adults, the elevated TyG-BMI and HGI levels were associated with an increased prevalence of HF. Notably, the concurrent elevation of TyG-BMI and HGI levels was associated with the highest prevalence of HF when compared to other combinations. The relationships between TyG-BMI and HGI and the prevalences of HF were found to be influenced by the presence of diabetes. Specifically, the adverse effects of TyG-BMI and HGI on HF prevalence were observed solely in populations with prediabetes and diabetes. The clinical relevance of this study lies in its demonstration that in hypertensive patients, particularly those with prediabetes and diabetes, the combined assessment of TyG-BMI and HGI can serve as a significant predictive tool for HF risk, thereby guiding more personalized and effective risk stratification and management strategies in clinical practice.
Data availability
No datasets were generated or analysed during the current study.
References
Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GM, Coats AJ. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovascular Res. 2022;118(17):3272–87.
Ponikowski P, Anker SD, AlHabib KF, Cowie MR, Force TL, Hu S, Jaarsma T, Krum H, Rastogi V, Rohde LE. Heart failure: preventing disease and death worldwide. ESC Heart Fail. 2014;1(1):4–25.
Association AD. Treatment of hypertension in adults with diabetes. Diabetes Care. 2003;26(suppl1):80–s82.
Ferrannini E, Cushman WC. Diabetes and hypertension: the bad companions. Lancet. 2012;380(9841):601–10.
Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and Cardiovascular Disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–84.
Er LK, Wu S, Chou HH, Hsu LA, Teng MS, Sun YC, Ko YL. Triglyceride glucose-body Mass Index is a simple and clinically useful surrogate marker for insulin resistance in nondiabetic individuals. PLoS ONE. 2016;11(3):e0149731.
Hempe JM, Liu S, Myers L, McCarter RJ, Buse JB, Fonseca V. The hemoglobin glycation index identifies subpopulations with harms or benefits from intensive treatment in the ACCORD trial. Diabetes Care. 2015;38(6):1067–74.
Tao LC, Xu JN, Wang TT, Hua F, Li JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. 2022;21(1):68.
Jiang C, Yang R, Kuang M, Yu M, Zhong M, Zou Y. Triglyceride glucose-body mass index in identifying high-risk groups of pre-diabetes. Lipids Health Dis. 2021;20(1):161.
Raimi TH, Dele-Ojo BF, Dada SA, Fadare JO, Ajayi DD, Ajayi EA, Ajayi OA. Triglyceride-glucose index and related parameters predicted metabolic syndrome in nigerians. Metab Syndr Relat Disord. 2021;19(2):76–82.
Cheng Y, Fang Z, Zhang X, Wen Y, Lu J, He S, Xu B. Association between triglyceride glucose-body mass index and cardiovascular outcomes in patients undergoing percutaneous coronary intervention: a retrospective study. Cardiovasc Diabetol. 2023;22(1):75.
Soros AA, Chalew SA, McCarter RJ, Shepard R, Hempe JM. Hemoglobin glycation index: a robust measure of hemoglobin A1c bias in pediatric type 1 diabetes patients. Pediatr Diabetes. 2010;11(7):455–61.
Twomey PJ, Viljoen A, Reynolds TM, Wierzbicki AS. Biological variation in HbA1c predicts risk of retinopathy and nephropathy in type 1 diabetes. Diabetes Care. 2004;27(10):2569–70.
Kim W, Go T, Kang DR, Lee EJ, Huh JH. Hemoglobin glycation index is associated with incident chronic kidney disease in subjects with impaired glucose metabolism: a 10-year longitudinal cohort study. J Diabetes Complications. 2021;35(1):107760.
Marini MA, Fiorentino TV, Succurro E, Pedace E, Andreozzi F, Sciacqua A, Perticone F, Sesti G. Association between hemoglobin glycation index with insulin resistance and carotid atherosclerosis in non-diabetic individuals. PLoS ONE. 2017;12(4):e0175547.
Schiattarella GG, Rodolico D, Hill JA. Metabolic inflammation in heart failure with preserved ejection fraction. Cardiovascular Res. 2021;117(2):423–34.
Banerjee D, Biggs ML, Mercer L, Mukamal K, Kaplan R, Barzilay J, Kuller L, Kizer JR, Djousse L, Tracy R. Insulin resistance and risk of incident heart failure: Cardiovascular Health Study. Circulation: Heart Fail. 2013;6(3):364–70.
Kishi S, Gidding SS, Reis JP, Colangelo LA, Venkatesh BA, Armstrong AC, Isogawa A, Lewis CE, Wu C, Jacobs DR. Association of insulin resistance and glycemic metabolic abnormalities with LV structure and function in middle age: the CARDIA study. JACC: Cardiovasc Imaging. 2017;10(2):105–14.
Ashrafian H, Frenneaux MP, Opie LH. Metabolic mechanisms in heart failure. Circulation. 2007;116(4):434–48.
Ren J, Wu NN, Wang S, Sowers JR, Zhang Y. Obesity cardiomyopathy: evidence, mechanisms, and therapeutic implications. Physiol Rev. 2021;101(4):1745–807.
Yu Y, Hu L, Huang X, Zhou W, Bao H, Cheng X. BMI modifies the association between serum HDL cholesterol and stroke in a hypertensive population without atrial fibrillation. J Endocrinol Investig. 2021;44:173–81.
Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130(6):461–70.
ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, Collins BS, Hilliard ME, Isaacs D, Johnson EL, et al. 2. Classification and diagnosis of diabetes: standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):19–s40.
Yu Y, Gu M, Huang H, Cheng S, Deng Y, Cai C, Chen X, Niu H, Ning X, Hua W. Combined association of triglyceride-glucose index and systolic blood pressure with all-cause and cardiovascular mortality among the general population. J Translational Med. 2022;20(1):1–12.
Bala C, Gheorghe-Fronea O, Pop D, Pop C, Caloian B, Comsa H, Bozan C, Matei C, Dorobantu M. The Association between six surrogate insulin resistance indexes and hypertension: a Population-based study. Metab Syndr Relat Disord. 2019;17(6):328–33.
Gu Q, Hu X, Meng J, Ge J, Wang SJ, Liu XZ. Associations of Triglyceride-Glucose Index and Its Derivatives with Hyperuricemia Risk: A Cohort Study in Chinese General Population. Int J Endocrinol 2020, 2020:3214716.
Li Y, You A, Tomlinson B, Yue L, Zhao K, Fan H, Zheng L. Insulin resistance surrogates predict hypertension plus hyperuricemia. J Diabetes Investig. 2021;12(11):2046–53.
Burgeiro A, Fuhrmann A, Cherian S, Espinoza D, Jarak I, Carvalho RA, Loureiro M, Patrício M, Antunes M, Carvalho E. Glucose uptake and lipid metabolism are impaired in epicardial adipose tissue from heart failure patients with or without diabetes. Am J physiology-endocrinology Metabolism. 2016;310(7):E550–64.
Bano G. Glucose homeostasis, obesity and diabetes. Best Pract Res Clin Obstet Gynecol. 2013;27(5):715–26.
Lyons TJ, Basu A. Biomarkers in diabetes: hemoglobin A1c, vascular and tissue markers. Translational Res. 2012;159(4):303–12.
Nathan DM, Kuenen J, Borg R, Zheng H, Schoenfeld D, Heine RJ. Translating the A1C assay into estimated average glucose values. Diabetes Care. 2008;31(8):1473–8.
Delpierre G, Veiga-da-Cunha M, Vertommen D, Buysschaert M, Van Schaftingen E. Variability in erythrocyte fructosamine 3-kinase activity in humans correlates with polymorphisms in the FN3K gene and impacts on haemoglobin glycation at specific sites. Diabetes Metab. 2006;32(1):31–9.
Gonzalez-Covarrubias V, Sánchez-Ibarra H, Lozano-Gonzalez K, Villicaña S, Texis T, Rodríguez-Dorantes M, Cortés-Ramírez S, Lavalle-Gonzalez F, Soberón X, Barrera-Saldaña H. Transporters, TBC1D4, and ARID5B variants to explain Glycated Hemoglobin variability in patients with type 2 diabetes. Pharmacology. 2021;106(11–12):588–96.
Hempe JM, Gomez R, McCarter RJ Jr., Chalew SA. High and low hemoglobin glycation phenotypes in type 1 diabetes: a challenge for interpretation of glycemic control. J Diabetes Complications. 2002;16(5):313–20.
Gomez-Peralta F, Choudhary P, Cosson E, Irace C, Rami‐Merhar B, Seibold A. Understanding the clinical implications of differences between glucose management indicator and glycated haemoglobin. Diabetes Obes Metabolism. 2022;24(4):599–608.
Melanson KJ, McINNIS KJ, Rippe JM, Blackburn G, Wilson PF. Obesity and cardiovascular disease risk: research update. Cardiol Rev. 2001;9(4):202–7.
Mazidi M, Kengne A-P, Katsiki N, Mikhailidis DP, Banach M. Lipid accumulation product and triglycerides/glucose index are useful predictors of insulin resistance. J Diabetes Complicat. 2018;32(3):266–70.
Calabrò P, Niccoli G, Gragnano F, Grove EL, Vergallo R, Mikhailidis DP, Patti G, Spaccarotella C, Katsiki N, Masiero G, et al. Are we ready for a gender-specific approach in interventional cardiology? Int J Cardiol. 2019;286:226–33.
Saad MI, Abdelkhalek TM, Saleh MM, Kamel MA, Youssef M, Tawfik SH, Dominguez H. Insights into the molecular mechanisms of diabetes-induced endothelial dysfunction: focus on oxidative stress and endothelial progenitor cells. Endocrine. 2015;50:537–67.
Deedwania P. Hypertension, dyslipidemia, and insulin resistance in patients with diabetes mellitus or the cardiometabolic syndrome: benefits of vasodilating β-blockers. J Clin Hypertens. 2011;13(1):52–9.
Castro PF, Miranda R, Verdejo HE, Greig D, Gabrielli LA, Alcaino H, Chiong M, Bustos C, Garcia L, Mellado R. Pleiotropic effects of atorvastatin in heart failure: role in oxidative stress, inflammation, endothelial function, and exercise capacity. J Heart lung Transplantation. 2008;27(4):435–41.
Zuchi C, Tritto I, Carluccio E, Mattei C, Cattadori G, Ambrosio G. Role of endothelial dysfunction in heart failure. Heart Fail Rev. 2020;25(1):21–30.
Incalza MA, D’Oria R, Natalicchio A, Perrini S, Laviola L, Giorgino F. Oxidative stress and reactive oxygen species in endothelial dysfunction associated with cardiovascular and metabolic diseases. Vascul Pharmacol. 2018;100:1–19.
Rochette L, Zeller M, Cottin Y, Vergely C. Diabetes, oxidative stress and therapeutic strategies. Biochim et Biophys Acta (BBA)-General Subj. 2014;1840(9):2709–29.
Nicolls MR, Haskins K, Flores SC. Oxidant stress, immune dysregulation, and vascular function in type I diabetes. Antioxid Redox Signal. 2007;9(7):879–89.
Monnier L, Mas E, Ginet C, Michel F, Villon L, Cristol J-P, Colette C. Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. JAMA. 2006;295(14):1681–7.
Acknowledgments
The authors thank the participants of the NHANES databases.
Funding
No external funding received.
Author information
Authors and Affiliations
Contributions
Rupeng Wang, and Zening Jin conceived the research and drafted the manuscript. Rupeng Wang, Ce Chen, Guiyu Xu, and Zening Jin performed the statistical analysis. Ce Chen, Guiyu Xu, and Zening Jin were the guarantors of this work and thus had full access to all data in the study and were responsible for the integrity of the data and the accuracy of the data analysis. All authors read and approved the fnal manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol for NHANES was approved by the NCHS Research Ethics Review Board, and written informed consent was obtained from all participants.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, R., Chen, C., Xu, G. et al. Association of triglyceride glucose-body mass index and hemoglobin glycation index with heart failure prevalence in hypertensive populations: a study across different glucose metabolism status. Lipids Health Dis 23, 53 (2024). https://doi.org/10.1186/s12944-024-02045-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-024-02045-9